










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkJournal of the Southern African Institute of Mining and Metallurgy
On-line version ISSN 2411-9717
Print version ISSN 2225-6253
J. S. Afr. Inst. Min. Metall. vol.121 n.8 Johannesburg Aug. 2021
http://dx.doi.org/10.17159/2411-9717/1318/2021
PROFESSIONAL TECHNICAL AND SCIENTIFIC PAPERS
Predicting standard threshold shifts for occupational hearing loss among miners at a large-scale platinum mine in South Africa
L. NtlhakanaI, II; G. NelsonI; K. Khoza-ShangaseII; I. MaposaI
ISchool of Public Health, University of the Witwatersrand, Faculty of Health Sciences, South Africa. L. Ntlhakana: https://orcid.org/0000-0002-8632-0616; G. Nelson: https://orcid.org/0000-0001-7815-3718; I. Maposa: https://orcid.org/0000-0002-3448-4096
IIDepartment of Speech Pathology and Audiology, School of Human and Community Development, University of the Witwatersrand, Faculty of Humanities, South Africa. K. Khoza-Shangase: https://orcid.org/0000-0002-6220-9606
SYNOPSIS
Occupational noise-induced hearing loss (ONIHL) is associated with various risk factors in South African mines. We investigated the association between standard threshold shifts (STSs) and exposure to noise and platinum mine dust (PMD), using demographic data, five years of annual audiometry screening results, and noise and dust exposure data.
Miners' age, sex, percentage hearing loss (PLH), and dust and noise exposure data were gathered, and a linear mixed effects regression model used to predict STS. Average occupational exposure levels to noise and dust were calculated from recorded measurements. A total of 12 692 records were analysed. Most miners were male (89.6%) and more than 50% were younger than 41 years. More than 70% were exposed to > 85 dBA noise and 58% were exposed to 1.5-2.99 mg/m3 PMD. Changes in hearing levels ranged from 8.3 dBHL at baseline (2014/2015) to 10 dBHL in 2016 (STS), with no changes thereafter. The model showed that the estimated effect on STS for males was 27% and 21% higher than for females, for the left and right ear, respectively The estimated effect of age, PLH, noise exposure and years of exposure on STS was < 10% for each variable. There was no statistically significant association between PMD and STS.
The combined effects of age, sex, years of exposure to noise, and noise exposure levels, and strength of associations can be used to predict STS for this group of miners. Our findings may be used to measure the efficacy of the mine's hearing conservation programme.
Keywords: occupational noise-induced hearing loss, noise, platinum mine dust, standard threshold shift.
Introduction
In 2005, the most recent year for which data is available 16% of global disabling hearing impairment, which affects about four million adults, was due to occupational noise; with the burden ranging from 7% to 21% in different subregions.(Nelson et al., 2005) The estimated prevalence in African countries was 18% (12-23%).(Nelson et al., 2005) In the USA, the estimated prevalence of occupational noise-induced hearing loss (ONIHL) in the mining industry for the period 2006-2010 was reported to be 24% (Masterson et al., 2015). For South African mines during the same period a prevalence of 30% was reported (Mine Health and Safety Inspectorate, 2017). ONIHL is common in South Africa across all mining commodities. The prevalence in the gold mining sector was estimated to be 17% in 2012 (Strauss et al., 2012).
An improved understanding of risk factors for miners' hearing deterioration, in addition to those already established and considered in hearing conservation programmes (HCPs), is essential. Research on the associations of socio-demographic factors (age, sex, and race), genetic predisposition, recreational noise exposure, and occupational exposures (noise, platinum mine dust, and chemicals) (Pillay, 2020, Sepadi, Chadyiwa, and Nkosi, 2020) with ONIHL has been extensively conducted, globally (Khoza-Shangase, 2019; Campo, Morat, and Hong, 2013; 2019, Strauss et al., 2012; Brits et al., 2012; Grobler et al., 2020). Research in South African mines has shown that age, sex (Strauss et al., 2014), ototoxic drugs used for treatment of pulmonary tuberculosis (PTB) and human immunodeficiency virus (HIV) (Khoza-Shangase, 2019; Brits et al., 2012), and noise exposure levels > 85 dBA are associated with ONIHL (Edwards et al., 2015; Strauss et al., 2012; Balfour-Kaipa, 2014).
Although exposure to platinum mine dust (PMD), which contains below detectable levels of crystalline silica (Nelson and Murray, 2013; Biffi and Belle, 2003), is not directly associated with any occupational diseases, platinum miners exposed to PMD experience symptoms such as blocked nose, scratchy throat, itchy ears and eyes (Levene and Calnan, 1971; Fickl, 2007). All of these are allergic reactions that are associated with conductive hearing loss (Signia, 2018), which occurs when there is an obstruction of sound waves from the outer ear (pinna to tympanic membrane) to the middle ear; also due to a build-up of ear wax or fluid (Katz et al., 2009). This type of hearing loss is treatable but causes temporary difficulty in hearing low-frequency sounds.
The prevalence of PTB in the South African mining industry is high ( Mine Health and Safety Inspectorate, 2017), and has been associated with ONIHL in gold miners (Khoza-Shangase, 2019). PTB is also associated with exposure to silica dust in the gold mines (Nelson, 2013; Sepadi, Chadyiwa, and Nkosi, 2020). HIV is a also a risk factor for PTB (Ebonyi et al, 2016), and treatments for both PTB and HIV are ototoxic (Khoza-Shangase, 2019). Certain cancers are also treated with ototoxic drugs, e.g. cisplatin, which contains platinum salts (Lenntech, 2020). Although some research has been conducted on the association between NIHL and PTB in the South African mining industry (Khoza-Shangase, 2019), no investigation has examined the association of NIHL with exposure to PMD or ototoxic TB, HIV, and cancer treatments (Lenntech, 2020; Phanguphangu and Ramma, 2018). There is a dearth of knowledge among mine medical practitioners on the multifactorial effects of certain diseases and medical conditions, and their treatments, on the auditory system (Edwards, van Coller, and Badenhorst, 2010).
The South African HCP guideline states that programmes to prevent ONIHL should include seven pillars: noise measurement, engineering and administrative controls, hearing protection devices, risk-based medicals, medical surveillance, and audiometry (SANS, 2013). However, audiometry data and reports on miners' hearing conditions in the South African mines surveillance programmes are not integrated (Ntlhakana, Khoza-Shangase, and Nelson, 2020). Data regarding risk factors associated with miners' hearing loss, health data, and occupational hygiene data (including noise exposure measurements) is recorded in different data-sets (under the auspices of HCPs). Data on diseases such as cancer, TB, and HIV is recorded separately from audiometry data, and records are not linked for hearing conservation reporting (Khoza-Shangase, Moroe, and Edwards, 2020).
The identification of risk factors associated with hearing loss, coupled with pure-tone and distortion-product otoacoustic emissions (DPOAEs) audiometric tests, can assist in the early diagnosis of ONIHL (Moepeng, Soer, and Vinck, 2017). These two tests measure hearing thresholds across low (250 Hz) mid (1000 Hz), and high (2-8 kHz) frequencies (Feuerstein and Chasin, 2009). While both the DPOAE and pure tone tests are used in HCPs (Edwards, van Coller, and Badenhorst, 2010), it has been reported that DPOAE is more sensitive, feasible, and helpful for the early identification of ONIHL than pure-tone audiometry (Edwards and Kritzinger, 2012; Edwards, van Coller, and Badenhorst, 2010). Results from the two tests are recorded separately in the miners' audiometry records, and DPOAE results are not always available.
Workers exposed to high noise levels lose the ability to hear high-frequency sounds first (Edwards, van Coller, and Badenhorst, 2010; Grobler et al., 2020). Hearing loss, as a decline in hearing thresholds, is measured by percentage loss of hearing (PLH) (Department of Labour, 2001) and standard threshold shifts (STS) (Department of Mineral Resources, 2016). The PLH is calculated from measured hearing thresholds (0.5, 1, 2, 3, and 4 kHz), and a baseline audiogram is recorded based on this value.(Department of Labour, 2001) This is the method that was used by South African hearing conservation practitioners to define hearing loss for compensation purposes from 2001 to 2016 (Department of Labour, 2001).
The STS method is based on an International Organization for Standardization (ISO) standard (ISO1999:2013) which specifies that a decline of 8 dB in the STS indicates early ONIHL. The STS method has been used by South African mines since 2016 to benchmark miners' hearing and to track STS deterioration as a function of hearing loss (Strauss et al., 2012; Grobler et al., 2020). In 2008, the Department of Mineral Resources and Energy (DMRE) set NIHL milestones for the mining industry, stating that, after December 2008, the HCP implemented by the industry 'must ensure that there is no deterioration in hearing greater than ten per cent amongst occupationally exposed individuals' (Msiza, 2014; Department of Mineral Resources and Energy, 2008). However, hearing loss prevention efforts were not successful (Edwards and Kritzinger, 2012) and the DMRE revised the milestones in 2014 (Chamber of Mines, 2016), stating that, by December 2016 no employee's STS will exceed 10 dBHL from the baseline when averaged at 2000, 3000, and 4000 Hz in one or both ears (MHSC, 2015).
Thus, STS was prioritized in the measurement of hearing loss for miners. Normal hearing is recorded as 0 dBHL (Chamber of Mines, 2016). A STS is defined as an average shift in hearing threshold of 10 dBHL. Although there is no hearing loss at this stage, any shift > 10 dBHL should be reported, and warrants investigation and intervention (Chamber of Mines, 2016). A shift in the hearing threshold of > 25 dBHL for one or both ears indicates hearing loss. Thus, diagnostic audiometry is required in order to confirm hearing loss (Department of Mineral Resources and Energy, 2016). Worldwide, STS has been used to describe the hearing function of workers exposed to excessive noise levels since the early 2000s (Masterson et al., 2016; Heyer et al., 2011). The South African mining industry's hearing loss prevention efforts, as per the NIHL 2016 milestones, are now aligned with first world countries such as the USA. However, the success of these interventions will only be assessed in 2024 (MHSC, 2015).
The purpose of our analysis was to examine the association of STS with exposure to noise and PMD, and to develop prediction model for STS for miners employed at one of South Africa's large platinum mines, using demographic data and five years of audiometry, noise, and dust data.
Methods
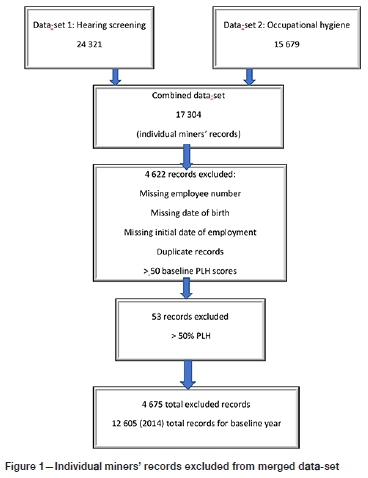
The results of individual miners' hearing screening tests and occupational hygiene data from 2014 to 2018 were analysed. Data on diseases was not available. We accessed 24 321 hearing screening records and 15 769 occupational hygiene records (noise exposure levels) from the mine's two available data-sets. The hearing screening data-set contained audiometry screening records from examinations conducted by a qualified audiometrist (occupational health nurse) according to the South African National Standard (SANS) 10083:2013.(SANS, 2013), bilateral audiometry results at frequencies of 0.5, 1, 2, 3, 4, 6, and 8 kHz, calculated PLH, and averaged bilateral STS. The occupational hygiene data-set contained information about occupation (job title), noise exposure levels (dBA), and total PMD exposure measurements (mg/m3) for each miner, collected by a qualified occupational hygienist. Both data-sets included the miner's employee number, age, and sex. These three variables were used to combine the data-sets using STATA (version 15.1). The data was further categorized using the mine's risk rankings as follows: PLH as low (0-2%), moderate (2.1-5%) and high (>5%); noise exposure levels as 0-81.99 dBA, 82-84.99 dBA, 85-104.99 dBA, and 105-160 dBA; dust exposure levels as 0-0.299 mg/m3, 0.3-1.499 mg/m3, 1.5-2.99 mg/m3, and 3-100mg/m3, as well as the standard hearing loss classifications of mild (26-45 dBHL), moderate (46-55 dBHL), moderately-severe (56-70 dBHL), severe (71-90 dBHL), and profound (>90 dBHL) (Katz et al., 2009).
Permission to use the miners' data was granted by the mine management, and ethical clearance was obtained from the University of the Witwatersrand's Human Research Ethics Committee (clearance certificate no. M180273).
The combined data-set contained 17 304 electronic records (Figure 1). A total of 4 675 duplicate records, records with no employee numbers, records with no initial dates of employment, records with more than two baseline PHL values, and records with > 50% PLH (invalid calculations) were excluded. The number of records included in the analysis differed from year to year - 12 605 for 2014, 12 602 for 2015, 12 599 for 2016, 12 591 for 2017, and 12 592 for 2018.
Data analysis
Frequencies and percentages were used to describe miners' sex, age group, noise exposure and PMD levels, and PLH and STS categories. Medians and ranges were used to describe continuous PLH and STS scores. Differences in male and female miners' STS were graphically depicted by age group and PLH category.
A linear mixed effects model was used to estimate the effects of different exposure factors on the bilateral STS, using continuous data from all the variables with the exception of sex.
Distributions of selected variables, including bilateral STS, were assessed to ascertain skewness before fitting the model. The bilateral STS (left and right) data were skewed and were therefore log-transformed before fitting the model. For the mixed effects model, when fitting the bilateral STS levels to predictor variables, a random intercept was assumed. The estimates are reported with 95% confidence intervals. Significance for two-sided tests was set at P < 0.05. Goodness of fit of the final prediction model was tested using the likelihood ratio test.
Results
The characteristics of the miners in the 2018 cohort are shown in Table I. There were more males (n = 11 283; 89.6%) than females (n = 1 309; 10.4%); most (53.4%) were younger than 41 years, most (76.4%) had low PLH; 72.4% were exposed to noise levels of 85 dBA or higher; and 57.9% were exposed to 1.5-2.99 mg/ m3 PMD. Approximately 10% of the miners had high PLH (> 5%) and STS > 26 dBHL.
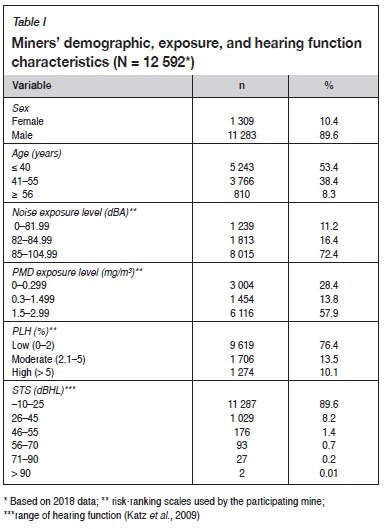
Table II shows the medians and range used to describe the miners' hearing function measurements (PLH and STS). The median PLH did not change throughout the study period (1.2%); some miners had a maximum PLH range of up to 50%. The median STS was 8.3-10 dBHL, with a hearing deterioration (STS) of 1.7 dBHL from baseline to 2016 in the left ear, and to 2017 in the right ear. Some miners had a maximum STS range of up to 99 dBHL at baseline, which increased to 95 dBHL by 2018.
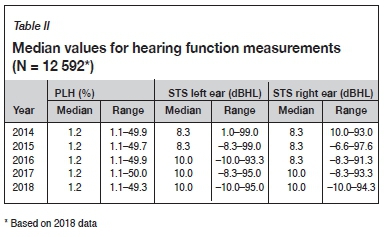
Figure 2 shows STS for the left ear for male and female miners of different age groups and PLH categories across the five years of follow-up. There was a small increase in mean STS over the five years in the high PLH category for males > 41 years. Male miners in most PLH categories had higher mean STS levels than female miners in all years of exposure, across different age categories. The differences in mean STS between males and females were greatest in the high PLH and > 41 years age categories.
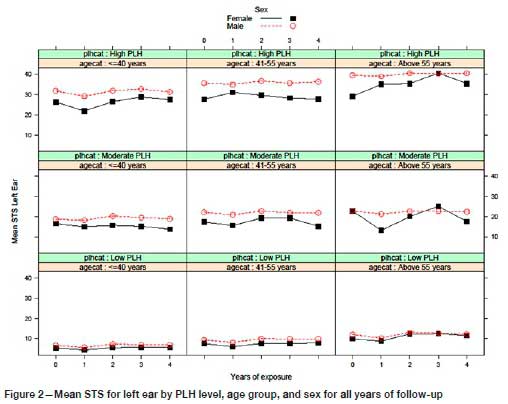
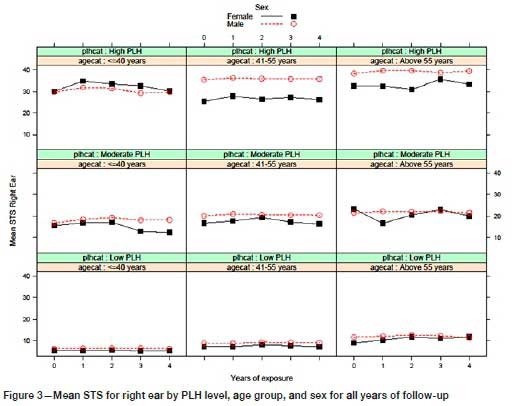
Figure 3 shows STS for the right ear for male and female miners of different age groups and PLH categories, across the five years of follow-up. There was a small increase in mean STS over the five years in the high PLH category for males > 41 years. Male miners in most PLH categories had higher mean STS levels than female miners in all years of exposure, across different age categories. The differences in mean STS between males and females were greatest in the high PLH and > 41 years age categories.
Predicting standard threshold shifts for occupational hearing loss
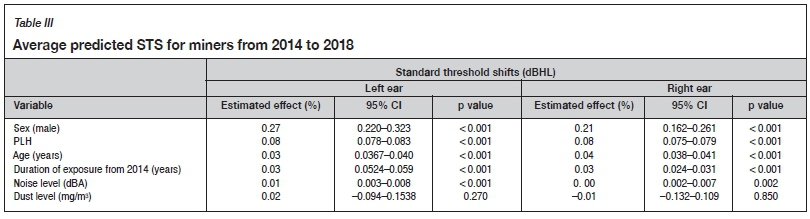
The year 2014 was set as the baseline year; 2015, 2016, 2017, and 2018 represented cumulative years of noise and dust exposure. The log-transformed STS data was used in the mixed effects linear regression model as the outcome variable; the predictor variables were sex, age, PLH, noise exposure level, dust exposure level, and years of exposure (as described in Table III). The model showed that the estimated effect on STS for males was 27% and 21% higher than for females, for the left and right ear, respectively. The estimated effects on STS of a unit increase in PLH, age, duration of exposure, and noise exposure level were all < 10%, but nevertheless statistically significant. The effect of dust exposure on STS was not statistically significant. The likelihood ratio test showed that the predictive model was a good fit (p < 0.001).
Figure 4 shows an increasing effect of years of exposure on predicted STS for both male and female miners, controlling for age, PLH, and noise and dust levels. There was a steady increase in the predicted STS (and, therefore, a gradual hearing deterioration) for both the left and the right ears over time. Males start with a higher baseline STS and maintain higher STS levels across all years of exposure, compared to females.
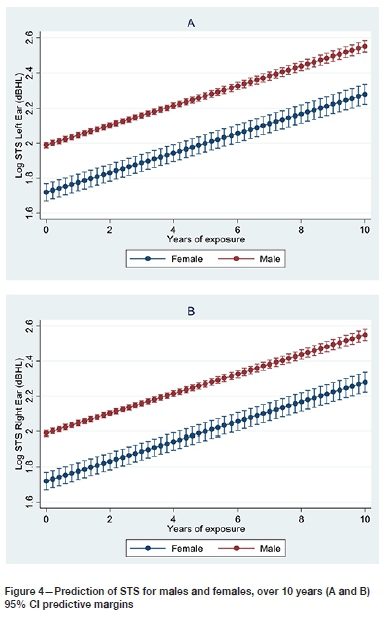
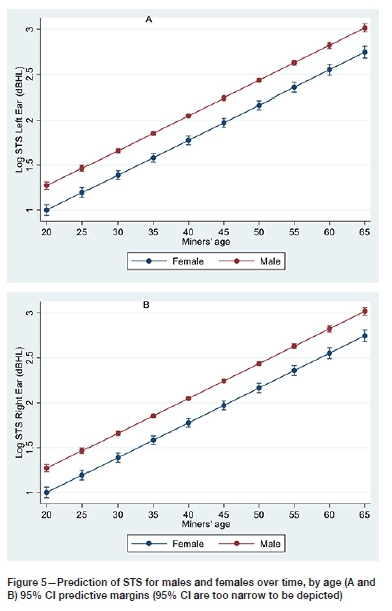
Figure 5 shows the effect of increasing age on the predicted STS for males and females, when years of exposure, PLH, and noise and dust levels were controlled for. For males, the predicted STS increased steadily, and was higher than that for females for both the left and right ears. Again, males start with a higher baseline STS than females, which is consistent across all ages.
Discussion
Although the STS milestone (Regulation 839) was introduced by the DMRE and due to be updated in 2024 ('by December 2016, no employee's STS will exceed 10 dB from the baseline when averaged at 2000, 3000 and 4000 Hz in one or both ears') (Chamber of Mines, 2016), our study is the first to evaluate the progress made by this platinum mine. By analysing the mine's data we were able to benchmark miners' hearing, track STS deterioration, and identify miners at risk of developing hearing loss.
In this group of miners, both age and sex were associated with deterioration in hearing, measured by increases in STS in the high frequencies. This supports the findings of Grobler et al. (2020) that male gold miners older than 40 years and exposed to excessive occupational noise had hearing deterioration in the high frequencies. Bilateral loss of hearing, measured by STS (HFA234) was generally worse in male than female miners. This may be due to differences in genetic susceptibility (Sliwinska-Kowalska and Pawelczyk, 2013), recreational noise exposure (Gates et al., 2000), previous occupational noise exposure (Grobler et al., 2020), diagnosis of conductive hearing loss (Ntlhakana, Khoza-Shangase, and Nelson, 2020), or medical conditions such as TB and HIV, and treatments thereof (Khoza-Shangase, 2019). Recently, coronavirus (COVID-19), associated with otitis media (Fidan, 2020) and otitis media, have been included among the risk factors that affect South African miners (Ntlhakana, Khoza-Shangase, and Nelson, 2020). Exclusion of this data from the audiometry records may lead to an under-estimation of the miners' hearing deterioration.
Hearing threshold changes and hearing deterioration that is due to a combination of various factors, including occupational noise exposure, are gradual and incremental. This has been reported previously in South African gold mines (Strauss et al., 2014; Grobler et al., 2020). Some miners had presented with hearing loss in 2018, ranging from 26 dBHL to 90 dBHL, which may prevent the mine from achieving the NIHL milestone target for 2024. Furthermore, some miners' pure-tone air conduction data was not available for every year, so the mine did not consistently follow audiometry requirements for individual miners who were at risk of developing ONIHL. Standard threshold shifts and hearing severity classification scales should be used together, from baseline, to measure miners' hearing deterioration and for early identification of at-risk miners. Our findings may be used by the participating mine to achieve the targets for the NIHL milestone for 2024.
Although the participating mine's noise exposure records showed a maximum noise exposure level (105 dBA) that was below the DMRE's targeted level of 107 dBA for 2024 (Chamber of Mines, 2016), more than 70% of the miners in the cohort were exposed to > 85 dBA over the five-year period. This is a concern as acoustic pressure at > 85 dBA damages the auditory system (Rodrigue, 2020; Grobler et al., 2020). Cumulative exposure to high noise levels had a negative impact on miners' auditory systems, as some of the miners in our study presented with STS that ranged between 26 dBHL and >90 dBHL (Ntlhakana, Khoza-Shangase, and Nelson, 2020). High noise exposure levels will continue to increase the miners' risks of ONIHL.
There are no studies on the effects of dust exposure on hearing loss, which may be due to the fact that dust exposure levels in the South African platinum mines are lower than the regulated occupational exposure level (OEL) of 3 mg/m3 (Belle and Stanton, 2007). Although more than half of the miners in the database were exposed to 1.5-2.99 mg/m3 PMD, which is classified as 'significant' according to the mine's PMD risk ranking scale, we found no effect of PMD on hearing function. However, some platinum miners have reported irritation of the throat, nose, ears, and eyes (Levene and Calnan, 1971), which are allergic reactions to PMD that are associated with conductive hearing loss (Levene and Calnan, 1971). Therefore, other types of hearing loss such as conductive hearing loss should be considered to avoid an over-estimation of ONIHL as well as to account for different types of hearing loss that affect miners (Sebothoma, 2020). The findings of this analysis also have implications for preventive audiology in the form of early identification of hearing impairment in miners, and interventions to both reduce the risk of progressive hearing loss in those already affected and prevent hearing loss in miners who are not yet affected (Khoza-Shangase, Moroe, and Edwards, 2020).
Despite the fact that some studies have reported effects of PTB and HIV treatment on miners' hearing function (Khoza-Shangase, 2019), and that certain treatments for these diseases and cancer are ototoxic (Khoza-Shangase, 2019; Lenntech, 2020; Phanguphangu and Ramma, 2018), we were not able to access miners' medical records on PTB, HIV, and cancer treatment, as these records were in a database that was separate from the audiometry data. A lack of integration of the miners' PTB, HIV, and cancer data with audiometry data limits understanding of the miners' hearing function and deterioration.
Hearing changes due to occupational and individual characteristics occur gradually over time and reflect the mine's HCP efficiency. Our findings were similar to those of Strauss et al. (2014) and Grobler et al. (2020) in that hearing thresholds of males were more adversely affected than those of females. We predicted that the estimated effect on STS associated with being males was more than that of PLH, age, years of exposure, and noise exposure, although all were statistically significant. Our model showed that age had a small effect on STS compared to sex, which was surprising because studies on South African gold miners have reported age to be associated with ONIHL (Strauss et al., 2014; Grobler et al, 2020). There was also evidence that males started with higher STS than females, when years of exposure and age were controlled for, and thus were more susceptible to hearing loss from baseline than females. Furthermore, our model predicted a gradual STS deterioration over 10 years which, without intervention, will continue. Although we used five years (2014-2018) of data in our analysis, the mean duration of employment and noise exposure for platinum miners was more than five years (Ntlhakana, Khoza-Shangase, and Nelson, 2020). The model showed that combined exposure variables produced an effect on the bilateral STS over a period of time. This presents an opportunity for the mines to use our prediction model and to include miners' exposure variables (age, sex, noise, dust exposure levels, and duration of exposure) to predict hearing deterioration, with the hope of identifying miners at risk of occupational hearing loss.
Most investigations of the prevalence of ONIHL among miners have used cross-sectional study designs (Khoza-Shangase, 2019; Moepeng, Soer, and VInck, 2017; Strauss et al., 2012, 2014; Brits et al., 2012; Campo, Morata, and Hong, 2013; Masterson et al., 2016; Heyer et al., 2011). These have provided limited evidence for synergistic risk factors in occupational hearing loss, and no time-specific information associated with the onset and development of ONIHL. We conducted a retrospective cohort analysis that used the miners' longitudinal data to understand risk factors associated with hearing function. However, prospective cohort longitudinal studies would improve our understand of the development of ONIHL and its associated risk factors over time (Seixas et al., 2012; Worku and Ohaju, 2004).
Strength and limitations
A strength of our study was the use of large data-sets that included miners' occupational exposures and audiometry data to understand the mine's recording of occupational exposure and audiometry data to determine trends in the miners' hearing function.
The main limitation was the unavailability of the miners' medical surveillance records linked to the data-sets used in the study. We could therefore not include medical conditions that cause conductive hearing loss (e.g. allergies, COVID-19), chronic medical conditions such as PTB and HIV, and medications used to treat PTB and HIV, in the analysis and in the predictive model. This mine cited the POPI and Medical Ethics Acts as stumbling blocks to providing the miners' medical records, which are classified as confidential with limited rights of access. Thus, effects due to ototoxicity were not factored into our analysis. In addition, there was no information about other factors associated with NIHL, such as recreational noise exposure and previous occupational noise exposure. It is therefore possible that we overestimated the prevalence of ONIHL. This mine's HCP data was not integrated, and some miners' records omitted demographic and audiometry data, hence 2014 was used as the baseline year, which was not necessarily a true baseline for miners in this study.
Conclusion
This is the first study conducted at a South African mine that includes miners' audiometry and occupational exposure data to predict hearing changes over a period of time. We showed that demographic characteristics (age and sex) and occupational exposures (noise) can be used to predict occupational hearing deterioration and calculated the contribution of each variable over a period of time. We showed that miners' STS changes are gradual over time and are due to a combination of risk factors, not only noise exposure. These findings may be used to evaluate HCP efficacy at this and other mines.
The miners' demographic data and risk ranking categories for occupational and audiometry data may be useful for development of the HCP data repository for this and other South African mines. We have highlighted gaps in the literature on the potential association of exposure to PMD and conductive hearing loss in the South African platinum mines. Our results reinforce the need to shift the focus from ONIHL prevention only towards HCPs that will address different types of hearing loss.
Acknowledgements
The authors would like to thank the participating mine for permission to use their data in this study, and the hearing conservation medical and occupational hygiene practitioners for technical guidance. This study was funded by the University of the Witwatersrand Faculty of Humanities Research Committee. Grant sponsor: Faculty of Humanities Research Committee; ad hoc grant.
References
Balfoür-Kaipa, T. 2014. Occupational Health Milestones and Chamber's response to key health issues. Occupational Health Southern Africa, vol. 20. pp. 26-27. [ Links ]
Belle, B.K. and Stanton, D.W. 2007. Inhalable and respirable dust. Handbook on Mine Occupational Hygiene Measurements. Stanton, D.W., Kielblock, J., and Schoeman, J.J. (eds). Mine Health and Safety Council (MHSC), Johannesburg. [ Links ]
Biffi, M. and Belle, B.K. 2003. Quantification of dust-generating sources in gold and platinum mines. GAP 802. Mine Health and Safety Council. Johannesburg. [ Links ]
Brits, J., Strauss, S., Eloff, Z., Becker, P.J. and De Swanepoel, W. 2012. Hearing profile of gold miners with and without tuberculosis. Occupational and Environmental Medicine, vol. 69. pp. 243-249. [ Links ]
Campo, P., Morata, T.C., and Hong, O. 2013. Chemical exposure and hearing loss. Disease-a-Month, vol. 59, no. 4. pp. 119-138. doi: 10.1016/j.disamonth.2013.01.003 [ Links ]
Chamber of Mines. 2016. Noise Team on the Mine Health and Safety Milestones. Johannesburg. [ Links ]
Department of Labour. 2001. Circular instruction no. 171 - The determination of permanent disablement resulting from hearing loss caused by exposure to excessive noise and trauma. Pretoria. [ Links ]
Department of Mineral Resources. 2016. Guidance note for the implementation of standard threshold shift in the medical surveillance of noise induced hearing loss. Pretoria. [ Links ]
Department of Minerals and Energy. 2008. Presidential Mine Health and Safety Audit. Pretoria. [ Links ]
Ebonyi, A.O., Oguche, S., Ejeliogu, E.U., Agbaji, O.O., Shehu, N.Y., Abah, I.O., Sagay, A.S., Ugoagwu, P. O., Okonkwo, P.I., Idoko, J.A., and Kanki, P.J. 2016. Prevalence of and risk factors for pulmonary tuberculosis among newly diagnosed HIV-1 infected Nigerian children. Germs, vol. 6. pp. 21-8. [ Links ]
Edwards, A. and Kritzinger, D. 2012. Noise-induced hearing loss milestones: past and future. Journal of the Southern African Institute of Mining and Metallurgy, vol. 112. pp. 865-869. [ Links ]
Edwards, A., van Coller, P., and Badenhorst, C. 2010. Early identification of noise induced hearing loss: A pilot study on the use of distortion product otoacoustic emissions as an adjunct to screening audiometry in the mining industry. Occupational Health Southern Africa, vol. 6. http://www.occhealth.co.za/?/viewArticle/1164 [ Links ]
Edwards, A.L., Malanzi, M., Khoza, N.N., and Zungu, L.I. 2015. Evaluation of the current practices of noise induced hearing loss awareness training in the South African mining industry. Occupational Health Southern Africa, vol. 21, no. 5. pp. 11-17. [ Links ]
Feuerstein, J. and Chasin, M. 2009. Noise exposure and issues in hearing conservation. Handbook of Clinical Audiology. 7th edn. Lippincott Williams & Wilkins, Baltimore, MD. [ Links ]
Fickl, H. 2007. Investigation of the pro-oxidative and pro-inflammatory interactions of cobalt, palladium, platinum and vanadium with human neutrophils in vitro. PhD thesis, University of Pretoria. [ Links ]
Fidan, V. 2020. New type of corona virus induced acute otitis media in adult. American Journal of Otolaryngology, vol. 41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7161479/ [ Links ]
Gates, G.A., Schmid, P., Kujawa, S O., Nam, F., and D'Agostino, R. 2000. Longitudinal threshold changes in older men with audiometric notches. Hearing Research, vol. 141. pp. 220-228. [ Links ]
Grobler, L.M. 2019. Occupational noise and age: A longitudinal study of hearing sensitivity. M. Pathology (Audiology) dissertation, University of Pretoria. [ Links ]
Grobler, L.M., Swanepoel, D.w., Strauss, S., and Eloff, P.B.Z. 2020. Occupational noise and age: A longitudinal study of hearing sensitivity as a function of noise exposure andage in South African gold mine workers. South African Journal of Communication Disorders, vol. 67, no. 2. https://sajcd.org.za/index.php/sajcd/article/view/687/1165 [ Links ]
Heyer, N., Morata, T.C., Pinkerton, I., Brueck, S.E., Stancesc, d., Panaccio, M.P., Kim, H., Sinclair, S.J., Waters, M.A., Estill, C., and Franks, J.R. 2011. Use of historical data and a novel metric in the evaluation of the effectiveness of heairng conservation program components. Occupational and Environmental Medicine, vol. 68. pp. 510-517. [ Links ]
Mine Health and Safety Inspectorate. 2017. State of health in the South African mining industry. Annual Report. Department of Mineral Resources, Pretoria. [ Links ]
Katz, J., Medwetsky, I., Burkard, R., and Hood, I. 2009. Pure tone evaluation. Handbook of Clinical Audiology. Katz, J. (ed.). Lippincott Williams & Wilkins, Baltimore, MD. [ Links ]
Khoza-Shangase, K. 2019. Hearing function of gold miners with and without a history of tuberculosis treatment: A retrospective data review. Brazilian Journal of Otorhinolaryngology, vol. 86, no. 3. pp. 294-299. [ Links ]
Khoza-Shangase, K., Moroe, N.F., and Edwards, A. 2020. Occupational hearing loss in Africa: An interdisciplinary view of the current status. South African Journal of Communication Disorders, vol. 67, no. 2. doi: 10.4102/sajcd.v67i2.700 [ Links ]
Lenntech, B.V. 2020. Platinum. https://www.lenntech.com/periodic/elements/pt.htm [accessed 7 May 2020]. [ Links ]
Levene, O. and Calnan, CD. 1971. Platinum sensitivity: treatment by specific hyposensitization. Clinical Allergy, vol. 1. pp. 75-82. [ Links ]
Masterson, A., Bushnell, P.T., Themann, CL., and Morata, T.C. 2016. Hearing impairment among noise-exposed workers - United States, 2003-2012. Morbidity and Mortality Weekly Report (MMWR), vol. 65. pp. 389-94. [ Links ]
Masterson, A., Deddens, J., Themann, C., Bertke, S., and Calvert, G.M. 2015. Trends in worker hearing loss by industry sector, 1981-2010. American Journal fo Industrial Medicine, vol. 58. pp. 392-401. [ Links ]
MHSC. 2015. 'Every mine worker returning from work unharmed every day. Striving for zero harm' - 2014 Occupational Health and Safety Summit Milestones. Journal of Occupational Health Southern Africa, vol. 20, no. 2. [ Links ]
Moepeng, M., Soer, M., and Vinck, B.M. 2017. Distortion product otoacoustic emissions as a health surveillance technique for hearing screening in workers in the steel manufacturing industry. Occupational Health Southern Africa, vol. 22. pp. 8-13. [ Links ]
Msiza, D. 2014. The road to zero harm: new milestones. Mine Health and Safety Council, Johannesburg. [ Links ]
Nelson, D.i., Nelson, R.Y., Concha-Barrientos, M., and Fingerhut, M. 2005. The global burden of occupational noise-induced hearing loss. American Journal of Industrial Medicine, vol. 48. pp. 446-58. [ Links ]
Nelson, O. 2013. Occupational respiratory diseases in the South African mining industry. Global Health Action, vol. 6. pp. 89-98. [ Links ]
Nelson, O. and Murray, J. 2013. Silicosis at autopsy in platinum mine workers. Occupational Medicine, vol. 63. pp. 196-202. [ Links ]
Ntlhakana, I., Khoza-Shangase, K., and Nelson, O. 2020. Occupational noise-induced hearing loss in platinum miners: What do the data tell us? Occupational Health Southern Africa, vol. 26. pp. 8-14. [ Links ]
Phanguphangu, M. and Ramma, I. 2018. High incidence of cisplatin-induced ototoxicity in paediatric patients in the Western Cape, South Africa. South African Journal of Oncology, vol. 2. doi: https://doi.org/10.4102/sajo.v2i0.41 [ Links ]
Pillay, M. 2020. Chemicals, noise and occupational hearing health in South Africa: A mapping study. South African Journal of Communication Disorders, vol. 67, no. 2. doi: https://doi.org/10.4102/sajcd.v67i2.693 [ Links ]
Rodrigue, J. 2020. Transportation and the environment. The Geography of Transport Systems. Rodrigue, J. (ed.). 5th edn. Routledge, New York. [ Links ]
SANS. 2013. The measurement and assessment of occupational noise for hearing conservation purposes. South African National Standards, Pretoria. [ Links ]
Sebothoma, B. 2020. Middle ear pathologies in adults within the mining industry: A systematic review. South African Journal of Communication Disorders, vol. 67. https://sajcd.org.za/index.php/sajcd/article/view/679/1157 [ Links ]
Seixas, N.S., Neitzel, R., Stover, F., Sheppard, I., Feeney, P., Mills, d., and Kujawa, S. 2012. 10-Year prospective study of noise exposure and hearing damage among construction workers. Occupational and Environmental Medicine,vol. 69. pp. 643-650. [ Links ]
Sepadi, M.M., Chadyiwa, M., and Nkosi, V. 2020. Platinum mine workers' exposure to dust particles emitted at mine waste rock ,crusher plants in Limpopo, South Africa. International Journal of Environmental Research and Public Health, vol. 17. doi: 10.3390/ijerph17020655 [ Links ]
SIGNIA. 2018. Allergy or sudden hearing loss-Can you tell the difference? [accessed 29 May 2020]. https://assets.signia-hearing.com/blog/allergy-sudden-hearing-loss-can-tell-difference/ [accessed 29 May 2020]. [ Links ]
Sliwinska-Kowalska, M. and Pawelczyk, M. 2013. Contribution of genetic factors to noise-induced hearing loss: A human studies review. Mutation Research/ Reviews in Mutation Research, vol. 752. pp. 61-65. [ Links ]
Strauss, S., Swanepoel, d., Becker, P., Eloff, Z., and Hall, J.W. 2012. Prevalence and degree of noise induced hearing loss in South African gold miners. Occupational Health Southern Africa, vol. 18, no. 6. pp. 20-25. shttps://journals.co.za/doi/10.10520/EJC128495 [ Links ]
Strauss, S., Swanepoel, D.w., Becker, P., Eloff, Z., and Hall, J.W. 3RD 2014. Noise and age-related hearing loss: a study of 40 123 gold miners in South Africa. International Journal of Audiology, vol. 53, suppl. 2. pp. S66-575. [ Links ]
Worku, Z. and Ohaju, M. 2004. A statistical analysis of common occupational diseases among South African miners from 2000 to 2003. Occupational Health Southern Africa, vol. 10, no. 5. pp. 16-21. [ Links ]
 Correspondence:
Correspondence:
L. Ntlhakana
Email: liepollo.ntlhakana@wits.ac.za
Received: 11 Aug. 2020
Revised: 15 Apr. 2021
Accepted: 22 Apr. 2021
Published: August 2021


{kind=link}