










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Industrial Engineering
On-line version ISSN 2224-7890
Print version ISSN 1012-277X
S. Afr. J. Ind. Eng. vol.33 n.3 Pretoria Nov. 2022
http://dx.doi.org/10.7166/33-3-2813
SPECIAL EDITION
Factors affecting the sustainability of lean in healthcare: a systematic literature review
R.S. Wagner*; T.S. Hattingh; H. Meijer
School of Industrial Engineering, North-West University, South Africa
ABSTRACT
The application of Lean in healthcare has been steadily climbing since 2000. However, Lean implementation in healthcare environments has experienced high failure rates that could be attributed to a lack of sustainable implementation. A knowledge gap has therefore been identified, in both practice and research, to understand the reason for failure and the impact of Lean sustainability on Lean success. The aim of the main study is to explore the factors that affect the sustainability of Lean healthcare in South African hospitals. This paper reports on the first part of the study, a systematic literature review (SLR) that identifies the factors that affect the sustainability of Lean healthcare in hospitals. Through the SLR, 50 factors affecting Lean sustainability in hospitals were identified and grouped into 12 themes. These themes were then tested against Lean principles. The results showed that the adaptation of Lean so that it makes sense to healthcare staff and is compatible with a hospital context is important for sustainability. Staff and organisational readiness during Lean implementation is also critical for long-term sustainability. The SLR results will be used to develop an interview protocol for the second part of the main study, which will involve interviews with South African-based practitioners, consultants, and academics who are directly involved in Lean implementation in South African hospitals.
OPSOMMING
Die toepassing van "Lean" in gesondheidsorg het geleidelik gestyg sedert 2000. Die implementering van "Lean" in gesondheidsorgomgewings het egter 'n hoè historiese falingsyfers wat toegeskryf kan word aan 'n gebrek aan volhoubare implementering. 'n Kennisgaping is dus gei'dentifiseer, in beide praktyk en navorsing, om die rede vir mislukking en die impak van die volhoubaarheid van "Lean" op "Lean"-sukses te verstaan. Die doel van die studie is om die faktore te ondersoek wat die volhoubaarheid van "Lean" in gesondheidsorg in Suid-Afrikaanse hospitale affekteer. Hierdie artikel doen verslag oor die eerste deel van die studie, 'n sistematiese literatuuroorsig (SLR) wat die faktore identifiseer wat die volhoubaarheid van "Lean" in gesondheidsorg in hospitale beinvloed. Deur die SLR is 50 faktore wat "Lean"-volhoubaarheid in hospitale beinvloed geidentifiseer en in 12 temas gegroepeer. Hierdie temas is daarna getoets teen "Lean"-beginsels. Die resultate het getoon dat die aanpassing van "Lean" sodat dit sin maak vir gesondheidsorgpersoneel en versoenbaar is met 'n hospitaalkonteks, belangrik is vir volhoubaarheid. Personeel en organisatoriese gereedheid tydens "Lean"-implementering is ook van kritieke belang vir langtermyn volhoubaarheid. Die SLR-resultate sal gebruik word om 'n onderhoudprotokol vir die tweede deel van die hoofstudie te ontwikkel, wat onderhoude met Suid-Afrikaans-gebaseerde praktisyns, konsultante en akademici sal behels wat direk betrokke is by "Lean"-implementering in Suid-Afrikaanse hospitale.
1. INTRODUCTION
1.1. Background
Over the last decade, many healthcare organisations have adopted Lean thinking to reduce waste and improve flow efficiency in patient processes [1]. However, evidence points to recurring failures in implementation [2]. The reason for these failures could lie in the interpretation and understanding of the Lean concept, as many healthcare organisations restrict their Lean implementation to eliminating process variation, reducing waste, and increasing financial performance [3]. Recent perspectives argue that Lean should be implemented in a more comprehensive way, as a cultural phenomenon instead of just a set of tools and techniques for process improvement [4]. Even though Lean tools are important, they depend for their effectiveness on the ability to develop an organisational culture to support continuous improvement [5]. Most current research focuses on evaluating Lean implementation in healthcare [6], but, to ensure sustainability, the focus should shift to a "more critical and theoretical understanding of how Lean interacts with the pre-existing healthcare context" [4].
Henrique et al. [5] highlight that Lean in healthcare has been widely reported in the literature. Owing to the complexity of hospital environments, the application of Lean thinking might encounter specific challenges that other industries do not, as further illustrated by Henrique et al. [5]. These hospital complexities can include, among other things, the need to balance strategy and care delivery [5].
Despite considerable practical and theoretical efforts towards the development and implementation of healthcare innovations such as Lean, comparatively little effort has been given to their sustainability [7]. Several studies in the literature report on the need for more in-depth studies of the long-term sustainability of Lean improvements in healthcare. This is specifically highlighted by the link between a continuous improvement culture and sustainability, with the premise that, to achieve higher performance, improvement has to be sustained so that the current state or baseline is consistently at a higher level [6]. This enables the creation of a continuous cycle of improvements [5]. As stated by Schell et al., "There remains a need to address the lack of conceptual clarity and comprehensive frameworks to understand how effective healthcare-related improvements can be successfully sustained" [8].
In the South African healthcare context, the management and leadership crisis, uneven resource distribution, ineffective government strategies to improve healthcare, biased preference by healthcare professionals between the private and public sector and between provinces in the public sector, and the slow progress of restructuring healthcare systems are some of the issues affecting healthcare [9]. Kruger [10] mentions that formal processes in public healthcare facilities are overwhelmingly manual and often non-existent. This creates an opportunity for Lean healthcare, which could be used as a philosophy to transform healthcare in South Africa.
It has been shown that Lean methodologies have the potential to reduce some waste in healthcare in a South African context, and that significant improvements in efficiency are possible without additional resource investment [11]. Mutingi et al. [12] identified a suite of South African-specific success factors for the application of Lean in healthcare. These included holistic and systems thinking, defining the customer to include other important stakeholders such as family members, caregivers, local communities and taxpayers, commitment and full involvement of healthcare staff, training and developing employees, giving employees responsibility to make improvement initiatives, management support at all levels, and the provision of sufficient resources. It was also highlighted that Lean philosophy needs to be taught and implemented as an improvement tool, and that employees at all levels need to be educated about the long-term benefits of Lean healthcare.
1.2. Purpose of the study
It is evident that, although Lean has been implemented in healthcare, the factors affecting the sustainability of Lean in healthcare have not been broadly researched or understood. The broader aim of the main study is to identify and analyse the factors that affect the sustainability of Lean healthcare in South African hospitals. This paper reports on the first phase of the main study, which is to identify in the literature the factors affecting Lean sustainability. The findings from this first phase will inform the development of a series of interview questions that will be used in the next phase to explore the experiences of practitioners and experts in hospital settings in South Africa. This paper reports on only the findings from the first phase of the study.
Therefore, the research question this paper aims to address is: What factors that affect the sustainability of Lean healthcare can be extracted from the current body of literature?
2. LITERATURE REVIEW
2.1. Lean
Lean is derived from the Toyota Production System, which is famous for its focus on the customer, continuous improvement, and waste elimination. Lean can be defined as the organisational practice that aims to eliminate waste along the entire value stream and to create more value for customers [13]. This definition emphasises two elements: value for the customer (which is the end goal), and waste elimination (which is the journey to achieve the end goal). Therefore, the key idea or objective of Lean is to increase value for the customer while reducing the number of resources consumed and cycle times via waste elimination [14].
Lean can also be described at different levels [14], where each level of abstraction captures its important features. First, Lean thinking refers to the overarching philosophy or beliefs, values, and purpose of an organisation. Second, Lean principles refer to the five principles of Lean: define customer value, capture the value stream, establish pull, establish flow, and continuously strive for perfection. Third, Lean practices include enabling tools and techniques such as value stream mapping and visual management.
Core to Lean philosophy are the concepts of continuous improvement and respect for people. These go hand-in-hand since, as we respect people, we are driven to improve continuously. This respect requires engagement with staff, physicians, and patients in the improvement process, and as a result, it is through this respect that improvement happens [15]. Pakdil et al. believe that Lean philosophy is therefore based on a 4-P model that emphasises the synergy between philosophy, processes, people and partners, and problem-solving [16].
2.2. Lean healthcare
As stated by Womack and Jones [17], many non-manufacturing contexts have adopted Lean as a tool to achieve results. Healthcare organisations have also adopted Lean as a model to improve the quality and productivity of their operations. In many cases, this has been done successfully by applying tools and concepts from the Lean model [18]. Lean healthcare typically focuses on developing a hospital culture that is characterised by increased patient and other stakeholder satisfaction. This is done through continuous improvement that engages all employees, including managers, physicians, nurses, laboratory staff, technicians, and administrators, who are encouraged actively to identify and reduce non-value-adding activities or waste [18]. Healthcare contexts are frequently characterised by limited resources and increasing demand. The performance and effectiveness of care amid these constraints can be improved by adopting a long-term philosophy that aims to embed Lean at the heart of healthcare organisations [19].
2.3. Sustainability in Lean healthcare
Naik et al. [20] recognised sustainability as a challenge in Lean healthcare and propose four suggestions to address this. These include clear communication and training, implementing new processes at off-peak hours with process owners and executives present, representation from all Lean teams due to the different conditions for each team and establishing clinical and mid-level management champions for sustainability. Executive commitment, stakeholder support and a vision statement aligned to departmental values [17], staff involvement and team creation [18] have also been defined as key elements for successfully sustaining Lean in healthcare contexts.
However, Dahlgaard et al. [21] state that, like other industries, healthcare providers often start Lean implementation without understanding the cultural and structural preconditions that Lean requires. "It normally requires a cultural change where the soft or intangible factors of management (the systemic factors) like leadership, people management and partnerships are changed, so that a new organisational culture is developed to support and improve the hospitals core processes" [21]. Furthermore, Radnor and Boaden [22] warn that a narrow focus on just tools and techniques can fail to align improvements with a long-term vision and wider strategy. As a result, the sustainability activities of continuous improvement and problem-solving culture can become neglected [23].
The incorporation of Lean typically can lead to radical organisational and process changes that can clash directly with the existing organisational culture [4]. To overcome organisational cultural barriers, the following typically needs to be in place: inter- and intra-departmental communication, a commitment to stabilise the organisation in a changing environment, a customer-centric approach, and a clear change strategy that is aligned with organisational ambitions [17].
Lean healthcare, therefore, needs to consider structures, systems, and mindsets to ensure sustainability after the initial investment [23]. Flynn et al. [24] note that improvement interventions are meaningless unless efforts are directed at long-term sustainability; and yet, the mechanisms that enable sustainability remain not well understood.
3. RESEARCH METHODOLOGY
To address the research question, a systematic literature review (SLR) is used. The purpose of this review is to identify the factors that affect the sustainability of Lean healthcare in hospitals. Henrique et al. [5] have done a similar review, but limited their findings to critical success factors.
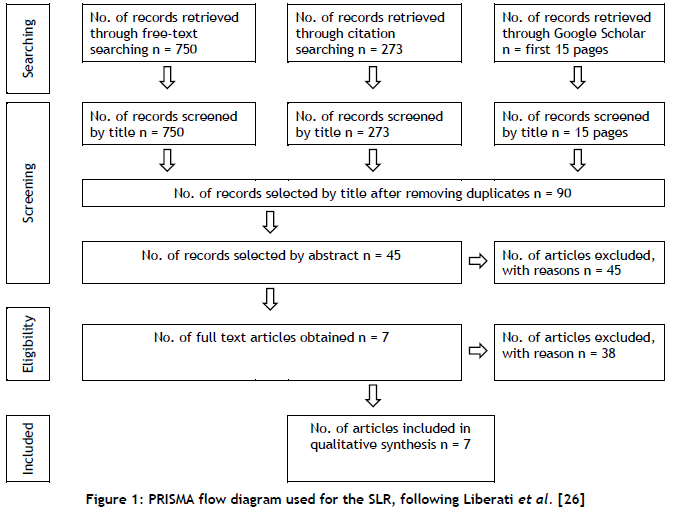
A PRISMA framework, shown in Figure 1, was used for this study. The four phrases that define the research purpose were used to search for relevant information. Synonyms were also used to extract as much information as possible. The following phrases and synonyms were used:
(a) FACTORS or (issues, causes, elements, components, aspects) AND
(b) SUSTAINABILITY or (sustainable, sustain, effective, effectiveness, successful)
AND
(c) LEAN or (Kaizen, improvement, 6-Sigma, 5S, Toyota Production Systems)
AND
(d) HEALTHCARE or (health, hospital)
This review only considered full-text academic journals and peer-reviewed articles written in English. It also only considered publications that are concerned with hospitals or sections of a hospital. However, the search term "healthcare" was used, as studies conducted in hospitals are often classified as healthcare in the literature. This review had no publication date restriction owing to the limited number of available articles.
3.1. Data search
The data search was done after consultation with the departmental librarian using EBSCOhost with the following databases: MEDLINE, Academic Search Complete, Directory of Open Access Journals, ScienceDirect, Business Source Complete, CINAHL with Text, Environment Complete, Health Source: Nursing/Academic Edition, Scopus, APA PsycInfo, Springer Nature Journals, Applied Science and Technology Source, Emerald Insight, Journals@OVID, ScIELO, SPORTDiscus with Full Text, JSTOR Journals, Directory of Open Access Books, GreenFILE, MasterFILE Premier, IEEE Xplore Digital Library, and Library Information Science & Technology Abstracts. The search phrases (with their synonyms and equivalent expanders) "Lean" and "Healthcare" were used in the title search, and "Factors" and "Sustainability" were used in the abstract search. 750 articles were identified for screening. A further search was done on Google Scholar using the search phrases where only the first 15 pages were screened. For exhaustive search purposes, Google Scholar was also used for a forward search (articles citing the reviewed articles) and a backward search (articles cited by the reviewed articles), from which 273 articles were selected for screening.
3.2. Exclusions
Identified articles were further screened using the title, and those not related to Lean and healthcare or hospital were excluded, with 90 articles remaining to be screened by abstract. After reading the abstracts to determine whether the articles included factors related to sustainability, 45 articles were chosen for full-text reading. Of these 45 articles, 38 were excluded because they were not specific to Lean or focused on the implementation stage without mentioning any sustainability factors. Seven final articles were selected for full review, as illustrated in Figure 1.
3.3. Analysis
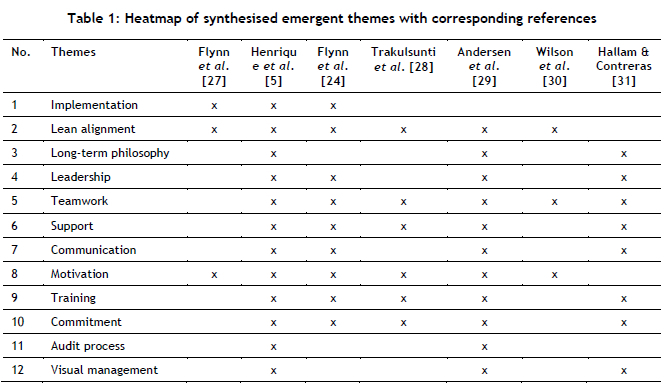
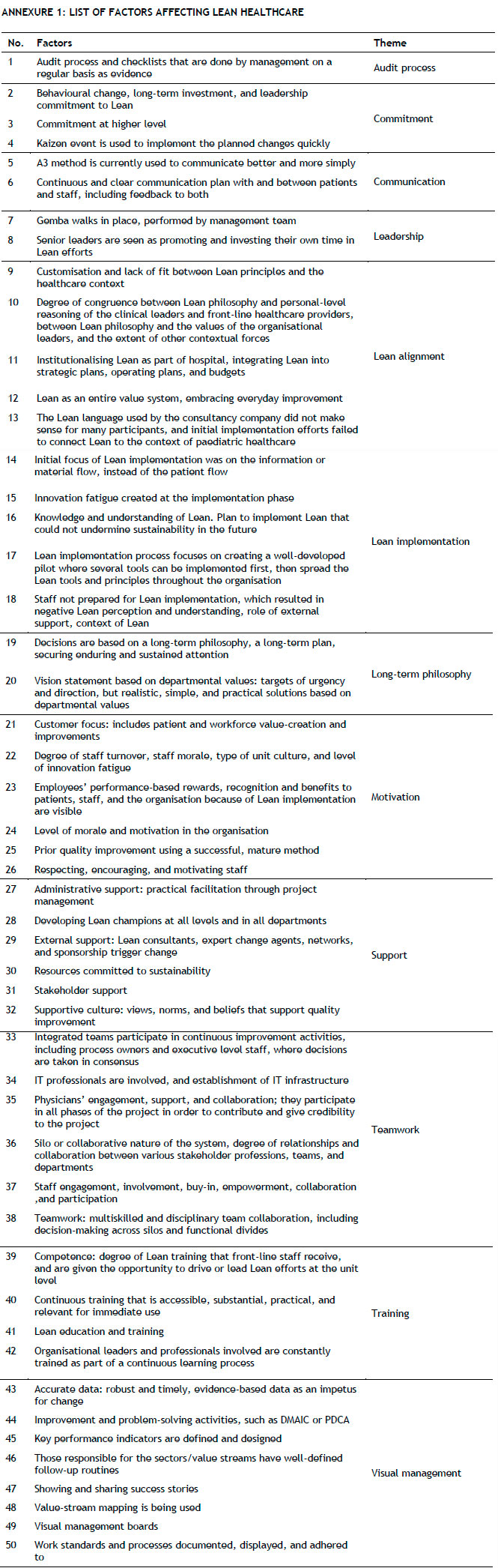
From the seven articles reviewed, 119 fact statements for Lean sustainability were extracted and synthesised in accordance with meta-synthesis. The language and terminology of 119 fact statements were matched, and 50 factors were identified; these are presented in Table 2 in Annexure 1. The 50 factors were consolidated into 12 distinct themes, as shown in Table 1. Themes were derived from the subject matter that factors were addressing or sought to address. These themes will be briefly discussed in the results section that follows.
4. RESULTS
The results show the need for the holistic implementation of Lean healthcare with sustainability in mind. Several authors highlight the need for Lean to be adapted so that it makes sense to healthcare workers. The complexities and rigidity of hospitals are also highlighted as barriers to Lean sustainability. The themes were chosen to unpack and show how the concept of sustainability can be linked to Lean philosophy and principles, people, and organisations. The themes are discussed individually in this section, but are brought together in the discussion section.
4.1. Implementation
This study identified implementation as a key driver of sustainability. If implementation is not done thoroughly with sustainability as the end goal, then sustainability cannot be achieved. Flynn et al. [27] mentioned that their interviews primarily illustrated how the nature, approach, processes, and outcomes of implementation phase shape the sustainability of Lean efforts.
The main issues found during implementation are adapting Lean language to the healthcare context, and preparation for a cultural mindset change that prepares the team so that they know what to expect and are able to accept and welcome the introduction of Lean. The approach and initial relationship between external consultants and staff plays a big role during implementation, as does the introduction of different disciplines working together as a team. The implementation phase also supports the other themes identified in Table 1, forming the foundation for sustainability as the outcomes shift to become the context for the sustainability phase [24].
4.2. Lean alignment
Lean alignment addresses the philosophy and culture of Lean, in terms of which Lean needs to be institutionalised in all activities, visions, and strategies of the organisation. Lean alignment issues identified from the review included the adaptation of Lean to a hospital context so that it makes sense to healthcare workers. It also included not only aligning Lean with healthcare but also aligning the healthcare organisation with Lean. To support this, Trakulsunti et al. [28] mentioned that institutionalising Lean is a key factor that can sustain the organisational culture approach. Flynn et al. [24] added that "the degree of success or failure in the sustainment of Lean efforts relies on the ways in which people make sense of Lean, align their values and the values of the organisation to the values of Lean".
4.3. Long-term philosophy
This study revealed that the presence of a long-term philosophy was a key contributor to the sustainability of Lean. The literature review highlighted continuous improvement as one of the basic principles of Lean. 'Continuous' here means that Lean is a long-term philosophy and vice versa: a long-term plan supports a continuous improvement approach [29]. A long-term philosophy, therefore, needs to align visions and future strategies with Lean and, by extension, continuous improvement. In expressing their support for this, Henrique et al. [5] concluded that organisational "decisions should be based on a long-term philosophy, even to the detriment of short-term financial losses, in order to help to establish a culture of continuous improvement and make employees more confident about the organisation's strategic alignment".
4.4. Leadership
Respect for people is one of the basic pillars of Lean, and includes the development of leaders who understand Lean and teach it to others. 13 of the 18 articles reviewed by Andersen et al. [29] identified management and leadership engagement as important for Lean sustainability. Management engagement includes maintaining urgency and expectations, giving direction, and making resources available [29]. Trakulsunti et al. [28] added that long-term leadership commitment and buy-in are key factors for sustaining Lean, even when previous Lean leaders leave the organisation. Leadership factors further identified in this study included the day-to-day involvement of management in continuous improvement activities, prioritising Lean initiatives, and management going where things happen to see for themselves.
4.5. Teamwork
Teamwork also falls under respect for people as a basic pillar of Lean, and has been identified by this study as a contributor to the sustainability of Lean in hospitals. As Flynn et al. [24] stated, "engaging healthcare professionals in designing, overseeing, and managing their own processes and opening new lines of communication through the hospital hierarchy is a contributor to the sustainability of Lean efforts". The role played by physicians as clinical leaders and role models to others is a very important factor for teamwork, as shown by Andersen et al. [29] in their findings that physicians' involvement, engagement, and collaboration are important at the strategic level. This study also revealed the importance of involving information technology (IT) professionals when improving activities and simplifying and automating complex processes [5].
4.6. Support
A supportive culture provides employees with a conducive environment in which to express their skills and creativity, take the initiative, explore, and deliver results [29]. Support includes sufficient resources being made available to sustain Lean efforts, and including financial, IT systems, and staff time in activities [29]. Support also includes the availability of internal and external Lean champions who are dedicated to Lean implementation and helping all staff members. The presence of effective support means that gaps can be identified and resources allocated to close these gaps. This enables employees to implement Lean without fearing failure.
4.7. Communication
This study revealed that communication has a compelling impact on the sustainability of Lean in hospitals. In the literature review section, inter- and intra-departmental communication was identified as one of the cultural challenges to be faced to achieve Lean sustainability. Clear, methodological, accurate, open, and timely communication provides a substantial boost to the sustainability of Lean. Opening new lines of communication and interaction between hierarchy levels is also essential. Visual management, a separately identified theme of this study, becomes a strong enabler of communication.
4.8. Motivation
Motivation also emerged as an important factor. Motivation can be positive or negative, depending on the actions, events, circumstances, and situations. As mentioned by Trakulsunti et al. [28], motivation can be harnessed by sharing Lean success stories and introducing reward and recognition programmes. Motivation factors also include making the benefits of Lean visible to the organisation, staff, and patients. Nurturing the morale and motivation of staff also aligns with the respect for people pillar.
4.9. Training
Becoming a learning organisation is one of the enablers of Lean that allows for a space that promotes problem-solving. Training was identified as an important contributor to the sustainability of Lean in hospitals, as it facilitates the sharing of knowledge and the development of a shared understanding among staff and management [30]. The implementation of Lean should start with training to introduce Lean and communicate the what, where, and how of the implementation process. Training can also break any existing perceptions in the organisation. Periodic Lean refresher training sessions are also important to update and reinforce Lean knowledge and skills [28]. Continuous training also addresses knowledge that gets eroded by staff movement or loss [26]. Training should include the philosophy of Lean thinking [5] and training in methods and tools to strengthen technical capability [29].
4.10. Commitment
'Commitment' refers to the dedication that an organisation and its people must have to their Lean journey. Commitment needs to include resources, time, personnel, management, and leadership. This commitment needs to extend to the overarching Lean philosophy, Lean principles, and the enabling tools and techniques. Trakulsunti et al. [28] mentioned that ensuring the daily use of Lean methodologies to solve problems and to improve requires "behavioural change, long-term investment, and commitment to Lean".
4.11. Audit process
Although not mentioned frequently in the reviewed articles, the importance of an audit process cannot be overstated. Henrique et al. [5], in their findings, mentioned the need for an audit process and for checklists to be done by management after Kaizen events to ensure that improvements are implemented and work standards are adhered to. Regularly conducted audits and measurements also build structural capability, which strengthens the evidence for the success of Lean interventions [29].
4.12. Visual management
Visual management is identified in this study as a contributor to the sustainability of Lean. Strategy, goals to be achieved, performance indicators, results, and value stream maps should be displayed on visual management boards [5], which would help to track work processes and display standard working procedures and performance. Visual management is a useful tool that enables the identification of issues or waste, and facilitates problem-solving. Visual management is also a great tool for communication, because information is readily available at all times. Hallam and Contreras [22] mentioned that documenting and visually communicating standard work ensures that changes stay in place.
5. DISCUSSION
Lean is defined as a philosophy and as a set of principles and tools that enable organisations to identify and eliminate waste in order to create value for customers. The application of Lean depends on different disciplines, sections, or departments in the organisation. Systems, mindset, culture, structure, understanding, know-how, resources, and focus are but some of the sustainability requirements that depend on the organisation. These support the kind of organisational readiness that enables the sustainability of Lean in healthcare.
The implementation theme is the starting point or input for the sustainability of Lean in healthcare. The quality and success achieved during implementation pave the way for continuous improvement and sustainability. The implementation phase, therefore, acts as the foundation and determinant of either success or failure.
The Lean alignment, long-term philosophy, and training themes are the basic principles of Lean that promote understanding, knowledge accumulation, and capacity development in the organisation. They promote the correct interpretation and adaption of Lean to suit the healthcare context. They also talk about the compatibility between Lean and healthcare organisations and the importance of a relationship that should be matched to reap the rewards of sustainability.
The leadership and teamwork themes bolster the notion of people as one of the basic pillars of Lean. The identified factors emphasise the quality, competence, and calibre of people in the organisation, both management and staff. These themes elaborate on the roles and responsibilities of people to achieve sustainability.
Motivation is a consequence of the people factors that are induced by what is happening and how it is happening. The factors for motivation make it clear that employees want to see results and want to be rewarded, praised, and congratulated. Employees also want their efforts to be meaningful and valuable in the workplace. The presence of visible success and added value has a positive impact on motivation and, ultimately, sustainability.
The themes of support, communication, commitment, and visual management refer to the state of the organisation, including its people. These are the conditions that an organisation must put in place, acquire, or make available to achieve sustainability. These themes represent the organisational contribution to accommodating Lean implementation and propelling implementation into sustainability.
The audit process is the final action process that monitors, assesses, and evaluates the process of implementation, the application of Lean, the state of the organisation, and the results of the relationship between Lean, people, and organisation.
6. CONCLUSIONS AND RECOMMENDATIONS FOR FURTHER WORK
It is clear from the factors identified in this study that the sustainability of Lean in hospitals requires a well-planned implementation with sustainability in mind, where the goals and strategies are long-term and aligned with Lean thinking. These Lean-aligned goals and strategies should be communicated holistically to the entire organisation. This study found that sustainability requires a committed leadership that leads by example and integrates with the rest of the team to create a conducive work environment and strong teamwork; a committed leadership that goes where things are happening and continually audits all of the necessary processes. It is also found that an engaged and continually trained team that is given all the support it needs will always be motivated and committed to the sustainability of Lean in healthcare. This study has also shown that an open and transparent work environment in which all work standards, key performance indicators, expectations, and rewards are communicated and visually displayed for all to see is a catalyst for sustainability.
Given the shortage of empirical data on sustainability, we recommend further practical studies that explore the factors affecting the sustainability of Lean in healthcare in real settings. We also recommend studies on organisational readiness as an interdisciplinary concept for Lean implementation. Furthermore, there is a need for longitudinal studies to be conducted over four or more years after Lean implementation, in which data could be sourced from staff who joined the organisation after implementation so that their contribution is not influenced by the initial implementation phase.
7. CONTRIBUTION OF THE STUDY
From this SLR, we show that, even though Lean has been adopted by and adapted to healthcare, there often remains the question whether the adaptation has been done correctly and holistically. We show that, even though there has been growth in the understanding of Lean implementation in healthcare, organisational readiness and inter-disciplinarity are not understood as well as they should be. We further show a lack of empirical research on the sustainability of Lean healthcare, as most of the reviewed articles present secondary information instead of primary data. The information and factors identified by this study will be used in the main study to shape interview questions and inform the analysis of the interview results.
If Lean concepts and approaches are to have a positive impact on the healthcare system in South Africa, an understanding of how to gain the most sustainable value is needed. This study makes a contribution by highlighting key factors that should be considered by researchers and practitioners when considering and evaluating Lean interventions. The second part of the study will aim to explore the current challenges experienced in South African hospital settings when applying and implementing Lean thinking. It is hoped that this will highlight contextual nuances and contribute to a better understanding of how Lean could be used successfully and sustainably to make a positive impact on healthcare in South Africa.
REFERENCES
[1] Y. Daultani, A. Chaudhuri, & S. Kumar, "A decade of lean in healthcare: Current state and future directions," Global Business Review, vol. 16, no. 6, pp. 1082-1099, 2015. [ Links ]
[2] J. Moraros, M. Lemstra, & C. Nwankwo, "Lean interventions in healthcare: Do they actually work? A systematic literature review," International Journal for Quality in Health Care, vol. 28, no. 2, pp. 150-165, 2016. [ Links ]
[3] J. J. Dahlgaard & S. M. Dahlgaard-Park, "Lean production, six sigma quality, TQM and company culture," The TQM magazine, vol. 18, pp. 263-281, 2006. [ Links ]
[4] A. Erthal, M. Frangeskou, & L. Marques, "Cultural tensions in lean healthcare implementation: A paradox theory lens," International Journal of Production Economics, vol. 233, 107968, 2021. [ Links ]
[5] D. B. Henrique, M. G. Filho, G. Marodin, A. B. L. de S. Jabbour, & C. J. Chiappetta Jabbour, "A framework to assess sustaining continuous improvement in lean healthcare," International Journal of Production Research, vol. 59, no. 10, pp. 2885-2904, 2021. [ Links ]
[6] J. P. Womack, D. T. Jones, & D. Roos, The machine that changed the world. New York: Rawson Associates, 1990. [ Links ]
[7] A. R. Fleiszer, S. E. Semenic, J. A. Ritchie, M.-C. Richer, & J.-L. Denis, "The sustainability of healthcare innovations: A concept analysis", Journal of Advanced Nursing, vol. 71, no. 7, pp. 14841498, 2015. [ Links ]
[8] S. F. Schell, et al., "Public health program capacity for sustainability: A new framework," Implementation Science, vol. 8, no. 1, pp. 1 -9, 2013. [ Links ]
[9] W. T. Maphumulo & B. R. Bhengu, "Challenges of quality improvement in the healthcare of South Africa post-apartheid: A critical review", Curationis, vol. 42, no. 1, pp. 1-9, 2019. [ Links ]
[10] D. J. Kruger, "Lean implementation in the Gauteng public health sector," in Proceedings of PICMET14 Conference: Portland International Center for Management of Engineering and Technology; Infrastructure and Service Integration, 2014, pp. 2699-2708. [ Links ]
[11] J. Price, "Lean management in the South African public health sector: A case study", South African Health Review, vol. 2013, no. 1, pp. 191-199, 2013. [ Links ]
[12] M. Mutingi, R. Monageng, & C. Mbohwa, "Lean healthcare implementation in Southern Africa: A SWOT analysis," in Proceedings of the World Congress on Engineering, vol. 2, pp. 866-869, 2015. [ Links ]
[13] D. Arfmann & G. T. Barbe, "The value of lean in the service sector: A critique of theory & practice," International Journal of Business and Social Science, vol. 5, no. 2, pp. 18-24, 2014. [ Links ]
[14] R. Ciarnienè & M. Vienazindienè, "Lean manufacturing: Theory and practice," Economics and Management, vol. 17, no. 2, pp. 726-732, 2012. [ Links ]
[15] M. Graban & J. Toussaint, Lean hospitals: Improving quality, patient safety, and employee engagement. Productivity Press, New York, 2018. [ Links ]
[16] F. Pakdil, T. N. Harwood, & F. B. Isin, "Implementing lean principles in the healthcare industry: A theoretical and practical overview," in Delivering Superior Health and Wellness Management with IoT and Analytics, Nilmini Wickramasinghe and Freimut Bodendorf, Springer, pp. 383-413, 2020. [ Links ]
[17] J. P. Womack & D. T. Jones, "Beyond Toyota: How to root out waste and pursue perfection," Harvard Business Review, vol. 74, no. 5, pp. 140-151, 1996. [ Links ]
[18] D. K. Sobek & M. Lang, "Lean healthcare: Current state and future directions," in Proceedings of the 2010 Industrial Engineering Research Conference, vol. 5, pp. 1 -6, 2010. [ Links ]
[19] G. S. Spagnol, L. L. Min, & D. Newbold, "Lean principles in healthcare: An overview of challenges and improvements", IFAC Proceedings Volumes, vol. 46, no. 24, pp. 229-234, 2013. [ Links ]
[20] T. Naik, et al., "A structured approach to transforming a large public hospital emergency department via lean methodologies," Journal for Healthcare Quality, vol. 34, no. 2, pp. 86-97, 2012. [ Links ]
[21] J. J. Dahlgaard, J. Pettersen, & S. M. Dahlgaard-Park, "Quality and lean health care: A system for assessing and improving the health of healthcare organisations," Total Quality Management & Business Excellence, vol. 22, no. 6, pp. 673-689, 2011. [ Links ]
[22] Z. Radnor & R. Boaden, Lean in public services - panacea or paradox? London: Taylor & Francis, 2008, doi:10.1111/j.1467-9302.2008.00610.x [ Links ]
[23] Z. J. Radnor, M. Holweg, & J. Waring, "Lean in healthcare: The unfilled promise?" Social Science & Medicine, vol. 74, no. 3, pp. 364-371, 2012. [ Links ]
[24] R. Flynn, et al., "The sustainability of lean in pediatric healthcare: A realist review". Syst Rev 7, 137, 2018. Doi: 10.1186/s13643-018-0800-z [ Links ]
[25] A. D'Andreamatteo, L. lanni, F. Lega, & M. Sargiacomo, "Lean in healthcare: A comprehensive review," Health Policy, vol. 119, no. 9, pp. 1197-1209, 2015. [ Links ]
[26] A. Liberati et al., "The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration," PLoS Medicine, 6(7):1-28, 2009. [ Links ]
[27] R. Flynn, T. Rotter, D. Hartfield, A. S. Newton, & S. D. Scott, "A realist evaluation to identify contexts and mechanisms that enabled and hindered implementation and had an effect on sustainability of a lean intervention in paediatric healthcare," BMC Health Services Research, vol. 19, no. 1, pp. 1-12, 2019. [ Links ]
[28] Y. Trakulsunti, J. Antony, & J. A. Douglas, "Lean Six Sigma implementation and sustainability roadmap for reducing medication errors in hospitals," The TQM Journal, vol. 33 no. 1, pp. 33-55, 2020. [ Links ]
[29] H. Andersen, K. A. Rovik, & T. Ingebrigtsen, "Lean thinking in hospitals: Is there a cure for the absence of evidence? A systematic review of reviews," BMJ Open, vol. 4, no. 1, e003873, 2014. [ Links ]
[30] W. J. Wilson, N. Jayamaha, & G. Frater, "The effect of contextual factors on quality improvement success in a lean-driven New Zealand healthcare environment," International Journal of Lean Six Sigma, vol. 9, no. 2, pp. 199-220, Jan. 2018, doi: 10.1108/IJLSS-03-2017-0022. [ Links ]
[31] C. R. Hallam & C. Contreras, "Lean healthcare: Scale, scope and sustainability," International Journal of Health Care Quality Assurance, Vol. 31 Issue: 7, pp.684-696, 2018. [ Links ]
* Corresponding author: sfisow@gmail.com
ORCID® identifiers
R.S. Wagner: 0000-0002-3839-2420
T.S. Hattingh: 0000-0001-5930-2546
H. Meijer: 0000-0002-0105-257X



{kind=link}
{kind=link}
{kind=link}