










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Industrial Engineering
On-line version ISSN 2224-7890
Print version ISSN 1012-277X
S. Afr. J. Ind. Eng. vol.33 n.2 Pretoria Jul. 2022
http://dx.doi.org/10.7166/33-2-2598
GENERAL ARTICLES
Short-term impacts of mobile touch-screen device use on musculoskeletal disorders during Covid-19 pandemic: risk assessment modelling and verification
A. ElghomatiI, *; O. KorhanI; B. SekerogluII; K. DogruyolIII
IDepartment of Industrial Engineering, Eastern Mediterranean University, 99628 Famagusta, Cyprus, TR, Mersin 10, Turkey
IIDepartment of Computer Engineering, Near East University, 99138, Nicosia, Cyprus, TR, Mersin 10, Turkey
IIIDepartment of Business Administration, Faculty of Economic and Administration Sciences, Cyprus International University, 99040, Nicosia, Cyprus, TR, Mersin 10, Turkey
ABSTRACT
The intensive and repetitive use of touch-screens may pose significant problems, such as ergonomic pain or musculoskeletal disorders. This research aims to study the effect of using mobile touch-screen devices on the human musculoskeletal system during the COVID-19 pandemic lockdown and to develop a model for classifying the effects of musculoskeletal stress (pain and discomfort) on the performance of educational activities. The Cornell musculoskeletal discomfort questionnaire was given to 544 participants (71% males and 29% females). An Association Rule Mining approach was applied to illustrate the correlation, and multiple machine-learning models - used to predict the impact of pain and discomfort on different body regions - were applied to determine risk levels that might interfere with the ability to perform daily activities. Most musculoskeletal disorders were reported in the neck region and lower back (64.33% and 55.33% respectively), followed by upper back (44.30%) and the right shoulder (38%). Analysis of association rules showed high positive correlation between the lower back and the neck (support = 43%, confidence = 77%). Additionally, it was found that the radial basis function network has the highest accuracy in prediction (84%). The results of the radial basis function model showed that interference in educational activities can be predicted by using pain indicators in body parts resulting from touchscreen device usage.
OPSOMMING
Die intensiewe en herhalende gebruik van raakskerms kan hewige probleme veroorsaak soos ergonomiese pyn of muskuloskeletale afwykings. Hierdie navorsing se doel is om die effek van die gebruik van mobiele raakskermtoestelle op die menslike muskuloskeletale stelsel tydens die COVID-19 pandemie inperking te bestudeer en om 'n model te ontwikkel vir die klassifikasie van die invloed van muskuloskeletale stres (pyn en ongemak) op opvoedkundige aktiwiteite. Die Cornell muskuloskeletale ongemakvraelys is aan 544 deelnemers gegee (71% mans en 29% vroue). Assosiasie Reel Ontginning benadering is toegepas om die korrelasie te illustreer en veelvuldige masjienleermodelle - wat gebruik word om die impak van pyn en ongemak op verskillende liggaamstreke te voorspel - is toegepas om risiko-vlakke te bepaal wat kan inmeng met die vermoe van daaglikse aktiwiteite uitvoer. Die meeste muskuloskeletale afwykings is in die nekstreek en laerug (64.33% en 55.33% onderskeidelik) aangemeld, gevolg deur bo-rug (44.30%) en die regterskouer (38%). Ontleding van assosiasie reels het hoe positiewe korrelasie tussen die lae rug en die nek getoon (ondersteuning = 43%, selfvertroue = 77%). Daar is ook gevind dat die radiale basisfunksienetwerk die hoogste akkuraatheid in voorspelling het (84%). Die resultate van die radiale basis funksie model het getoon dat inmenging in opvoedkundige aktiwiteite voorspel kan word deur pynaanwysers in liggaamsdele te gebruik wat ontstaan uit die gebruik van aanraakskermtoestelle.
1 INTRODUCTION
In today's digital age, contemporary technology has become a regular part of people's realities and experiences. The use of electronic devices, especially touch screens, smartphones, and tablets, continues to increase as a result of the technological revolution in the information era for both occupational and leisure activities. The use of mobile touch-screen devices (MTSDs) is somewhat different from that of conventional electronic devices. This is because MTSDs tend to be smaller and easier to handle, making it possible for them to be used in various non-traditional workstations and postures where a monitor, keyboard, and mouse could not be used [1, 2].
Interestingly, a large majority of millennials are users of mobile devices [3]. Worldwide, ownership of these devices is expected to reach 3.8 billion by 2021 [4]. In recent years, the surface of mobile touch-screen devices has provided users with a large display screen with few physical keys [5]. As the designs have improved and functions diversified, many people have become addicted to their use. Some of the consequences of this addiction include irresistibility and a lack of self-control when using mobile touchscreen devices [6]. For example, MTSDs can be used while lying on the couch or riding on public transportation rather than in the traditional way of sitting in a chair and placing the device on a desk at home or at work. These new postures cause different musculoskeletal risks with neck flexion [1]. Moreover, the usage of mobile touch-screen devices is related to weaker hand-grip and pinch-grip [7].
Many schools and universities worldwide were closed at the beginning of the COVID-19 pandemic, which negatively affected around 1.37 billion learners around the world [8]. Educational institutions were thus obliged to resort to online education as an alternative to the traditional model. University students use mobile touch-screen devices in their daily activities, such as communication, social media, health tracking, etc. Wallace, Clark and White [9] confirm that university students use MTSD for daily activities to access text books (70 per cent), medical podcasts (60 per cent), medical calculators (75 per cent), and online lectures (50 per cent), and to take notes (45 per cent). The three main daily activities in which MTSDs were used by students were related to recreation (82.5 per cent), communication (81.7 per cent), and educational purposes (62.7 per cent) [10]. The pandemic forced students to increase the time they spent on their gadgets, as they changed from being merely social communication tools to becoming essential educational tools [11]. Thus they have become more exposed to musculoskeletal disorders, which interfere with their ability to perform daily activities.
A cross-sectional study of musculoskeletal disorders (MSD) and online education was undertaken during the pandemic. The participants of the study were 261 undergraduate students in an Indian university who responded to an online questionnaire about the pain they experienced as a result of online education. The findings revealed that 80 per cent of the participants experienced pain in the head, eyes, and neck. The study also found that two other areas experienced pain: the right shoulder and the right-hand fingers (58 per cent and 56 per cent respectively). In addition, 40 per cent of the participants reported experiencing pain in all of their body parts as a consequence of the new study mode [12].
Although smartphones offer numerous advantages, their use can increase the risks of musculoskeletal injury and discomfort [13,14]. In a recent systematic review by Legan and Zupan [15], in which the researchers identified the prevalence of mobile-device-related discomfort in the lower extremities, they found that the prevalence of musculoskeletal discomfort ranged from 0.4 per cent to 73 per cent among users. According to a comprehensive review, the spread of musculoskeletal problems among users was reported to be between 1 per cent and 67.8 per cent, of which neck complaints were the highest at between 17 per cent and 68 per cent [16].
In another survey of pain in university students due to the usage of smartphones, the results revealed that 54.4 per cent of students experience pain in four areas of their body: their neck, shoulders, and upper and lower back [17]. Suwalee,Rungthip,Manida Swangnetr and Rose [18] performed an analysis of Khon Kaen University undergraduate students who used smartphones; their findings showed that the most painful region was the neck (up to 32.5 per cent) because of the effects of increased neck flexion. Another study investigated the significance of neck kinematics and muscle activities during the operation of touch-screens and smartphones. The study found a single significant effect from the use of these devices. Although it was at lower levels, neck muscle activities resulted in more occurrence of pain while performing a reading task and holding the device in the hand [19].
Along with the ergonomic effects on users, other studies have shown that multiple factors - physical factors such as screen size, configuration, and keyboard design; task-related factors such as typing strategies and the standing or sitting posture; user factors including gender, age, and musculoskeletal condition [14,2022]; and personal habit factors such as smoking - are also related to the occurrence of MSD [18]. A study conducted with 292 university students indicated that back pain had a positive correlation with the size of the LCD screen, while pain in the legs and feet had a negative correlation with the period of smartphone use. Most of the musculoskeletal symptoms occurred mainly in the neck and shoulder region, and were reported to be prevalent among 56 per cent of MTSD users [23]. A recent study of 249 university students found that the prevalence of musculoskeletal pain in neck, shoulder, wrist/hand, and upper back was higher among females than among males [24].
For MTSD users, most recommendations that address neck disorders emphasise reducing the flexed-neck posture, smoking less [18], or reducing biomechanical loading in the neck region as remedies [25]. In addition, to prevent the occurrence of discomfort, especially in the back, a person should maintain a correct posture and take breaks when performing tasks [26].
A systematic review of the ergonomic and stress-related literature by Toh,Coenen,Howie, and Straker [2] highlighted the need for scholars to investigate the relationship between the increasing number of touchscreen device users and the surge in the occurrence of MSDs. The results of preliminary studies showed that complaints about musculoskeletal disorders in the neck, back, shoulders, and lower extremities have been increasing alongside the growing MTSD use. These increase the risk of musculoskeletal stress (pain and discomfort) in performing educational activities. In most cases, these require medical treatment and rest, resulting in time loss, low performance, and health care costs.
The participants in this study were university students. Therefore, it was speculated that a large part of their daily activities was related to education and several other auxiliary activities. Given the pervasive use of MTSDs in most aspects of human life, and that this is a global phenomenon, the premise of this study could be considered purposeful and relevant to the current context and time. More importantly, in general those who use mobile hand-held devices are exposed to symptoms of musculoskeletal disorder (MSD) in their necks and upper limbs during their activities of daily living (ADL), and that these symptoms interfere with their ability to perform educational activities. Moreover, MSD symptoms also interfere with ADL abilities. The Covid-19 pandemic has shifted education to online media at every level. University students were the focus of this study to identify their experiences on mobile touch-screen device use for online education during the Covid-19 pandemic. This study aimed to reveal the impact of mobile touch-screen device use on musculoskeletal disorders for educational purposes during the Covid-19 pandemic. The effects of this interference on the performance of ADL, as with education, are not clear in the literature. Therefore, there is a need for further studies in this area. There is also a need for a model to predict the risk levels of MSD in users of mobile touch-screen devices, since they can have such detrimental outcomes.
Owing to the spread of artificial neural networks (ANNs) and machine-learning (ML) algorithms, there have been many different approaches to their application, such as the artificial neural network-based approach, the robotics telecommunication approach, the entertainment approach, and medical applications. Haung,Lan,Thomson, Fang,Hoffmann and Lacey [27] considered ANNs to be the newest technology for processing the data of toolboxes devoted to engineering applications. Somers [28] suggested that ANNs have greater accuracy than conventional statistical analysis. ANNs even have the ability to deal with nonlinear relationships and to check data. Other similar studies considered ANNs to be more insightful in providing thorough and more accurate results than normal statistical methods [29,30]. On the other hand, various studies indicated that machine-learning algorithms were more insightful in providing thorough results that are more accurate in predictive modelling. Bosman, Roelen, Twisk, Eekhout and Heymans [31] applied machine-learning algorithms to predict the risk of sick leave as a result of musculoskeletal disorders, and Sasikumar and Binoosh [32] suggested that machine-learning algorithms predict the risk of musculoskeletal disorders with the greatest accuracy.
This research adopted the association rule mining (ARM) approach and a machine-learning algorithm to increase the chance of a more accurate prediction of pain or discomfort and its associated interference with daily activities. Prediction methods in machine-learning algorithms and data-mining approaches are still lacking in the MTSD field. The proposed model could be used in an organisation to predict whether there would be interference with MTSD users' educational performance.
The contribution of this study is to predicting the risk of muscularskeletal (MSK) stress (pain and discomfort) from MTSD usage that then result in MSDs, and to defining a classification of risk levels for interference with the ability to perform educational activities. The importance of developing a model to predict the risk of MSDs is the fact that, in cases of risky behaviour by MTSD users, the interference of pain levels increases their risk of underperforming ADL.
2 METHODS
2.1 Participants
In order to calculate the number of study participants, the Yamane formula [33] with a 95 per cent confidence level and a five per cent sampling error was used. The required sample size was found to be 394 respondents; questionnaires were distributed to 600 participants at the Eastern Mediterranean University (EMU) in the Turkish Republic of Northern Cyprus. Data collection took place between 1 and 22 October 2020. However, 56 participants did not complete the questionnaire; while participants with confirmed medical conditions of severe pain or discomfort in the neck and the upper and lower extremities, and those that had been diagnosed with osteoarthritis, were excluded from the study. Most of the participants were male (71 per cent), and the rest self-identified as female (29 per cent).
2.2 Study design and procedure
A questionnaire was used to ask about MSDs in the neck and the upper and lower extremities, which included shoulders, upper and lower back, arms, forearms, hands and wrists, buttocks, thighs, knees, and lower legs. The questionnaire was designed to exclude any forms of compromise or prejudice. However, researchers confirmed that all the participants were users of MTSDs (smartphones, tablets, smart watches, and similar devices). Owing to the Covid-19 pandemic, an online web-based questionnaire was directly and randomly administered to participants, who were invited by using the app Microsoft Teams.
2.3 Questionnaire description
The survey had two sections: participants' demographics, and questions about musculoskeletal pain or discomfort. The collected demographic information covered age, gender, smoking habits, right or left dominance, type of MTSD, posture, and how much time each day MTSDs were used. The questionnaire was adapted from the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) [34], a 54-item questionnaire addressing all body segments. The CMDQ included questions about aches, pains, and musculoskeletal discomfort that respondents had experienced within the previous week while using touch-screen devices. The CMDQ covered questions about eleven different regions of the body's upper and lower extremities (neck, shoulders, upper back, upper arms, lower back, forearms, hands and wrists, hips and buttocks, thighs, knees, and lower legs). The questions were grouped into three columns: (i) frequency (never, 1-2 times per week, 3-4 times per week, once per day, and several times per day); (ii) level of discomfort (slight, moderate, and very uncomfortable); and (iii) interference with the ability to work or engage in educational activities (not at all, slightly, and substantially interfered).
The internal consistency of the CMDQ was examined by the authors during the course of the study, and the results showed that all of the questions were valid, with Cronbach's alpha found to be 0.975 for 54 items. The reliability and validity of the CMDQ were also examined by Dr Oguzhan Erdinc [34] in Turkey. To ensure its feasibility and comprehensibility for participants, piloting was conducted using 10 per cent of the sample size, for which the responses of 60 participants were considered. After obtaining feedback from the pilot study's respondents, the format of the questionnaire was amended slightly to ensure that the questions were understandable and clear.
2.4 Data analysis
2.4.1 Statistical analysis
Descriptive statistics were obtained for MTSD users and musculoskeletal disorders. The collected data were entered into and analysed using the Statistical Package for the Social Sciences (SPSS) version 22.0. The mean age and gender ratios of the respondents were calculated. The body regions of the respondents where physical discomforts were frequently experienced were identified. In addition, binary logistic regression was used to determine the risk assessment model, which shows the significant risk factors that contribute to the experience of physical discomfort among MTSDs users. The experience of physical discomfort was chosen as the dependent variable, which was a Boolean variable (yes/no). The other variables were regarded as independent variables, as stated in the questionnaire.
2.4.2 Machine learning algorithms
Association rule mining (ARM) was used via the apriori algorithm in the Python programming language to detect any relationship between the different parts of the body experiencing pain or discomfort. For this purpose, two approaches (mining patterns and assigning weights) were applied. The researchers defined the item sets of the mining patterns to determine the interval support for the threshold (0.20). Then the significant least pattern tree (SLP tree) was created using the items from the study. After that, the researchers generated the significant least pattern growth (SLP growth), which led to the significant factors of the study. The last stage of the analysis applied the correlations through association rules, which were derived from the lift equation (Equation 1 or Equation 2).

or

where
• A and B = item sets;
• Supp(B) = a number of transactions containing B;
• Conf = confidence that an association rule depicts the accuracy of the rule.
The lift equation was identified as the simplest correlational measure, in which > 1 means a positive correlation. Therefore, since A and B were dependent variables, the occurrence of one variable implied the occurrence of the other variable. This led to the discovery of the highly correlated least association rules [35].
Of course, the threshold of support and confidence are the constraints of the mining through association rules. Typically, the deformation of these concepts has become a subject of research, with many authors opining that thorough and expansive studies are needed to specify accurate values fairly. However, according to Olafsson, Li and Wu [36], each researcher has developed a set for which the values of the threshold of support and confidence can be valid. The use of the minimum threshold and confidence has been embraced by many authors. Given this fact, each author makes or specifies the minimum support and the minimum confidence that are relevant to their study, and sometimes that meet their preference. The idea is that, through the item set, the apriori algorithm could properly determine the mode and frequency of the item set in the database through inductive learning. Furthermore, Fan [37] argued that, although there are diverse positions on analysis involving the association rules, the values of the threshold of support and confidence depend absolutely on the researcher's objectives, interpretations, and applications of the research subject. This position had earlier been asserted by Kotsiantis and Kanellopoulos [38] - that the threshold of support and confidence are usually predefined by the users to avoid 'ambiguous' rules that would make the threshold too low or too high. For the sake of reliability, we have set min Supp to 20 per cent [36].
It should be noted that min Supp and min Conf are core indicators that are used mainly as inductive learning within the algorithm to decipher the mode and frequency of the item set within the database. In other words, it might be different from the proposition of Spearman correlation or others that are used mainly to determine the nature of the relationship(s) and the extent of such relationships that exist between variables (dependent and/or independent). Aside from the foregoing, this work is not built on the arguments of linear models, upon which most correlations are based. Again, in the application of association rules mining, the user's preferences are always uncorrelated, and so the predictive information hidden in the behavioural patterns would be useful for analysing and predicting customer behaviour [39]. We applied the ARM approach because it addresses the major drawbacks of the linear correlation approach - namely, the importance of the correlations by users is not captured, and articles cannot be the same under the correlation approach, even if they share the same interest, until the two users rate the articles the same [40].
Machine-learning (ML) algorithms were implemented to predict the impact of pain or discomfort on different body regions from MTSD usage and to define the risk levels for interference with the ability to perform daily activities. The risk levels of MSD that interfered with the ability to perform educational activities were categorised into three levels: low, medium, and high. The frequency of aches, pains, and discomfort in various body regions was input into the ML algorithms as 544 samples after data preprocessing. The CMDQ consisted of three parts and their occurrence in the previous week. The first part dealt with the frequency of aches, pains, and discomfort; the second part addressed the severity of the aches, pains, or discomfort; and the third part measured interference with the ability to perform daily activities. Ultimately, the second part was ignored in the experiments to provide the classification with the minimum number of input data for neural networks.
For the present study, first the sample data was collected. Then, even though it was not compulsory for inputs that have similar input ranges, minimum-maximum normalisation was applied to all of the input and output data for data preprocessing in order to reduce the computational time. Thus the minimum and maximum data values in the dataset were equalised to 0 and 1 respectively, and the data values that fell within the minimum and maximum range were scaled between 0 and 1. In addition, the hold-out method, which is based on dividing all data randomly into two sets for training and testing, was used during the training of all the ML models. The training set comprised 70 per cent of the total data, and the rest of the data was assigned to the test set. Subsequently, the sample data was tested using four different ML models: the support vector machine (SVM), the long-short-term memory (LSTM) neural network, the back-propagation (BP) neural network, and the radial basis function (RBF) neural network. Finally, model evaluation was performed using the prediction accuracies obtained for each model. The steps of the data analysis with respect to the machine-learning algorithms are illustrated in Figure 1.
The parameters for each ML algorithm were determined after several experiments, separately. The radialbasis function neural network has a constant hidden layer and uses radial-basis functions as activation functions. Therefore, the tuning of hyper-parameters was minimised, and optimal convergence was obtained. Eighteen hidden nodes were selected, and the number of maximum epochs, the number of clusters, and the learning rate were set as 3 000, 18, and 0.09 respectively. Concurrently, the radial-basis function kernel was used with gamma = 0.001 in SVM, and the architecture of BP consisted of four hidden layers with 500 hidden nodes for each layer. The maximum iteration was set to 250. Finally, LSTM was used with four LSTM layers; the maximum epoch number was set to 100. The 'Adam' optimiser was used for both BP and LSTM. The implementation of the ML models was performed using the Python programming language (v. 3.8.1 [R14]).
3 RESULTS
Table 1 presents the results of the questionnaire regarding the general characteristics of the participants. The majority (89.7 per cent) of them were between 17 and 33 years of age. The mean age of the participants was 24.6 years. The majority of the participants who owned MTSDs and were considered in the study were using smartphones (94.5 per cent), while only a few participants used tablets (5.5 per cent). Of those who used their MTSD for more than six hours a day, smartphone use accounted for 32.5 per cent, while the use of tablets was 1.8 per cent. Longer usage times imply a greater risk of MSK stress and symptoms.
The manner of holding their devices varied in the responses of the participants. Right-hand holding of smartphones and tablets was 58.1 per cent and 66.6 per cent respectively, while 34.4 per cent and 33.3 per cent respectively used both hands. The percentage of left-hand use was only 8.36 per cent for smartphones. A total of 35.8 per cent of the participants also had the habit of smoking, and 37 per cent of the participants had pain or discomfort in the neck region during the previous week. The majority of the participants who experienced pain or discomfort during the previous week used their MTSD either in sitting positions or while lying down on a sofa. Furthermore, 16.0 per cent of them held one posture (sitting), and 80.9 per cent had more than two postures (sitting and another posture).
A total of 544 questionnaires were retrieved at the end of the evaluation. This represented 90.6 per cent of the 600 participants. Of these, 386 participants were male (representing 71 per cent) and 158 were female (29 per cent). The results show that the participants (n = 544) experienced pain or discomfort in one or more body parts during the previous week, with a higher prevalence among males than among females. Table 2 shows the parts of the body where pain or discomfort was experienced during the previous week because of the use of MTSDs, and which body parts had the highest frequency of pain or discomfort. The results reveal that 350 of the participants (64 per cent) reported pain or discomfort in the neck region; 257 were males (73.4 per cent) and 93 were females (26.6 per cent). Furthermore, 301 (55.3 per cent) reported pain or discomfort in the lower back; they were 220 males (73.4 per cent) and 81 females (26.4 per cent). At the upper back, 241 (44.3 per cent) of the participants experienced pain, of whom 177 were males (73.4 per cent) and 64 were females (26.6 per cent). On average, from Table 2, 73.3 per cent of the males and 26.6 per cent of the female participants experienced pain or discomfort in the neck and the upper and lower extremities.
The last notable result was pain or discomfort in the right shoulder, which was reported by 37.5 per cent of the whole population (145 males and 59 females). Pain or discomfort frequency in other body parts varied between 28 per cent (left shoulder or right hand and wrist) and 12.5 per cent (left forearm).
Table 3 presents the ARM results for the various body parts in which respondents experienced pain or discomfort; these results are based on the support and confidence values, which are higher than the threshold value of 20 per cent. 'Support of antecedent' represents the first body part, while 'Support of consequence' represents the second body part. Consequently, 'Support of item set' represents the percentage of the positive relationship between antecedent and consequence. 'Confidence', conversely, signifies the percentage of the pain or discomfort in the consequence when the item set is available. The 'Lift' column gives values for the areas that have a positive relationship. When the lift is 1 or more, there is a positive relation between the associated body parts.
The ARM approach has shown that a positive correlation of body regions exists for the neck and the upper limbs. Similarly, pain or discomfort in the back, right shoulder, left shoulder, and right hand and wrist were the symptoms most commonly experienced (Figure 2). It was observed that there were 40 positive correlations of ARM, based on the minimum support. For instance, the results reveal that 56 per cent of the participants had pain or discomfort in their lower back and 67 per cent had pain or discomfort in their neck, while among the whole sample, 43 per cent had pain or discomfort in both the lower back and the neck. Furthermore, 77 per cent of those who had pain or discomfort in the lower back also experienced pain or discomfort in their neck.
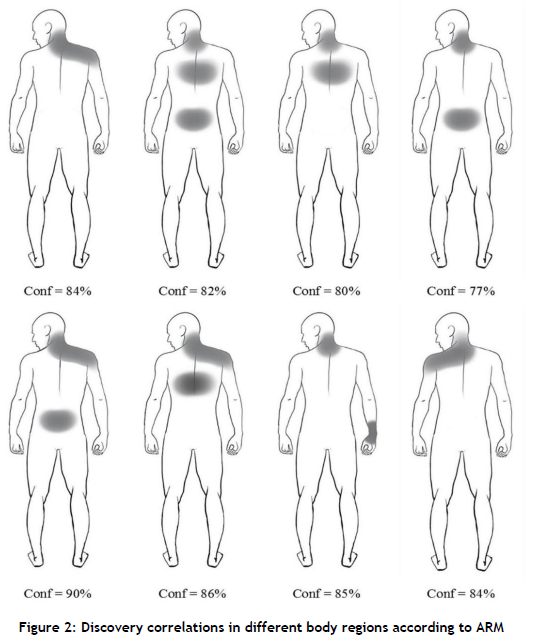
There are 15 extracted association rules that have a confidence of more than 70 per cent, which means that there is a significant relationship between the pains experienced in many different parts of the body. From these rules, we can conclude the following:
The participants had a high frequency of pain or discomfort in the neck, with a 77 to 90 per cent confidence. The participants who felt pain or discomfort in the neck region most likely also had pain or discomfort in the upper back, lower back, or right shoulder, with support from 32 to 43 per cent.
The significance level of the logistic regression technique used in this study is a = 5%. A list of significant factors is provided in Table 4. The logistic regression model has shown that 'sitting positions and postures while performing a task' have a significant effect on the MSDs. The body regions of neck, lower back, and upper back were also statistically significant factors (i.e., they had a large effect on the response variable). Based on the probability of 'yes' (feeling an MSD) for the logistic model, it was found that sitting without a desk most probably causes MSDs as a result of using MTSDs.
The model was developed using four machine-learning algorithms that were tested and validated. The next section compares four machine-learning algorithms radial basis function (RBF), long-short-term memory (LSTM), back-propagation (BP) neural networks, and support vector machine (SVM) - in terms of accuracy, macro-averaged F1-score, macro-precision, and macro-recall, because of the multinomial classification task. This was revealed after applying the training data to the machine-learning algorithms.
We implemented four different algorithms to determine the superior machine learning classifier in terms of prediction ability when studying risk levels that interfere with the ability to perform daily activities. A comparison of the considered metrics of each algorithm is shown in Figure 2. The RBF neural network achieved the highest scores of all of the metrics (84.0 per cent, 85.1 per cent, 77.8 per cent, and 81.3 per cent for accuracy, macro-precision, macro-recall, and macro-averaged F1-score respectively) and outperformed other models. The LSTM algorithm followed the RBF neural network by obtaining 79.8 per cent, 82 per cent, 74.5 per cent, and 78 per cent for accuracy, macro-precision, macro-recall, and macro-averaged F1-score respectively. On the other hand, the level of accuracy for the SVM algorithm (63.0 per cent) was lower than that for the BP algorithm (73.7 per cent).
4 DISCUSSION
This study has offered insights into the symptom prevalence of MSD in users of MTSDs who are prone to suffering pain or discomfort in various body regions. MTSD use can be logically expected to overload the neck, the dominant upper extremities, and the neck region. Unexpectedly, the authors found that participants also had pain or discomfort in the lower extremities, although with a higher prevalence in the upper extremities; the relevant results were 64.3 per cent pains in the neck region, 37.5 per cent in the right shoulder, 27.9 per cent in the left shoulder, 44.3 per cent in the upper back, 55.3 per cent in the lower back, 19.3 per cent in the right upper arm, 15.0 per cent in the left upper arm, 16.9 per cent in the right forearm, 12.5 per cent the left forearm, 27.7 per cent in the right hand/wrist, and 19.6 per cent in the left hand/wrist. Interestingly, male correspondents reported levels of higher pain in the neck region and the upper extremities than females. For the males, the pain that was experienced ranged between 73.4 and 69.1 per cent, while the females experienced pain ranging between 30.9 and 24.8 per cent.
Similarly, for the lower extremities, participants experienced 16.9 per cent pain in the hip/buttocks, 17.4 per cent in the right thigh, 13.7 per cent in the left thigh, 21.3 per cent in the right knee, 16.9 per cent in the left knee, 21.6 per cent in the right lower leg, and 15.6 per cent in the left lower leg. Male correspondents showed higher levels of pain in the lower extremities (between 77.3 and 74.6 per cent) than the females (between 29.3 and 22.7 per cent). This finding is therefore consistent with the neck, upper back, and shoulder discomfort reported in the literature. Can and Karaca [17] found that about half of their participants reported discomfort in the neck region and some parts of the upper extremities. The results of this study also corroborated the findings of Berolo, Wells and Amick III [41], who showed that daily usage affects the upper extremities. Likewise, Chiang and Liu [42] confirmed that participants using tablets had symptoms related to the neck and the intensity of discomfort in the back. The authors found that the lower back was more often a prominent site of mSd symptoms in participants - possibly a result of adopting a sitting posture while using MTSDs. Todd, Bennett and Christie [43] revealed that, over the long term, the sitting posture leads to higher levels of pain in the upper and lower back areas.
Conversely, Namwongsa et al. [18] reported that the symptoms of MSD were less prevalent in the lower back among smartphone users (17.2 per cent). Legan and Zupan reported that the prevalence of pain in the lower back ranged between 32.9 and 39.4 per cent. Our results aligned with the findings of these previous studies, but the percentages were higher in our study. In detail, the lower back was found to be the second-highest area of pain after the neck (55.3 per cent).
In addition, the logistic regression analysis showed that spending a long portion of the day while sitting or performing a task using an MTSD were significantly associated with a high prevalence of musculoskeletal pain in the neck, upper back, and lower back regions. In a recent study, Mustafaoglu et al. [24] used logistic regression models that showed that spending more than six hours a day on a smartphone and that sitting without support for the arms causes an increased frequency of pain in the neck and upper back. Similarly, in our study, we observed that the posture of sitting was associated with the presence of neck, upper back, and lower back pain or discomfort. Hakala, Rimpelà, Saarni and Salminen [44] found an increase in the risk of pain or discomfort in the neck, shoulder, and lower back when using smartphones for long periods.
In general, the prevalence of musculoskeletal disorders among users of MTSDs is a result of the application of sustained muscle load on the body. It is reasonable to assume that the participants in this study (university students) might be spending long hours in static postures to meet their academic requirements. However, the Covid-19 pandemic has also increased the time they spend with those devices for educational reasons. Therefore, MTSD use or overuse appears to lead to MSK overload, stress, and the resultant symptoms.
In our study, the mean age of the participants was 24.6 years. Therefore, they could be considered to be in the prime of health and physical function. The pain or discomfort experienced by these respondents might be because of the static postures they adopt for their studies, their associated daily activities, and their reduced physical activity caused by their academic burden. Neck flexion is the most common posture among smartphone users, and it can cause associated MSDs [45]. In this study, the prevalence of MSDs in the neck and lower back might be related to adopting a flexed neck posture while staring down at devices that are held lower than head level. It is clear that the excessive use of devices can lead to habitual, repetitive, and continuous movement of the head and neck regions [46,47].
In this study, the researchers used the ARM model to verify the results. From the extracted association rules, participants that had pain or discomfort in the lower back and neck had the highest positive correlation of support and confidence in the lower back and neck. In this way, pain in the lower back was associated with pain in the neck. Chan, Wong, Wang, Cheung and Samartzis [48] conducted a cross-sectional study to compare the prevalence of neck pain among undergraduate students at the University of Hong Kong. The results revealed that students with low back pain or discomfort were three times more likely to report neck pain or discomfort. Similarly, discomfort in the upper back and right shoulder was associated with discomfort in the neck region.
The current study also revealed that 57.5 per cent of the participants were right-hand dominant. Concurrently, the results revealed the association between pain or discomfort in the neck and pain or discomfort in the right shoulder and right hand and wrist, with confidence of between 84 per cent and 85 per cent. The prevalence of discomfort on the right side might be indicative of the dominance of usage and holding their devices with the right hand. This suggests that those who continuously hold MTSDs with one hand are more uncomfortable, and that continued use would lead to the increased pain or discomfort of MSD in that side. Moreover, 25 per cent of pain or discomfort in the right shoulder and lower back was associated with 64 per cent of pain or discomfort in the neck, with 90 per cent confidence, pointing to the probability that the pain or discomfort occurred simultaneously in these parts. Syamala, Ailneni, Kim and Hwang [25] found that muscle activities such as flexion angle and gravitational moments are all significant predictors of pain in the neck and upper extremities when mobile devices are in use. They also asserted that the use of an adequately supportive chair could serve as a remedy for such pain.
The findings in this study are consistent with those found in the literature. Our results highlight a direct relationship between mobile device use and the prevalence of experiencing symptoms of pain or discomfort. The literature suggests that these problems can be alleviated through increased participation in physical activities, reduced sitting time during usage, the use of appropriate chairs, and the adoption of correct postures [17, 25, 49].
Zhao, Zheng and Wen [50] confirmed that the RBF network is superior to other algorithms, not only in theory but also in prediction. Likewise, Ladstatter, Garrosa, Badea and Moreno [30] pointed out that the results produced by the RBF network are 15 per cent better than the results from traditional statistical methods. Accordingly, by comparing different kinds of predictive modelling networks to detect their accuracy, this study also discovered that simulating the RBF network with validation data produced better results (with 84.0 per cent accuracy) than cross-validation did using other networks.
The predictive performance of the RBF algorithm tended to be superior to the other models. This could be because of the superiority of its method in defining the importance of the variables and its ability to show the interactions among the predictor variables. Moreover, the results of this study showed that the support vector machine is the weakest algorithm in predicting accuracy (63.0 per cent). This matches the results of Sasikumar and Binoosh [32], who found that SVM was the lowest in accuracy (56.2 per cent). According to the literature review for this study, no previous research has used machine learning to assess the impacts of MTSD usage. This study fills the gaps in the scholarship by identifying MSK-symptom prevalence, body region distribution, the relationships between body parts, and predictors. It also applied the ARM approach to detect any relationship between the body parts where respondents experienced discomfort.
This study concentrated on both the traditional approach and the analytical approach, which included machine learning in the field of MSDs. According to work-related MSD steps, the authors identified the step of the development of intervention(s) to reduce a possible risk factor [51]. This study revealed that machine-learning algorithms accurately predicted MSD risk among respondents who use MTSDs. It incorporated RBF to predict accurately the relationship of pain or discomfort with risk levels that interfere with the ability to perform ADL. Regarding the algorithms used in the study, the RBF and LSTM were superior in terms of their F1-score and accuracy to the other algorithms. Even though BPNN is a superior neural network for MSD research and is widely used [52], the results that were obtained in this study demonstrated that the implementation of different ANN types such as RBF and LSTM could outperform BPNN, and would provide more accurate results.
The major limitations associated with the current study were that some important issues were not considered, such as the purpose of MTSD use and physical exercise. Other drawbacks included that the data to gauge the relationships between touch-screen device use and MSDs was solicited from a limited population, and convenience sampling was used. The influence or effect of other variables such as age brackets, which could constitute noise in the total outcome, is also being considered a ground for further research. Furthermore, the group of those aged 17 to 33 raises more concern because of the increase in variability among them. There are also behavioural changes that can affect the use of mobile devices by that age group. In addition, the sample size was small, and might not provide a sufficiently accurate prediction to detect differences in risk levels that interfere with the ability to perform ADL.
Nevertheless, this study can aid researchers as a reliable reference for any future studies related to this field. For such purposes, the authors recommend intervention and follow-up studies to examine the effects of MTSDs in the long term, and a comparison of self-reported data with observed data in the use of various touch-screen devices. Future researchers are also advised to collect more baseline demographic characteristics on the prevalence of MSDs. In addition, a greater number of respondents to the questionnaire would increase the predictive accuracy in detecting MSDs when using MTSDs.
5 CONCLUSION
This study was designed to examine the pain and discomfort of MSK, which can result in MSDs experienced by users of MTSDs. With the intention of investigating MSDs, it provided analysis and comparison of the body regions where discomfort occurs while using touch-screen devices. The results obtained from this study showed a similarity to the majority of findings in other studies of the impact of MTSDs on the physical discomfort of participants, except for those related to the lower back region. Specifically, this study showed that the neck, lower back, upper back, and right shoulder are the primary parts of the body where the responding MTSD users experienced pain and discomfort.
The RBF model developed in our study of MTSD users could be used to raise the alarm when people exhibit high-risk levels of pain interference. Our model could thus help users reduce the risk of interference with their ability to perform daily activities. Bosman et al. [31] found that MSD was one of the strongest predictors of sick leave. So the model developed here could be used by an organisation to predict whether there would be interference with employees' work performance or a rise in absenteeism as a result of pain in various body parts. Organisations and employees could thus take preliminary measures to safeguard organisational performance. In addition, a more regular assessment of employee well-being could also incentivise increased employee productivity.
REFERENCES
[1] Werth, A. and Babski-Reeves, K. 2014. Effects of portable computing devices on posture, muscle activation levels and efficiency. Applied Ergonomics, vol. 45, no. 6, pp. 1603-1609. [ Links ]
[2] Toh, S.H., et al., 2017. The associations of mobile touch screen device use with musculoskeletal symptoms and exposures: A systematic review. PLoS One, vol. 12, no. 8, e0181220. [ Links ]
[3] McCasland, M. 2005. Mobile marketing to millennials. Young Consumers, vol. 6, no. 3, pp. 8-13. [ Links ]
[4] Statista. 2020. Number of smartphone users worldwide from 2016 to 2021. Available from: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide.[Accessed 27 July 2020]. [ Links ]
[5] Yatani, K. and Truong, K.N. 2009. SemFeel: A user interface with semantic tactile feedback for mobile touch-screen devices. In Proceedings of the 22nd Annual ACM Symposium on User Interface Software and Technology, Association for Computing Machinery, pp. 111-120. [ Links ]
[6] Toh, S.H., et al., 2019. "From the moment I wake up I will use it™ every day, [e]very hour": A qualitative study on the patterns of adolescents' mobile touch screen device use from adolescent and parent perspectives. BMC Pediatrics, vol. 19, no.1, pp. 1-16. [ Links ]
[7] Osailan, A. 2020. The relationship between smartphone usage duration (using smartphone's ability to monitor screen time) with hand-grip and pinch-grip strength among young people: An observational study, BMC Musculoskeletal Disorders, vol. 22, no. 1, pp. 1-8. [ Links ]
[8] UNESCO. 2020. 1.37 billion students now home as COVID-19 school closures expand. Ministers scale up multimedia approaches to ensure learning continuity, United States Environmental.Unesco. Available from: https://en.unesco.org/news/137-billion-students-now-home-covid-19-school-closures-expand-ministers-scale-multimedia. [Accessed: 27 July 2020]. [ Links ]
[9] Wallace, S., Clark, M. and White, J. 2012. 'It's on my iPhone': Attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open, vol. 2, no. 4, e001099. [ Links ]
[10] Vafa, S. and Chico, D.E. 2013. A needs assessment for mobile technology use in medical education. Int J Med Educ, vol. 4, pp. 230-235. [ Links ]
[11] Adedoyin, O.B. and Soykan, E. 2020. Covid-19 pandemic and online learning: The challenges and opportunities. Interactive Learning Environments, vol.2, no. 1, pp. 1-13. [ Links ]
[12] Karingada, K.T. and Sony, M. 2021. Demonstration of the relationship between MSD and online learning during the COVID-19 pandemic. Journal of Applied Research in Higher Education, vol. 14, no. 1, pp. 200-222. [ Links ]
[13] Xie, Y., et al. 2016. A comparison of muscle activity in using touchscreen smartphone among young people with and without chronic neck-shoulder pain. Ergonomics, vol. 59, no. 1, pp. 61-72. [ Links ]
[14] Gustafsson, E., Johnson, P.W. and Hagberg, M. 2010.Thumb postures and physical loads during mobile phone use - A comparison of young adults with and without musculoskeletal symptoms. Journal of Electromyography and Kinesiology, vol. 20, no. 1, pp. 127-135. [ Links ]
[15] Legan, M. and Zupan, K. 2022. Prevalence of mobile device-related lower extremity discomfort: A systematic review. International Journal of Occupational Safety and Ergonomics, vol. 28, no. 2, pp. 1091-1103. [ Links ]
[16] Xie, Y., Szeto, G. and Dai, J. 2017. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: A systematic review. Applied Ergonomics, vol. 59, pp. 132-142. [ Links ]
[17] Can, S. and Karaca, A. 2019. Determination of musculoskeletal system pain, physical activity intensity, and prolonged sitting of university students using smartphone. Biomedical Human Kinetics, vol. 11, no. 1, pp. 28-35. [ Links ]
[18] Namwongsa, S., et al. 2018. Factors associated with neck disorders among university student smartphone users. Work, vol. 61, no. 3, pp. 367-378. [ Links ]
[19] Ning, X., et al. 2015. Neck kinematics and muscle activity during mobile device operations. International Journal of Industrial Ergonomics, vol. 48, pp. 10-15. [ Links ]
[20] Lee, S., Kang, H. and Shin, G. 2015. Head flexion angle while using a smartphone. Ergonomics, vol. 58, no. 2, pp. 220-226. [ Links ]
[21] Schabrun, S.M., et al. 2014. Texting and walking: Strategies for postural control and implications for safety. PLoS One, vol. 9, no. 1, e84312. [ Links ]
[22] Young, J.G., et al. 2012. Touch-screen tablet user configurations and case-supported tilt affect head and neck flexion angles. Work, vol. 41, no. 1, pp. 81-91. [ Links ]
[23] Kim, H.-J. and Kim, J.-S. 2015. The relationship between smartphone use and subjective musculoskeletal symptoms and university students. Journal of Physical Therapy Science, vol. 27, no. 3, pp. 575-579. [ Links ]
[24] Mustafaoglu, R., et al., 2021. The relationship between smartphone addiction and musculoskeletal pain prevalence among young population: A cross-sectional study. The Korean Journal of Pain, vol. 34, no.1, pp. 72-81. [ Links ]
[25] Syamala, K.R., et al. 2018. Armrests and back support reduced biomechanical loading in the neck and upper extremities during mobile phone use. Applied Ergonomics, 73, pp. 48-54. [ Links ]
[26] Kim, Y.M., et al. 2018. Classification of children's sitting postures using machine learning algorithms. Applied Sciences, vol. 8, no. 8, pp. 1280-1300. [ Links ]
[27] Huang, Y., et al. 2010. Development and applications of soft computing in agricultural and biological engineering. Computers and Electronics in Agriculture, vol. 71, no. 2, pp 107-127. [ Links ]
[28] Somers, M.J. 2001. Thinking differently: Assessing nonlinearities in the relationship between work attitudes and job performance using a Bayesian neural network. Journal of Occupational and Organizational Psychology, vol. 74, no. 1, pp. 47-61. [ Links ]
[29] Walczak, S. 2007. Neural networks in organizational research: Applying pattern recognition to the analysis of organizational behavior. Organizational Research Methods, vol. 10, no.4, pp. 710-712. [ Links ]
[30] Ladstatter, F., et al. 2010. Application of artificial neural networks to a study of nursing burnout. Ergonomics, vol. 53, no. 9, pp. 1085-1096. [ Links ]
[31] Bosman, L.C., et al. 2019. Development of prediction models for sick leave due to musculoskeletal disorders. Journal of Occupational Rehabilitation, vol. 29, no. 3, pp. 617-624. [ Links ]
[32] Sasikumar, V. and Binoosh S.C.A.B. 2020. A model for predicting the risk of musculoskeletal disorders among computer professionals. International Journal of Occupational Safety and Ergonomics, vol. 26, no. 2, pp. 384-396. [ Links ]
[33] Yamane, T. 1967. Problems to accompany 'Statistics: An introductory analysis'. Harper & Row, New York. [ Links ]
[34] Hedge, A. 1999. Cornell musculoskeletal discomfort questionnaires (CMDQ). Available from: http://ergo.human.cornell.edu/ahmsquest.html. [Accessed 18 June 2018]. [ Links ]
[35] Abdullah, Z., et al. 2011. Extracting highly positive association rules from students' enrollment data. Procedia-Social and Behavioral Sciences, vol. 28, pp. 107-111. [ Links ]
[36] Olafsson, S., Li, X. and Wu, S. 2008. Operations research and data mining. European Journal of Operational Research, vol. 187, no.3, pp. 1429-1448. [ Links ]
[37] Fan, C.-L. 2020. Defect risk assessment using a hybrid machine learning method. Journal of Construction Engineering and Management, vol. 146, no. 9, 04020102. [ Links ]
[38] Kotsiantis, S. and Kanellopoulos, D. 2006. Association rules mining: A recent overview. GESTS International Transactions on Computer Science and Engineering, vol. 32, no. 1, pp. 71-82. [ Links ]
[39] Ngai, E.W., Xiu, L. and Chau, D.C. 2009. Application of data mining techniques in customer relationship management: A literature review and classification. Expert Systems with Applications, vol. 36, no.2, pp. 2592-2602. [ Links ]
[40] Billsus, D. and Pazzani, M.J. 1998. Learning collaborative information filters. In Proceedings of the Fifteenth International Conference on Machine Learning, Morgan Kaufmann Publishers Incoporated, San Francisco, CA, USA, pp. 46-54. [ Links ]
[41] Berolo, S., Wells, R.P. and Amick, B.C. III. 2011. Musculoskeletal symptoms among mobile handheld device users and their relationship to device use: A preliminary study in a Canadian university population. Applied Ergonomics, vol. 42, no. 2, pp. 371 -378. [ Links ]
[42] Chiang, H.-y.A. and Liu, C.-H. 2016. Exploration of the associations of touch-screen tablet computer usage and musculoskeletal discomfort. Work, vol. 53, no. 4, pp. 917-925. [ Links ]
[43] Todd, A.I., Bennett, A.I. and Christie, C.J. 2007. Physical implications of prolonged sitting in a confined posture: A literature review. Ergonomics SA: Journal of the Ergonomics Society of South Africa, vol. 19, no. 2, pp. 7-21. [ Links ]
[44] Hakala, P.T., et al. 2006. Frequent computer-related activities increase the risk of neck-shoulder and low back pain in adolescents. The European Journal of Public Health, vol. 16, no. 5, pp. 536541. [ Links ]
[45] Kang, J.-H., et al. 2012. The effect of the forward head posture on postural balance in long time computer based worker. Annals of Rehabilitation Medicine, vol. 36, no. 1, pp. 98-104. [ Links ]
[46] Veiersted, K.B. and Westgaard, R.H. 1993. Development of trapezius myalgia among female workers performing light manual work. Scandinavian Journal of Work, Environment & Health, vol. 19, pp. 277-283. [ Links ]
[47] AlAbdulwahab, S.S., Kachanathu, S.J. and AlMotairi, M.S. 2017. Smartphone use addiction can cause neck disability. Musculoskeletal Care, vol. 15, no. 1, pp. 10-12. [ Links ]
[48] Chan, L.L.Y., et al. 2020. The prevalence of neck pain and associated risk factors among undergraduate students: A large-scale cross-sectional study. International Journal of Industrial Ergonomics, vol. 76, 102934. [ Links ]
[49] Xie, Y.F., et al. 2018. Spinal kinematics during smartphone texting: A comparison between young adults with and without chronic neck-shoulder pain. Applied Ergonomics, vol. 68, pp. 160-168. [ Links ]
[50] Zhao, H., Zheng, G. and Wen, W. 2010. Human-machine posture prediction and working efficiency evaluation of virtual human using radial basis function neural network. In 2010 IEEE International Conference on Intelligent Computing and Intelligent Systems, vol.1, pp. 406-410. [ Links ]
[51] Van Der Beek, A.J., et al. 2017. A research framework for the development and implementation of interventions preventing work-related musculoskeletal disorders. Scandinavian Journal of Work, Environment & Health, vol. 43, no. 6, pp. 526-539. [ Links ]
[52] Chan, V.C., et al. 2022. The role of machine learning in the primary prevention of work-related musculoskeletal disorders: A scoping review. Applied Ergonomics, 98, 103574. [ Links ]
Submitted by authors 14 Sep 2021
Accepted for publication 03 Jul 2022
Available online 29 Jul 2022
ORCID® identifiers
A. El ghomati: 0000-0001-7488-1507
O. Korhan: 0000-0002-9388-8605
B. Sekeroglu: 0000-0001-7284-1173
K.Dogruyol: 0000-0001-5782-5802
* Corresponding author: ali_algomati@yahoo.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}