










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Laboratory Medicine
On-line version ISSN 2225-2010
Print version ISSN 2225-2002
Afr. J. Lab. Med. vol.9 n.1 Addis Ababa 2020
http://dx.doi.org/10.4102/ajlm.v9i1.854
BRIEF REPORT
Herpes simplex virus-2 infections in pregnant women from South Africa: Evaluation of the ImmunoFLOW rapid test
Shanthie GovenderI; Lungile MbamboI; Makandwe NyirendaII; Motshedisi SebitloaneIII; Nathlee AbbaiI
ISchool of Clinical Medicine Research Laboratory, Nelson Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IISouth African Medical Research Council, HIV Prevention Research, Durban, South Africa
IIIDepartment of Obstetrics and Gynecology, School of Clinical Medicine Research Laboratory, Nelson Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
The diagnostic performance of ImmunoFLOW, a rapid test for detecting herpes simplex virus type-2 (HSV-2) infections, was investigated in 248 antenatal women. Approximately one hundred and seventy-seven (71%) of the enrolled women were infected with HSV-2. Sero-positivity was associated with older age ([≥ 30 years] 104/177, 58%), having a secondary level of education but not tertiary level of education (125/177, 70.6%), and being unmarried (150/177, 84.7%). The sensitivity of the ImmunoFLOW test in relation to the HerpeSelect HSV-2 enzyme-linked immunosorbent assay was 89.7% and specificity was 96.2%. The ImmunoFLOW therefore can serve as a valuable test in screening for HSV-2 infections in pregnant women.
Keywords: HSV-2 infection; pregnant women; rapid test; South Africa.
Introduction
The South African HIV/AIDS and Sexually Transmitted Infections (STI) Strategic Plan deems the prevention and early treatment of STIs to be a major health priority for the country; emphasis has been placed on the delivery of quality services for testing and treating of STIs.1 Simple, rapid and affordable point-of-care tests for diagnosing STIs may be advantageous, because patients can be tested and treatment commenced in a single visit.2 Cassette- and strip-based point-of-care tests are highly applicable for use in resource-poor settings, because they do not require electricity, a laboratory or highly trained staff to perform the testing.3 Additionally, such tests could have tremendous potential for use in community clinics in an STI-endemic country such as South Africa.
In highly endemic herpes simplex virus type-2 (HSV-2) regions such as South Africa,4,5 routine screening for HSV-2 infections would pose a huge financial burden on the health system, because the only available diagnostic tests for HSV-2 are enzyme-linked immunosorbent assays (ELISA), which are expensive and time consuming. Due to the high turn-around time to receive test results, many infected individuals may be lost to follow up. In addition, ELISA requires the use of specialised equipment and highly trained laboratory staff. To address these limitations, rapid point-of-care tests that: are easy to operate, provide results on the same day and are relatively inexpensive would result in a larger number of testing and subsequent treatment infected individuals. The ImmunoFLOW HSV Test (GenBio, San Diego, California, United States) is a point-of-care cassette test that detects IgG to HSV gG-2 (specific HSV type 2 and total HSV [type 1 + type 2]) for type-specific classification, which is not possible using whole virus lysate, and also provides epidemiological information on these diseases. Currently, the diagnostic performance of this test has not been evaluated in a South African setting. Additionally, there is a lack of published research studies on this point-of-care test, both locally and globally.
This study compared the results of the ImmunoFLOW with the HerpeSelect HSV-2 ELISA (Focus Diagnostics, Cypress, California, United States). We used the HerpeSelect HSV-2 ELISA from Focus Diagnostics as our reference test, because this test has been approved by the manufacturer and has a certification mark approval (GmbH, Hannover, Germany) for detection of HSV antibodies in pregnant women globally.
Methods
Ethical considerations
The study and all study related materials were approved by the Biomedical Research Ethics Committee, University of KwaZulu-Natal (BE392/17).
Study setting and population
The study was conducted between April 2017 and August 2017 at the King Edward VIII Hospital antenatal clinic in Durban, KwaZulu-Natal, South Africa. Two hundred and forty-eight women participated in this study. During screening, an estimated 20% of the women approached refused study participation. The study criteria included: being pregnant and aged 18 years or older, willing to give written informed consent, willing to undergo a blood draw, and willing to allow the study team to document their HIV status from their clinic cards.
Data and specimen collection
For this study, data on the women's demographics and clinical information were recorded on a case report form. Women who had symptoms of genital ulcers and sores were treated by syndromic management. For the syndromic management approach, patients presenting with a genital ulcer or sore were treated with aciclovir, oral, 400 mg 8-hourly for 7 days.
Venous blood (3.5 mL) was collected by a hospital professional nurse. The blood was collected into a serum separator gel tube. The blood was processed and tested at University of KwaZulu-Natal, School of Clinical Medicine Research Laboratory.
ImmunoFLOW test
The samples were tested according to the manufacturer's instructions. Test cassettes were placed on a dry level surface, and 100 µL of wash solution was added to the cassette. The patient samples were diluted in sample diluent and thereafter 200 µL of the dilution was added to the cassette. A second wash step was conducted before the addition of 100 µL of Color G to the cassette. A final wash step was performed and the results were available within 2 min. Each cassette included a reagent-positive control. The presence of a red or pink dot in the individual test and control windows was read as a positive result.
HerpeSelect HSV-2 enzyme-linked immunosorbent assay
The HerpeSelect HSV-2 ELISA assay is a glycoprotein G-based type-specific ELISA technique which produces qualitative results. Two hundred ul of each serum sample was tested according to the manufacturer's recommendations (Focus Diagnostics, Cypress California, United States). Controls that were provided with kits were included for all runs: IgG High Positive Control (index value greater than 3.5); IgG Low Positive Control (index value between 1.5-3.5); and Negative Control (index value less than 0.8). The cut-off value used to determine a positive result was > 1.10 index value; 0.9-1.10 index values were considered equivocal and index values < 0.9 were considered as negative results. All samples that produced equivocal index values were re-tested.
Data analysis
All analyses were performed using STATA, version 14 (StataCorp LLC, College Station, Texas, United States). The diagnostic performance (i.e. sensitivity, specificity, positive predictive value, and negative predictive value) of the ImmunoFLOW test was compared to the gold standard HerpeSelect HSV-2 ELISA. A p-value of < 0.05 was considered as significant.
Results
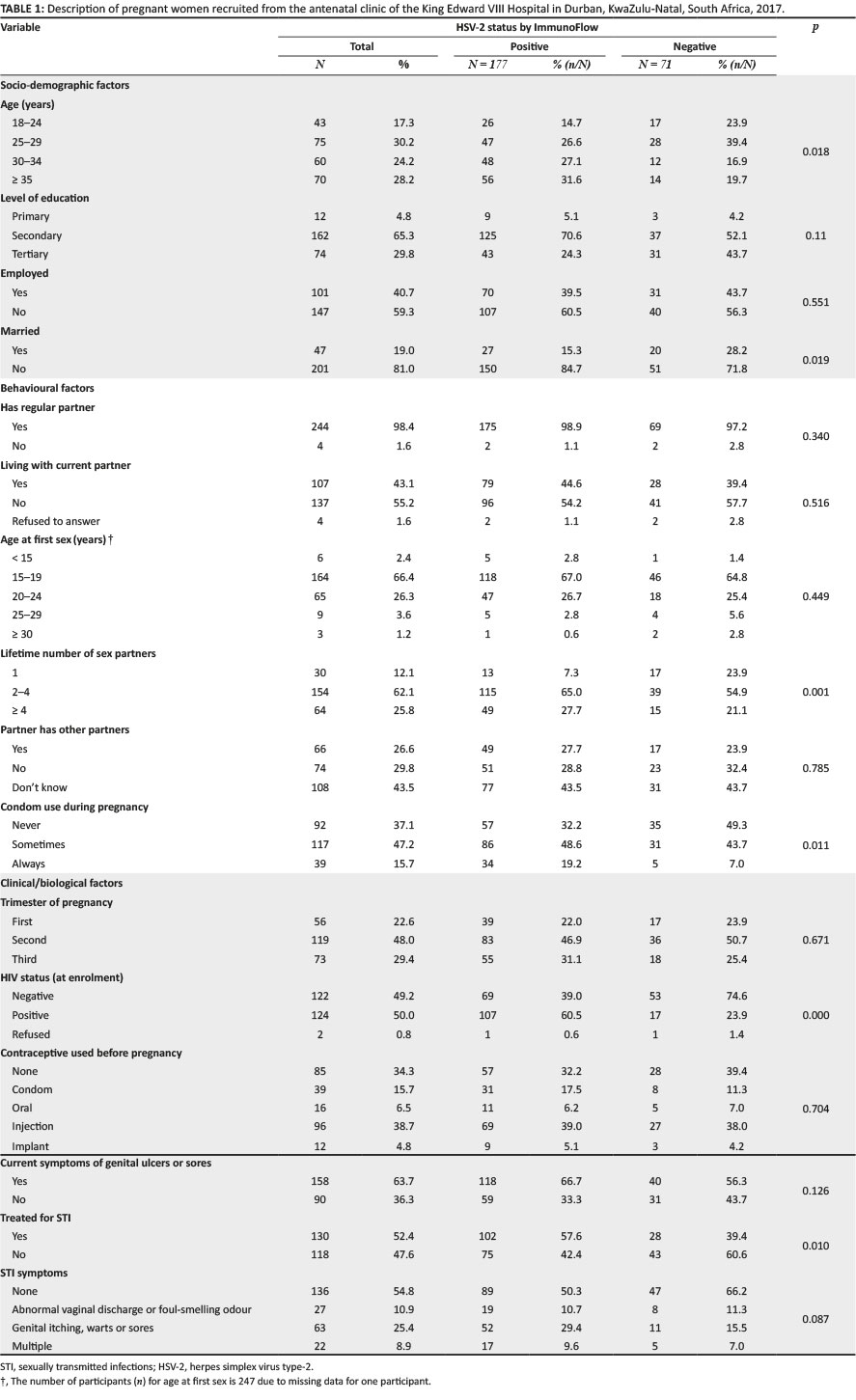
A prevalence of 177/248 (71.4%) for HSV-2 was observed on the ImmunoFLOW test and prevalence was 195/248 (78.6%) on the HerpeSelect HSV-2 ELISA. The prevalence of HIV in this population was 124/248 (50.0%). Approximately (107/177) of the women were positive for HSV-2 and were also HIV-positive. The majority of the women who tested positive for HSV-2 were older than age 30 years (104/177, 58%, p = 0.001), had completed secondary education but not tertiary education (125/177, 70.6%, p = 0.05), were unemployed (107/177, 60.5%, p = 0.55), were unmarried (150/177, 84.7%, p = 0.02) and reported having more than one lifetime sexual partners (164/177, 92.6%, p = 0.0002) (Table 1).
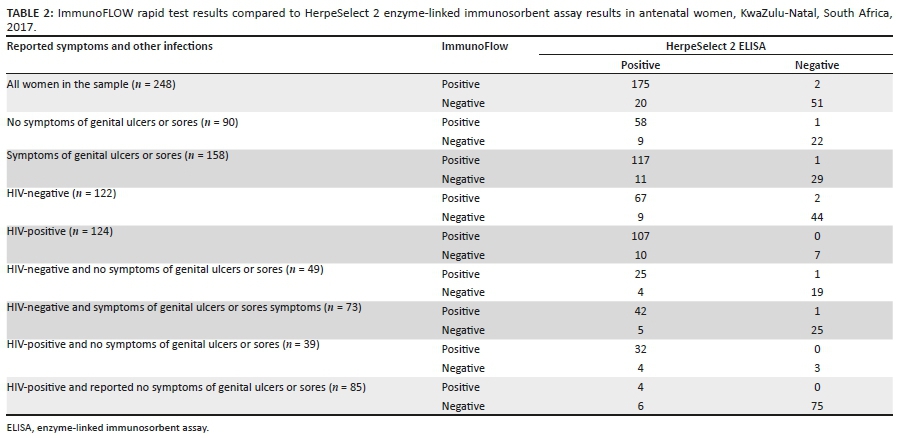
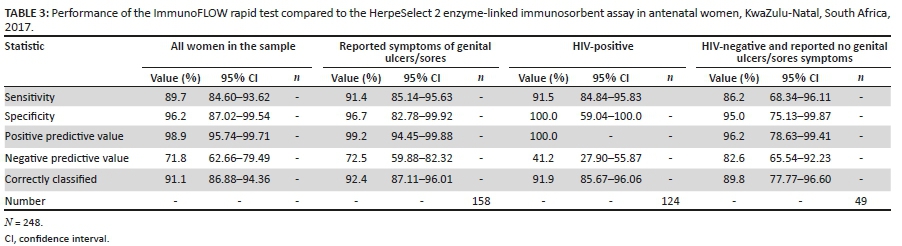
The sensitivity of the ImmunoFLOW test was 89.7% and its specificity was 96.2%. Of the 248 samples tested, 175 samples were correctly classified as positive by the ImmunoFLOW test. However, there were 2 samples that the ImmunoFLOW test classified as positive whereas the reference test classified these as negative. In addition, 20 samples were falsely classified as negative by the ImmunoFLOW (Table 2). The positive predictive value of the ImmunoFLOW was 98.9% and its negative predictive value was 71.8%. The overall predicitive accuracy of the ImmunoFLOW test was 91.1% (95% confidence interval: 86.9% - 94.4%) (Table 3).
Discussion
The 78.6% prevalence of HSV-2 reported in this study was found to be higher than other published studies on antenatal women.6,7,8,9,10 A high prevalence of HSV-2 was observed in women who had more partners, thereby emphasising the association between increased number of sex partners and risk of contracting STIs. The performance of the ImmunoFLOW was comparable to other published reports on HSV-2 rapid tests, which reported sensitivities and specificities > 90%.11,12,13,14,15 Other published studies on HSV-2 rapid tests have not reported on the performance of those tests in the presence of other viral infections, such as HIV, or genital symptoms relating to infection. In this study, the ImmunoFLOW rapid test performance was not shown to be negatively affected by HIV infection. The test yielded a sensitivity of 91.5% and specificity of 100% among HIV-positive women. In addition, the test was able to detect infection in women who were presenting with symptoms of genital ulcers or sores. Among women who were symptomatic, the sensitivity of the test was 91% and its specificity was 97%. This study highlights that having a test such as the ImmunoFLOW test could greatly contribute to early detection and treatment of women with herpes simplex viruses for improved outcomes for pregnant woman and their babies.
Limitations
The limitations of the study were as follows: Western blotting could not be performed as a second confirmatory test due to the high cost of the tests. The testing was performed at a research laboratory by medical technicians and is not a reflection of how the test would be performed at a clinic. Medical technicians are more experienced at laboratory procedures and quality checks. If the test had been conducted by a clinic nurse who has no laboratory experience, the results may have been different. This is yet to be confirmed. However, conducting evaluation studies at antenatal clinics will be a future research consideration. The test required the use of serum. With slight modifications, such as using blood collected by finger-prick instead of serum, this test could serve as a valuable test in screening for HSV-2 infections. However, this needs to be evaluated.
Conclusion
Overall, we have shown that the ImmunoFLOW rapid test performed well in relation to the ELISA. Rapid laboratory tests for diagnosis of STIs will directly contribute to United Nations Sustainable Development Goals that focus on improvement in health.16
Acknowledgements
We gratefully acknowledge the contribution of the women who participated in this study.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship or publication of this article.
Authors' contributions
N.A. designed and funded the study. M.N. performed all the statistical analysis. S.G. and L.M. performed all the laboratory testing and analysis. M.S. provided clinical assistance. All authors contributed to the writing of the final manuscript.
Sources of support
We thank the National Research Foundation of South Africa for funding this study.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.Lewis DA, Maruma E. Revision of the national guideline for first-line comprehensive management and control of sexually transmitted infections: What's new and why? South Afr J Epidemiol Infect. 2009;24(2):6-9. https://doi.org/10.1080/10158782.2009.11441341 [ Links ]
2.Hsieh Y-H, Hogan MT, Barnes M, et al. Perceptions of an ideal point-of-care test for sexually transmitted infections-A qualitative study of focus group discussions with medical providers. PLoS One. 2010;5(11):e14144. https://doi.org/10.1371/journal.pone.0014144 [ Links ]
3.Tucker JD, Bien CH, Peeling RW. Point-of-care testing for sexually transmitted infections: Recent advances and implications for disease control. Curr Opin Infect Dis. 2013;26(1):73. https://doi.org/10.1097/QCO.0b013e32835c21b0 [ Links ]
4.Abbai NS, Wand H, Ramjee G. Socio-demographic and behavioural characteristics associated with HSV-2 sero-prevalence in high risk women in KwaZulu-Natal. BMC Rese Note. 2015;8(1):1. https://doi.org/10.1186/s13104-015-1093-0 [ Links ]
5.Kenyon C, Colebunders R, Buve A, Hens N. Partner-concurrency associated with herpes simplex virus 2 infection in young South Africans. Int J STD AIDS. 2013;24(10):804-812. https://doi.org/10.1177/0956462413482810 [ Links ]
6.Lima L, Padalecki G, Castro C, Cordeiro J, De Paula V. Seroprevalence of human herpesvirus type 2 in a reference center for pregnant women in Rio de Janeiro, Brazil. VRR. 2017;22:20-21. https://doi.org/10.17525/vrrjournal.v22i1.327 [ Links ]
7.Domercant JW, Louis FJ, Hulland E, et al. Seroprevalence of Herpes Simplex Virus type-2 (HSV-2) among pregnant women who participated in a national HIV surveillance activity in Haiti. BMC Infect Dis. 2017;17(1):577. https://doi.org/10.1186/s12879-017-2674-4 [ Links ]
8.Anjulo AA, Abebe T, Hailemichael F, Mihret A. Seroprevalence and risk factors of herpes simplex virus-2 among pregnant women attending antenatal care at health facilities in Wolaita zone, Ethiopia. Virol J. 2016;13(1):43. https://doi.org/10.1186/s12985-016-0501-y [ Links ]
9.Nakubulwa S, Kaye DK, Bwanga F, Tumwesigye NM, Nakku-Joloba E, Mirembe FM. Incidence and risk factors for herpes simplex virus type 2 seroconversion among pregnant women in Uganda: A prospective study. J Infect Dev Countr. 2016;10(10):1108-1115. https://doi.org/10.3855/jidc.6874 [ Links ]
10.Perti T, Nyati M, Gray G, et al. Frequent genital HSV-2 shedding among women during labor in Soweto, South Africa. Infect Dis Obstet Gynecol. 2014;2014:Article ID 258291:8 pages. https://doi.org/10.1155/2014/258291 [ Links ]
11.Ashley RL, Eagleton M, Pfeiffer N. Ability of a rapid serology test to detect seroconversion to herpes simplex virus type 2 glycoprotein G soon after infection. JCM. 1999;37(5):1632-1633. https://doi.org/10.1128/JCM.37.5.1632-1633.1999 [ Links ]
12.Wald A, Ashley-Morrow R. Serological testing for Herpes Simplex Virus (HSV)-1 and HSV-2 infection. Clin Infect Dis. 2002;35(2):S173-S182. https://doi.org/10.1086/342104 [ Links ]
13.Philip SS, Ahrens K, Shayevich C, et al. Evaluation of a new point-of-care serologic assay for herpes simplex virus type 2 infection. Clin Infect Dis. 2008;47(10):e79-e82. https://doi.org/10.1086/592696 [ Links ]
14.Laderman EI, Whitworth E, Dumaual E, et al. Rapid, sensitive, and specific lateral-flow immunochromatographic point-of-care device for detection of herpes simplex virus type 2-specific immunoglobulin G antibodies in serum and whole blood. CVI. 2008;15(1):159-163. https://doi.org/10.1128/CVI.00218-07 [ Links ]
15.Shevlin E, Morrow RA. Comparative performance of the Uni-Gold™ HSV-2 Rapid: A point-of-care HSV-2 diagnostic test in unselected sera from a reference laboratory. J Clin Virol. 2014;61(3):378-381. https://doi.org/10.1016/j.jcv.2014.08.012 [ Links ]
16.United Nations General Assembly. Sustainable devlopment goals [homepage on the Internet]. 2015 [cited 2018 Jun 27]. Available from: https://www.un.org/sustainabledevelopment/sustainable-development-goals/ [ Links ]
 Correspondence:
Correspondence:
Nathlee Abbai
abbain@ukzn.ac.za
Received: 27 June 2018
Accepted: 17 Apr. 2020
Published: 31 Aug. 2020


{kind=link}
{kind=link}
{kind=link}