










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Industrial Engineering
versión On-line ISSN 2224-7890
versión impresa ISSN 1012-277X
S. Afr. J. Ind. Eng. vol.34 no.4 Pretoria dic. 2024
http://dx.doi.org/10.7166/34-4-2880
GENERAL ARTICLES
Comprehensive study of mobile assistance systems and their potential application areas in operating theatres
A. EngelI, II, ; F. DietrichI, II; T. LacknerI, II; I. de KockII; D. PalmI, III
IESB Business School, Reutlingen University, Baden-Württemberg, Germany
IIDepartment of Industrial Engineering, University of Stellenbosch, Stellenbosch, South Africa
IIIFraunhofer Institute for Manufacturing Engineering and Automation, Reutlingen, Germany
ABSTRACT
Mobile assistance systems (MAS) promise to overcome personnel shortages in operating theatres worldwide. A literature review inspired by the PRISMA 2020 method determines the state of the art of MAS, and identifies a lack of application areas for MAS in the operating theatre. Interviews with subject-matter experts aim to investigate application areas for MAS. The results show that most operational tasks refer to material management and patient management. MAS, with their potential to reduce the time needed for material and patient management, and the physical and mental strain of patient management, have great potential in the operating theatre.
OPSOMMING
Mobiele bystandstelsels (MAS) beloof om die personeeltekorte in die operasiesaal wêreldwyd te oorkom. 'n Literatuuroorsig geïnspireer deur die PRISMA 2020 metode bepaal die stand van die kuns van MAS en identifiseer 'n gebrek aan toepassingsareas vir MAS in die operasieteater. Onderhoude met vakkundiges het ten doel om toepassingsareas vir MAS te ondersoek. Die resultate toon dat die meeste operasionele take na materiaalbestuur en pasiëntbestuur verwys. MAS met die potensiaal om die tyd in materiële en pasiëntbestuur te verminder, sowel as fisiese en geestelike spanning in pasiëntbestuur, het groot potensiaal in die operasieteater.
1. INTRODUCTION
A shortage of personnel is the biggest challenge in healthcare systems worldwide. Various sectors in healthcare claim to have a shortage of personnel, including the operating theatres of hospitals, which do not have enough qualified nurses and surgical personnel [1]. To address the problem of personnel shortages, technological solutions are being extensively researched in healthcare and industry, primarily in the areas of artificial intelligence, robotics, and digitalisation [1]. The use of mobile assistance systems (MAS) - a sub-section of robotics - enables a high degree of autonomy and mobility in areas of operation. While MAS have already been deployed in hospitals, applications in operating theatres have not yet been sufficiently investigated. MAS promise to relieve personnel of burdensome health issues, repetitive tasks, and highstress procedures in the operating theatre [2-4]. Therefore, the application of MAS has the potential to overcome personnel shortages by improving the working conditions of nurses and surgical personnel.
This article aims to describe the state of the art of MAS in operating theatres and to motivate further research in this field. The objective is to analyse the state of the art of MAS in operating theatres with a literature review and, through semi-structured expert interviews, to identify areas in which MAS could be applied in operating theatres.
To generate such understanding first requires that MAS be defined. MAS are part of the category of collaborative robots with the ability to drive autonomously, to work in cooperation with humans in the same workspace, and to perform tasks such as locomotion, manipulation, or positioning, based on state and sensing [5-8]. According to the definition of the International Organization for Standardization (ISO), MAS include a control system that allows monitoring, controlling, and communicating with the environment [9,10].
After providing an overview of the general topic in Section 1, Section 2 reviews the relevant literature and describes the rationale of the paper. Section 3 describes the expert interviews and assesses the results. Section 4 recaps all of the findings, and Section 5 rounds off the topic with concluding remarks.
2. STATE OF THE ART OF MOBILE ASSISTANCE SYSTEMS IN OPERATING THEATRES
In this section, the approach, methodology, and aim of the literature review through the three phases of the PRISMA 2020 method - identification, screening, and results and synthesis - are described.
2.1. Approach, methodology, and aim of the literature review
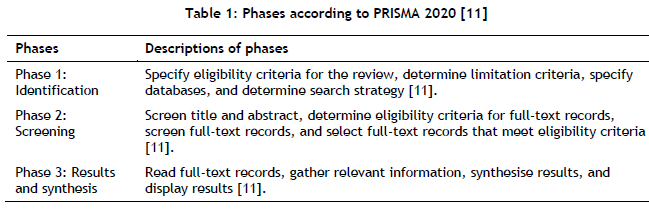
First, this paper describes a literature review according to the phases of the PRISMA 2020 method [11]. The aim of the literature review is to analyse the state of the art in areas in which MAS could be applied in operating theatres, and assesses their relevance in overcoming their current difficulties. The literature review is divided into three phases: phase 1: identification; phase 2: screening; and phase 3: results and synthesis. Table 1 below describes the phases further.
Phase 1: Identification
The first step was to specify eligibility criteria such as publication type, language, and publication date. Peer-reviewed white literature that was written in German or English and published between 2017-2022 was selected
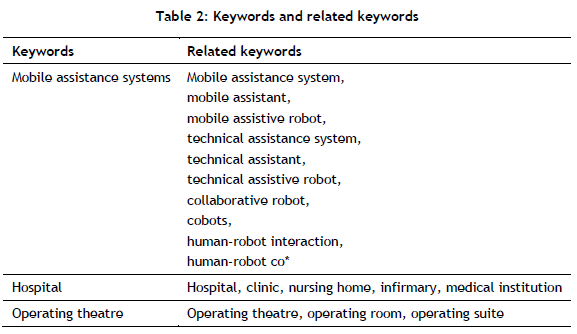
To cover a broad range of multi-disciplinary studies of MAS in technology and healthcare, the databases Scopus, Google Scholar, IEEE Xplore, the National Library of Medicine (NIH) and PMC US National Library were accessed to collect the literature for this study. To gain a deeper understanding of the keywords, related terms and synonyms, the snowballing method, using backwards and forward citation research, tested the first keyword selection [12]. Table 2 describes the final keywords selection for the literature review in detail.
Phase 2: Screening
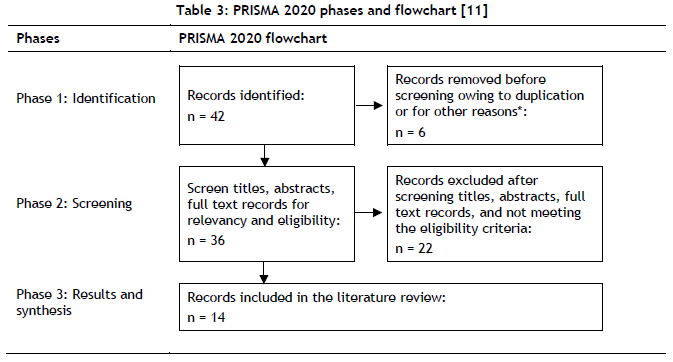
The screening phase screened the results of the articles from the databases. Table 3 describes the phases and the process of selecting the articles in a flowchart, which focused on MAS in hospitals and operating theatres, and encompassed the operational tasks associated with these systems.
In total, the literature review produced n = 42 matches. Six articles were excluded because of the limitation criteria, resulting in n = 36 articles. After removing duplicates and unavailable full-text articles, the literature review resulted in n = 14 articles for further investigation.
Phase 3: Results and synthesis
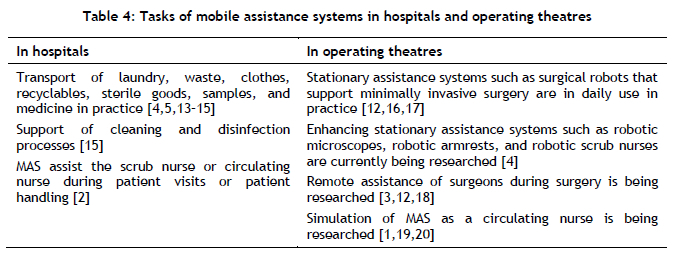
Several articles described the state of the art of MAS in hospitals and operating theatres and their operational tasks. Table 4 synthesises the results of the articles, and differentiates between operational tasks in hospitals and those in operating theatres.
To summarise, MAS in hospitals assist with operational tasks such as fetching and bringing material [4,5,1315], cleaning [15], and patient handling [2]. In the operating theatre, stationary operational tasks during surgery are used in practice and are being enhanced in research. Furthermore, remote surgery is an emerging topic in research [3,12,18]. First simulations analyse MAS in the context of fleet management in operating theatres to support the operational tasks of a circulating nurse [1,19,20]. In conclusion, MAS find application in hospitals for both mobile and stationary tasks. In operating theatres, stationary MAS systems are valuable in assisting medical procedures. However, the integration of MAS for mobile tasks in operating theatres is currently difficult, owing to the dynamic and safety-critical nature of this environment, especially during surgical procedures. In addition, research that evaluates the operational tasks that MAS could perform in operating theatres is lacking. To address this gap, this study conducted interviews with experts from several disciplines to identify tasks that MAS could undertake in operating theatres. This aimed to reduce the current lack of comprehensive research in this area.
3. EXPERT INTERVIEWS TO IDENTIFY POTENTIAL APPLICATION AREAS OF MAS IN OPERATING THEATRES
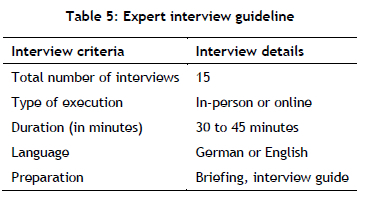
The objective of the semi-structured expert interviews was to identify areas for the application of MAS in operating theatres. To show the framework for the expert interviews, Table 5 describes the interview guideline.
Based on the framework for the interviews, the next section explains the interview phases in detail.
3.1. The approach of the semi-structured interviews
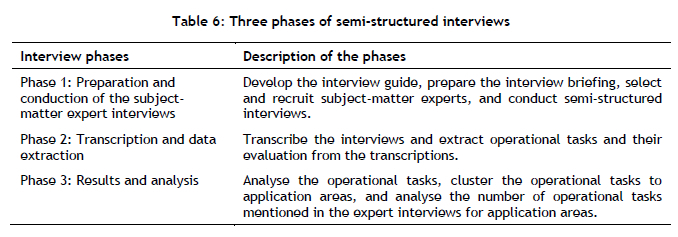
The method of Gläser and Laudel (2010) guided the interviews in three phases, as illustrated in Table 6.
3.1.1. Phase 1: Preparation and conducting of the subject-matter expert interviews
First, the identified gaps in the literature served to develop the interview questions for the interview guide. The structure of the interview guide followed the phases of surgery in operating theatres: pre-operative period, intra-operative period, and post-operative period.
• The pre-operative period starts when the decision is made to conduct the surgery, and ends after transferring the patient to the operating room bed [22].
• The intra-operative period starts when the patient is put on the operating table, and ends with transferring the patient to the postsurgical area [22].
• The post-operative period starts when transferring the patient to the postsurgical area, and ends with decreasing sequela for the patient from the surgical procedure [22].
Second, preparing a briefing was necessary to ensure the technical understanding and capability of MAS of a subject-matter expert with primary expertise and experience in the medical and clinical field. Further, a common understanding of the evaluation criteria for quality, time, risk, and the human factor was required. The evaluation criteria represented key performance indicators for operating theatres from the literature in order to evaluate the potential of MAS assisting operational tasks.
• The potential to improve the quality of personnel and patients by providing effective, safe, and people-centred care [17].
• The definition of time is linked to the general understanding of time with the potential to reduce the time of operational tasks and the entire process with MAS [23].
• The potential to reduce the risk is by evaluating the impact of uncertainty on the goals, typically by considering sources, potential events, consequences, and likelihood [10]. In this context, it was about reducing the risk by using MAS.
• The potential to improve the human factor refers to maximising human well-being and the total system performance. The scientific field focuses on understanding the interactions between humans and the other components of a system. This is related to the different types of ergonomics: physical, cognitive, and organisational. In this context, the assistance of MAS potentially reduced the physical and mental strain of medical experts [24].
Third, the selection of experts aimed to cover the generic roles in operating theatres that participate actively in the surgical process. The following generic roles in operating theatres and the corresponding number of interviewed experts are identified [13,18,19]: surgeons (n=2), surgical assistants (n=2), circulators (n=3), scrub practitioners/nurses (n=3), anaesthetists (n=3), and anaesthetic assistants (n=2).
In the interviews with the experts, each role was covered at least twice to ensure that all of the perspectives involved in surgery were included. To differentiate and reduce the risk of bias further, the subject-matter experts had experience in working in different hospitals worldwide. In addition, a workshop with technical experts in the domain of MAS was conducted to cover the technical perspectives on MAS and their implementation in hospitals.
In the interviews, the interviewer asked the subject-matter experts to propose and describe the operational tasks that could be assisted by MAS and to evaluate these from an operational perspective in respect of quality, time, risk, and the human factor.
3.1.2. Phase 2: Transcription and data extraction
The transcription of each interview, as well as the data extraction, followed the guidelines of Gläser and Laudel (2010) [21].
The data extraction served to extract the operational tasks and their evaluation from the transcription. Five main steps were involved: (i) the preliminary theoretical consideration, (ii) preparation of the extraction, (iii) the extraction, (iv) processing, and (v) evaluation. These were needed to substantiate scientifically a qualitative content analysis [21]. The predefined codes were 'pre-operative period', 'intraoperative period', and 'post-operative period', following the structure of the interview guide. Further relevant information was added by creating additional codes to achieve a better result in determining the objective. The evaluation and justification for each application area were in the form of codes that were added while extracting the information. Adding a new code included reviewing the previous transcriptions with the additional code.
3.1.3. Results and analysis
The data extraction resulted in a list of 222 operational tasks, including redundant answers from the experts. These operational tasks related to opportunities for MAS in hospitals from a clinical perspective. To synthesise the operational tasks, the application areas - visualisation, patient management, material management, guidance support, equipment and furniture set-up, cleaning operating theatre, and administrative support - clustered the redundant operational tasks. These application areas served to analyse the number of operational tasks, using the following structure: (i) comparison of the number of operational tasks for the application areas; (ii) comparison of the number of operational tasks in the pre-, intra-, and post-operative periods; (iii) analysis of the number of operational tasks in the pre- and postoperative periods in comparison with the intra-operative period; and (iv) analysis of the evaluation criteria relating to quality, time, risk, and the human factor.
Visualisation
The operational tasks of visualisation described displaying the vital signs of the patient. Further, the MAS could display information about risks, the patient's treatment history, images, and guidelines.
(i) Comparison of the number of operational tasks for application areas.
For visualisation, 21 operational tasks were mentioned.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 5
• Intra-operative period: 8
• Post-operative period: 8
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
From the perspective of the surgery schedule for one day in an operating theatre, the post-operative period of one surgical operation that has just been performed can, at the same time, be the pre-operative period for the next surgery. In addition, for some application areas, the operational tasks in the pre- and postoperative periods do not differ. Therefore, this analysis served to contrast similar operational tasks in the pre- and post-operative periods with the intra-operative period from the perspective of an entire day in the operating theatre.
First, the extra-operative period synthesised the pre-and post-operative periods. Second, the analysis included exploring similar operational tasks in the pre- and post-operative periods and clustering them in the extra-operative period. This resulted in similar operational tasks in the pre- and post-operative periods for six out of seven application areas. For visualisation, the analysis resulted in the following figures:
• Intra-operative period: 8
• Extra-operative period: 13
The second-highest number of operational tasks were found under visualisation in the extra-operative period.
(iv) Analysis of the evaluation criteria relating to quality, time, risk, and the human factor:
• Time was the most frequently mentioned criterion for visualisation
Patient management
'Patient management' relates to operational tasks with the patient, namely communicating with and supporting the patient with the desired service - for instance, completing documentation with the patient and bringing them something to drink. It also includes handling the patient by lifting and reposition them; assessing the patient (for instance, help in washing the patient, guiding them through a breathing exercise, checking the cables and tubes attached to the patient, and transporting the patient).
(i) Comparison of the number of operational tasks for application areas.
In patient management, 48 operational tasks were identified, solidifying its position as the second most frequently mentioned application area.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 21
• Intra-operative period: 1
• Post-operative period: 26
In the post-operative period, the majority of operational tasks referred to patient management.
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
Intra-operative period: 1
Extra-operative period: 47
The majority of operational tasks were in patient management in the extra-operative period. In particular, most referred to transportation.
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
Most of the criteria for quality and the human factor referred to patient management.
Material management
'Material management' covers transporting, commissioning, providing, preparing, storing, and checking material.
(i) Comparison of the number of operational tasks for application areas.
In relation to material management, 85 redundant operational tasks were mentioned. Material management was the application area with the majority of operational tasks for MAS.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 37
• Intra-operative period: 26
• Post-operative period: 22
The majority of the operational tasks in the pre- and intra-operative periods were in material management.
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
In relation to material management, the operational tasks differed among the three operative periods. Within the pre-operative period, the focus of material management is to transport and commission material; within the intra-operative period, it is mainly about providing and preparing the material; and in the post-operative period, it involves storing, refilling, and cleaning the material.
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
Material management occupied the majority of the criteria time. Most of the criteria for quality and the human factor referred to material and patient management.
Guidance support
'Guidance support' refers to analysing patients' vital signs, with feedback if they reach the threshold; checking, advising, guiding, and recommending personnel - for instance, when material or documentation is missing; and exchanging information. Further operational tasks are to prioritise and orchestrate tasks, to assist with the count control of material, and to offer remote support during surgery by guiding another surgeon (by voice) through the surgery.
(i) Comparison of the number of operational tasks for application areas.
Guidance support ranked as the third most frequently mentioned operational tasks, with 32 specific tasks.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 12
• Intra-operative period: 13
• Post-operative period: 7
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
• Intra-operative period: 13
• Extra-operative period: 19
In the intra-operative period, most of the operational tasks were clustered under guidance support, with 13 operational tasks.
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
Time was the most frequently mentioned criterion for guidance support.
Equipment and furniture set-up
Operational tasks for equipment and furniture involve positioning the equipment - for instance, the operating table, screens, and lamps. Further operational tasks for MAS are to push and pull movable infrastructure equipment such as ultrasound machines.
(i) Comparison of the number of operational tasks for application areas.
For equipment and furniture set-up, 18 redundant operational tasks were mentioned.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 9
• Intra-operative period: 3
• Post-operative period: 6
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
• Intra-operative period: 3
• Extra-operative period: 15
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
For the equipment and furniture set-up, the human factor was the criterion with the most comments.
Cleaning operating theatre
'Cleaning the operating theatre' involves cleaning the operating room - for instance, disinfecting surfaces and cleaning the walls and floors. This application area also includes cleaning the equipment in the operating room.
(i) Comparison of the number of operational tasks for application areas.
In relation to cleaning the operating theatre, eight redundant operational tasks were mentioned.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 1
• Intra-operative period: 0
• Post-operative period: 7
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
• Intra-operative period: 0
• Extra-operative period: 8
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
Time was the most frequently mentioned criterion for cleaning the operating theatre.
Administrative support
'Administrative support' involves displaying relevant information - for instance, the patient's name and address, required laboratory tests, and material used for surgery. In addition, the MAS could enter and save the documentation.
(i) Comparison of the number of operational tasks for application areas:
In relation to administrative support, 10 redundant operational tasks were mentioned.
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
• Pre-operative period: 5
• Intra-operative period: 1
• Post-operative period: 4
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
• Intra-operative period: 1
• Extra-operative period: 9
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
Time was the most frequently mentioned criterion for administrative support.
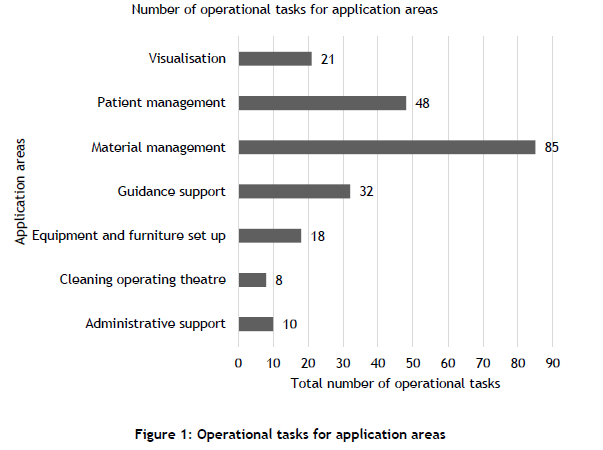
The charts below visualise the analysis in the form of bar charts, compare the application areas, and emphasise the outcomes.
(i) Comparison of the number of operational tasks for application areas
Figure 2 shows the number of operational tasks for the application areas of visualisation, patient management, material management, guidance support, equipment and furniture set-up, cleaning operating theatre, and administrative support. The difference between material management and patient management was 37, and between patient management and guidance support it was 16. The differences between guidance support and visualisation, between equipment and furniture set-up and administrative support, and between administrative support and cleaning the operating theatre were comparatively low (between 2 and 11). To summarise, Figure 2 shows that material management was the application area with the majority of operational tasks for MAS; it was followed by patient management, guidance support, and visualisation.
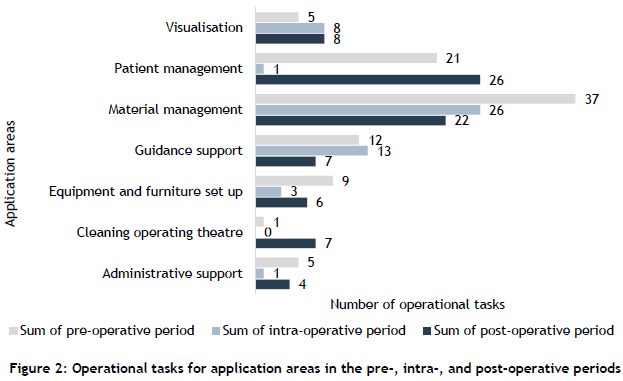
(ii) Comparison of the number of operational tasks in the pre-, intra-, and post-operative periods:
Figure 3 shows the number of operational tasks for application areas in the pre-, intra-, and post-operative periods. In the pre-operative period, the greatest number of operational tasks were mentioned in relation to material management, with 37 operational tasks, followed by patient management with 21 operational tasks. In the intra-operative period, the greatest number of operational tasks were found under material management, with 26 operational tasks; guidance support had 13 operational tasks. In the post-operative period, the greatest number of operational tasks were clustered under patient management, with 26 operational tasks, followed by material management with 22 operational tasks. To summarise, material management involved the majority of the operational tasks during the pre- and intra-operative periods, while patient management required the majority of the operational tasks in the post-operative period.
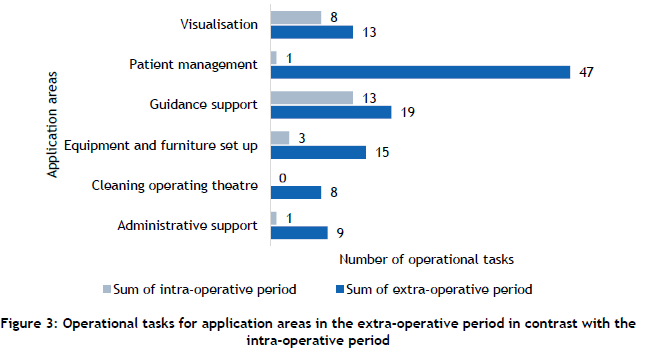
(iii) Analysis of the number of operational tasks in the pre- and post-operative periods in comparison with the intra-operative period:
Figure 4 shows the number of operational tasks for the application areas in the intra- and extra-operative periods. The majority of the operational tasks were in patient management, with 47 operational tasks; the second-highest number of operational tasks were found under visualisation, with 13 operational tasks; both were in the extra-operative period. In the intra-operative period, the greatest number of operational tasks were clustered under guidance support, with 13 operational tasks. However, all of the operational tasks for the application areas in the extra-operative period were greater in number than those in the intraoperative period. This showed a clear tendency towards using the assistance of MAS for operational tasks in the extra-operative period. Since patient management was the application area with the greatest number of operational tasks in the extra-operative period, the next analysis explores patient management in depth.
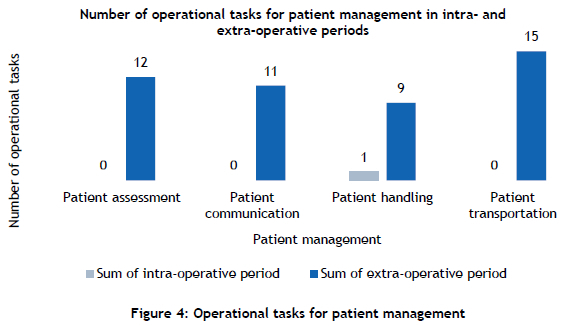
Figure 5 shows the number of operational tasks for patient management in relation to patient assessment, communication, handling, and transportation in the intra- and extra-operative periods. The greatest number of operational tasks were clustered under patient transportation, with 15 operational tasks, while the second-highest number of operational tasks were found in patient assessment with 12 operational tasks, followed by patient communication with 11 operational tasks and patient handling with nine operational tasks. In the intra-operative period, patient handling was the only operational task to be mentioned. To summarise, the majority of the operational tasks in patient management were for patient transportation in the extra-operative period.
(iv) Analysis of the evaluation criteria for quality, time, risk, and the human factor:
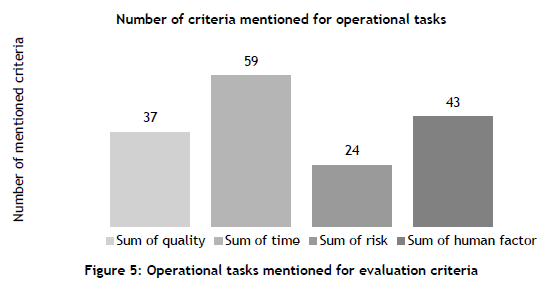
Figure 5 shows the number of criteria mentioned for quality, time, risk, and the human factor as the main criteria for the specific operational task. Quality was mentioned 37 times, time 59 times, risk 24 times, and the human factor 43 times. Time was identified as the main criterion, with the human factor mentioned as the next-highest.
An in-depth analysis of the criteria for each application area showed that, for all of the application areas, risk was the lowest-ranked criterion. Time was mentioned most often for six of the seven application areas. For equipment and furniture set-up, the human factor was the criterion with the most comments. Material management contained the majority of the criterion of time, followed by patient management. The criteria of quality and the human factor referred most often to material management and patient management. While the number for time in material management showed a clear gap between it and the human factor, the difference between time and the human factor was smaller for patient management.
Another finding from the interviews was that, while all of the operational tasks would benefit from improvements in quality and the human factor and from reductions in time and risk, the application areas for evaluating the main criteria varied. The subject-matter experts also emphasised that the operational tasks were generic for many operating rooms and could be transferred to other operating rooms.
To summarise the data extraction analysis and results: material management and patient management were the application areas that contained the majority of the operational tasks. The in-depth analysis of the pre-, intra-, and post-operative periods identified the greatest number of operational tasks in material and patient management for the pre- and post-operative periods. Most of the same operational tasks in the extra-operative period related to patient management, especially patient transportation.
4. RESULTS
To summarise the literature review: MAS would assist with hospitals' operational tasks such as fetching and bringing material [4,5,13-15], cleaning [15], and patient handling [2].
To transfer the MAS from the hospital to the operating theatre, simulations helped to assess the operational tasks of a circulating nurse [1,19,20]. The literature review showed that there has been little research into identifying and evaluating the operational tasks of MAS in operating theatres. To identify the potential tasks of MAS in operating theatres, interviews with experts from a range of disciplines were conducted.
The analysis of the interviews resulted in the following. The majority of the operational tasks related to material management, followed by patient management and guidance support. The majority of the operational tasks for material management were in the pre-operative and intra-operative periods. In the post-operative period, the majority of the operational tasks were found in patient management. The analysis comparing the pre- and post-operative periods with the extra-operative period revealed that patient management in the extra-operative period had the greatest number of operational tasks. A more thorough review of patient management in the extra-operative period showed that most of the operational tasks related to patient transportation. The analysis of the evaluation criteria identified time as the main criterion, followed by the human factor, quality, and risk for all of the application areas. For the individual application areas in detail, time was most frequently mentioned for material management and patient management.
5. CONCLUSION
The systematic literature review clearly revealed the gap in research into the operational tasks of MAS in hospitals, despite the increasing shortage of medical staff worldwide.
In hospitals, mobile assistance systems could assist in pre-, post-, and intra-operative tasks such as material handling and transportation, cleaning, and patient handling. In operating theatres, stationary surgical assistance systems that perform operational tasks have been improved by research and industry over the past decade. Furthermore, research into remote surgery is underway. To support a circulator's operational tasks, simulations first analysed mobile assistance systems in an operating theatre.
Since operational tasks are rarely identified in the literature, 15 expert interviews were conducted for this study. The experts covered each surgical role in operating theatres at least twice in order to cover all of the common roles in operating theatres. The expert interviews identified 222 potential operational tasks for MAS. The analysis of the interviews showed in particular that material handling and transport by MAS would be highly relevant to operating theatres. According to the technical experts, the development of MAS for material management in operating theatres showed great potential for implementation. The strategy recommended by the medical and technical experts was first to implement MAS for tasks outside the operating room before extending the capabilities to include intra-operative tasks. In this context, achieving acceptance among the medical staff for the use of MAS would play a critical and decisive role. The proposed MAS would assist in standardised procedures in the pre- and post-operative periods according to the surgical plan and case card. In the intra-operative period, the MAS would provide material at the entrance to the operating room.
During the initial implementation phase of the MAS, entering the operating room would be prohibited while a patient was undergoing surgery owing to limited space, high traffic density, moving obstacles, and high sterility requirements. Outside the operating room, however, the MAS would execute the material tasks autonomously, receiving and processing instructions from the surgeon and navigating autonomously.
In addition, the criteria analysis assessed time as the key criterion for material handling and for transportation and patient management. Consequently, the assistance of MAS in those application areas would be especially beneficial in reducing processing time or relieving medical staff from physical and mental strain.
REFERENCES
[1] L. Bernhard, A.F. Amalanesan, O. Baumann, F. Rothmeyer, Y. Hafner, M. Berlet, D. Wilhelm, & A. Knoll, Mobile service robots for the operating room wing: Balancing cost and performance by optimizing robotic fleet size and composition, International Journal of Computer Assisted Radiology and Surgery, 18(2), 195-207, 2022. https://doi.org/10.1007/s11548-022-02735-8 [ Links ]
[2] E. Ackerman, Moxi prototype from diligent robotics starts helping out in hospitals, IEEE Spectrum (18 September 2018). https://spectrum.ieee.org/moxi-prototype-from-diligent-robotics-starts-helping-out-in-hospitals [accessed 8 December 2023]. [ Links ]
[3] F. Mathis-Ullrich & P.M. Scheikl, Robotik im operationssaal - (Ko-)Operieren mit kollege roboter, Der Gastroenterologe Zeitschrift fur Gastroenterologie und Hepatologie, 16, 25-34, 2020. https://doi.org/10.1007/s11377-020-00496-x [ Links ]
[4] X. Sun, J. Okamoto, K. Masamune, & Y. Muragaki, Robotic technology in operating rooms: A review, Current Robotics Report, 2, 333-341, 2021. https://doi.org/10.1007/s43154-021-00055-4 [ Links ]
[5] G. Fragapane, R. de Koster, F. Sgarbossa, & J.O. Strandhagen, Planning and control of autonomous mobile robots for intralogistics: Literature review and research agenda, European Journal of Operational Research, 294, 1-22, 2021. https://doi.org/10.1016/j.ejor.2021.01.019 [ Links ]
[6] P. Hold, F. Ranz, W. Sihn, & V. Hummel, Planning operator support in cyber-physical assembly systems, IFAC-PapersOnLine 49, 60-65, 2016. https://doi.org/10.1016/jj.ifacol.2016.12.190 [ Links ]
[7] M. Wiesbeck, Struktur zur representation von montagesequenzen für die situationsorientierte werkerführung. Technische Universität München, Dissertation, München, 2014. [ Links ]
[8] G. Reisinger, T. Komenda, P. Hold, & W. Sihn, A concept towards automated data-driven reconfiguration of digital assistance systems, Procedia Manufacturing, 23, 99-104, 2018. https://doi.org/10.1016/j.promfg.2018.03.168 [ Links ]
[9] International Organization for Standardization (ISO), ISO 8373:2012(en): Robots and robotic devices - Vocabulary, 2012. https://www.iso.org/obp/ui/#iso:std:iso:8373:ed-2:v1:en:term:5.12 [accessed 7 November 2022]. [ Links ]
[10] International Organization for Standardization (ISO), ISO 31000:2018(en): Risk management - Guidelines, 2018. https://www.iso.org/obp/ui/#iso:std:iso:31000:ed-2:v1:en [accessed 5 January 2023]. [ Links ]
[11] M.J. Page, D. Moher, P.M. Bossuyt, I. Boutron, T.C. Hoffmann, C.D. Mulrow, L. Shamseer, J.M. Tetzlaff, E.A. Akl, S.E. Brennan, R. Chou, J. Glanville, J.M. Grimshaw, A. Hróbjartsson, M.M. Lalu, T. Li, E.W. Loder, E. Mayo-Wilson, S. McDonald, L.A. McGuinness, L.A. Stewart, J. Thomas, A.C. Tricco, V.A. Welch, P. Whiting, & J.E. McKenzie, PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews, BMJ (Clinical research ed.), 372, 1-36, 2021. https://doi.org/10.1136/bmj.n160 [ Links ]
[12] J. Spiegelberg, T. Iken, M.K. Diener, & S. Fichtner-Feigl, Robotic-assisted surgery for primary hepatobiliary tumors - Possibilities and limitations, Cancers, 14, 1-18, 2022. https://doi.org/10.3390/cancers14020265 [ Links ]
[13] E. Ahmadi, D.T. Masel, A.Y. Metcalf, & K. Schuller, Inventory management of surgical supplies and sterile instruments in hospitals: A literature review, Health Systems, 8(2), 134-151, 2019. https://doi.org/10.1080/20476965.2018.1496875 [ Links ]
[14] G. Fragapane, H.-H. Hvolby, F. Sgarbossa, & J.O. Strandhagen, Autonomous mobile robots in hospital logistics, advances in production management systems: The path to digital transformation and innovation of production management systems, Proceedings APMS 2020, 591, 672-679, 2020. https://doi.org/10.1007/978-3-030-57993-7_76 [ Links ]
[15] J. Steil, D. Finas, S. Beck, A. Manzeschke, & R. Haux, Robotic systems in operating theaters: New forms of team-machine interaction in health care, Methods of Information in Medicine, 58, e14-e25, 2019. https://doi.org/10.1055/s-0039-1692465 [ Links ]
[16] J. Brandenburg, D. Junger, A. Schulze, M.A. Pieumi Nzeuhang, E. Just, A. Billeter, S. Bodenstedt, S. Speidel, O. Burgert, M. Wagner, & B. Müller-Stich, Interaktive workflow analyse am beispiel der roboter-assistierten ösophagusresektion ein checklisten -Tool für chirurgen im operationssaal, Hochschule Reutlingen, 2022. https://doi.org/10.34645/opus-3188 [ Links ]
[17] E. Mewes, A. Bergmüller, A. Minow, S. Wassmann, & R. Mecke, Digitale Assistenzsysteme zur mobilen Verwendung im technischen Service - Ein Leitfaden für die Gestaltung und Nutzung, Fraunhofer IFF, 2020. ISBN 978-3-00-065405-3 [ Links ]
[18] H.R.M. Pelikan, A. Cheatle, M.F. Jung, & S.J. Jackson, Operating at a distance - How a teleoperated surgical robot reconfigures teamwork in the operating room, Proc. ACM Hum.-Comput. Interact., 2, 1-28, 2018. https://doi.org/10.1145/3274407 [ Links ]
[19] D.I. Athanasiadis, S. Monfared, J. Whiteside, T. Engle, L. Timsina, A. Banerjee, A. Butler, & D. Stefanidis, Comparison of operating room inefficiencies and time variability in laparoscopic gastric bypass, Surgery for Obesity and Related Diseases, 16, 1226-1235, 2020. https://doi.org/10.1016/j.soard.2020.04.046 [ Links ]
[20] A. Bhosekar, T. Isik, S. Eksjogïu, K. Gilstrap, & R. Allen, Simulation-optimization of automated material handling systems in a healthcare facility, IISE Transactions on Healthcare Systems Engineering, 11(4), 316-337, 2021. https://doi.org/10.1080/24725579.2021.1882622 [ Links ]
[21] J. Gläser & G. Laudel, Experteninterviews und qualitative inhaltsanalyse als instrumente rekonstruierender untersuchungen, 4th ed., Wiesbaden: VS Verlag, 2010. [ Links ]
[22] T. Goodman & C. Spry, Essentials of perioperative nursing, Burlington, MA: Jones & Bartlett Learning, 2017. [ Links ]
[23] W.H. Newton-Smith, The structure of time, Boca Raton, FL: Routledge, 1980. [ Links ]
[24] W. Karwowski, Ergonomics and human factors: The paradigms for science, engineering, design, technology and management of human-compatible systems, Ergonomics, 48, 436-463, 2005. https://doi.org/10.1080/00140130400029167 [ Links ]
Submitted by authors 25 Feb 2023
Accepted for publication 24 Oct 2023
Available online 14 Dec 2023
* Corresponding author: annika.engel@student.reutlingen-university.de
ORCID® identifiers
A. Engel: https://orcid.org/0009-0006-1178-3049
F. Dietrich: https://orcid.org/0009-0008-3155-802X
T. Lackner: https://orcid.org/0009-0009-8394-2549
I . de Kock: https://orcid.org/0000-0003-4136-7418
D. Palm: https://orcid.org/0000-0003-1485-8078


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}