










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Laboratory Medicine
On-line version ISSN 2225-2010
Print version ISSN 2225-2002
Afr. J. Lab. Med. vol.12 n.1 Addis Ababa 2023
http://dx.doi.org/10.4102/ajlm.v12i1.2044
ORIGINAL RESEARCH
Using the SLIPTA checklist to assess laboratory readiness for Joint Commission International accreditation
Abdul K. El Karaaoui; Nada Assaf
Department of Pathology and Laboratory Medicine, Faculty of Medicine, American University of Beirut, Beirut, Lebanon
ABSTRACT
BACKGROUND: The Stepwise Laboratory Improvement Process Towards Accreditation (SLIPTA) helps prepare laboratories in low- and middle-income countries to achieve international accreditation aligned with the ISO 15189:2012 standards. Accreditation by the Joint Commission International (JCI) is among the highest sought by hospitals worldwide. While the readiness of laboratories with a five-star SLIPTA score to undergo ISO 15189:2012 accreditation was recently assessed, the compliance of the SLIPTA checklist with JCI is still unknown
OBJECTIVE: The study evaluated the SLIPTA checklist's utility in assessing laboratories to meet the JCI standards.
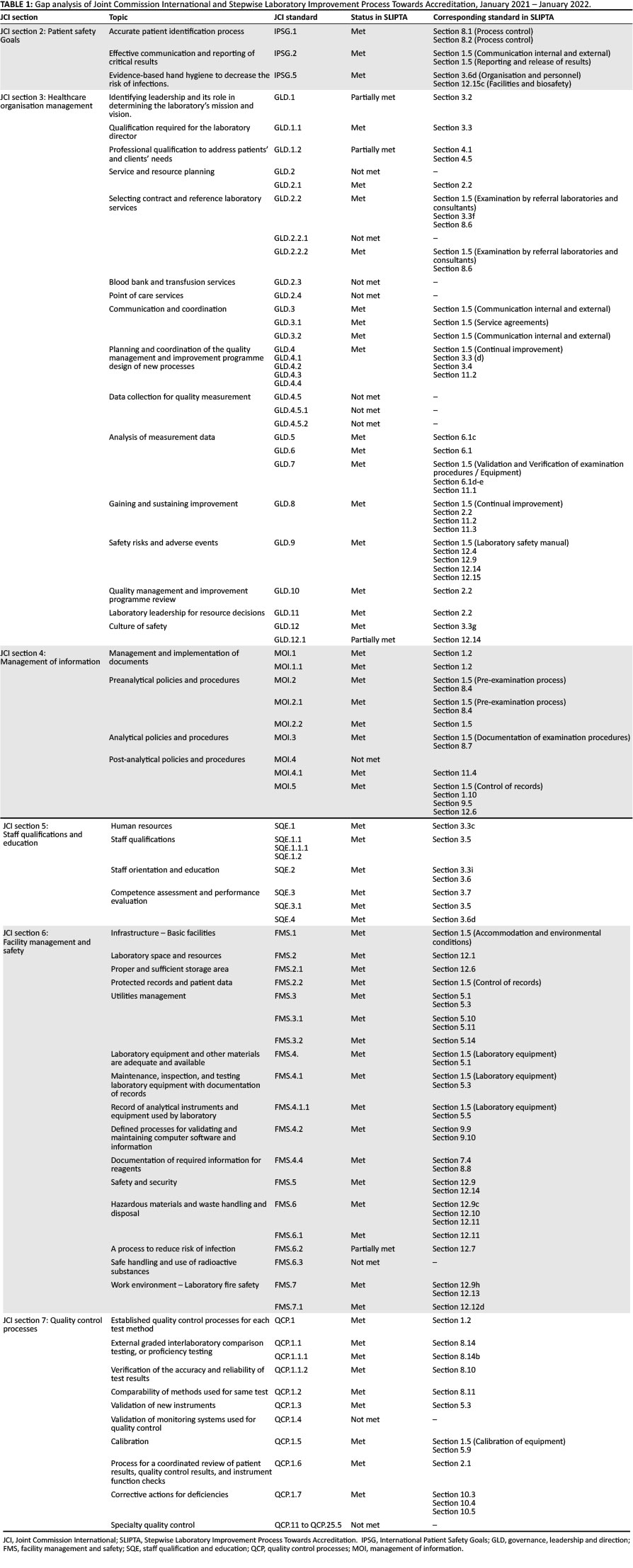
METHODS: We conducted a detailed gap analysis between SLIPTA and JCI laboratory standards from January 2021 to January 2022. We cross-matched the JCI standard requirements to SLIPTA clauses and categorised each standard into 'met', 'partially met', and 'not met'. We highlighted similarities, discrepancies, and improvement areas.
RESULTS: A total of 109 JCI standards were included. The SLIPTA checklist completely met 61 standards, partially met four, but did not meet 44. The unmet JCI standards focused on the quality planning, control, and improvement sections. Healthcare organisation management and quality control processes, including selecting an accredited reference laboratory, collecting quality management data, creating of post-analytical policies and procedures, and validating monitoring systems, constitute the basis of this preparation.
CONCLUSION: The SLIPTA checklist covers major quality management system elements of the JCI standards for laboratories. However, some components should be addressed to assure readiness for JCI accreditation.
What this study adds: This study identified additional areas not covered by the SLIPTA checklist that are required for JCI accreditation.
Keywords: standard culture; Joint Commission International; laboratory accreditation; low- and middle-income countries.
Introduction
Medical laboratories play a pivotal role in maintaining the healthcare chain in a nation. Laboratory services are crucial for disease prevention, diagnosis, surveillance, and treatment.1,2 In developed countries, up to 70% of clinical decisions depend on laboratory test results.3,4 As such, maintaining quality laboratory services is essential for the efficient functioning of the healthcare system.
Accreditation is an external quality review that evaluates an organisation's conformity with a predefined set of standards to receive formal recognition of compliance by an authorised external body.5 As a primary goal, laboratory accreditation aims to improve patient safety and the standard of care.6 In addition, accredited laboratories show superior test reliability, better operational efficiency, and higher competence.7
With increased outbreaks of diseases such as HIV, tuberculosis, and the recently emerging coronavirus disease 19 in low- and middle-income countries (LMICs), there is increased attention on strengthening healthcare systems in limited-resource areas.8
In 2009, the World Health Organization Regional Office for Africa, in collaboration with the African Society for Laboratory Medicine, the United States Center for Disease Control and Prevention and African countries consorted on the creation of a Stepwise Laboratory Improvement Process Towards Accreditation (SLIPTA) to implement quality management systems (QMS) and organise quality improvement processes in LMIC laboratories.9 The SLIPTA programme consists of a checklist questionnaire linked to a five-star recognition depending on the level of compliance ranging from ≤ 55% (0 stars) to ≥ 95% (5 stars).8,9 It is an interim recognition, and laboratories that achieve a SLIPTA five-star rating are encouraged to apply for international accreditations such as ISO 15189:2012 and Joint Commission International (JCI).8
Founded in 1951, JCI is today the largest international accreditation body for hospitals.11 The JCI laboratory accreditation standards cover all laboratory needs for continual improvement within a quality management environment.11 It also addresses essential laboratory managerial and clinical functions while focusing on patient safety.11 Because JCI is a hospital accreditation scheme, laboratory JCI clauses are clinically oriented. Therefore, it is complementary to ISO 15189 standards, which are process based. As an increasing number of hospitals worldwide are seeking JCI accreditation, laboratories (including LMIC laboratories) might undergo on-site evaluation by the JCI during their hospital accreditation inspection.
The suitability of the latest version of SLIPTA to guide laboratories towards an ISO 15189:2012 accreditation was recently assessed by Datema et al.8 However, the readiness of SLIPTA five-star laboratories to undergo JCI accreditation is yet undetermined. The aim of this study was to evaluate the SLIPTA checklist's usefulness in assessing laboratories to meet JCI standards.
Methods
Ethical considerations
The local institutional review board (Human Research Protection Program at the American University of Beirut) deemed the study exempt from review. This study did not involve human or non-human participants and did not require participant consent or data protections.
Study design
This study was conducted at the College of American Pathologists accredited Department of Pathology and Laboratory Medicine at the American University of Beirut Medical Center, Lebanon. The American University of Beirut Medical Center is a JCI-accredited tertiary healthcare facility. The assessors (the manuscript's two authors) were selected based on their experience in the different accreditation processes and their certification as auditors for select certification bodies. The latest versions of SLIPTA (version 2:2015) and JCI standards for laboratories (3rd edition; January 2017) were retrieved from the World Health Organization Regional Office for Africa and JCI websites9,10,11.
Data analysis
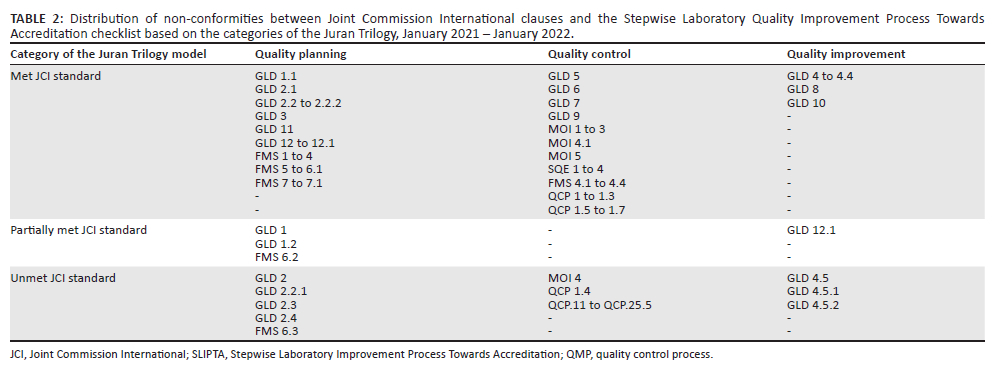
After thoroughly reviewing the JCI and SLIPTA standards, the authors performed a gap assessment separately between January 2021 and January 2022. First, each JCI clause was compared to its counterpart in the SLIPTA checklist and categorised as a 'met', 'partially met', or 'not met'. 'Met' JCI clauses were addressed and totally covered by the SLIPTA checklist, 'partially met' standards were addressed but not all elements were covered by the checklist, while 'not met' standards were not addressed. Percentages were calculated using a spreadsheet, Microsoft Excel (Microsoft, Redmond, Washington, United States). We then compared each author's results, discussed areas of discrepancies, and issued a unified consensual analysis. The JCI standards were divided into the three categories of the Juran Trilogy model (quality planning, quality control and quality improvement) as similarly done by Juran.12 The results of our scoring system were used to determine the categories with the highest percentage of gaps.
The SLIPTA comprises 12 sections, each corresponding to a single QMS element, which can be grouped into three categories: 'quality planning', 'quality control' and 'quality improvement', according to the Juran Trilogy model.12
The JCI booklet comprises three general divisions, 'accreditation participation requirements', 'patient-centred standards', and 'healthcare organisation management standards', subdivided into seven sections.
Of the 152 JCI standards, 109 were reviewed and compared to their counterparts in the SLIPTA checklist. Forty-three standards in Sections 1 and 7 of JCI were excluded from this review. Section 1 targets accreditation participation requirements. This section is specific to JCI and includes general principles such as the timely submission of accurate and complete data to the JCI committee. Section 1, including its 12 clauses, was excluded from the gap analysis due to lacking a counterpart. Section 7 includes standards covering speciality quality control process (QCP) (QCP. 2 - QCP. 10.1 and QCP. 26 - QCP. 27.5: 31 clauses), which details requirements for single laboratory speciality sections. Because SLIPTA views hospital laboratories as a single unit, it lacks speciality-specific questions, and the corresponding standards (20%; 31/152) were excluded from the analysis.
Results
The SLIPTA V2:2015 addresses 60% of the 109 JCI standards reviewed (56%; 61/109 wholly met and 4%; 4/109 partially met) but does not meet 40% (44/109) (Table 1). Among 'partially met' standards, 75% (3/4 standards) belong to the quality planning category and 25% (1/4) to quality improvement (Table 2). Among the 'not met' JCI clauses, 11% (5/44) are quality planning clauses, 82% belong to quality control (36/44) and 7% (3/44) to quality improvement.
Gaps were noted in standards related to the organisation's vision and mission statement, the accreditation of referral laboratories, ongoing communication with stakeholders, and quality monitoring. In terms of quality control, the validation of monitoring systems before implementation was also missing in the SLIPTA checklist.
SLIPTA checklist coverage of Joint Commission International standards
Joint Commission International Section 2: Patient safety goals
This section focuses on patient safety goals and includes correct patient identification, effective communication of critical results, and hand hygiene standards. Section 8 of the SLIPTA (process control) addresses all the requirements for preanalytical quality checks, including patient identification, sample collection and reception. The first section of the SLIPTA covers effective reporting of critical results, including adequate documentation and record keeping, while the facilities and biosafety section cover the hand hygiene standards. In addition, the SLIPTA standards require proper staff training on hand hygiene practices (section 3.6 d).
Joint Commission International Section 3: Healthcare organisation management
The JCI section 3 consists of healthcare organisation management standards, for which the initial step is the design of a leadership organisational chart and the determination of the laboratory's mission and vision. The SLIPTA checklist enquires about the presence of an organisational chart and a narrative description (section 3.2) of the different internal and external relationships within the laboratory. However, no points are assigned to developing a vision and mission statement. The following organisation management requirement is the appointment of a qualified laboratory manager, a clause fulfilled in the SLIPTA checklist. Despite the presence of a section in the SLIPTA checklist addressing client management and customer service, there is no requirement for a qualified individual to oversee these procedures. In the JCI, management is also responsible for service organisation and continuous communication with stakeholders; however, this is uncovered by the SLIPTA checklist. Resource planning is addressed in section 2.2 of the SLIPTA checklist as part of the output review by leadership.
The following section in JCI regulates the contracts and services with reference laboratories, namely the presence of standard operating procedures to define the process for selecting and approving contracts and services by the leadership (governance, leadership and direction [GLD] [GLD.2.2]), the need for proof of accreditation or certification (GLD.2.2.1), and performance monitoring (GLD.2.2.2). While the SLIPTA sets detailed requirements for the choice of referral laboratories and their continuous monitoring, along with the responsibility of the laboratory director in these tasks, it does not require checking the accreditation status of referral laboratories.
The SLIPTA checklist views the laboratory as a single unit rather than different laboratory speciality sections. Thus, unlike the JCI, it does not address standards for blood bank (GLD.2.3) and point-of-care services (GLD.2.4). Nevertheless, the SLIPTA standard 3.3, section 3, requires a laboratory director with adequate competency to supervise all laboratory workstations, which by extension includes blood bank and point-of-care services, as required by the JCI GLD.2.3 and GLD2.4.
In the JCI, GLD.3, 3.1 and 3.2 regulate effective inter- and intra-laboratory communication and efficient determination of clients' needs; these are also detailed in SLIPTA.
The next JCI section defines the different aspects of planning and coordination of a quality management programme, including the responsibilities of the leadership in developing the programme (GLD.4) and implementing activities (GLD.4.3), along with the required criteria for a well-functioning programme (GLD.4.1) and its monitoring by a qualified individual (GLD.4.2). The SLIPTA checklist conforms to the JCI requirements for quality management design. However, it does not completely cover quality management monitoring. For example, the JCI quality management monitoring the leadership to determining processes to be measured (GLD.4.5) and standards required to identify critical measures for clinical (GLD.4.5.1) and managerial (GLD4.5.2) structures, all of which SLIPTA does not address. In addition, the analysis of measurement data requires skilled individuals (GLD.5), an internal process to validate data (GLD.6) and an appropriate investigation of off-target trends (GLD.7). These criteria are met in the SLIPTA checklist sections 1.5, 6.1 and 11.1 that determine the need for effective auditing, including personnel, procedures, and trend verification tools.
The Joint Commission InternationalGLD.8 to 12.1 state principles for well-functioning safety and quality insurance programmes, including, but not limited to, the presence of an ongoing programme (GLD.9), and the responsibility of the leaders to create, implement (GLD.8), provide resources (GLD.11) and monitor ongoing programmes (GLD.10) while maintaining a safety culture throughout the laboratory (GLD.12 and GLD.12.1). Laboratories with a five-star SLIPTA accreditation are considered compliant with the safety and quality insurance programmes set by JCI.
Joint Commission International Section 4: Information management
Section 4 of the JCI focuses on information management. It states the need for the presence of written policies and procedures addressing all testing phases (preanalytical: [management of information {MOI}] MOI.1, 2, 2.1, 2.2; analytical: MOI.3; post-analytical: MOI.4) and storage (MOI.5), as well as their implementation (MOI.1.1). It also requires the definition of a turnaround time (MOI.4.1). The SLIPTA checklist requires the presence of written policies and procedures (section 1.2) and their implementation (section 1.2). Therefore, SLIPTA meets all standards for all testing phases (preanalytical: sections 1.5, 8.4; analytical: sections 1.5, 8.7; post-analytical: section 1.5), including setting turnaround time and storage requirements for records and specimens.
Joint Commission International Section 5: Staff qualifications and education
Section 5 standards are related to staff qualification and education. The first standard ([staff qualification and education {SQE}] SQE.1) mentions the role of laboratory leaders in defining the education and skills required for staff members, which is met by SLIPTA section 3.3 on the role of laboratory directors.
Section 3 of SLIPTA complies with the second standard in JCI Section 5, which discusses the training and experience required for supervisors and other leaders, licensure and registration of pathologists, and the need for defined responsibilities in the job descriptions.
The next JCI standard focuses on staff orientation, ongoing education, and yearly competency assessment needed to maintain and improve staff skills and knowledge (SQE.2, 2.1 and 3); the SLIPTA sections 3.3, 3.6, and 3.7 meet these requirements. Also, the SLIPTA section 3.5. mentions the JCI standard SQE.3.1 (maintenance of documented personnel information for every staff member) requirements. Finally, the last standard in this section requires the laboratory to provide health services to all staff (SQE.4) and is met by the SLIPTA checklist.
Joint Commission International Section 6: Facility management
Laboratory facility management constitutes the focus of Section 6. The first standard targets the responsibilities of laboratory leaders in providing the basic facilities and their facility's compliance with laws and regulations. This requirement is met by SLIPTA section 1.5 on accommodation and environmental conditions.
The next standards state the requirement for sufficient storage space ([facility management and safety {FMS}] FMS.2.1) and proper record keeping (FMS.2.2). Resources for this goal should be provided by the laboratory leadership (FMS.2). Storage requirements, record keeping, and leadership roles are covered by the SLIPTA sections 12.6, 1.5 (records control and sections) and 12.1.
The JCIstandards FMS.3 to 4.1.1 mention the different aspects for efficient and effective operation of all utility systems and equipment. These aspects include inspection, testing of critical operating components, maintenance, and availability of emergency backup for critical utilities. Interestingly, SLIPTA section 1.5 on laboratory equipment and section 5 on equipment give a more detailed description of proper equipment protocol due to the question format checklist.
The JCI standard FMS.4.2 on the requirement for a defined process for validating and maintaining computer software and laboratory information is met by SLIPTA sections 9.9 and 9.10.
The standards for periodic evaluation, labelling and documentation of reagents are met in SLIPTA sections 7.4 (inventory control) and 8.8 (reagents acceptance testing).
Finally, section 12 in SLIPTA (12.8-12.13) covers all safety aspects required by the last JCI section 6 standard on safety (FMS.5), including the management of hazardous materials, waste (FMS.6 to 6.3), and fire (FMS.7 and 7.1).
Joint Commission International Section 7: Quality control
The last JCI section deals with quality control (QC) standards for all testing areas. It includes establishing QC processes for the different test methods, external and internal QC, verification of results accuracy, and methods comparison. It also targets new instrument validation and instrument monitoring systems implementation. The QC processes are addressed through several SLIPTA sections with high compliance with JCI clauses. However, the SLIPTA checklist does not have questions on the validation of all monitoring systems before their implementation, as required by JCI.
Discussion
The level of compliance of SLIPTA with JCI requirements appears to be lower than its compliance with ISO 15189, as determined by Datema et al.8 This observation is because the SLIPTA checklist is primarily based on the ISO 15189 and the Clinical and Laboratory Standards Institute guideline QMS01-A4 clauses in 2009.9
The SLIPTA checklist and JCI standards are structured differently. In addition to its checklist format, SLIPTA is more detailed and extensive than JCI, with specific instructions. The structure difference is because of their respective perspectives and objectives. The SLIPTA checklist leans towards operations rather than management and targets laboratories with newly implemented QMS. On the other hand, the JCI accreditation standards are more outcome based than process based. They focus on the role of the laboratory leadership and management structure in achieving the desired quality outcomes, resource management, QC processes, the laboratory environment and development. The JCI thus targets healthcare organisations with a particular quality background to achieve higher excellence. The JCI booklet contains general standards addressing the laboratory as a single unit (similar to the SLIPTA checklist). This approach is important to cover essential laboratory QMS elements. In addition, requirements related to specific sections within the laboratory (blood bank, haematology, chemistry) are delineated. Quality managers of laboratories undergoing JCI evaluation might benefit from ensuring that section-specific requirements are met as they constitute up to 20% of JCI standards.
Our analysis also reveals that the SLIPTA quality planning and control sections contain the highest number of gaps when compared to JCI (Table 2). As an example, the definition of the organisation's mission and vision, which SLIPTA does not address, is crucial in the initial steps of the establishment of any QMS. Similarly, the role of leadership in service and resource planning and the implementation of culture safety should be emphasised in SLIPTA. Also, in the quality planning section, the safety programme should be improved in future versions, focusing on reducing infection risks and handling radioactive material.
Essential QC elements are missing in the SLIPTA checklist. The relationship with external (referral) laboratories should be regulated. Another important requirement for JCI is the validation of QC systems before their implementation. The post-analytical testing phase should receive special focus for the improvement of the next versions, with the appropriate policies, procedures, and controls. In terms of quality improvement, our analysis reveals a need for the improvement of the managerial decisions of improvement activities and the associated data collection for quality measurement to comply with JCI. However, the SLIPTA checklist is skewed towards quality planning and QC sections, with quality improvement having the lowest number of allocated points.8 Thus laboratories might focus on quality planning and QC clauses while neglecting quality improvement, which is a critical element in JCI accreditation.8
Limitations
This study reviewed the SLPITA and JCI checklists; thus, limitations are due to possible human errors during the review. Each of the manuscript's authors performed a full review independently to minimise errors.
Conclusion
This article encourages all laboratories in LMICs seeking a QMS programme to start by implementing SLIPTA, as per the World Health Organization Regional Office for Africa recommendations. Laboratories with high SLIPTA scores seeking JCI accreditation might benefit from addressing the following elements: selecting an accredited reference laboratory, collecting data for QM, creating post-analytical policies and procedures, and validating monitoring systems used in QC. Because gap analysis is the initial step of any accreditation transition process, this analysis constitutes a useful guide for laboratory quality managers and directors in LMICs planning to undergo the JCI accreditation process as part of their healthcare organisations.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
N.A, and A.K.E.K. performed data collection and analysis, N.A. and A.K.E.K. wrote the manuscript. N.A. and A.K.E.K. reviewed drafts and approved the final version of the manuscript.
Sources of support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data availability
Data supporting the findings of this study are available from the corresponding author, N.A., on request.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.Datema TA, Oskam L, Van Beers SM, Klatser PR. Critical review of the Stepwise Laboratory Improvement Process Towards Accreditation (SLIPTA): Suggestions for harmonisation, implementation and improvement. Trop Med Int Health. 2012;17(3):361-367. https://doi.org/10.1111/j.1365-3156.2011.02917.x [ Links ]
2.Nkengasong JN. Strengthening laboratory services and systems in resource-poor countries. Am J Clin Pathol. 2012;131(6):774. https://doi.org/10.1309/AJCP8GYX8KTKDATZ [ Links ]
3.Forsman RW. Why is the laboratory an afterthought for managed care organisations? Clin Chem. 1996;42(5):813-816. https://doi.org/10.1093/clinchem/42.5.813 [ Links ]
4.Centers for Medicare & Medicaid Services. Medicare and Medicaid statistical supplement [homepage on the Internet]. Baltimore: Centers for Medicare & Medicaid Services [cited 2022 Feb 03]. Available from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Archives/MMSS [ Links ]
5.International Organization for Standardization. ISO 15189:2012 Medical laboratories - Requirements for quality and competence [homepage on the Internet]. Geneva: International Organization for Standardization [cited 2022 Feb 03]. Available from: https://www.iso.org/standard/56115.html [ Links ]
6.Zima T. Accreditation of medical laboratories - System, process, benefits for labs. J Med Biochem. 2017;36(3):231-237. https://doi.org/10.1515/jomb-2017-0025 [ Links ]
7.Peter TF, Rotz PD, Blair DH, Khine AA, Freeman RR, Murtagh MM. Impact of laboratory accreditation on patient care and the health system. Am J Clin Pathol. 2010;134(4):550-555. https://doi.org/10.1309/AJCPH1SKQ1HNWGHF [ Links ]
8.Datema TAM, Oskam L, Broerse JEW, Klatser PR. Review of the Stepwise Laboratory Quality Improvement Process Towards Accreditation (SLIPTA) version 2:2015. Afr J Lab Med. 2020;9(1):1068. https://doi.org/10.4102/ajlm.v9i1.1068 [ Links ]
9.World Health organisation, WHO Regional Office for Africa. Stepwise Laboratory Quality Improvement Process Towards Accreditation (SLIPTA Checklist Version 2:2015 for Clinical and Public Health Laboratories) [homepage on the Internet]. [cited 2022 Feb 03]. Available from: https://apps.who.int/iris/bitstream/handle/10665/204423/slipta-checkist0711.pdf?sequence=1&isAllowed=y [ Links ]
10.African Society for Laboratory Medicine. SLIPTA audited laboratories distribution map [homepage on the Internet]. Ethiopia:. African Society for Laboratory Medicine. Addis Ababa. [cited 2022 Feb 03]. Available from: https://aslm.org/resource/slipta-map/ [ Links ]
11.Joint Commission International. Joint Commission International Accreditation standards for laboratories [homepage on the Internet]. Illinois: Joint Commission International. [cited 2022 Feb 03]. Available from: https://www.jointcommissioninternational.org/en/ [ Links ]
12.Juran JM. Juran on leadership for quality - An executive handbook. New York, NY: Collier Macmillan. [ Links ]
 Correspondence:
Correspondence:
Nada Assaf
na167@aub.edu.lb
Received: 28 July 2022
Accepted: 13 Dec. 2022
Published: 15 Mar. 2023


{kind=link}
{kind=link}