









Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Industrial Engineering
versión On-line ISSN 2224-7890
versión impresa ISSN 1012-277X
S. Afr. J. Ind. Eng. vol.23 no.2 Pretoria ene. 2012
CASE STUDIES
The pen is mightier than the scalpel: the case for electronic medical records#
D. HartmannI, *; S. SooklalII
IThe author was enrolled for an MSc. Eng (Industrial) degree in the School of Mechanical, Industrial and Aeronautical Engineering at the University of the Witwatersrand. School of Mechanical, Industrial and Aeronautical Engineering University of the Witwatersrand, South Africa. Dieter.Hartmann@wits.ac.za
IIThe author was enrolled for a BSc. Eng (Industrial) degree in the School of Mechanical, Industrial and Aeronautical Engineering at the University of the Witwatersrand
ABSTRACT
A case study evaluated how physical medical records are managed and curated at a large tertiary hospital. It was found that the current microfiching technology was outdated, ineffective, and in many cases an impediment to appropriate care. Alternative record-keeping techniques were evaluated. A proposal for a localised electronic medical record (EMR) system, disseminated by tablet computer, is presented in this paper. Issues about ethics and access to information are explored, and some of the issues that have affected global implementation are highlighted.
OPSOMMING
'n Gevallestudie wat handel oor die bestuur van mediese rekords van 'n tersiêre hospitaal word voorgehou 'n Voorstel word gemaak om die bestaande datastelsel te vervang met 'n elektroniese rekordstelsel. Etiese- en toegangsaangeleenthede word behandel.
1. INTRODUCTION
The methods of data storage and patient record management at a South African tertiary hospital were investigated. This paper explores the feasibility of using electronic medical records at this site [1], and further investigates what would be necessary for their implementation, both on a single-site basis and for a wider network. Impediments to implementing centralised systems are highlighted, and issues concerning ethics and access to information are explored.
Excessive waiting in hospitals can be caused by wasteful processes before or during treatment. This includes time spent waiting for medical records.
Medical records allow for continuity in treatment, and enable a smooth patient hand-over between medical professionals. Records mitigate risks that might otherwise arise when medical professionals are not personally familiar with the medical histories and needs of their patients [2].
It is vital to have a robust, accurate, reliable, inviolable, and accessible medical record system that is easily shared and understood. Medical records must not degrade or become otherwise inaccurate over time.
1.1 Objectives
This research is intended to:
- critically evaluate the current state of a hospital's health record system;
- establish global best practice in record storage and management;
- determine the desirability of introducing more technological record storage mechanisms; and
- quantify the benefits of alternative systems.
2. METHODOLOGY
A single case study [3] was conducted at a South African public hospital. The current state of data storage was investigated using qualitative and quantitative methods [4]. Direct observation [3], data base extraction, and work studies were employed. The deficiencies were evaluated, and recommendations for systematic improvements were made, based on international best practice from the literature. From this, a sample feasibility and implementation plan was constructed. This concentrated on cost implications (especially on a break-even analysis), ethical issues, and infrastructural feasibility. This was then extrapolated to a more generalised level for the South African context, and identified the lessons learned that might require further research.
3. CURRENT SITUATION
The medical records department is the curator of all medical records created in the hospital under study. It occupies more than 400 square metres, and employs 46 people, of whom 39 fulfil a clerical role; the rest are messengers. The total wage bill is R3,000,000 p.a., and the overall budget amounts to R4.5 million p.a. [5], excluding the cost of the paper used for record-keeping.
The department has two roles: storing medical records, and issuing them when requested. These functions differ in terms of criticality. Storing is less time-critical than issuing; treatment without records may be dangerous or compromise a patient's health, while delayed storage should not.
Documents are stored on microfiche in a system introduced in 1980 [5]. Creating microfiche requires several steps. A document is photographed and chemically developed to be 9003 times smaller than the original document. The negative is mounted on a card, and the original is destroyed by shredding. Cards are stored in a numerically-indexed library system. Retrieval requires that a positive of the microfiche be generated and printed to paper.
Microfiche technology represented a compact and simple storage and management solution before the advent of affordable computerisation. Now, however, it is out-dated. Despite the technological deficiencies inherent in this system, it remains functionally adequate. There are, however, concerns related to access to information, particularly speed of access, data integrity, and the ultimate quality and legibility of records.
The department stores about 50,000 records per day, and issues about 2,000. The significant difference between the number of stored and issued documents is curious, and points to the fact that doctors were disinclined to request medical records for every patient. Retrieving documents took too long, and thus they were of little value by the time that they had arrived. Due to their limited contact with each patient, doctors generally didn't have the time to read records. For a range of reasons, doctors often assume the content of the record, or rely on medical information - including precise condition and treatment history - from the patient, who is in many cases uneducated.
3.1 Problems experienced
Several issues relating to document quality, reliability of the technology, and speed of service were identified.
The process is slow. The average retrieval time for booked records was 52 minutes per delivery, while emergency retrievals took 13 minutes on average. Both of these times are further compounded by runners4 who deliver documents in the hospital. This adds a further 27 minutes to the process, and particularly in emergency cases, it can delay or compromise the safety of the treatment. Because of these delays, the file-opening station preferred to open new files rather than call up an existing record for the patient. The file-opening process, however, is also slow: it takes an average total time of 57 minutes per patient [6].
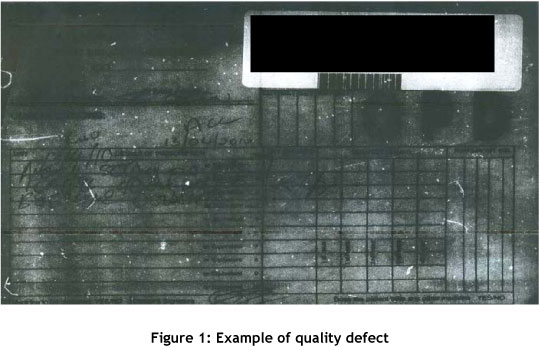
Several quality issues were identified, relating to both technological and procedural matters. Figure 1 shows an example of the type of quality defect that is possible. This kind of issue is common, and renders the patient record worthless. This is an example of a problem with exposure, which may have been caused at either the photography or the development stage. Other issues include documents that are out of focus, microfilm that has been cut across a record, or instances where the film is otherwise damaged - for example, scratched or kinked. In all these cases, the document is irreparable and therefore deemed 'lost'.
Filing microfiche is problematic. It can be placed in the incorrect envelope, or envelopes can be filed in the wrong shelf-position, or individual microfiche sheets can be lost or misplaced. Such records are deemed to be irretrievable, and so are also considered 'lost'.
The records department uses large amounts of paper. The records arrive on paper, which is microfiched, and the original is destroyed. On retrieval, the patient record is reprinted on paper, the record is augmented by doctors, and again microfiched. The current carbon footprint of the paper operations of the hospital was calculated to be at least 300,000 kg of CO2e p.a. This was calculated only on the value of the paper consumed, and excluded paper transportation cost from the mill, the inefficiency of the mill, and the actual carbon footprint contribution of the printing process. Our conservative estimate is that the actual carbon footprint of paper operations is at least double this value.
Most documents scanned arrive as DIN A4. However, in the absence of standardised document sizes, up to 10% of them arrive in other sizes, thicknesses, or colours, making standardisation difficult and causing paper jams.
The 35-year-old machines have frequent breakdowns. Most spare parts are no longer available, and therefore need costly rebuilds or hybridisation. Service technicians are scarce.
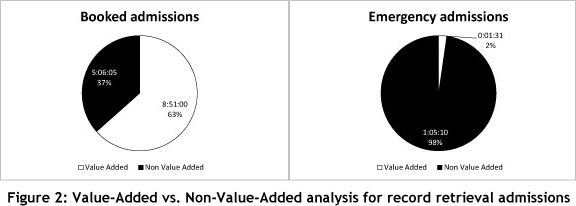
Value-stream mapping the unit showed that non-value-adding (NVA) steps account for about 40% (see Figure 2). Waste is largely due to movement. As can be seen for emergency admissions, the NVA component is overwhelmingly larger (98%). This is due to the time that the runner takes - more than an hour - to deliver the document.
The lack of trust in the central system has caused some specialist departments to keep their own records. This exacerbates the problem, as there are multiple versions of patient records. Treatment continuity is consequently prejudiced.
4. SOLUTIONS FOR PATIENT RECORD STORAGE
This paper explores three categories: the input method and storage format; the dissemination medium; and storage locations.
4.1 Input and format
The modern equivalent to microfiching is document imaging: a document is scanned and saved in picture format. Retrieval and reproduction in document imaging is materially faster, reducing lead time. The human resources required to operate the system are lower, as searching and maintaining the library are eliminated. The quality and integrity of the document may be better, while the number of lost and misfiled documents will be negligible. Being an evolved form of microfiching, however, means that images remain uneditable and unsearchable, and the technology relies on the use of paper.
An alternative is a full text record, which saves records where possible in an editable format. The advantages of this vary. Digitised content results in smaller files and allows physicians to search for content. A major drawback is that the burden of creating text records will fall either to the doctors [7] - who are usually unwilling to take on the role of typing (as opposed to hand-scribbling) records - or data capturers, who would be responsible for transcribing doctors' handwritten notes about a patient. Because of the volume of around 50,000 documents per day in the current system, this would require significant human resources. Unfortunately optical character recognition (OCR) is not an option, as the records are hand-written, thus perpetuating the reliance on paper.
4.2 Storage
Three options exist for storage location: national, local, and patient-borne databases.
The national option is a centralised national health record database, such as has been established in Denmark [8]. Each individual's medical history is stored centrally, and is accessible to any medical professional, from those in large hospitals to private practitioners. The benefit of such a system is that accurate and comprehensive medical information is available to all clinicians, thus reducing the danger of 'missing something' during diagnosis. The greatest difficulty of implementing such a system is the complex architecture: this system requires a significant investment in hardware, software, and ICT professionals to create, administer, run, and maintain it.
A second, less intensive method of storage is to have a local server at each hospital. This is a less complex system than a national one. However, significant duplication occurs, and it may potentially lead to site-specific document customisation occurring, rather than standardised medical records. As there is no way to prevent patients from having records at more than one facility, there may be discontinuous medical information on the patient.
A third option is to store patient information on a medium that is carried by the patient. The South African Department of Home Affairs has discussed the introduction of a 'smart' identification card for South Africans [9], which will be able to store personal, biometric, licence, and other information [10]. This information may include medical information. This storage system is useful, as it places the patients' records under their personal curatorship; and whenever patients have their card with them, their full medical records are available. Several precautions would need to be taken, particularly in safeguarding medical records on these cards from unauthorised access, and also ensuring that complete record loss does not occur if patients lose their ID. Any such system would therefore need adequate access control and back-up solutions.
None of the three options is sufficient by itself. All have deficiencies: these include the skills required, the ICT infrastructure needed, or issues of document safety and recoverability.
The risk inherent to electronic patient records is highlighted by Valli [11], who warns of the dangers of such records being hacked or otherwise compromised. He points out that encryption and suitable protection systems are available, but these should nevertheless be augmented by making sure that only physicians who have a legitimate reason to access a patient's records are able to do so.
4.3 Dissemination media
The final major issue in setting up a new patient record system is the choice of the dissemination medium - that is, how doctors will access these records. Here we can distinguish between two options: a traditional paper format, or an electronic dissemination format.
The use of paper is the most common way of disseminating patient records. The difficulty of moving away from paper is one of the greatest impediments to implementing electronic medical records [12] [13]. The advantages of paper records are that they are physically tangible, easily editable by writing on them, and easily understood and circulated among people who work closely together.
If paper records are favoured, then the decision needs to be made whether to print centrally or locally. If printing records remains centralised with the record department, the losses implicit in manually running paper within a hospital will remain, but the large printing infrastructure will benefit from economies of scale. If printing were done at ward level, documents would be accessible more quickly. However, the associated cost of additional staff and ICT infrastructure in each ward would need to be considered. This would include localised breakdowns and the maintenance strategy necessary to deal with this.
The institution that was investigated for this study uses at least twenty boxes of paper per day. This means that the hospital spends about R10 million annually on paper, the bulk of which is destroyed. This excludes the additional cost of custom-printed stationery. Paper, though traditionally appealing, is far from ideal, as it can only be in one place at a time, and poses the risk of there being different versions of patient records. Paper furthermore requires intensive archival effort to ensure that records remain legible and recoverable.
Early implementers of fully electronic patient records used a conventional laptop computer that could be wheeled around. This solution was found to be adequate, and was successfully adopted in at least one hospital in the USA [12], as can be seen in Figure 3.
Some hospitals in the USA and Europe have equipped doctors with tablet computers or smart phones so that they can access medical records at the bedside [14]. The speed and convenience of accessing records in this way makes doctors more likely to use them. Such records would be editable and updated in real time, and with the wireless infrastructure they would be available to any other medical professional also involved in the treatment of that patient. This system is updated by the medical professionals. Maintenance, however, becomes a crucial function. The hospital would have to invest in skills to ensure that this system remained functioning, and did not 'go down' - which could be literally a matter of- life or death. Management would have to ensure the 'buy in' of doctors and nurses, as their participation would be fundamental to the success of such a system.
5. ETHICAL CONSIDERATIONS AND ACCESS TO INFORMATION
Keeping health records and maintaining confidentiality and patient privacy is required by law, both globally and in South Africa [2] [15]. Systems need to maintain patient confidentiality so that, within reason, medical information may even be withheld from other treating physicians if this is deemed appropriate [16].
Ease of access to electronic medical records is possibly the single greatest benefit of such a system, though it is also one of its greatest inherent risks. Many fear that security and confidentiality will be weak in electronic health records [17]. In a large network, such as the internet, records are potentially vulnerable to being accessed illegitimately or inappropriately [18] by unauthorised people.
The parallels between electronic and physical records seem tenuous, but they are similar, because both forms of record need to be generated, preserved, stored, kept safe, shared appropriately, and destroyed in a controlled manner when necessary.
Physical records are not accessible worldwide, and are physically and geographically constrained. This means that a document can only be violated if the violator is in the space where the record is. Nevertheless, the safeguard for physical records remains fallibly human. This means that a lock pick, a corrupt filing clerk, or someone carelessly leaving files lying around can undermine document security5.
To secure electronic patient data, access to information must be rigorously managed by setting up rights, and by retaining the medical professional as the person who decides on the extent of record sharing, as it is the doctor's duty to maintain patient confidentiality. With these measures in pkace, the confidentiality of electronic records would be at least as secure as physical records.
To draw a parallel: electronic safeguards protect worldwide banking data, and it is generally agreed that breaches of banking security are usually traceable to irresponsible client behaviour [19]. Unscrupulous individuals who have legitimate access to documents and who are thus able to disseminate records remain the biggest threat to data integrity [17]. However, random, accidental, or incidental access may occur less often than with the hard copy system.
5.1 The role of the State Information Technology Agency (SITA)
The State Information Technology Agency was created in 1998 by an Act of the South African Parliament [20], and later amended [21]. The agency is responsible for providing ICT support, systems, and related systems to government departments as needed [20]. The requirements of a national data system would fall within the ambit of section 7 of the Act [20]. However, the SITA may be excluded from the development of localised systems, as these would be administrative site functions rather than systematic government support functions. Future development would require the involvement of the SITA as a data integrator, and would centralise security and control of medical information in line with the SITA's mandate [20].
6. INTERNATIONAL PERSPECTIVE ON CENTRALISATION
Developed nations, primarily those in North America and in Europe, are establishing universal and comprehensive medical information systems. Many have attempted to implement national health record systems. Very few have succeeded in full. Attempts in developed economies have been costly [22], slow, and not yet universally successful [23].
Electronic medical records in developing countries, by contrast, are usually characterised by very small networks or containing limited information. 'AMRS' in Kenya [24] and 'Careware' in Uganda [24] both have two sites, and 'EMR' in Malawi [24] has only one. Dispersed networks were found only in Brazil, where a nationwide drug-control system (SIClOM) monitors prescriptions [24]. A literature search found no geographically wide information-rich EMR systems in the developing world.
Introducing centralised medical records in South Africa may be an overly ambitious venture, particularly in light of the fact that this country has a large and widely dispersed population, with vastly diverging levels of development. Countries that have been successful to an extent tend to be either physically small (like Denmark) or have small populations (such as Norway or Saudi Arabia), or both (such as Estonia). Common to all these nations is that they have a 'very high' human development index (HDI) [25]. By comparison, South Africa's HDI is 'medium', which is mid-range (ranked 110th of 169 countries).
The authors view implementing a nationwide system as unwise, as it lacks competently implemented international role models. Caution should nevertheless be applied before summarily rejecting the notion of a future universal health record system. Instead, configuration management should be introduced, including standards for future integration.
7. THE NEW SYSTEM
Switching over to and implementing the new system will need to be phased. This paper proposes, in the light of the archival rigorousness of modern computing power, that an electronic storage and indexing system would be a more suitable method to administer medical records in this particular hospital. It would be a text-based, locally-stored system; medical practitioners would enter the data using suitable wireless devices. These records would be centrally stored on a server maintained by a local ICT specialist. Records would be regularly backed up off-site.
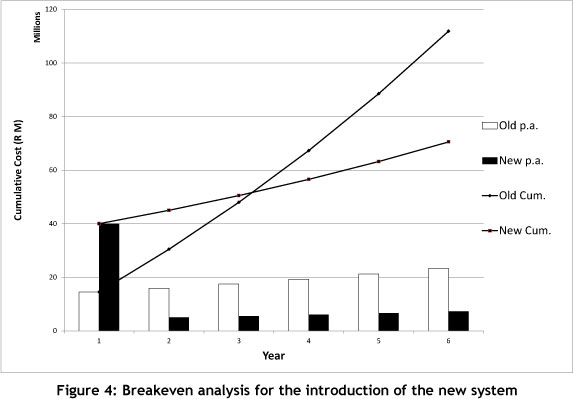
Introducing the system would cost roughly R35 million to install the necessary infrastructure. The system would use the existing LAN backbone.
A breakeven analysis (Figure 4) shows the implementation and running costs of the new system compared with the existing one, and indicates that breakeven for the new system would be after about three-and-a-half years. Cost escalation in both cases was estimated at 10% p.a., which is consistent with recent medical record department budget increases.
The staff required to implement the new system would be drastically reduced: the department could now be serviced by three ICT specialists, rather than the current staff of 46. Staff could be redeployed elsewhere in the hospital. This would reduce the salary budget from about R3 million p.a. to about R800,000 p.a. The paper cost to the institution would reduce by roughly R10 million p.a.
8. DISCUSSION
A costly, out-dated, maintenance-intensive infrastructure needs high levels of skill, yet it only produces sub-standard documents slowly, with random data loss, misfiling, and high paper usage. A lack of standardised reporting formats makes efficient data capture problematic. An unwillingness to engage the inefficiency of the medical record department explains why there is a huge difference between the number of records requested and the number of records stored daily.
The cost of introducing the system is estimated at R35 million, which includes the installation of wireless equipment that would piggyback on the hospital's existing LAN6. The principal cost would be for the purchase, installation, and maintenance of the servers and- the wireless infrastructure, and the purchase of reading and editing devices. Electronic medical record storage reduces the overall cost of producing medical records, as the technology is paperless.
There is a concern that the new system would slow doctors down. The old system mostly saw doctors using no records for their consultations, and then scribbling notes when necessary. The new system might induce doctors to make use of medical records far more regularly, and then have to type up notes related to the case. Typing might slow down the care process somewhat, perhaps leading to increased queues. However, this is likely to be offset by the improved quality of care that EMR can bring [26]. This improved care may reduce the incidence of failure demand - i.e. where incorrect treatment requires a patient to return with the same condition. We suspect that this would reduce the number of cases where treatment has caused harm.
We believe that the increased ease with which records could be accessed would result in their being used more. We have no basis for predicting a significant increase in requested volumes, but this is a reasonably likely scenario. Our expectation is that there would be a demand on the new system for 20,000 documents per day.
Introducing centralised medical records in South Africa would be a highly ambitious venture, particularly in light of the fact that we have a large, widely-dispersed population, with vastly diverging levels of development.
It is our opinion that the optimum would be to create a localised system in hospitals that took over the role of the current physical record department. Such a record system would need a common medical record (CMR) standard and a standardised vocabulary for future integration [18].
9. CONCLUSION
Use of document imaging, whether computer-based or on microfiche, is out-dated and ineffective because such images cannot be searched or edited. Introducing a locally-stored, full-text-plus-picture, tablet-computer-disseminated EMR system to the hospital in question would be wise and cost-effective.
Such a system significantly reduces the space and infrastructure dedicated to medical record storage. The risk of lost, misplaced, illegible, damaged, or otherwise useless documents is virtually eliminated. The reduced reliance on paper records should save at least R10 million p.a., and reduce the hospital's carbon footprint by at least 300,000kg of CO2e p.a. Such a system should break even after a period of less than four years, and significantly reduce maintenance and associated costs.
Simplifying access to medical records would encourage their use, which in turn should improve the quality of treatment and care. Real-time access to, and editing of, records improves the ability of medical professionals to collaborate on patient treatment.
South Africa's level of development is insufficient to adopt a national centralised electronic medical record system. In anticipation of future integration, the record system must conform to standards of diagnostic language and format. The State Information Technology Agency would become involved at the point of integration, and consultation at this level of development would be wise.
10. FUTURE WORK
To implement this work fully, the IT infrastructure and the official policy need to be addressed.
The ICT infrastructure has been described superficially; however, it is in need of detailed design, and should particularly focus on three areas. First, the database needs to be designed, being guided by medical professionals in respect of structure and desired fields. Second, network security must be designed to give easy access to authorised medics and to block all other attempts to access data. Third, the interface with which medics will interact must be designed to allow user-friendly and intuitive access to the information contained in the database.
On a policy level, three important aspects present themselves. First, legislative changes need to be made to the National Health Act explicitly to permit web-based electronic medical records. Second, it is important that a long-term policy decision is taken to develop an electronic health record standard, accompanied by a roadmap to realise eventual universal coverage for South Africans. Third, it is necessary to implement ventures that improve efficiency in healthcare generally and in patient record management specifically.
REFERENCES
[1] Hartmann, D. & Sooklal, S. 2011.The pen is mightier than the scalpel. International Conference on Industrial Engineering, Systems Engineering, and Engineering Management, Stellenbosch. [ Links ]
[2] Health Professions Council of South Africa. 2007. Guidelines for good practice in the healthcare professions. HPCSA, Pretoria. [ Links ]
[3] Yin, R.K. 1987. Case study research: design and methods, 6th ed. Beverley Hills: Sage Publications, Inc. [ Links ]
[4] Fuller, S.S. & Watt, R. 1992. Using qualitative and quantitative research to promote oral health, 1st ed. London: Eden Bianchi Press. [ Links ] [5] Sooklal, S. 2010. As-is analysis of the data systems in a public hospital. University of the Witwatersrand, Johannesburg, final year project. [ Links ]
[6] Jagjiwan, S. 2010. Improving the file opening procedure at a public hospital. University of the Witwatersrand, Johannesburg, final year thesis. [ Links ]
[7] Shortliffe, E.H. 1999. The evolution of electronic medical records. Academic Medicine, 74(4), 414-419. [ Links ]
[8] Timmins, N. 2009. System upgrade. Financial Times: Health, 2, 20-23. [ Links ]
[9] SA Press Association. 2008. Smart card ID to be launched soon. The Star, February 2008. [ Links ]
[10] Beharie, S. 2006. SA to get 'smart' with new ID system, The Star, February 2006. [ Links ]
[11] Valli, C. 2006. The insider threat to medical records: Has the network age changed anything? Edith Cowan University, Mount Lawley. [ Links ]
[12] McDonald, C.J. 1997. The barriers to electronic medical record systems, and how to overcome them. Journal of the American Medical Informatics Association, 4, 213-221. [ Links ]
[13] Sheldon M.R. & Wentzel, R.P. 1999. Electronic medical record systems at academic health centers: Advantages and implementation issues. Academic Medicine, 74,(5), 493-498. [ Links ]
[14] Müller, M., Frankewitsch, T., Ganslandt, T., Bürkle, T. & Prokosch, H.-U. 2004. The clinical document architecture (CDA) enables electronic medical records to wireless mobile computing, Medinfo, 1448-1451. [ Links ]
[15] Parliament of the Republic of South Africa. 2003. The National Health Act. Government Gazette, 469. [ Links ]
[16] Kluge, E.-H.W. 2004. Informed consent and the security of the electronic health record (EHR): Some policy considerations. International Journal of Medical Informatics, 73(3), 229-234. [ Links ]
[17] National Research Council. 1997. For the record: Protecting electronic health information. National Research Council, Washington D.C. [ Links ]
[18] Kohane, I.S. et al. 1996. Sharing electronic medical records across multiple heterogeneous and competing institutions. AMIA, 608-612. [ Links ]
[19] Abad, C. 2005. The economy of phishing: A survey of the operations of the phishing market. First Monday, 10(9). [ Links ]
[20] Parliament of the Republic of South Africa. 1998. State Information Technology Agency Act. Government Gazette, 400. [ Links ]
[21] Parliament of the Republic of South Africa. 2002. State Information Technology Agency Amendment Bill. Government Gazette, 28 021. [ Links ]
[22] Gunter, T.D. & Terry, N.P. 2005. The emergence of national electronic health records architectures in the United States and Australia: Models, costs and questions. Journal of Medical Internet Research, 7(1). [ Links ]
[23] Jha, A.K. et al. 2009. Use of electronic health records in US hospitals. The New England Journal of Medicine, 360, 1628-1638. [ Links ]
[24] Fraser, H.S.F. et al. 2005. Implementing electronic medical record systems in developing countries. Informatics in Primary Care, 13, 83-95. [ Links ] [25] UNDP. 2010. Human development index rankings. United Nations Development Programme, New York. [ Links ]
[26] Baron, R.J. 2007. Quality improvement with an electronic health record; achievable but not automatic. Annals of Internal Medicine, 147, 549-552. [ Links ]
[27] Hartmann, D. & Mandavha, R. 2010. Lean healthcare, a casualty of inefficiency. SAIIEConference. [ Links ]
[28] Parliament of the Republic of South Africa. 1998. Medical Schemes Act. Government Gazette, 131. [ Links ]
[29] Minister of Transport. 2007. Questions related to eNatis. Department of Transport, Parliament of the Republic of South Africa, Cape Town, Parliamentary Q and A session N867E. [ Links ]
[30] Bramley, S. 2001. Medical records and the law. BJU International, 86, 286-290. [ Links ]
[31] Denzin, N.K. & Lincoln, Y.S. 1994. Handbook of qualitative research, 1st ed. Thousand Oaks: Sage. [ Links ]
[32] US Environmental Protection Agency. 2006. Solid waste management and greenhouse gases: A life-cycle assessment of emissions and sinks. EPA, EPA530-R-06-004. [ Links ]
* Corresponding author.
# This article is an extended version of a paper presented at the 2011 ISEM conference.
3 In area. Typically a DIN A4 sheet of paper will be reduced to less than 10 mm x 10 mm.
4 In most cases the term is very inappropriate.
5 A good example of this was the sale and subsequent publication in the media of the medical records of the South African Minister of Health, Dr Manto Tshabalala Msimang [3].
6 The LAN is old and may need to be upgraded in future. This cost is excluded.

