










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Laboratory Medicine
versión On-line ISSN 2225-2010
versión impresa ISSN 2225-2002
Afr. J. Lab. Med. vol.9 no.1 Addis Ababa 2020
http://dx.doi.org/10.4102/ajlm.v9i1.939
ORIGINAL RESEARCH
Kaposi's sarcoma-associated herpesvirus protein ORF75 among HIV-1 patients in Kenya
Rodgers N. DembaI, II; Sylviah M. AradiIII; Matilu MwauIV; Walter O. MwandaII
ISchool of Health Sciences, Kisii University, Kisii, Kenya
IIInstitute of Tropical and Infectious Diseases, University of Nairobi, Nairobi, Kenya
IIIDepartment of Internal Medicine, University of Nairobi, Nairobi, Kenya
IVCenter for Infectious and Parasitic Diseases Control Research, Kenya Medical Research Institute, Busia, Kenya
ABSTRACT
BACKGROUND: Histology is used to identify Kaposi's sarcoma (KS) in countries with low resources to fund healthcare costs. Approximately 95% of KS cases can be detected using a polymerase chain reaction.
OBJECTIVE: To determine the presence of the open reading frame 75 (ORF75) gene associated with Kaposi's sarcoma herpes virus among HIV-1/AIDS patients and to describe morphological presentations of KS.
METHODS: This was a retrospective, descriptive study of archived tissue blocks collected from 2013 to 2016. Haematoxylin and eosin staining was used to identify KS. Deoxyribonucleic acid from archived tissue blocks was extracted and a nested polymerase chain reaction was used to detect the ORF75 gene.
RESULTS: All 81 cases in this study had been diagnosed as HIV-1 positive, of which 68 had hallmark features of KS in the histology report and 13 had features suggestive of KS ('KS-like'). Microscopic identification of KS by haematoxylin and eosin staining was considered a significant indicator of KS herpes virus ORF75 gene positivity (p = 0.002). The ORF75 gene was detected in 60.5% (49/81) of tissue blocks; 27.2% were men (22/81) and 33.3% were women (27/81). The ORF75 gene was observed to be present in up to 15.4% (2/13) of the cases reported to have KS-like features.
CONCLUSION: Following the initial diagnosis of KS by histology, the ORF75 gene was fur-ther detected from both cases that had hallmark features of KS as well as among cases with KS-like features.
Keywords: Human herpes virus 8; Kaposi's sarcoma; histology; nested PCR; ORF75 gene.
Introduction
Kaposi sarcoma (KS) is a tumor formed from blood vessels; it later shows lesions on the skin or organs of HIV-positive people.1 All forms of KS are caused by Kaposi's sarcoma herpesvirus (KSHV), also known as human herpesvirus 8 (HHV-8).2,3 The genome of HHV-8 contains a minimum of 100 open reading frames (ORF), of which 4 to 75 are known to be unique to herpesvirus.4 The KSHV genome encodes more than 84 proteins that play a role in viral replication and host-virus interaction.5 The replication cycle of KSHV entails latent and lytic phases. During the lytic cycle, the ORF75 genes are expressed resulting in the manifestation of KS.6,7 The ORF75 gene product has been proven to aid in lytic replication and enhancement of virus pathogenesis in host cells.8
Kaposi's sarcoma is listed among the defining malignancies of HIV/AIDS.9,10,11 The dis-tinct feature of HIV-associated KS is that it might affect the lymph nodes, gastrointestinal tract, lungs or liv-er.12,13 Despite the fact that saliva is the main route by which KSHV is transmitted,14 HHV-8 has been isolated from other body fluids.14,15,16 The main route of HHV-8 transmission to the opposite sex is through sexual relations.17 The pathogenesis of KS presents as an abnormal neoangiogenesis, proliferation of cancer cells and inflammation of endothelial cells.18 A classic KS lesion manifests various features ranging from maculopapular to nodular or plaque-like and, in most cases, is pain-less.12,19,20,21
In sub-Saharan Africa, KSHV is endemic and approximately 84% of worldwide cases of KS occur in this region.22 Since KS is common among HIV/AIDS pa-tients,13 early detection of KSHV is essential in disease monitoring.22 The sensitivity of diagnostic tests for detection of KSHV depends on the sample selected for analysis.23 For example, biopsies obtained from patients with HIV/AIDS-KS were found to yield better results compared to using peripheral blood mononuclear cells from the same patient.23 Identification of KS in tissue biopsies by use of histological staining techniques should not be underestimated.24 In tissue biopsies, microscopic examination involves identification of proliferated spindle cells and oedema.25 Clinical diagnoses of KS have been shown to have limited predictive value.26 The use of molecular techniques such as polymerase chain reaction (PCR) permits the detection of the HHV-8 gene even for patients who present with early vascular lesions that histological techniques might miss.27 The use of PCR in the diagnosis of KS can detect approximately 95% of cases.28 The HHV-8 DNA has been successfully amplified using nested PCR previously.29,30 This study was aimed at determining the presence of the ORF75 gene linked to KSHV among HIV-1/AIDS patients. In addition, the objective of this current study was to describe the morphological presentations of KS among the studied cases.
Methods
The present study only included patients aged 18 years and older. Data on clinical information that was useful for this study were extracted from the registry records with the help of the data clerk. The following data were obtained from the registry records: sex, age, HIV-1 status, if patient was on antiretroviral or Highly Active Antiretroviral Therapy treatment, anatomic location of KS lesions, number of KS lesions, distribution of KS lesions, cluster of differentiation 4 cell count and histology diagnosis.
Ethical considerations
Study approval number P682/11/2014 was assigned by Kenyatta National Hospital/University of Nairobi Ethics and Research Committee.
Study design
A cross-sectional, descriptive, hospital-based study was used. Formalin-fixed, paraffin-embedded tissue blocks were retrieved from archives following histological reports of the patients who were diagnosed with KS or KS-like disease between 2013 and 2016. A consecutive sampling technique was used to select the archived tissue blocks from Thematic Unit of Anatomic Pathology, Department of Human Pathology, College of Health Sciences, University of Nairobi, and Department of Laboratory Medicine, Cytology Section, Kenyatta National Hospital.
For this study, a total of 81 tissue blocks were selected and analysed. A rotary microtome was used to section the formalin-fixed, paraffin-embedded blocks. A different blade was used for every formalin-fixed, paraffin-embedded block so as to avoid carry-over of genetic material. Once a block was cut, the microtomes surface was decontaminated using DNAZapTM PCR DNA degradation solution (catalog number: AM9890; Thermo Fisher Scientific, Waltham, Massachusetts, United States). Each tissue section was cut to 10 µm thick. The tissue sections were processed for haematoxylin and eosin staining and a qualified pathologist reported on the results.
Deoxyribonucleic acid extraction and polymerase chain reaction
Isolation of DNA from tissue sections was done using a GeneRead DNA FFPE kit (Qiagen, Hilden, Germany). The extraction kit removes paraffin and reverses formalin cross-links from tissue before DNA is bound to the QIAampMinElute column (Qiagen, Hilden, Germany). The eluted DNA is then ready to be used for nested PCR to detect the ORF75 gene in HHV-8. A Taq PCR Core Kit (catalog number: 201223; Qiagen, Hilden, Germany) was used to detect the ORF75 gene. The set of primers used were; ORF75 product size 895 bp Forward KS 1000 5′CGGTTCGGTGGCATACAGGC3′; Reverse KS 1034 5′CTGACTACAGAGGGTGTCCCCG3′.31 ORF75 product size 804 bp Forward KS 2000 5′GGAAACAGGGTGCTGTG3′; Reverse KS 2034 5′CATGGCCTACGACGTCAC3′.32 The cycling conditions of the PCR for the targeted KS regions were similar and consisted of 30 cycles of: initial denaturation at 94 °C for 3 minutes, denaturation at 94 °C for 1 min, annealing at 63 °C for 1 min, extension at 72 °C for 1 min and final extension at 72 °C for 10 min. Amplified PCR products were analysed by electrophoresis on a 1% agarose gel containing ethidium bromide (1 µL/mL of agarose solution) and were visualised under ultraviolet light alongside a 1 Kilobase (Kb) deoxyribonucleic acid (DNA) ladder. For a positive control, a known case of KS was used. The ribonuclease-free water was used as a negative control.
Statistical analysis
The data were analysed using Statistical Package for Social Sciences version 21 (SPSS Inc Binghamton, New York, United States); the relationship between the ORF75 gene and clinical characteristics were tested by using chi-square and t-tests. A p-value of less than 0.05 was considered to be statistically significant. Odds ratios in a cross-sectional study are known as prevalence odds ratios and were used as a measure of association.33
Results
Of the 81 tissue samples included in the study, 43.2% (35/81) were from women and 56.8% (46/81) were from men (Table 1). All of the 81 cases studied had been diagnosed with HIV-1 implying that they were living with the virus. In addition, it was observed that none of the cases had a cluster of differentiation 4 cell count above 350 cells/mm3. Among the 81 cases, the ORF75 gene was detected in 49 cases (60.5%); 27.2% (22/81) were women and 33.3% (27/81) were men. Among cases positive for the ORF75 gene, 4.1% (2/49) were never on any form of antiretroviral therapy and 95.9% (47/49) were on antiretroviral therapy. No statistically significant association was found between the presence of the ORF75 gene and sex, antiretroviral treatment status, number of KS lesions or distribution of the KS lesions (all p-values > 0.05).
Age
The mean age of patients with tissue blocks positive for the ORF75 gene was 41 years (standard deviation = 9.2; maximum age, 66 years; minimum age, 19 years). Detection of the ORF75 gene was most common in the 30-39 years age group (n = 21; 42.9%). Age had a statistically significant association with ORF75 gene positivity (prevalence odds ratio: 1.05; 95% confidence interval: 1.00-1.11, P = 0.047).
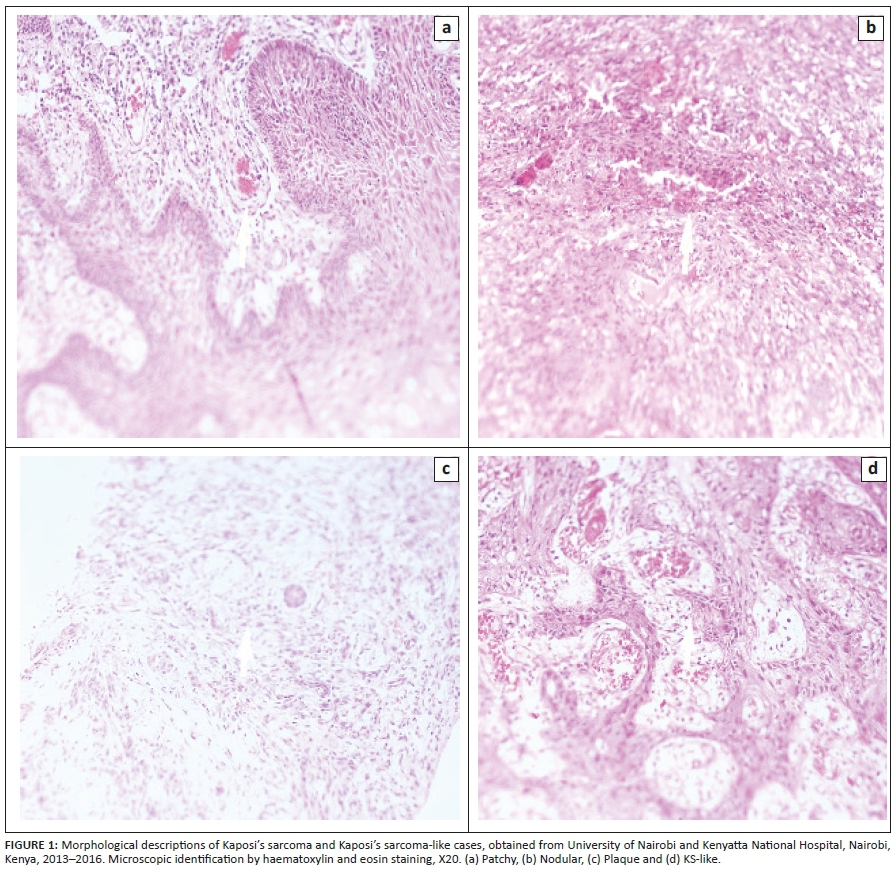
Kaposi sarcoma morphology and distribution of lesions
In the histology report, 68 cases had hallmark features of KS, whereas 13 cases had features suggestive of KS (KS-like). The types of KS morphology identified included patchy, nodular, plaque and KS-like (Figure 1). The morphological distribution of KS was as follows: 61.7% (50/81) was nodular, 16% (13/81) was patchy, and 22% (18/81) were plaques. Among the cases that were positive for the ORF75 gene, 75.51% (37/49) was nodular, 4.08% (2/49) patchy, and 20.41% (10/49) were plaques.
The total number of KS cases diagnosed by histology was 68 (84%) and 13 cases (16%) had KS-like features (Table 1). Among the 49 cases with the ORF75 gene, 47 (95.9%) showed hallmark features of KS and 2 (4.1%) had KS-like features with microscopic examination. There was an association between microscopic identification of KS by histology and the presence of the ORF75 gene (prevalence odds ratio = 12.3; 95% confidence interval = 12.51 - 60.49; P = 0.002) (Table 1).
The amplified ORF75 genes of HHV-8 were identified by 1% agarose gel electrophoresis (Figure 2).

Discussion
Retrieved clinical data revealed that all of the tissue blocks retrieved in the present study were collected from patients who had been diagnosed with HIV-1. These patients might have developed KS lesions due to immunosup-pression or because they were immunocomprised due to increased viral load that impaired their immune system. Other studies have also associated KS as an HIV/AIDS-defining illness.9,13,24,34,35,36
The findings of this study revealed that men were more prone to development of KS: 56.8% (46/81) compared with women 43.2% (35/81). This observation is concordant with others who also noted more frequent development of KS among men.37,38,39,40 There is a lack of consensus as to why all forms of KS are more common among men than women.41,42 We hypothesise that gender-related factors such as hormones might influence the development of KS lesions. The results of this study showing KS pre-ponderance among men was consistent with the country's published data on the distribution of malignancy cases as captured in the National Cancer Control strategy, 2017.43
Kaposi's sarcoma immune reconstitution occurs when a portion of AIDS-KS cases responds to the introduction of combined antiretroviral therapy with disease advancement.44,45,46 In this study, KS lesions manifested among patients despite the fact that 77 (95.1%) were on antiretroviral treat-ment. Contrary to other findings that antiretroviral therapy alone can result in the resolution of KS,47,48 in our study, being on antiretroviral treatment did not have a statistically significant association with the presence of KS (P = 0.66). This finding is in agreement with another study that stated that there has been continued diagnosis of KS in HIV-positive patients, despite the availability of highly active antiretroviral therapy.49 Other studies have stated that patients infected with AIDS-associated KS respond to combined antiretroviral therapy by 50% depending on geographical location and severity of the presentation, thereby resulting in immune reconstitution and HIV suppression.50,51,52 In the current study, these manifestations of KS could be attributed to the weakening of the immune system by HIV-1.
This study found patchy, plaque and nodular morphological presentations of KS. The morphological appearance of KS shows progression from plaques to nodular form and fungiform.1 Kaposi sarcoma lesions are known to progress from asymptomatic to macule, papule, plaque and nodule forms.53 The findings of this study revealed that the KS lesions were disseminated in different body regions, including the lower limbs, upper limbs, genitalia, eyelids, palate, oral cavity and trunk (chest and back). In another study, fatality was witnessed in HIV-positive patients who had KS lesions manifested in the gastrointestinal tract, lungs and lymph nodes.54
The decision in this study to use tissue biopsy for detection of the ORF75 gene of HHV-8 is in agreement with another study that supported the use of tumor biopsies as suitable for viral DNA identification due to high viral load as opposed to the use of blood.30 Further to that, nested PCR has been used successfully to assess the prevalence of HHV-8 among HIV-positive patients in Brazil.27 A tissue biopsy excised from a KS lesion has been shown to have high viral load; hence, biopsies are the ideal sample for the detection of KSHV DNA.55 The detection of the ORF75 gene implies that this gene was present in 49 (60.5%) of the studied cases.
Strength and limitations
Our study used the haematoxylin and eosin staining technique and the nested PCR method for detection of the ORF75 genes of the KSHV. However, HHV-8 immunohistochemical biopsy has been demonstrated to be the 'gold standard' for KS diagnosis.56 Cases in the present study had a dark skin pigmentation. In another study of dark-skinned patients, KS had been confirmed to mimic a number of non-KS-like dermatological conditions.56 In another study, it was observed that it is difficult to identify KS in dark-skinned individuals, who presented with violaceous skin lesions.56
The use of the PCR technique in the detection of KSHV has been shown to give the utmost specificity compared to the use of tests that determine exposure to infection.28 In addition, the PCR technique can detect approximately 95% of all KS cases.28 However, the cost associated with the use of PCR is quite high, which would limit the clinical application of HHV-8 DNA detection in resource-limited facili-ties.28
Implications and recommendations
The present study considered microscopic detection of KS by haematoxylin and eosin as a significant indicator of KSHV ORF75 gene positivity. It therefore recommends the use of both clinical diagnosis and routine microscopy in the diagnosis of KS in resource-limited facilities. However, among individuals with dark skin pigmentation, there is the need to employ the use of a robust diagnostic technique to ascertain the true causative agent.
Conclusion
The presence of the ORF75 gene of KSHV among immunosuppressed patients due to HIV-1 was successfully detected. Following the initial diagnosis of KS by histology, the ORF75 gene was further detected from both cases that had the hallmark features KS and those that had KS-like features. Microscopic detection of KS by haematoxylin and eosin should be considered a significant indicator of KSHV ORF75 gene positivity.
Acknowledgements
The authors of this manuscript would like to extend their gratitude to Kenyatta National Hospital and University of Nairobi for allowing them to use their archived tissue blocks.
Competing interests
The authors declare no conflict of interest.
Authors' contributions
R.N.D., S.M.A., M.M. and W.O.M. critically revised the manuscript for important intellectual content. R.N.D., S.M.A. and W.O.M. drafted the manuscript. R.N.D. and W.O.M. conceptualised and designed the study and ana-lysed and interpreted the data. R.N.D. and S.M.A. acquired the data.
Sources of support
This study was funded by the principal investigator (R.N.D.) as a fulfilment for the award of a postgraduate de-gree.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the offi-cial policy or position of any affiliated agency of the authors.
References
1.Warpe BM, Kaposi sarcoma as initial presentation of HIV infection. N Am J Med Sci. 2014;6(12):650. https://doi.org/10.4103/1947-2714.147984 [ Links ]
2.Betsem E, Cassar O, Afonso PV, et al. Epidemiology and genetic variability of HHV-8/KSHV in Pygmy and Bantu populations in Cameroon. PLoS Negl Trop Dis. 2014;15;8(5):e2851. https://doi.org/10.1371/journal.pntd.0002851 [ Links ]
3.Coen N, Duraffour S, Snoeck R, et al. KSHV targeted therapy: An update on inhibitors of viral lytic replication. Viruses. 2014;6(11):4731-459. https://doi.org/10.3390/v6114731 [ Links ]
4.Raab-Traub N. Novel mechanisms of EBV-induced oncogenesis. Curr Opin Virol. 2012;2(4):453-458. https://doi.org/10.1016/j.coviro.2012.07.001 [ Links ]
5.Dittmer DP, Damania B. Kaposi sarcoma associated herpesvirus pathogenesis (KSHV) - An update. Curr Opin Virol. 2013;1;3(3):238-244. https://doi.org/10.1016/j.coviro.2013.05.012 [ Links ]
6.Thomas S, Sindhu CB, Sreekumar S, et al. AIDS associated Kaposi's sarcoma. J Assoc Phys India [serial online]. 2011;59:387-389. Available from: https://europepmc.org/abstract/med/21751599 [ Links ]
7.Ye F, Lei X, Gao SJ. Mechanisms of Kaposi's sarcoma-associated herpesvirus latency and reactiva-tion. Adv Virol. 2011;2011. https://doi.org/10.1155/2011/193860 [ Links ]
8.Van Skike ND, Minkah NK, Hogan CH, et al. Viral FGARAT ORF75A promotes early events in lytic infection and gammaherpesvirus pathogenesis in mice. PLoS Pathog. 2018;14(2):e1006843. https://doi.org/10.1371/journal.ppat.1006843 [ Links ]
9.Stolka K, Ndom P, Hemingway-Foday J, et al. Risk factors for Kaposi's sarcoma among HIV-positive individuals in a case control study in Cameroon. Cancer Epidemiol. 2014;38(2):137-143. https://doi.org/10.1016/j.canep.2014.02.006 [ Links ]
10.Rohner E, Wyss N, Heg Z, et al HIV and human herpesvirus 8 co-infection across the globe: Systematic review and meta-analysis. Int J Cancer. 2016;138(1):45-54. https://doi.org/10.1002/ijc.29687 [ Links ]
11.Fang Q, Liu Z, Zhang Z, Zeng Y, Zhang T. Prevalence of Kaposi's sarcoma-associated herpesvirus among intravenous drug users: A systematic review and meta-analysis. Virol Sin. 2017;32(5):415-422. https://doi.org/10.1007/s12250-017-4051-2 [ Links ]
12.La Ferla L, Pinzone MR, Nunnari G, et al. Kaposi's sarcoma in HIV-positive patients: The state of art in the HAART-era. Eur Rev Med Pharmacol Sci [serial online]. 2013;17(17):2354-2365. Available from: https://www.researchgate.net//links/02e7e53537273f30c7000000.pdf [ Links ]
13.Hoffmann C, Sabranski M, Esser S. HIV-associated Kaposi's sarcoma. Oncol Res Treat. 2017;40(3):94-98. https://doi.org/10.1159/issn.2296-5270 [ Links ]
14.Minhas V, Wood C. Epidemiology and transmission of Kaposi's sarcoma-associated herpesvirus. Viruses. 2014;6(11):4178-4194. https://doi.org/10.3390/v6114178 [ Links ]
15.Ganem D. KSHV and the pathogenesis of Kaposi sarcoma: Listening to human biology and medicine. J Clin Invest. 2010;120(4):939-949. https://doi.org/10.1172/JCI40567 [ Links ]
16.Sathish N, Yuan Y. Evasion and subversion of interferon-mediated antiviral immunity by Kaposi's sarcoma-associated herpesvirus: An overview. J Virol. 2011;85(21):10934-10944. https://doi.org/10.1128/JVI.00687-11 [ Links ]
17.Shebl FM, Dollard SC, Pfeiffer RM, et al. Human herpesvirus 8 seropositivity among sexually active adults in Uganda. PLoS One. 2011;6(6):e21286. https://doi.org/10.1371/journal.pone.0021286 [ Links ]
18.Cancian L, Hansen A, Boshoff C. Cellular origin of Kaposi's sarcoma and Kaposi's sar-coma-associated herpesvirus-induced cell reprogramming. Trends Cell Biol. 2013;23(9):421-432. https://doi.org/10.1016/j.tcb.2013.04.001 [ Links ]
19.Curtiss P, Strazzulla LC, Friedman-Kien AE. An update on Kaposi's sarcoma: Epidemiology, patho-genesis and treatment. Dermatol Ther. 2016;6(4):465-470. https://doi.org/10.1007/s13555-016-0152-3 [ Links ]
20.El-Mallawany NK, Kamiyango W, Slone JS, et al. Clinical factors associated with long-term complete remis-sion versus poor response to chemotherapy in HIV-infected children and adolescents with Kaposi sarcoma receiving bleomycin and vincristine: A retrospective observational study. PLoS One. 2016;11(4):e0153335. https://doi.org/10.1371/journal.pone.0153335 [ Links ]
21.Stefan DC. Patterns of distribution of childhood cancer in Africa. J Trop Pediatr. 2015;61(3):165-173. https://doi.org/10.1093/tropej/fmv005 [ Links ]
22.Olp LN, Shea DM, White MK, Gondwe C, Kankasa C, Wood C. Early childhood infection of Kaposi's sarcoma-associated herpesvirus in Zambian households: A molecular analysis. Int J Cancer. 2013;1;132(5):1182-1190. https://doi.org/10.1002/ijc.27729 [ Links ]
23.Oetvoes R, Juhasz A, Szalai E, et al. Molecular typing of human herpesvirus 8 isolates from patients with Kaposi's sarcoma in Hungary. Anticancer Res [serial online]. 2014;34(2):893-898. Available from: http://ar.iiarjournals.org/content/34/2/893.short [ Links ]
24.Johann WS, Dirk PD. Diagnosis and treatment of Kaposi Sarcoma. Am J Clin Dermatol. 2017;18(4):529-539. https://doi.org/10.1007/s40257-017-0270-4 [ Links ]
25.Kumar P, Kuwa NY, Minhas V, et al. Higher levels of neutralizing antibodies against KSHV in KS patients compared to asymptomatic individuals from Zambia. PLoS One. 2013;14;8(8):e71254. https://doi.org/10.1371/journal.pone.0071254 [ Links ]
26.Amerson E, Woodruff CM, Forrestel A, et al. Accuracy of clinical suspicion and pathologic diagnosis of Kaposi sarcoma in East Africa. J Acquir Immune Defic Syndr. 2016;71(3):295-301. https://doi.org/10.1097/QAI.0000000000000862 [ Links ]
27.Machado PR, Farias KJ, Pereira MG, Freitas PP, Fonseca BA. Human herpesvirus 8 (HHV-8) detected by nested polymerase chain reaction (PCR) in HIV patients with or without Kaposi's sarcoma. An analytic cross-sectional study. Sao Paulo Med J. 2016;134(3):187-192. https://doi.org/10.1590/1516-3180.2014.8973010 [ Links ]
28.Crabtree KL. The epidemiology of Human Herpesvirus-8: Transmission of infection to children in Zambian households [homepage on the Internet]. 2013 [cited 2013 Dec 7];(12) Available from: https://digitalcommons.unl.edu/bioscidiss/53/ [ Links ]
29.Jalilvand S, Tornesello ML, Buonaguro FM, et al. Molecular epidemiology of human herpesvirus 8 variants in Kaposi's sarcoma from Iranian patients. Virus Res. 2012;163(2):644-649. https://doi.org/10.1016/j.virusres.2011.09.027 [ Links ]
30.Kourí V, Martínez PA, Capo V, et al. Kaposi's Sarcoma and Human Herpesvirus 8 in Cuba: Evidence of subtype B expansion. Virology. 2012;432(2):361-369. https://doi.org/10.1016/j.virol.2012.06.014 [ Links ]
31.Kakoola DN, Sheldon J, Byabazaire N, et al. Recombination in human herpesvirus-8 strains from Uganda and evolution of the K15 gene. J Gen Virol. 2001;82(10):2393-2404. https://doi.org/10.1099/0022-1317-82-10-2393 [ Links ]
32.Poole LJ, Zong JC, Ciufo DM, et al. Comparison of genetic variability at multiple loci across the genomes of the major subtypes of Kaposi's sarcoma-associated herpesvirus reveals evidence for recombination and for two distinct types of open reading frame K15 alleles at the right-hand end. J Virol. 1999;73(8):6646-6660. https://doi.org/10.1128/JVI.73.8.6646-6660.1999 [ Links ]
33.Ashutosh RT, Andrew OW, Greer AB, Gary RC. Prevalence odds ratio versus prevalence ratio: Choice comes with consequences. Stat Med. 2016;35(30):5730-5735. https://doi.org/10.1002/sim.7059 [ Links ]
34.Robbins HA, Pfeiffer RM, Shiels MS, Li J, Hall HI, Engels EA. Excess cancers among HIV-infected people in the United States. J Natl Cancer Inst. 2015;107(4), article #dju503. https://doi.org/10.1093/jnci/dju503 [ Links ]
35.Dryden-Peterson S, Medhin H, Kebabonye-Pusoentsi M, et al. Cancer incidence following expansion of HIV treatment in Botswana. PLoS One. 2015;10(8):e0135602. https://doi.org/10.1371/journal.pone.0135602 [ Links ]
36.Mehta S, Garg A, Gupta LK, et al. Kaposi's sarcoma as a presenting manifestation of HIV. Indian J Sex Transm Dis. 2011;32(2):108. https://doi.org/10.4103/0253-7184.85415 [ Links ]
37.Ahmed A, Muktar HM, Bugaje MA. Epidemiological and clinical features of AIDS-associated Kaposi's sarcoma in Northern Nigeria. Archiv Int Surg. 2013;3(1):29. https://doi.org/10.4103/2278-9596.117132 [ Links ]
38.Chalya PL, Mbunda F, Rambau PF, et al. Kaposi's sarcoma: A 10-year experience with 248 patients at a single tertiary care hospital in Tanzania. BMC Res Notes. 2015;8(1):440. https://doi.org/10.1186/s13104-015-1348-9 [ Links ]
39.Biryahwaho B, Dollard SC, Pfeiffer RM, et al. Sex and geographic patterns of human herpesvirus 8 infection in a nationally representative population-based sample in Uganda. J Infect Dis. 2010;202(9):1347-1353. https://doi.org/10.1086/656525 [ Links ]
40.Ngalamika O, Minhas V, Wood C. Kaposi's sarcoma at the University Teaching Hospital, Lusaka, Zambia in the antiretroviral therapy era. Int J Cancer. 2015;136(5):1241. https://doi.org/10.1002/ijc.29184 [ Links ]
41.Tukei VJ, Kekitiinwa A, Beasley RP. Prevalence and outcome of HIV-associated malignancies among children. AIDS. 2011;25(14):1789-1793. https://doi.org/10.1097/QAD.0b013e3283498115 [ Links ]
42.Begré L, Rohner E, Mbulaiteye SM, Egger M, Bohlius J. Is human herpesvirus 8 infection more common in men than in women? Systematic review and meta-analysis. Int J Cancer. 2016;139(4):776-783. https://doi.org/10.1002/ijc.30129 [ Links ]
43.National Cancer Control Strategy. Ministry of Health, Kenya. Strategy 2017 - 2022 Nairobi. 2017. [ Links ]
44.Achenbach CJ, Harrington RD, Dhanireddy S, Crane HM, Casper C, Kitahata MM. Paradoxical immune reconstitution inflammatory syndrome in HIV-infected patients treated with combination antiretroviral therapy after AIDS-defining opportunistic infection. Clin Infect Dis. 2011;54(3):424-433. https://doi.org/10.1093/cid/cir802 [ Links ]
45.Letang E, Lewis JJ, Bower M, et al. Immune reconstitution inflammatory syndrome associated with Kaposi sarcoma: Higher incidence and mortality in Africa than in the UK. AIDS. 2013;27(10):1603-1613. https://doi.org/10.1097/QAD.0b013e328360a5a1 [ Links ]
46.Kowalkowski MA, Kramer JR, Richardson PR, Suteria I, Chiao EY. Use of boosted protease inhibitors reduces Kaposi sarcoma incidence among male veterans with HIV infection. Clin Infect Dis. 2015;60(9):1405-1414. https://doi.org/10.1093/cid/civ012 [ Links ]
47.Borok M, Fiorillo S, Gudza I, et al. Evaluation of plasma human herpesvirus 8 DNA as a marker of clinical outcomes during antiretroviral therapy for AIDS-related Kaposi sarcoma in Zimbabwe. Clin Infect Dis. 2010;51(3):342-349. https://doi.org/10.1086/654800 [ Links ]
48.Mosam A, Shaik F, Uldrick TS, et al. A randomized controlled trial of highly active antiretroviral therapy ver-sus highly active antiretroviral therapy and chemotherapy in therapy-naive patients with HIV-associated Kaposi sarcoma in South Africa. J Acquir Immune Defic Syndr. 2012;60(2):150-157. https://doi.org/10.1097/QAI.0b013e318251aedd [ Links ]
49.Gbabe OF, Okwundu CI, Dedicoat M, Freeman EE. Treatment of severe or progressive Kaposi's sarcoma in HIV-infected adults. Cochrane Database Syst Rev. 2014;(9);CD003256. https://doi.org/10.1002/14651858.CD003256.pub2 [ Links ]
50.Krown SE, Roy D, Lee JY, et al. Rapamycin with antiretroviral therapy in AIDS-associated Kaposi sarcoma: An AIDS Malignancy Consortium study. J Acquir Immune Defic Syndr. 2012;59(5):447. https://doi.org/10.1097/QAI.0b013e31823e7884 [ Links ]
51.Krell J, Stebbing J. Broader implications of a stage-guided stratified therapeutic approach for AIDS-related Kaposi's sarcoma. J Clin Oncol. 2014;32(5):373. https://doi.org/10.1200/JCO.2013.53.7126 [ Links ]
52.Chinula L, Moses A, Gopal S. HIV-associated malignancies in sub-Saharan Africa: Progress, challenges, op-portunities. Curr Opin HIV AIDS. 2017;12(1):89. https://doi.org/10.1097/COH.0000000000000329 [ Links ]
53.Vaishnani JB, Bosamiya SS, Momin AM. Kaposi's sarcoma: A presenting sign of HIV. Indian J Der-matol Venereol Leprol. 2010;76(2):215. https://doi.org/10.4103/0378-6323.60542 [ Links ]
54.Fulciniti F, De Chiara A, Apice G, et al. Fine-needle cytology of Kaposi's sarcoma in an intramammarylymphnode: Report of one case. Diagn Cytopathol. 2012;40(S2):E149-E152. https://doi.org/10.1002/dc.21783 [ Links ]
55.Ouyang X, Zeng Y, Fu B, et al. Genotypic analysis of Kaposi's sarcoma-associated herpesvirus from patients with Kaposi's sarcoma in Xinjiang, China. Viruses. 2014;6(12):4800-4810. https://doi.org/10.3390/v6124800 [ Links ]
56.Van Bogaert LJ. Clinicopathological proficiency in the diagnosis of Kaposi's sarcoma. ISRN AIDS. 2012(5); Article #565463, 7 pages doi:10.5402/2012/565463 [ Links ]
 Correspondence:
Correspondence:
Rodgers Demba
dembanorman@gmail.com
Received: 01 Dec. 2018
Accepted: 15 May 2020
Published: 25 Aug. 2020


{kind=link}
{kind=link}