










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Industrial Engineering
On-line version ISSN 2224-7890
Print version ISSN 1012-277X
S. Afr. J. Ind. Eng. vol.30 n.3 Pretoria Nov. 2019
http://dx.doi.org/10.7166/30-3-2243
SPECIAL EDITION
A Strategic Framework for Start-up Medical Device Manufacturers in South Africa
I. MaharajI, II, *; B.P. SunjkaI
ISchool of Mechanical, Industrial & Aeronautical Engineering, University of the Witwatersrand, South Africa
IIAssociate Director, Dynamed Pharmaceuticals (Pty) Ltd, South Africa
ABSTRACT
An exploratory, qualitative study was conducted to establish why local medical device manufacturing firms are not starting up in South Africa. Semi-structured interviews were conducted with local medical device manufacturers to understand the market and the competitive environment in which companies operate, as well as elements of strategy implemented within these companies. The study concluded that local medical device manufacturers were not starting up in South Africa due to the high capital investment required, the prohibitive and unaligned regulatory framework, brand representation and the unwillingness of end users to switch to smaller brands, and cash flow and liquidity problems. Recommendations were made for start-up medical device manufacturers to mitigate any potential problems that might be faced, as well as for future policy development of medical devices. Included in this was the suggestion to realign South African medical device regulations with other successfully implemented regulations across the world.
OPSOMMING
'n Verkennende, kwalitatiewe studie is van stapel gestuur om te bepaal waarom plaaslike mediese toestel vervaardigingsfirmas nie in Suid-Afrika vestig nie. Semi-gestruktureerde onderhoude is gevoer met plaaslike mediese toestel vervaardigers om die mark en mededingendheidsomgewing, saam met elemente van die firmas se strategieë, beter te verstaan. Daar word afgelei dat plaaslike mediese toestel vervaardigers nie in Suid-Afrika vestig nie vanweë die hoë aanvangskoste, voorkomende en swak belynde regulasie raamwerk, handelsmerk verteenwoordiging en die onbereidwilligheid van eindgebruikers om van kleiner handelsmerke gebruik te maak, sowel as kontvloei en likiditeit uitdagings. Aanbevelings is gemaak wat nuwe ondernemings sal help om potensiële probleme te addresseer en sal bydra tot toekomstige beleidsontwikkeling binne die verband. Ingesluit in die aanbevelings is die voorstel om die Suid-Afrikaanse mediese toestel regulasies te belyn met ander, suksesvol geïmplementeerde regulasies wat in ander dele van die wêreld aangetref word.
1 INTRODUCTION
Healthcare is a critical area for service delivery in South Africa, yet 90 per cent of the market value of medical devices is still imported into South Africa [1]. The South African medical device industry was estimated to be worth US$ 1.2 billion [2] in 2013. While the industry was forecast to grow at a compound annual growth rate of 7.74 per cent from 2013 to 2018, medical devices imported into South Africa were forecast to grow at almost twice that rate - 12.65 per cent - during the same period [2]. The Department of Trade and Industry's strategic objectives include increasing South Africa's medical device manufacturing capacity; yet there are diminishing numbers of start-up medical device manufacturers in the country [2].
Maresova and Kuca [3] attribute the lack of start-up manufacturers to competitive forces experienced by industry participants - i.e., barriers to market entry [3]. Dawar and Frost [4] suggest that competing with industry leaders is the most significant challenge for start-up manufacturers which rely on protectionist trade barriers or other governmental support to survive. As a result, they become subordinate partners to multinationals, or simply sell out and leave the industry [4].
No previous research has been conducted on the challenges faced by local start-up medical device manufacturers in South Africa. It is important to address and understand the contributing factors to this reluctance to enter the market in order to increase South Africa's medical device manufacturing capacity. This research thus sought to address this gap by establishing the reasons for the lack of local start-up medical device manufacturers in the South African industry.
2 LITERATURE REVIEW
Understanding the competitive forces experienced by manufacturers in the medical device industry is important in order to understand a firm's reluctance to enter the industry. Frameworks describing competitive forces in the medical device industry, strategy development, and strategy implementation were used to determine the forces experienced by South African medical device manufacturers, and the survival and growth strategies implemented by companies.
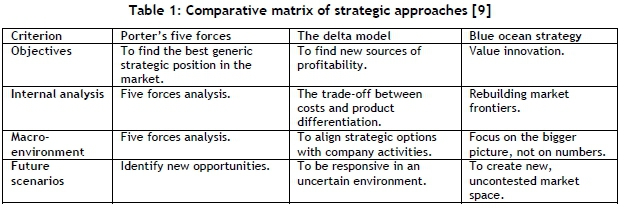
2.1 Strategic frameworks
Porter [5] contends that the essence of business strategy formulation lies in the ability to cope with competitive forces in the marketplace. Porter describes the state of competition, which includes five basic forces: the threat of new entrants, the bargaining power of suppliers, the threat of substitute products, the bargaining power of customers, and jockeying for position among current competitors [5]. An extension of Porter's [5] five forces framework includes a sixth 'force': complementors. A company can be described as a complementor if customers value their product more when they are in possession of that other product than when they have the original product alone [6].
Hax and Wilde [7] argue that companies remain product-centred as a result of classic strategic frameworks that emphasise a product-orientated strategy. Hax and Wilde [7] propose the delta model, which provides three distinct strategic positions: system lock-in, total customer solutions, and best product. 'Best product' explains that the way companies retain customers is through the inherent characteristics of the product itself [7]. 'Total customer solutions' represents solutions consisting of customised products and services that meet the demand of unique customers [7]. 'System lock- in' describes the most demanding strategic choice and addresses the full network of the relevant scope. It focuses on gaining the complementor's market share as the main objective, while focusing on the system economics as the driving force. This situation enforces a customer lock-in and a competitor lock-out [7].
Kim and Mauborgne [8] maintain that industries are constantly evolving and that products eventually become economically obsolete and stop generating profit. This suggests that the traditional business environment, which saw the development of traditional strategic approaches, disappears at an increasing rate. Kim and Mauborgne [8] describe the normal life of the firm, with its commercial and technological routine, as the 'red ocean'. 'Blue ocean' strategy originates from the analysis of the red ocean. Blue ocean pursues unique market spaces untapped by competitors, where firms can grow. It is defined as the continual search for value innovation [9]. Value innovation occurs where firms have a favourable impact on cost structure and value proposition to customers. Value is created by improving and creating attributes not yet offered in the industry [8].
Jussani, de Castro Krakauer & Polo. [9] produced a set of analysis criteria for the evaluation and comparison of Porter's five forces, the delta model, and blue ocean strategy.
2.2 Competitive forces in the medical device industry
The global medical device industry is characterised by significant competitive challenges such as high barriers to entry, including capital intensive research and development, regulatory restrictions, and the inability of small manufacturers to compete with larger multinationals [3]. The threat of substitute products can be described as a medium impact force. For a medical device to be a viable substitute, it must perform the same function as the current product. Although intent is shown to purchase substitute products, the demand for current products still grows [3]. The bargaining power of buyers can also be described as a medium impact force. The bargaining power of suppliers, however, can be described as a low impact force due to the large number of suppliers and ease of substitutability [3]. There are numerous competing companies in the medical device industry. Competition in the industry is strong due to low product differentiation, low switching costs for buyers, and changes connected with reimbursement and regulatory policies respectively [10].
2.3 The South African environment
South African small to medium enterprises have one of the highest failure rates in the world - 75 per cent [11]. To understand the obstacles that small to medium enterprises face, as well as their success factors, Olawale and Garwe [11] described a separated internal and external business environment.
Company demographics such as the size of the firm, the age of the firm, and the product and its competitiveness affect the survival of the firm [12]. A dearth of managerial competencies is the biggest reason that new firms fail: a lack of education and training has reduced management capacity in South African small to medium enterprises [13]. Kunene [12] describes entrepreneur demographics as one of the most influential factors relating to the firm's performance and competitiveness. Entrepreneur demographics include gender, role models such as parents or other entrepreneurs, and education. Kunene [12] also described the quality of an entrepreneur as being directly proportional to the entrepreneur's previous experience. The learning process involved allows entrepreneurs to identify opportunities, reduce initial inefficiencies, and improve capacity [12].
Beck [14] described the external environment as economic variables and markets, crime, corruption, and labour; and infrastructure and regulations. Economic factors have a direct impact on the attractiveness of different strategies. These factors include fiscal policies, monetary policies, inflation, interest rates, and foreign exchange rates. These factors influence the supply and demand of goods and services, and therefore affect the growth of small to medium enterprises [11]. Kunene [12], however, stated that the success of a start-up firm is dependent on the state of the national economy at the time.
South Africa's business sector is the largest organised group suffering from crime and violence. Businesses are not actively pursuing growth, as they are too focused on operational matters as a result of the high crime rate [11]. Corruption in South Africa's public and private sector is growing [11]. Gaviria [15] argued that the reason that small to medium enterprises engage in corruption is their lack of bargaining power and influence to turn down unofficial payments and other attempts at corruption.
South African small to medium enterprises find it difficult and expensive to find labour that is suitably skilled and suitably motivated [11]. The quality of infrastructure also determines a small to medium enterprise's ability to grow. Electricity supply does not meet the demand in South Africa; so companies experience power cuts. And the cost of regulations is a barrier to entry, as firms must still obtain registration licences and pay taxes [11]. With the rising costs of electricity and petroleum, it is necessary for firms to reduce waste and to determine the most efficient means of production [12].
From the business environment segmentation, Olawale and Garwe [11] determined the most significant obstacles to growth faced by South African small to medium enterprises. In order of the highest impact obstacles, these are:
1. Lack of access to finance
2. Lack of collateral
3. Crime
4. Lack of owner's equity contribution
5. Bad credit record
6. Insufficient government support
7. High production costs
8. Inadequate market research
9. Lack of information technology
10. Corruption
On the other hand, key success factors for Small and Medium Enterprise (SME) manufacturers, as defined by Olawale and Garwe [12], include:
1. Company demographics - Creating sustainable competitive advantage through high quality products and good brand representation.
2. Previous experience - Founders to have experience in the medical device, or another related, industry at senior management level.
3. Economic factors - Medical device manufacturers experience limitations in raising capital due to high interest rates, value added tax, and general economic conditions in South Africa. The success of a local firm is dependent on the state of South Africa's economy.
4. Policy/institutional - Understanding of the legislation and regulatory frameworks governing medical device manufacture in South Africa.
2.4 The South African medical device industry
The South African medical device industry was a previously unregulated industry, unlike most other medical device industries around the world. The Medicines and Related Substances Amendment Act 14 of 2015 brought significant changes to the existing regulatory atmosphere in South Africa [16], and creating a new regulatory authority, the South African Health Products Regulatory Authority (SAHPRA). Previously, only electronic medical devices were governed by Medicines Control Council regulations [16]. The fundamental changes brought about by the amendment include the introduction of a new regulatory body, tier-based licensing and registration, and sales and distribution regulations [17].
SAHPRA replaced the Medicines Control Council, and is responsible for the regulatory oversight of medicines, medical devices, complementary medicines, cosmetics, foodstuffs, and related substances [18]. SAHPRA is an extension outside of the state public service [16]. The authority is empowered to register medicines, medical devices, and complementary medicines and foodstuffs, while also being assigned to re-evaluate and re-assess products [16].
The amendment includes a four-tier licensing system to import, manufacture, and distribute medical devices. The risk classification is broken down into Class A - low risk; Class B - low-moderate risk; Class C - moderate risk; and Class D - high risk [17]. Class B, Class C, and Class D medical devices and in-vitro diagnostics may not be imported into South Africa without obtaining the necessary registration documents. Only registered medical devices may be sold in South Africa. Domestic manufacturers, wholesalers, and distributors are required to obtain licences, while foreign manufacturers are not [16].
3 RESEARCH METHODOLOGY
To understand why local medical device manufacturers are not starting up in the South African industry, the trends in challenges and experiences faced by local medical device manufacturers, and the opinions of key South African manufacturers, required investigation. Although the medical device industry is global, many restricting factors were attributed specifically to South African regulations and the South African market environment [1].
Semi-structured interviews were deemed to be the most appropriate means of understanding problems and situations in each company, given that all business models and/or revenue models are specific to a single enterprise or group of enterprises. Participant observation was also employed, noting the challenges faced by medical device manufacturers in their competitive environment, and the challenges faced as a result of South Africa's regulatory framework.
3.1 Research design
3.1.1 Semi-structured interviews
Semi-structured interviews were conducted using a five-step approach outlined by Wilkinson and Birmingham [19]: draft the interview, pilot the questions, select the interviewees, conduct the interviews, and analyse the interview data.
Interviews were drafted around key themes identified in the literature to ensure that no issues were overlooked, and followed a logical progression [19]. The interviews were drafted to address the following issues:
• Barriers to entry faced by companies on start-up in the medical device manufacturing industry.
• Competitive forces faced by the firm in the South African market environment.
• Factors that have ensured the firm's success in the medical device manufacturing industry.
The interviews included a comprehensive company background, a market background of the environment in which the firm competes, obstacles to the firm's growth, and strategy development and strategy implementation. Participants were granted complete anonymity. Audio recordings were used to transcribe the interviews and to capture all necessary information.
To ensure a good understanding of the interview questions, the first interviewee was used to pilot all the questions. Piloting interview questions eliminates ambiguous questions and generates feedback about the flow of the interview [18,19]. All the interview questions were open-ended, and allowed the interviewees to provide as much information as possible. Follow-up questions were asked to probe for further information. The selected pilot participant was an experienced member of the medical device manufacturing industry, and served multiple roles in the industry, including as a manufacturer. The pilot responses were assessed to determine whether sufficient information was obtained to understand the market in which the company operates, its competitive environment, and the elements of strategy implemented by the company.
3.1.2 Participant observation
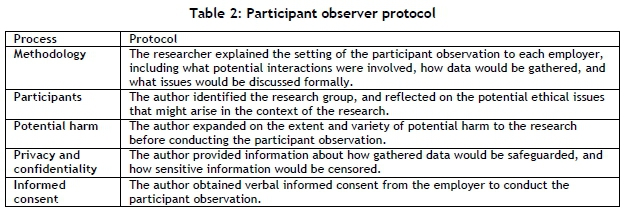
Participant observation is an experimental, inductive, field research strategy in which the researcher is immersed in the day-to-day activities of the group being studied [25]. Vinten [26] argued that researchers supplement other research methods with participant observation. It allows a more comprehensive understanding of the research topic and enhances the rigor of the study [26]. The participant observation followed the protocol described by Rankin and Bertrand [25], shown in Table 3, to ensure that the participant observer (the researcher) had weighed potential harms against the benefits of the research.
3.2 Sampling methodologies
Purposeful sampling was selected as the sampling method because of the in-depth information and thorough understanding of the research topic it provides [20]. As a result of selecting purposeful sampling, potential researcher bias associated with the method was addressed as follows:
A number of purposeful sampling methodologies were used in this research, including criterion sampling, extreme or deviant case sampling, critical case sampling, chain sampling, and maximum variation sampling [20,21]. Criterion sampling, or selecting a sample based on a set of predetermined criteria deemed to be important to achieve the research objectives, was used as the basis for all the other sampling methodologies [20]. The pre-determined criteria used to select participants included:
1. The participants must have been involved through the company's initial growth stages.
2. The participants must have been involved in strategy development and/or strategy implementation.
3. The participant must have served in a senior management position at the firm.
4. The participants, including the company they represent, must be a compliant member of the South African Health Products Regulatory Authority.
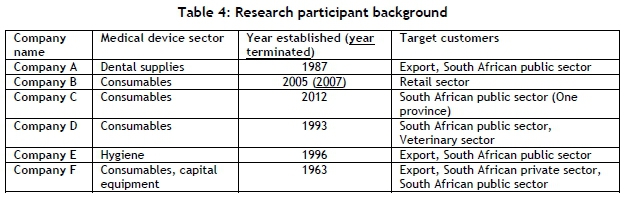
Extreme or deviant case sampling was selected, as participants were chosen based on their success as a medical device manufacturer in South Africa. Participants that had failed in the industry, and those that had succeeded in the industry, were selected. These factors enhanced the study through the identification of key factors that resulted in a firm's success or decline. Critical case sampling was selected, as participants could provide key insights into a highly regulated industry with a strongly competitive environment. Key manufacturers were identified that could provide insight into the medical device industry. Chain sampling was selected, as participants were identified using key resources in the medical device industry, including other interviewees. Maximum variation sampling was selected to maximise the central themes across the medical device industry. The method aimed to maximise the diversity of the participants through their geographic location, medical device sector, manufacturing capacity and operations, and company size. As a result, a sample of six CEOs, founders, directors, and/or senior managers of local medical device manufacturers were selected for interviews (Table 4).
3.3 Data collection and analysis procedures
Data analysis was done both during each interview and after the interview. Data collected was subject to either a deductive content analysis or a directed content analysis [21]. In content analysis, data is 'coded' into explicit categories and described by identifying patterns and using statistics [22]. Deductive content analysis can be described as an approach to validate or conceptually extend a theory [22]. It can be used when the structure of analysis is based on previous knowledge [23].
Key concepts and variables were identified from previous research in the South African medical device industry, the South African market environment, strategy, and start-up companies. All data thereafter was allocated to predetermined concepts and analysed for patterns and other similarities. The interviews were used to generate data separated into founding member background; company core operations and changes; company target market and export ratios; the competitive environment and its changes; market growth and company growth; obstacles to growth in the industry; regulatory issues; and company survival and growth strategies. These concepts were presented in three categories: the business background, the competitive environment, and strategic objectives.
A comparative analysis was conducted between categorised interview data and the literature [24]. Business strategy, the South African medical device industry, and the South African market environment were categories used to conduct the comparative analysis, where key similarities and differences were identified.
3.4 Reliability and validity
The concept of reliability in qualitative research is referred to as 'dependability', which closely corresponds to 'reliability' in quantitative research [27]. To reveal the congruence between reliability and validity in qualitative research, Lincoln and Guba [27] argued that there is no validity without reliability. Creswell and Miller [28] suggested that validity is affected by the researcher's perception of validity in the study. Researchers have, as a result, generated more appropriate terms for validity, such as quality, rigour, and trustworthiness [29]. Sustaining the trustworthiness of a research report is dependent on establishing confidence in the research findings [29]. The rigour of a study is determined by exploring subjectivity, reflexivity, and the social interaction of interviewing [29].
To ensure the credibility, validity, rigour, and trustworthiness of this research, multiple strategies were used, including these:
1. Triangulation - Information was cross-checked over multiple procedures or sources [30].
2. Low inference descriptors - Descriptions phrased close to the participant accounts, or verbatim transcriptions, were used to analyse the data [30,31].
3. Reflexivity - A self-reflection on potential biases, predispositions, and how they affected the research process was conducted by the researcher.
4. Participant feedback - Feedback and discussion of the researcher's interpretation of the interview data was distributed to the participants for further insight and verification, and to assess whether the concepts adequately reflected what was being investigated [30].
5. Dependability - Dependability was ensured through a detailed explanation of the research methodology in the light of existing dependable research, data analysis, and results, allowing for the methodology to be replicated [32].
6. Transferability - The results, conclusions, and recommendations of this study can be transferred to other highly regulated industries in South Africa, such as food, microbiology, and pharmaceuticals [32].
4 RESULTS
Six semi-structured interviews were conducted with local medical device manufacturers around South Africa.
4.1 The business environment
The founding members of all the participating companies (6/6) all had experience in an industry before starting their manufacturing companies. They had experience in the design of medical devices, experience in the medical device industry as a non-manufacturer, or experience at multinational medical device companies. Participants who had no prior experience in the medical device industry (2/6) had gained experience in a related industry, a business venture, or a corporate environment.
All existing participating companies (5/6) have experienced significant growth from inception, and continue to grow. Participating companies that were not established as manufacturers (2/6) began operating in the medical device industry as distributors or consultants. The number of years of operation of the business showed a direct relation to the size of the company and the growth experienced. All existing companies (5/6) experienced rapid growth at inception, which has since tapered off. The growth of companies that export is reflected in the growth of their export volumes.
Half of all the research participants (3/6) imported raw materials into South Africa. The reasons for participants not procuring locally included the unreliability of South African suppliers to meet lead times; the inconsistent quality of the supplied raw materials; the lack of local subcontractors, component manufacturers, and raw material manufacturers; and the cost effectiveness of independently importing raw materials as a result of high distributor mark-ups. The manufacturers all primarily supply medical device end users directly, as opposed to prioritising other wholesalers and distributors.
4.2 The competitive environment
A trend in increasing numbers of competitors in the medical device manufacturing industry was noted by all the research participants (6/6). All of the companies that were founded before 1990 (2/6) were the sole manufacturers of their medical devices in South Africa, and competition came mainly from multinational importers and distributors. Presently, all medical device companies (6/6) compete with multinational importers and distributors, Middle East and Far East importers, South African importers and distributors, and other South African manufacturers. Company F, a capital equipment manufacturer, has remained the sole manufacturer of its product in South Africa since its inception.
The companies all experienced obstacles to growth in the South African medical device industry - a fact that partially correlates with Olawale and Garwe's [11] top obstacles to growth in South Africa.
All research participants abided by medical device regulations, but faced many problems with the regulatory framework, including:
1. The regulations imposed mirror a pharmaceutical model, and are not appropriate for medical devices.
2. There is a conflict between South African and international regulation, which greatly increases compliance costs for exporters.
3. The grossly high costs of implementing quality management systems for medical device manufacture.
4. The compliance costs of manufacture are much higher than those of a distributor.
5. The definition of a medical device manufacturer in South Africa allows those that are not physically manufacturing a product, but rather labelling or packaging, to be defined as a local manufacturer.
4.3 Strategic objectives
All the research participants had elements of strategy built into their company culture and business operations. No participants noted formalised growth or survival strategies. All the participants sustained competitive advantage through:
1. Brand representation
2. Product quality
3. Reduced cost through import substitution
4. Product innovation
5. First-to-market
6. After sales technical support
On start-up, medical device manufacturers incorporated several survival strategies into their businesses:
1. Brand awareness - Creating an internationally renowned brand of products. Brand representation is the most important factor in the medical device industry.
2. Product design - Creating and sustaining the highest quality medical devices.
3. Cash flow - Ensuring that all capital equipment and other costs are paid for in cash.
4. Customer relationships - Establishing and maintaining good customer relationships.
5. Collaboration - Participating in medical device collaboration opportunities, such as the Medical Device Manufacturers of South Africa, and others.
To enhance further growth, companies implemented growth strategies focused on products, regulations, manufacturing, and business operations.
4.4 Participant observation
The participant observation protocol focused on issues that included competition in the medical device industry, the regulatory framework that governs the medical device industry, and opportunities for company growth in the South African medical device industry. Results of the participant observation included the following:
• Importers are the largest competition for local manufacturers in South Africa.
• The South African public sector remains extremely price sensitive, and public health institutions are willing to compromise quality for price.
• A large amount of corruption exists in both the public and the private health sectors.
• Health institutions continue to procure goods from unlicensed or non-compliant manufacturers.
• Private healthcare groups have not attempted to support local South African manufacturers.
• Brand awareness and representation are important factors in determining medical device sales.
• Medical device regulations are not aligned with other international medical device regulations.
• Public health institutions still accept medical devices from unlicensed firms.
• Regulatory authorities have had endless technical and administrative issues, and have been unavailable to solve problems faced by industry stakeholders.
• Funding and incentives are available to local manufacturers, but are not well communicated to all industry stakeholders.
5 DISCUSSION
To achieve the objective of this research, and to understand the competitive forces faced by medical device manufacturers, the strategies implemented in that industry and the competitive forces faced by start-up companies and small to medium enterprises in South Africa were identified.
5.1 The competitive environment
All participating companies experienced rapid growth at start-up, which then tapered off. However, the choice of products they manufactured proved to be a determining factor in the success of the businesses. As competition with distributors and importers increases, it is important for manufacturers to focus on products with a greater requirement for quality. Therefore, manufacturing products that are not solely suited to mass production are better suited to South African market conditions. Competition from importers and distributors is a high impact force in the medical device industry. Due to the price sensitivity of the market, end users in the public health sector are willing to compromise quality for better pricing structures.
Competing on price only has proved difficult for local medical device manufacturers. Apart from competing with the mass production and cheap labour of the Middle East and the Far East, local manufacturers are also forced to abide by South African and international regulations. Newly imposed South African regulations add further costs to already-compliant manufacturers. It is critical that the South African regulatory system aligns with international regulations, and is not just a mirror of South Africa's pharmaceutical model. A preliminary study of key participants in the industry revealed that a mirror of the pharmaceutical model is not appropriate, as the intended uses of medical devices and pharmaceuticals are different.
Import duty structures have also created additional costs for local manufacturers. Because of the unavailability and unreliability of local raw material suppliers, manufacturers are forced to procure materials elsewhere. Import duties imposed on raw materials are more than import duties imposed on finished products. The import tariff classification system also proved to be inappropriate, as specific medical device data cannot be extracted.
In addition to the import duty structure imposed on medical device manufacturers, cash flow problems were created by public health institutions. South African public health institutions do not guarantee timeous payments within 30 days, and are also not subject to interest on overdue payments - as stipulated by The National Credit Act No.34 of 2005 [33]. Medical device manufacturers are forced to comply with stringent payment policies by overseas manufacturers that entail full payment on shipment of goods. The delay in payments by public sector institutions, compared with the rate of payments to overseas suppliers, causes cash flow restrictions for medical device manufacturers.
The dominant presence of multinational products and brands in the private sector forces local device manufacturers to sell products mainly to public sector institutions. Multinationals are tied to long-term contracts with large discount schemes, making it difficult for smaller, local companies to penetrate the market. Private healthcare groups have not committed themselves, like public sector institutions, to the strategic procurement of locally manufactured goods. This was highlighted by the lack of documentation available from private healthcare institutions with respect to tender bidding processes and preferential procurement.
Funding and incentive initiatives are available for local medical device manufacturers, but they are limited to microenterprises and BB-BEE-compliant companies. Relevant governmental departments do not have a direct link to local medical device manufacturers in South Africa, but rather to industry collaborations - such as the Medical Device Manufacturers of South Africa (MDMSA) and the South African Medical Technology Industry Association (SAMED).
5.2 Success factors of South African small to medium enterprises
Four major success factors of local device manufacturers, as defined by Olawale and Garwe [11] and described in Section 2.3, included company demographics, previous experience, economic factors, and policy/institutional factors.
Company demographics, including the size and age of the firm, were important factors to consider in the medical device industry as a result of the importance of brand representation. Brand representation is built with the company's age, size, product offering, and competitiveness. Entrepreneurs should have the relevant knowledge, skills, problem-solving ability, and rational decision-making ability to ensure the success of the business. Previous experience in the medical industry is also an important factor in determining the success of the business, due to the highly regulated nature of the industry.
Economic factors have a major impact on all South African industries. The enterprise density of two per cent and the medical device company growth proved that there is more space for new company growth in the industry [12]. Despite the success of research participant companies, high interest rates and taxes have plagued the entrepreneurial process in South Africa. Policy/institutional factors have had a major impact on the medical device industry. A prohibitive regulatory framework has deterred new manufacturers. Regulatory compliance costs have proved to be too costly for start-up companies to deal with. All research participant companies were founded prior to medical device regulations being imposed in South Africa in 2016. The cost of compliance with South African regulations for companies already compliant with international regulations was minimal. Market opportunity factors also had a major impact on the medical device industry. The South African medical device industry continues to grow, and the demand for products continues to increase despite further developments and new products being released in the industry [1].
Obstacles to growth faced in the medical device industry were linked with obstacles to growth faced by South African small to medium enterprises [11]. Local manufacturers noted that the lack of funding and incentives results from a lack of finance and collateral, and a lack of government support through import duties, grants, and regulatory support. High production costs were linked to imports and exports and to the unreliability and unavailability of local raw material suppliers. Inadequate market research was linked to the regulatory atmosphere and the lack of knowledge of laws, regulations, licensing, and other regulatory aspects. Regulations may be product-specific, and lack of market research could imply unforeseen cost implications. Other obstacles to growth faced by medical device manufacturers include cash flow and the private sector, which are not generally major obstacles to South African small to medium enterprises. Medical device manufacturers were also subject to corruption, lack of information technology, bad credit records, and lack of owner's equity contribution; but these were not immediate threats.
5.3 Medical device manufacturer strategy
Elements of strategy were built into business operations and company culture by all the research participants. The most important strategic element adopted by medical device manufacturers was brand representation. To build brand awareness, firms should consider a number of factors, including what would give the firms a competitive advantage over already established firms with high quality products and good brand representation. Key focus areas for medical device manufacturers should be regulatory compliance; price reduction through import substitution; product quality; marketing strategy; and building customer relationships.
Potential start-up companies have focused on innovation; but being first-to-market incurs exorbitant capital and research and development costs. Therefore product development and being first-to-market are not appropriate strategies for South African medical device manufacturers.
Company growth strategies included those focused on continually improving product quality and complying with regulations. Established medical device companies were focused on reflecting company growth through export volume growth. Due to the prohibitive nature of South Africa's regulatory framework, and the difficulty in penetrating the private sector, local medical device manufacturers are focused on being export-ready and on complying with international regulations.
The highest-impact competitive forces in South Africa's medical device industry are the barriers to entry and competitive rivalry or jockeying for position in the market. Although some elements of the delta model may be appropriate to implement in medical device manufacturing companies, the model is not suitable due to the comprehensive planning and analyses of industry structure, industry attractiveness, core competencies, and resources and skills required to implement the strategy. The blue ocean strategy model also proved to be unsuitable for South African start-up medical device manufacturers, due to exorbitant research and developments costs. The costs of product development may be too costly for start-up manufacturers. Research participant companies were founded using the entrepreneurial process more than formalised strategic planning. No formalised strategic planning was used in any participating companies. Rather, previous experience factors, characteristics of the entrepreneur, and understanding the industry's competitive environment and regulatory atmosphere were the critical factors in determining the success of the firm.
6 CONCLUSIONS AND RECOMMENDATIONS
To understand why local medical device manufacturers are not starting up in the South African industry, trends in the challenges and experiences faced by local medical device manufacturers and the opinions of key South African manufacturers were investigated.
The research established that the lack of local start-up medical device manufacturers in South Africa may be attributed to a number of factors. The most significant barrier to entry is the capital investment required to manufacture medical devices, where capital investment includes capital required for machinery, licensing, regulatory compliance, marketing, and general operational costs. Other factors include the inconsistency of South African regulations compared with international regulations, where the implementation of a quality system, obtaining licences, product certification, and other ongoing compliance costs are unsustainable for start-up companies. Regulations are, thus, not strictly followed, and non-compliant manufacturers are still allowed to trade. Complying with South African regulations, however, does not grant access to international markets. Being a compliant manufacturer guarantees preferential public healthcare procurement, but it does not guarantee private sector penetration.
Brand representation and the unwillingness of end users and clients to switch to smaller, local brands is another challenge they face. Brand representation is the most important element of strategy in the medical device industry, where the supply of medical devices is difficult for start-ups with no product guarantees or track record of product performance. Cash flow problems, as a result of erratic and late payments from the public sector, present a further hurdle that affects the liquidity of a start-up manufacturer.
The industrial engineering strategic thinking that assists in the development of operations' strategies and tactics may be harnessed to develop recommendations for medical device start-ups and policymakers at a government level.
Thus, to mitigate the immediate problems outlined above, it is recommended that start-up companies begin manufacturing operations only with packaging and labelling operations to strengthen company liquidity and build capital for equipment required; that they abide by all regulations and quality standards from the inception of the firm; and that only one brand is created for the company, built around price competitiveness and product quality. These recommendations, however, need to be supported by changes in medical device regulations and future policy development, such as the development of a medical device regulatory framework specific to medical devices only - that is, separate from a pharmaceutical model framework - similar to the American 'FDA' or European 'CE'.
All manufacturers should be encouraged to become members of medical device collaborations such as MDMSA or SAMED to identify new opportunities and procure locally; and a government representative should be identified and appointed to host quarterly networking events for medical device companies throughout South Africa. This representative should also search for development opportunities with multinationals and importers. The governing body should appoint quality management representatives to design and implement appropriate and compliant systems for medical device manufacturers. The import duty structure should be changed to an eight-digit descriptor to allow access to accurate import and export data. A centralised payment system for public healthcare institutions to reimburse suppliers timeously should also be implemented. Funding opportunities directed at medical device regulatory compliance should be developed for smaller, local medical device manufacturers. Monthly training for company 'authorised representatives' should be required to allow companies to understand the newly enforced regulations and the requirements for keeping companies compliant. Financial assistance should be directed to companies preparing to export, to ensure international regulatory compliance and assistance with increased working capital.
REFERENCES
[1] South African Medical Technology Association. 2014. The South African Medical Device Industry - Facts. SAMED. [ Links ]
[2] Deloitte & Touche, for Department of Trade and Industry. 2014. Research to guide the development of strategy for the medical devices sector of South Africa. Deloitte & Touche. [ Links ]
[3] Maresova, P. & Kuca, K. 2014. Porter's five forces on the medical device industry in Europe. Military Medical Science Letters, 83(4), pp. 134-144. [ Links ]
[4] Dawar, N. & Frost, T. 1999. Competing with giants: Survival strategies for local companies in emerging market. Harvard Business Review, March-April, pp. 119-129. [ Links ]
[5] Porter, M.E. 1979. How competitive forces shape strategy. Harvard Business Review, March-April, pp. 137145. [ Links ]
[6] Nalebuff, B. and Brandenburger, A. 1997. "Co-opetition: Competitive and cooperative business strategies for the digital economy", Strategy & Leadership, Vol. 25 No. 6, pp. 28-33Hax, A.C. & Wilde, D.L. 2003. The delta model: A new framework of strategy. Journal of Strategic Management Education, 1(1), pp. 1-21. [ Links ]
[7] Kim, W. & Mauborgne, R. 2005. Blue ocean strategy: How to create uncontested market space and make the competition irrelevant. 1st ed. HBS Press, Boston, USA. [ Links ]
[8] Jussani, A.C., de Castro Krakauer, P.V. & Polo, E.F. 2010. Reflections on blue ocean strategy: A comparison with Ansoff's, Porter's and Hax and Wilde's strategies. Future Studies Research Journal: Trends and Strategies, 2(2), pp. 17-35. [ Links ]
[9] Wipperfurth, A., Savary, K. & Gilchrist, A. 2010. Microecomonics of competitiveness. University of Minnesota - Minnesota Medical Device Cluster. [ Links ]
[10] Olawale, F. & Garwe, D. 2010. Obstacles to the growth of new SMEs in South Africa: A principal component analysis approach. African Journal of Business Management, 4(5), pp. 729-738. [ Links ]
[11] Kunene, T. 2008. A critical analysis of entrepreneurial and business skills in SMEs. PhD Thesis. Pretoria: University of Pretoria. Available online: https://repository.up.ac.za/handle/2263/24173?show=full [ Links ]
[12] Herrington, M. & Wood, E. 2009. Global entrepreneurship monitor: South African report. Cape Town: University of Cape Town Graduate School of Business. [ Links ]
[13] Beck, T. 2007. Financing constraints of SMEs in developing countries: Evidence, determinants and solutions. World Bank Development Research Group. [ Links ]
[14] Gaviria, A. 2002. Assessing the effects of corruption and crime on firm performance: Evidence from Latin America. Emerging Markets Review, 3(3), pp. 245-268. [ Links ]
[15] Saidi, T. & Douglas, T. 2018. Medical device regulation in South Africa: The Medicines and Related Substances Amendment Act 14 of 2015. South African Medical Journal, 108(3), pp. 168-170. [ Links ]
[16] Republic of South Africa. 2016. Medicines and Related Substances Amendment Act, 2015 (Act No. 14 of 2014). Government Gazette No.39585. Pretoria. [ Links ]
[17] South African Health Products Regulatory Authority. 2015. Guideline for a licence to manufacture, import, export or distribute medical devices. SAHPRA. [ Links ]
[18] Wilkinson, D. & Brimingham, P. 2003. Using research instruments: A guide for researchers. 1st ed. RoutledgeFalmer, London, UK. [ Links ]
[19] Marshall, M. 1996. Sampling for qualitative research. Family Practice, 13(6), pp. 522-526. [ Links ]
[20] Patton, M. 1990. Qualitative evaluation and research methods. 2nd ed. Sage Publications, Thousand Oaks, California. [ Links ]
[21] Hseif, H. & Shannon, S. 2005. Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), pp. 1277-1288. [ Links ]
[22] Elo, S. & Kyngas, H. 2008. The qualitative content analysis process. Journal of Advanced Nursing, 62(1), pp. 107-115. [ Links ]
[23] Walk, K. 1998. How to write a comparative analysis. Harvard: Harvard College Writing Centre, Harvard University. [ Links ]
[24] Rankin, K. & Bertrand, J.C. 2005. Guidelines for ethical conduct in participant observation. Toronto: Social Sciences and Humanities Research Ethics Board, University of Toronto. [ Links ]
[25] Vinten, G. 1994. Participant observation: A model for organizational investigation. Journal of Managerial Psychology, 9(2), pp. 30-38. [ Links ]
[26] Lincoln, Y. & Guba, E. 1985. Naturalistic enquiry. 1st ed. Sage Publications, Beverly Hills, California. [ Links ]
[27] Creswell, J.W. & Miller, D.L. 2000. Determining validity in qualitative inquiry. Theory into Practice, 39(3), pp. 124-130. [ Links ]
[28] Golafshani, N. 2003. Understanding reliability and validity in qualitative research. The Qualitative Report, 8(4), pp. 597-607. [ Links ]
[29] Burke Johnson, R. 1997. Examining the validity structure of qualitative research. Education, 118(2), pp. 282-292. [ Links ]
[30] Morse, J., Barrett, M., Mayan, M., Olson, K. & Spiers, J. 2002. Verification strategies for establishing reliability validity in qualitative research. International Journal of Qualitative Research, 1(2), pp. 13-22. [ Links ]
[31] Cough Ian, M., Cronin, P. & Ryan, F. 2007. Step-by-step guide to critiquing research. Part 2: Qualitative research. British Journal of Nursing, 16(11), pp. 738-744. [ Links ]
[32] Republic of South Africa. 2005. National Credit Act (No.34 of 2005). Government Gazette No.28619. Pretoria. [ Links ]
* Corresponding author: ishanmaharaj20@yahoo.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}