










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkStellenbosch Papers in Linguistics Plus (SPiL Plus)
On-line version ISSN 2224-3380
Print version ISSN 1726-541X
SPiL plus (Online) vol.64 Stellenbosch 2022
http://dx.doi.org/10.5842/64-1-927
ARTICLES
Metacognition and the complex process of developing identities via a second language: addressing the challenges healthcare professionals are facing in a multilingual context
Christine Fourie
Department of Linguistics, University of Antwerp, Belgium | Language Centre, Stellenbosch University, South Africa E-mail: christine@sekelmaan.com
ABSTRACT
This qualitative study takes into account that healthcare professionals are increasingly required to function in a multilingual environment where they often have to communicate with patients in a second or third language (Ushioda & Dörnyei 2009, Burford 2012). In this regard the identity of the healthcare worker can be compromised, as identity is interrelated with language (Joseph 2004, Gollin-Kies et al. 2015, Skjeggestad et al. 2017). Therefore, communication training courses in the healthcare context should accommodate professional identity formation processes, as a healthy identity would support stress and change management (Monrouxe 2009, Goldie 2012, Mavor et al. 2014). Data was collected during two separate courses: firstly at Stellenbosch University, South Africa, where medical students took part in a communication training course in Afrikaans and secondly when nurses in Antwerpen, Belgium took part in a similar communication training course in English. Both courses followed a blended learning approach and for each course an online community of practice via Facebook was utilised. Data was analysed according to the principles of grounded theory. Metacognitive markers that support the identity formation process were identified during the first course and refined for the second course. The result is a framework that supports both metacognitive awareness and the manifestation of metacognition that could facilitate the professional identity formation process alongside the process of language learning for healthcare purposes.
Keywords: healthcare communication; blended learning; multilingualism; identity; medical communication training; language for specific purposes
1. Introduction
A healthy sense of self or healthy identity is associated with improved well-being, as well as an improved ability to deal with stress and change (Monrouxe 2009, Goldie 2012, Mavor et al. 2014). The professional healthcare context often requires healthcare professionals to deal with stress and change, and a healthy identity would therefore be beneficial to such professionals. However, identity is interrelated with language (Joseph 2004:11) and it is therefore not surprising that the identities of healthcare workers who have to communicate in a second or third language, are often compromised (Skjeggestad et al. 2017).
In multilingual South Africa a study was conducted in 2014 among a group of first year medical students, whose developing identities were challenged by the changes normally associated with academic acculturation, as well as by the fact that they had to cross linguistic and cultural barriers (Fourie 2015). These students all took part in a medical communication training course. A blended learning approach was used that included an autonomous online platform, face-to-face teaching and a closed Facebook group. During this course certain metacognitive markers were identified that supported the identity formation process of these students.
Following upon this research, a study was conducted in Belgium in 2016 when nursing students followed a communication training course with a similar structure and blended learning approach. The metacognitive markers identified during the South African study were used with a specific focus on the Facebook community of practice. Based on the results from this study, a framework was developed to support the metacognitive development of the identity of a healthcare worker in a second language context.
2. Literature Review
2.1. Identity and (second) language
Identity is a commonly used term, referring in general to an individual by name and in doing so, singling out that person from others, but the term also refers to "who that person really is" or self-identity (Joseph 2004:3). Apart from self-identity, group or communal identities also exist, pointing for instance at ethnicity, gender, religion and profession. However, self-identity can consist of various group identities, in which a person can participate. For example Christine (self-identity) is a female (group identity) South African (group identity). Group identities are abstract in the sense that they do not exist without the individual identities they consist of, but at the same time they feed into the individual identity as the individual joins or discards groups (Joseph 2004). Therefore the individual identity is fluid in nature and in a constant process of transformation (Pratt et al. 2006, Roberts 2010, Goldie 2012, Rahimian 2015). In spite of this fluidity, the individual or self-identity can still be seen as singular and coherent (Joseph 2004).
Both individual and group identities are dependent on language as it is language that enables the individual to convey experiences in words. Language can furthermore enable the individual to reflect on the experience, beyond the experience itself. In this regard "language enables us to from a conception of self rather than simply being ourselves" (Joseph 2004:11). The interrelation of language, identity and culture (group identity) is well researched as evident in publications such as the comprehensive Routledge Handbook of Language and Identity (Preece 2016). This article will concentrate on the role of language in identity from an applied linguistic point of view and will mainly focus on the directly noticeable and discernible roles of language in people's lives, compared to philosophical and psychological points of view on language.
Linguistic research has shown that language can shape identity. At the same time identity can also shape language, for instance an individual can modulate speech depending on the audience and at the same time, an individual's notions about other people's identities can be based upon the way they speak. In this regard, identity and language are inseparable (Joseph 2004).
During the past two decades an increase in social, political and economical migration resulted in ever-increasing linguistic and cultural diversity in most parts of the world (Ushioda & Dörnyei 2009, Burford, 2012). For these migrating second language learners the relationship between language and identity becomes more pronounced as they will, by learning a new language, also invest in a new identity and new culture (Ushioda & Dörnyei 2009). Coetzee-Van Rooy (2006) warns that learning a new language does not imply that the new target language and identity is at the cost of the first language and "old" identity, but rather that multidimensional identities and pluralism exist in a globalised world. Migrating second language learners therefore have complex identities (Gollin-Kies et al. 2015). These identities are reproduced during interaction with others (Norton 2011). At educational institutions, where the medium of instruction is the student's second or third language, "[t]he relationship between identity and language intersects with teaching and learning in many spheres, including an individual's sense of belonging and affiliation to an institution, and with an individual's integration into the academic community of practice" (Leibowitz et al. 2005:34).
2.2 Identity of mobile medical (pre-)professionals
Healthcare students experience similar challenges with regards to their identity and academic acculturation, particularly with regard to the challenges that first year students face due to changes in, for instance, their academic, social and cultural contexts. Like all first year students, healthcare first year students have to engage with discipline-specific academic literacy so that they can participate fully in the process of genuine acculturation and academic integration (Van de Poel & Van Dyk 2015).
Healthcare students, like other (pre-)professionals, need to develop a professional identity, to enable them to function as individuals at work as well as members of communities (Pratt et al. 2006, Goldie 2012). The process of professional identity formation is on-going and self-reflective (Wilson et al. 2013) and develops when medical professionals learn more about their work and acquire a work-related self-esteem. An important aspect of this process takes place when they interact with a variety of individuals who can validate them as healthcare professionals (Ashmore et al. 2004, Pratt et al. 2006, Roberts 2010, Burford 2012). These interactions often have significant impact on the professional identities of individuals and occur while they attend institutions such as universities, hospitals, hospices and community care organisations (Goldie 2012). Apart from a professional (group) identity, healthcare (pre-)professionals also have various ethnic, family and social identities. The well-being of healthcare professionals is influenced by the conceptualization of these multiple identities (Mavor et al. 2014). Students and healthcare professionals who have a large number of group identities tend to be inclusive about membership, and demonstrate complex social identities. Social identity complexity can be a buffer to the stress normally associated with the daily work of healthcare workers and can furthermore assist these professionals to manage change, value social justice and exhibit empathy with others (Monrouxe 2009, Goldie 2012, Mavor et al., 2014).
In addition to the migration trends mentioned in 2.1 above, a considerable international migration of healthcare workers is taking place (Burford 2012, Gasiorek & Van de Poel 2012). As discussed in 1.1, learning a second language makes the interrelated nature of language and identity more complex and healthcare (pre-)professionals, who are also second language learners, are involved in complicated identity formation processes.
The intricacy of the second language healthcare worker's context is illustrated in current research. For example, researchers Gasiorek and Van de Poel (2012) report in their study on the importance of language in nurses' cross-cultural skills, and explain that nurses expressed high confidence in their nursing skills if communication with patients across cultures is in their (the nurses') first language, but that they feel significantly less confident about their nursing skills when they have to communicate with patients in a second language. These nurses perceive themselves to be less efficient as professionals if they have to communicate in a second language. In their earlier research the same researchers explored how mobile medical professionals perceived their communication with their colleagues in the host country and how these colleagues evaluated the communication of their second language colleagues. The research found important discrepancies between these groups' perception about the communication competency of the mobile medical professionals, and suggested that this should be addressed in communication training programmes that focus on language as well as culture related issues (Gasiorek & Van de Poel, 2012). The need for communication training programmes for healthcare professionals within a multilingual context is also emphasised by research done by Skjeggestad et al. (2017).
2.3 Communities of practice and interaction
Communities of practice are groups of people actively engaged with each other in order to support collective learning regarding a common interest (Wenger et al. 2002, Wenger 1998). Such communities can encourage collaboration and interaction amongst peers and between learners and lecturers. Since interaction is crucial in second language learning (Wang 2004, Larsen-Freeman 2013) and can lead to better learning outcomes than motivation, communities of practice can provide second language learners with the opportunity to engage in the process of learning (Pike et al. 2010, Norton 2011). Research has also shown that communities of practice dedicated to medical students can help students "to establish their professional identity and recognise their significant roles and responsibilities as medical students and their future roles as medical practitioners" (Burgess & Nestell 2014:406).
2.4 Metacognitive awareness about the self
Existing research explains why metacognition should be supported in the learning process. Metacognition develops alongside intelligence and is, compared with intelligence, a more accurate predictor of learning outcomes in face-to-face learning as well as in computer-based learning environments (Veenman & Spaans 2005, Veenman 2013). Metacognition evolves and manifests during the process of performing a challenging task (Schraw 1998). Furthermore, the benefits of metacognition can extend to the advantage of a community, as research suggests that people can share metacognition in a community of practice in order to improve the outcome of collective task performance (Shea et al. 2014).
Metacognition is often referred to as self-regulation to support task performance and learning (Veenman 2013). The working definition for this current research divides metacognition into two types of knowledge, namely declarative knowledge and procedural knowledge. Declarative knowledge is more stable and refers to "knowing when and what you know and do not know, including what you need to know" (Tarricone 2011:157). Declarative knowledge can further be divided into knowledge and awareness about the person or self as learner, knowledge about the task of learning and knowledge about strategies to solve challenges. Procedural knowledge, on the other hand, is dynamic and activated in the process of addressing a challenging task (Flavell 1979, Pintrich 2002, Tarricone 2011, Schraw 1998, Fourie 2015).
Taking into account that identity and a sense of self is the focus of this article, declarative knowledge about the person is defined in more detail: It refers to beliefs about oneself as a learner, as well as about the abilities and beliefs of other learners, as compared to oneself (Schraw 1998, Tarricone 2011). Accordingly, this self-knowledge includes intuitive knowledge, understanding and misunderstandings about one's own abilities and processes of learning, as well as about the abilities of others. It refers to beliefs about motivation and self-confidence and is a crucial basis for the development of other types of metacognitive knowledge (Flavell 1979, Pintrich 2002, Tarricone 2011).
2.5 Confidence and learner tasks and challenges
For the purposes of this research, self-confidence refers to a judgement by a person about own existing skills and abilities to address a task or challenge and is seen as a significant motivating and regulating factor of behaviour in order to reach a goal (Bandura 1977, Bandura 2012, Bjork & Druckman 1994). However, Bandura (1977) claims that alongside confidence, the necessary skills as well as incentives to perform or address a challenge, can influence learner behaviour positively. Furthermore, if a learner succeeds in a challenge, the experience will influence self-confidence levels (Bandura 1977, 2012). In this regard there is a relationship between learner self-confidence and learner experience or behaviour, so that self-confidence is a significant motivating factor when addressing a challenge, while the experience of addressing the challenge will impact on self-confidence (Bjork & Druckman 1994).
3. Research relevance, focus and context
3.1 Research relevance and focus
Taking the literature into account, it appears imperative that healthcare professionals need to be supported in their identity formation processes, and that linguistic relevance lies in the fact that identity is interrelated with language (Joseph 2004, Wilson et al. 2013). Furthermore, in a global environment, healthcare professionals are increasingly required to communicate in a second or third language (Burford 2012, Gasiorek & Van de Poel 2017). Their identity formation processes are therefore more complex than those of healthcare professionals who communicate in a first language with patients (using the same language for communicating). Apart from the interrelation with language, it should be taken into account that identity is not fixed, but fluid and comprised of multiple identities (Pratt et al. 2006, Roberts 2010, Goldie 2012, Rahimian, 2015). The personal well-being of healthcare professionals is also related to the conceptualization of their multiple identities (Mavor et al. 2014). Existing research suggests that an individual with multiple group identities will demonstrate improved well-being, as social identity complexity is known to be not only a buffer to stress, but also contributes positively to change management (Monrouxe 2009, Goldie 2012, Mavor et al. 2014). This is significant as managing both stress and change are key ingredients of a typical day in a healthcare student's and professional's life and, even more so, when they have to adapt to a new language and culture (of the patient, colleagues and/or institution).
Taking this into account, the present research focus was:
• Firstly, to establish what metacognitive awareness (declarative knowledge) and metacognitive skills (procedural knowledge) healthcare (pre-)professionals demonstrate about their developing identities during communication training;
• And, secondly, to explore what the effects of a training programme that incorporates these elicited metacognitive awareness identity markers has on healthcare (pre-)professionals' developing identities.
In order to address the research focus, two sets of data were collected. In 2014 data was collected during a communication training course for medical students studying at the University of Stellenbosch, South Africa. After the analysis of these research results, data was collected in 2016 during a similar communication training course with professional nurses as participants at the Artesis Plantijn Hogeschool in Antwerpen.
3.2 Participants
The participants in the first group were first year medical students at the University of Stellenbosch. These students (N = 35; 17 male and 18 female) were enrolled for a compulsory medical communication training course: 16 face-to-face hours (eight sessions in eight weeks), Medics on the Move (Van de Poel & Fourie, 2013) in Afrikaans. Afrikaans, together with English and Xhosa, are the three dominant languages in the Western Cape province of South Africa. The country has 11 official languages. At the time that the study was conducted, the University of Stellenbosch was a predominantly Afrikaans-medium university. English was the home language of eleven participants in this study, while the home languages of the remainder of the students were Tsonga, North-Sotho, Zulu, South Sotho, Xhosa, Pedi and Tswana. The students were all new to Afrikaans and their preferred medium of instruction was English.
The participants from the Antwerpen group took part in an English communication training course for nursing professionals at Artesis Plantijn Hogeschool, Antwerpen - a school for vocation training. The Nurses on the Move (Van de Poel & Fourie 2016) communication course in English was a graded component of a course which these students elected to follow as part of their professional bachelor's degree in nursing. The 23 participants (3 male, 20 female) were all practising nurses, all having completed a diploma in care. Dutch was the home language of 22 of the participants and Arabic the home language of 1 participant, while English was at varied proficiency levels. Before the start of the course they self-evaluated their spoken English abilities on a scale of 1 to 10 (where 1 - 3 is low and 8 - 10 is high) and the mean was 5, with a low of 2 and a high of 8 and a Standard Deviation at 1.86.
The teacher-lecturer was a participant observer during both courses. Although a native speaker of Afrikaans she is an experienced lecturer in English for specific purposes.
3.3 The components of the communication training courses
The base of the course used for the Stellenbosch group was called Medics on the Move (MoM) and the base of the course used for the Antwerpen group was called Nursing on the Move (NoM). The development of both courses was co-funded by the European Commission and each course was designed as an autonomous online communication training platform (Van de Poel & Fourie 2013, Van de Poel & Fourie 2016, Van de Poel 2016).
During both the Stellenbosch and Antwerpen courses the task-based syllabus of each online module was used as the core for the design of each course presented to students. A task-based syllabus consists of communicative tasks that encourage the use of specific aspects of the target language. Each course also utilised a closed Facebook group as a third learning platform, parallel with the classroom and autonomous online platforms. The MoM online course consisted of ten units which approximately follow the consultation timeline. Each unit consists of medical scenarios with corresponding sound, vocabulary, grammar and communication exercises. Similarly, the NoM online course consisted of five units that follow the key communication functions of nursing. The two courses contained a library with concise grammar, glossary and communication training resources (Van de Poel & Fourie 2013, Van de Poel & Fourie 2016).
The closed Facebook group in each group functioned as an online community and students had to perform tasks that were integrated with the work done in class as well as with the tasks and content of the autonomous online platform. In each instance the lecturer functioned as facilitator, though she retreated when students took initiative to, for instance, raise new questions, support each other and answer each other's questions. Although the positive outcomes of the various roles that members of a community of practice can play are well researched, the focus and scope of this article does not include these aspects of learning communities. Based on the metacognitive awareness that the South African students demonstrated via their Facebook community, the decision was made to direct the Antwerpen (NoM) students more specifically towards metacognitive awareness via tasks. These tasks contained a variety of instructions, such as instructions for tasks with a specific focus on raising awareness about students' personal needs that included the following:
• Introduce yourself
• Post how you feel about ...
• What did you like about...
• What did you find difficult about ...
In other tasks the focus shifted from the individual student to learning in general, especially in collaboration with others (the fact that all Facebook posts are visible to group members made this possible) e.g.
• Comment on what others posted ...
• You may agree with another student's response ...
• Take comments of others into account when you .
• What did you learn from .
Some instructions introduced and raised awareness about learning strategies, for example
• Take comments of others into account when you ...
• Edit your written response according to ....
• Advice on the future tense can be found in the First Aid Kit (online library with resources)...
• Write a language learning strategy for yourself to follow after completion of the course ... (Van de Poel & Fourie 2016).
4. The research process
4.1 Research approach
By exploring the impact of metacognitive markers on the identity formation process of healthcare professionals within a communication training context, a largely unknown learning context was being mapped. Therefore, the approach taken for this article was mainly qualitative as the research purpose was to explore the nature and impact of a training programme, rather than to test a theory or measure variables (Dörnyei 2007). In order to accommodate the flexibility needed to complement the scope of the research, an emergent research design was chosen. An emergent research design "refers to the fact that data collection and analysis can develop and be transformed as a consequence of what is learned during the earlier phases of the research" (Morgan, 2008).
4.2. Data handling procedure
4.2.1 Collection instruments
Typical of emergent research design, mixed methods were used and a variety of data sets were used (Charmaz, 2014). For both the Stellenbosch and the Antwerpen groups the following data sets were collected:
• Entries/posts from the relevant closed Facebook groups;
• Pre-course questionnaire with Likert scale and open questions on biodata and questions on language learning (for example what do you think would be the best way to learn a new language);
• Post-course questionnaire that included for instance an open question to evaluate the use of Facebook as part of the course;
• Recorded and transcribed post-course focus discussions (Stellenbosch group).
4.2.2 Data collection
For the Stellenbosch group, the questionnaires were completed individually on hard copy at the beginning and the end of the course. The focus group discussions were also conducted at the end of the course and transcribed. The data from the questionnaires as well as from the focus group discussion were then submitted to Survey Monkey Gold (www.surveymonkey.net).
For the Antwerpen group, the pre-course questionnaires were conducted on hard copy during the first class of the course and the post-course questionnaires were done online. The answers to open questions were translated and all the data was submitted to Survey Monkey Gold.
The Facebook posts from both groups were also copied in the form of Word documents.
4.2.3 Data handling procedure
In order to complement the emergent research design, the data was analysed according to the principles of grounded theory, since grounded theorists aim to analyse the data without preconceived ideas and therefore aim to code the meaning suggested by the data (Charmaz 2014). The analysis focussed on data collected as text and followed the three phases of coding that are outlined according to the principles of grounded theory (Dörnyei 2007).
The first phase of coding, open coding, is descriptive and often relies on gerunds with which actions are exemplified and identified (Dörnyei 2007, Charmaz 2014). This heuristic procedure keeps the focus on the data as well as on that which is still unexplained, as opposed to preconceived ideas. In this regard the purpose of the analysis shifts from focussing on known structures and theories to emergent processes and relationships (Charmaz 2014). The second step, or theoretical coding, takes open coding further as more abstract connections are identified - by categorising the most significant or most frequent earlier codes. In doing so, the theoretical direction of the emerging analysis progresses, although the codes are still directly related to the data (Charmaz 2014). The third phase, selective coding, exposes core categories and the relationships between the categories (Dörnyei 2007, Charmaz 2014). These conceptualisations can then be compared with existing research and the analysis can also be integrated into a (new) theory (Dörnyei 2007, Charmaz 2014).
See Tables A, B and C in Appendix 1 for examples of how the raw data from the Stellenbosch corpus developed from first to second and finally to third level coding.
Similar to the analyses of the Stellenbosch data, the Antwerpen data was developed from first and second level coding into third level coding. See Tables 1 - 4 below:
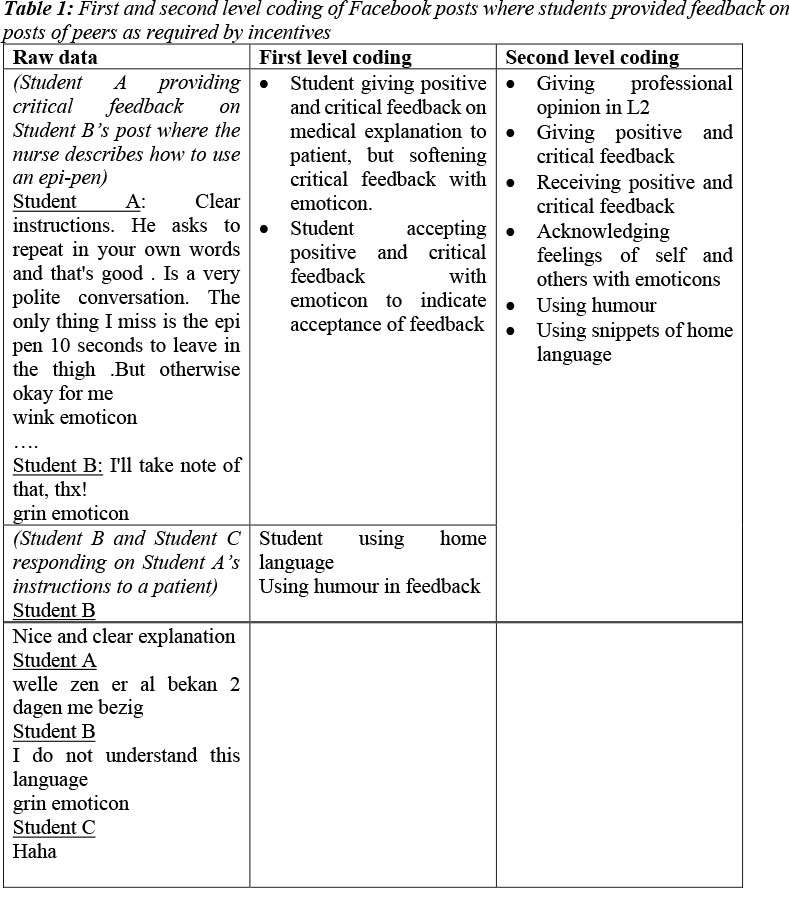


In Table 2 below Facebook posts that consist of students' reflections, not directly inspired by tasks given, were analysed and coded.
Reflections were also made by students in reaction to prompts and incentives contained by in prescribed tasks (see Section 3.3). Table 3 below contains examples of first and second level coding.
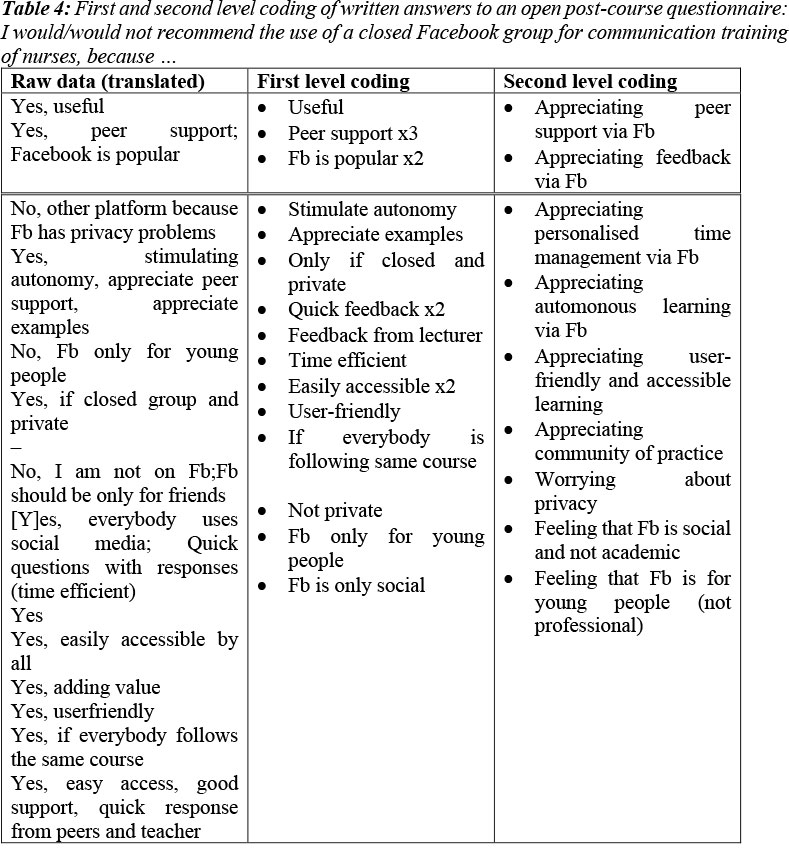
First and second level coding of written answers to a post-course questionnaire were added to the Facebook-data. See Table 4 below.
Table 5 below demonstrates how the Level 2 data from Tables 1 - 4 are conceptualised and compared with existing research, leading to Level 3 coding. It furthermore shows how a community of practice can facilitate metacognitive awareness to support the student's healthcare identity formation process while learning a second language in a blended learning environment. These results take into account that in order for metacognition to develop, both declarative knowledge (reflection) and procedural knowledge (interaction) are necessary learning processes. For a detailed description of how metacognition supports the identity formation process, see section 5 below.

5. Discussion
The results are discussed in two separate sections according to the stages in which the data was collected, followed by a general discussion.
5.1 The Stellenbosch data
The analysis of the Stellenbosch data provides an overview of the metacognitive awareness (declarative knowledge) regarding concerns and experiences of first year medical students from Stellenbosch University during a blended learning communication training course. Further, the metacognitive procedural knowledge that these students demonstrated facilitated positive outcomes that could support the development of their (pre-)professional identities. An overview of the various stages of the analysis process can be seen in Appendix 1.
These results, as set out in Table 6, indicate how students became aware of and counteracted potential threats.
5.1.1 The two metacognitive processes
By means of two processes, reflecting and interacting (Table 6, Column 2) these students could gain several positive outcomes to facilitate positive learning experiences and confidence (Columns 3 and 4). This could support the development of their (pre-)professional identities. For example, students perceived their learning through the programme as relevant (Column 3) with respect to their professional context - as one student explained: "it is ... relevant as it focused on body parts, how to greet patients, consultation stuff I am going to use in the near future when I interact with patients". The students mentioned that learning via the engaging and interactive tasks was relevant as well as authentic, and counteracted boredom and a sense of time wasting (see Table 6 - Columns 1 and 3). Within the context of these students' learning experiences, detachment refers to the linguistic and cultural barriers that existed between them and the majority of the students and lecturers who spoke Afrikaans. As a result, instead of being involved in social and learning experiences on campus, students were often removed from the reality of this experience and were uninformed (see Table 6 - Column 1b). This isolated them socially and academically from their fellow students (see Table 6 - Column 1c). The general feeling of isolation can be counteracted by peer and lecturer support (see Table 6 - Column 3c). Feelings of frustration and stress can be offset by the experience of being part of a community (see Table 6 - Column 3e). The learning community generated a warm and inviting atmosphere in which students did not feel trapped, but were willing to explore, even if this meant making mistakes (see Table 6 - Column 3f). Since it was enjoyable and fun at times, the work done in class and via the Facebook community balanced the stress normally associated with challenging tasks (see Table 6 - Column 3d). Finally, the contact sessions had a dynamic and flexible quality that relied on interaction and learning experiences occurring on different platforms, which added an "energetic" quality to learning (see Table 6 - Column 3b).
The analysis shows that the positive descriptors (Table 6 - Column 3) are the results of two main processes, namely reflection and interaction. On the one hand, the students reflected on their learning context and indicated that they felt bored, uninformed, stressed, lonely and were afraid of losing face. On the other hand, the positive counterparts, such as be(com)ing involved with learning, experiencing peer and lecturer support, sharing experiences and feeling energetic, all rely on collaborative learning via the Facebook platform.
Two processes are at work within the context of metacognition. First, there is declarative knowledge that refers to the opportunities that students have to reflect on as learners and on their learning processes (Flavell 1979, Pintrich 2002, Tarricone 2011, Schraw 1998, Fourie 2016). In doing so students raised their own awareness as well as that of others regarding the process of learning a new language for healthcare purposes. The second process is interactive learning, which is how the process of learning a language manifests itself. From a metacognitive point this manifestation of learning is called procedural knowledge. Students were required to interact in order for any of the positive descriptors (e.g. such as having to do tasks that required feedback on each other's work and experiencing peer support via Facebook posts (see Appendix A for more examples). Procedural knowledge can only manifest itself during task performance (Schraw 1998, Veenman 2013) and it was therefore important for students to interact in order for their metacognition to develop.
The two processes (interaction and reflection) were the main processes that facilitated opportunities to gain experience in learning. Gaining experience is linked to gaining confidence (see 5.1.2) and both experience and confidence are important aspects in order to progress towards a new identity (Ashmore et al. 2004, Pratt et al. 2006, Roberts 2010, Norton 2011, Burford 2012).
5.1.2 Two features
The students also perceived the Facebook community as a safe place where they could learn by making mistakes (see Column 3 of Table 6) and in doing so they gained self-confidence (Bandura 1977). The students were therefore gaining work related confidence and work related experience, which are necessary for the process of identity development (Ashmore et al. 2004,
Pratt et al. 2006, Roberts 2010, Burford 2012).
5.2 The Antwerpen data
Based on the experience with the Stellenbosch students, the design of the programme for the Antwerpen students specifically aimed to support their metacognition and metacognitive growth in the course of learning a new language for medical purposes. The intention was to support the development of their identities. To this end, the tasks which students had to engage in, focused on both declarative knowledge (mainly through awareness raising and opportunities to reflect) and procedural knowledge (mainly through opportunities to enact metacognition through interaction). See Table 7 below for an overview of how the community of practice facilitated metacognition and supported the identity formation processes.

5.2.1 The two metacognitive processes
The focus of the Antwerpen research shifted from the experience of the individual towards the experience of members of a community of practice and the collected data accordingly centred on the Facebook posts (see 3.3). The reason behind this shift in focus is that the various and complex needs of the individual student can be better met through collaboration as a member of a community of practice (Fourie 2015). Research has shown that communities of practice dedicated to professional healthcare can help students with the development of their professional identities and responsibilities associated with their future careers in healthcare (Burgess & Nestell 2014:406). The community of practice gained a further purpose since metacognition can be shared to the advantage of all community members when they collaborate (Shea et al. 2014). Students collaborated with each other via the Facebook platform, following the incentives included in the tasks. They also collaborated beyond the incentives, for instance by using humour and by encouraging feedback from others.
The Stellenbosch data, alongside existing research, outlined that reflection is a necessary process within a communication training programme. Reflection is a significant aspect of declarative knowledge or metacognitive awareness and is usually triggered before, during or after a task when a student reflects about an aspect of learning (also see 6.1.1). Students were asked to reflect upon their learning experiences when answering pre- and post-course questionnaires, as well as during some of the Facebook tasks. In addition, all posts made by each student were visible to the whole group and in this way the Facebook platform supported the process of reflection as students could read what the others wrote. Existing literature has indicated that reflection is an important aspect of the identity formation process (Wilson et al. 2013). Accordingly, students in the Antwerpen group were encouraged to reflect amongst others on the following: on their own practice as medical professionals; on the comments of others regarding their specific medical practices; on the linguistic aspects of their own use of the target language as well as on the linguistic aspects in comments of others; on communicative functions in the target language; on being part of a community and also on making mistakes (See Table 7, Column 1).
The second process outlined by the Stellenbosch data is interaction, which is also the process through which procedural knowledge manifests in a language learning context (see 5.1.1). Within the context of the Facebook community students were given incentives that encouraged interaction. The incentives facilitated the use of grammatical structures and specific vocabulary, such as the grammatical structures needed to ask patients open and closed questions. Apart from the functional healthcare content, the communication on the Facebook platform also covered the more personal feelings and contexts of students' learning experiences and daily lives. For example, students conveyed feelings that indicated that criticism was meant to be supportive, thus not only reinforcing that the Facebook community was a safe space to make mistakes, but also a space that supported collaboration. Following incentives to do so, students also interacted with each other by introducing themselves in the target language and explained more about their personal and family lives, as well as other interests beyond healthcare. Some of them continued to refer to their family lives beyond the incentives - for instance how family schedules clashed with studies and work schedules and by including photographs of children in the other Facebook tasks. Other subjects of the nursing degree course were also discussed in the group. At times students also interacted in the common home language, mainly to joke or to deal with administrative issues. One student also spontaneously mentioned being dyslexic and how this condition influenced her writing. The Easter celebrations as well as a terrorist attack in Brussels took place during the five-week course and students referred to these cultural and socio-political events in a general, considerate manner. (See Table 7, Column 1).
Confirming the results from the Stellenbosch research, most of the Antwerpen nursing communication students also claimed in their pre-course reflections that interaction is the best way to learn a new language and in the post-course reflections that they valued the interactive nature of the course. Research indeed indicates that interaction is both the means and objective in second language learning (Wang 2004, Larsen-Freeman 2013). A second reason behind the importance of interaction is that the process of acquiring a new identity relies on interaction with others (Ashmore et al. 2004, Pratt et al. 2006, Roberts 2010, Norton 2011, Burford 2012).
The results indicated that these processes, namely interaction and reflection, though mentioned separately in this discussion, were often integrated during learning and task performance. For instance, the results from the data indicated that, as the tasks encouraged students to respond in the second language to typical scenarios in a healthcare context, they interacted and engaged using medical terminology and practised using specific linguistic structures such as sentence structure (giving instructions, asking questions). In doing so, students also became aware that being polite requires different communicative strategies, as politeness indicators did not translate directly from the home language to the target language and culture. They were also asked to give critical feedback on the content of peer posts and accordingly, they also had to interact and reflect on the comments others made on their nursing communication strategies. This stimulated reflection on their own use of language.
5.2.2 The three features
As with the Stellenbosch study, the results of the Antwerpen study indicated that two features were necessary for the students to progress towards a new identity, i.e. to gain experience and to gain confidence. By engaging with peers and the lecturer in performing tasks, students were interacting and gaining experience in communicating in the second language within a nursing context, as well as on a personal level. Positive feelings, such as feeling safe enough to (allow yourself to) make mistakes, contributed to gaining confidence. As shown before with the Stellenbosch data (see 5.1.2), there is also a reciprocal relationship between confidence and positive learning experiences (Bandura 1977, 2012). However, based on the results of the Antwerpen data as well as on the existing literature (Ashmore et al. 2004, Pratt et al. 2006, Roberts 2010, Burford 2012), a third feature was added, namely to validate identities. This is based on the fact that the community of practice also provided a platform where students could claim various group identities in one space, for example being a professional nurse, being a student, being a parent, being a partner, being a horse rider or being a politically conscious citizen of a particular country (see Table 7). These various identity claims were directly or indirectly carried out through the online interaction with others (Ashmore et al. 2004, Pratt et al. 2006, Roberts 2010, Burford 2012). When viewing the posts of others, students had the opportunity to become aware of others' identities that are different from or overlapping with their own group identities. Within the Facebook group students could also reflect on how language communicates a specific culture or identity. By acknowledging different identities next to each other, the students took part in a dynamic process to validate their evolving identities in the second language.
As with the two processes (reflection and interaction) there is also an interrelated and reciprocal relationship between the three features (gaining confidence, gaining experience and validating identities). Apart from confidence and positive learning experience that are reciprocal (Bandura 1977, 2012), the process of validating a new identity also relies on gaining experience in communication and interaction with others (Ashmore et al. 2004, Pratt et al. 2006, Roberts 2010, Norton 2011, Burford 2012).
6. Conclusion
The purpose of this study was to provide an overview or framework (see Table 7) of how an online community of practice within a second language communication training course for healthcare (pre-)professionals can serve as an environment to support on-going identity formation processes. Based on the metacognitive awareness that the Stellenbosch first year medical students demonstrated, a set of tasks and incentives were developed and integrated into a communication training course for the Antwerpen nurses to stimulate not only metacognitive awareness and reflection (declarative knowledge), but also the manifestation of metacognition (procedural knowledge). Metacognition manifests itself during task performance (Schraw 1989) which, in the context of this communication training environment means that metacognition manifests during the process of interaction. Therefore, students not only had the opportunity to reflect and raise their own metacognitive awareness (declarative knowledge) but they also had the opportunity to implement their own metacognition (procedural knowledge). In return these dynamic processes can facilitate a gain in experience and a gain in confidence, as well as opportunities to validate evolving identities, which was facilitated by the social and transparent online community. Existing research has shown that these features, namely to gain experience, to gain confidence and to validate identities, are all significant aspects in the dynamic process of a developing identity (Bandura 1986, Bandura 1990, Ashmore et al. 2004, Pratt et al. 2006, Burford 2012).
The framework in Table 7 is therefore showing how communication training can be combined with identity formation processes, as language and identity are interrelated. In a world where healthcare professionals are increasingly travelling across (linguistic) borders, the identities of these professionals are challenged, because they have to perform their professions in multilingual contexts. In this regard this research study attempted to contribute to the well-being of the healthcare professional and ultimately to the well-being of the patient.
References
Ashmore, R.D., K. Deaux and T. McLaughlin-Volpe. 2004. Framework for collective identity: Articulation and multidimensionality. Psychology Bulletin, 130: 80-114. https://doi.org/10.1037/0033-2909.130.L80 [ Links ]
Bandura, A. 1977. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84: 191-215. https://doi.org/10.1037/0033-295x.84.2.191 [ Links ]
Bandura, A. 2012. Functional properties of perceived self-efficacy revisited. Journal of Management, 38(1): 9-44. [ Links ]
Burford, B. 2012. Group processes in medical education: Learning from social identity theory. Medical Education, 46: 143-152. https://doi.org/10.1111/j.1365-2923.2011.04099.x [ Links ]
Burgess, A. and D. Nestel. 2014. Facilitating the development of professional identity through peer assisted learning in medical education. Advances in Medical Education and Practice, 5: 403-406. https://doi.org/10.2147/amep.s72653 [ Links ]
Charmaz, K. 2014. Constructing grounded theory. London: Sage Publications. [ Links ]
Coetzee-Van Rooy, S. 2006. Integrativeness: Untenable for world Englishes learners? World Englishes, 25(3/4): 437-450. https://doi.org/10.1111/j.1467-971x.2006.00479.x [ Links ]
Dörnyei, Z. 2007: Research methods in applied linguistics: Quantitative, qualitative and mixed methodologies. Oxford: Oxford University Press. [ Links ]
Druckman, D. and R.A. Bjork (eds.). 1994. Learning, remembering, believing: Enhancing human performance. Washington: National Academy Press. [ Links ]
Flavell, J.H. 1979. Metacognition and cognitive monitoring: A new area of cognitive-developmental inquiry. American Psychologist, 34(10): 906-911. https://doi.org/10.1037/0003-066x.34.10.906 [ Links ]
Fourie, C. 2015. Lowering the threshold for online learning with Facebook: A South African pilot study. Dutch Journal of Applied Linguistics, 4(2): 154-173. https://doi.org/10.1075/dujal.4.2.02fou [ Links ]
Gasiorek, J. and K. van de Poel. 2012. Divergent perspectives on language-discordant mobile medical professionals' communication with colleagues: An exploratory study. Journal of Applied Communication Research, 40(8): 368-383. https://doi.org/10.1080/00909882.2012.712708 [ Links ]
Goldie, J. 2012. The formation of professional identity in medical students: Considerations for educators. Medical Teacher, 34: e641-e648. https://doi.org/10.3109/0142159x.2012.687476 [ Links ]
Gollin-Kies, S., Hall, D.R. and Moore, S.H. 2015. Language for Specific Purposes. Basingstoke: Palgrave Macmillan. [ Links ]
Joseph, J. 2004. Language and Identity. Basingstoke: Palgrave Macmillan. [ Links ]
Larsen-Freeman, D. 2013. Complexity theory: A new way to think. RBLA, 13(2): 369-373. [ Links ]
Leibowitz, B., H. Adendorff, S. Daniels, A. Loots, S. Nakasa, N. Ngxabazi, A. van der Merwe and I. van Deventer. 2005. The relationship between identity, language and teaching and learning in higher education in South Africa. Per Linguam, 21(2): 23-37. https://doi.org/10.5785/21-2-74 [ Links ]
Mavor, K.I., K.G. McNeill, K. Anderson, A. Kerr, E. O'Reilly and M.J. Platow. 2014. Beyond prevalence to process: the role of self and identity in medical student well-being. Medical Education, 48: 351-360. https://doi.org/10.1111/medu.12375 [ Links ]
Morgan, D.L. 2008. Emergent design. In L.M. Given (ed.) The SAGE Encyclopedia of Qualitative Research Methods. London: SAGE Publications. pp. 245-248. [ Links ]
Monrouxe, L. 2009. Identity, identification and medical education: Why should we care? Medical Education, 44(1): 4-49. https://doi.org/10.1111/j.1365-2923.2009.03440.x [ Links ]
Norton, B. 2011. Identity. In J. Simpson (ed.) The Routledge Handbook of Applied Linguistics. London: Routledge. pp. 318-330. [ Links ]
Pike, G.R., G.D. Kuh, and A.C. McCormick. 2010. An investigation of the contingent relationships between learning community participation and student engagement. Research in Higher Education, 52: 300-322. https://doi.org/10.1007/s11162-010-9192-1 [ Links ]
Pintrich, P.R. 2002. The role of metacognitive knowledge in learning, teaching and assessing. Theory into Practice, 41(4): 219-225. https://doi.org/10.1207/s15430421tip4104 3 [ Links ]
Pratt, M.G., K.W. Rockmann and J.B. Kaufmann. 2006. Constructing professional identity: The role of work and identity learning cycles in the customization of identity among medical residents. Academy of Management Journal, 49(2): 235-262. https://doi.org/10.5465/amj.2006.20786060 [ Links ]
Preece, S. 2016. Introduction: Language and identity in applied linguistics. In S. Preece (ed.) The Routledge Handbook of Language and Identity. London: Routledge. pp. 1-16. https://doi.org/10.4324/9781315669816 [ Links ]
Rahimian, M. 2015. Identity issues among post-secondary students in an English speaking country. Procedia - Social and Behavioural Sciences, 174: 305-312. https://doi.org/10.1016/j.sbspro.2015.01.663 [ Links ]
Roberts, C. 2010. Language socialization in the workplace. Annual Review of Applied Linguistics, 30(1): 211-227. https://doi.org/10.1017/s0267190510000127 [ Links ]
Schraw, G. 1998. Promoting general metacognitive awareness. Instructional Science, 26: 113-125. [ Links ]
Shea, N., A. Boldt, D. Bang, N. Yeung, C. Heyes and C.D. Frith. 2014. Supra-personal cognitive control and metacognition. Trends in Cognitive Sciences, 18(4): 186-193. https://doi.org/10.1016/j.tics.2014.01.006 [ Links ]
Skjeggestad, E., J. Gerwing and P. Gulbransen. 2017. Language barriers and professional identity: A qualitative interview study of newly employed international medical doctors and Norwegian colleagues. Patient Education and Counselling, 100(8): 1466-1472. https://doi.org/10.1016/j.pec.2017.03.007 [ Links ]
Tarricone, P. 2011. The Taxonomy of Metacognition. Hove: Psychology Press. [ Links ]
Van de Poel, K. 2016. Effective medical professionals: translating foreign language needs in online intercultural communication training. In EDULEARN 16 Proceedings. Barcelona: IATED. pp. 672-681. https://doi.org/10.21125/edulearn.2016.1131 [ Links ]
Van de Poel, K. and C. Fourie. 2013. A critical approach to the development of blended medical communication training materials. Stellenbosch Papers in Linguistics Plus, 42: 1 -19. https://doi.org/10.5842/42-0-149 [ Links ]
Van de Poel, K. and C. Fourie. 2016. Guidelines to foster metacognitive skills in online professional communication training. In EDULEARN 16 Proceedings. Barcelona: IATED. pp. 522-531. https://doi.org/10.21125/edulearn.2016.1100 [ Links ]
Van de Poel, K. and T. van Dyk. 2015. Discipline-specific academic literacy and academic integration. In R. Wilkinson and M.L. Walsh (eds.) Integrating Content and Language in Higher Education: From Theory to Practice. The 2013 ICLHE Conference. Frankfurt: Lang. pp. 161-180. https://doi.org/10.3726/978-3-653-05109-4/21 [ Links ]
Veenman, M.V.J. 2013. Assessing metacognitive skills in computerized learning environments. In R. Azevedo and V. Aleven (eds.) International Handbook of Metacognition and Learning Technologies. Springer: London. pp. 157-168. https://doi.org/10.1007/978-1-4419-5546-3 11 [ Links ]
Veenman, M.V.J. and M.A. Spaans. 2005. Relation between intellectual and metacognitive shills: Age and task differences. Learning and Individual Differences, 15: 159 -176. https://doi.org/10.1016/j.lindif.2004.12.001 [ Links ]
Wang, Y. 2004. Distance language learning: Interactivity and fourth generation internet-based video conferencing. CALICO Journal, 21(2): 373-395. https://doi.org/10.1558/cj.v21i2.373-395 [ Links ]
Wenger, E. 1998. Communities of practice: Learning, meaning and identity. New York: Cambridge University Press. [ Links ]
Wenger, E., R. McDermont and W.M. Snyder. 2002. Cultivating communities of practice. Boston: Harvard Business School Press. [ Links ]
Wilson, I., L. Cowin, M. Johnson and H. Young. 2013. Professional identity in medical students: Pedagogical challenges to medical education. Teaching and Learning in Medicine 25(4): 369-373. https://doi.org/10.1080/10401334.2013.827968 [ Links ]
Ushioda, E. and Z. Dörnyei. 2009. Motivation, language Identities and the L2 self: A theoretical overview. In Z. Dörnyei and E. Ushioda (eds.) Motivation, Language Identities and the L2 Self. Bristol: Multilingual Matters. pp. 1-8. https://doi.org/10.21832/9781847691293-002 [ Links ]
Tables A, B and C below exemplify how the raw data from the Stellenbosch medical corpus developed from first, second and finally to third level coding. For the sake of clarity, three examples given in different focus group discussions were selected and presented here.
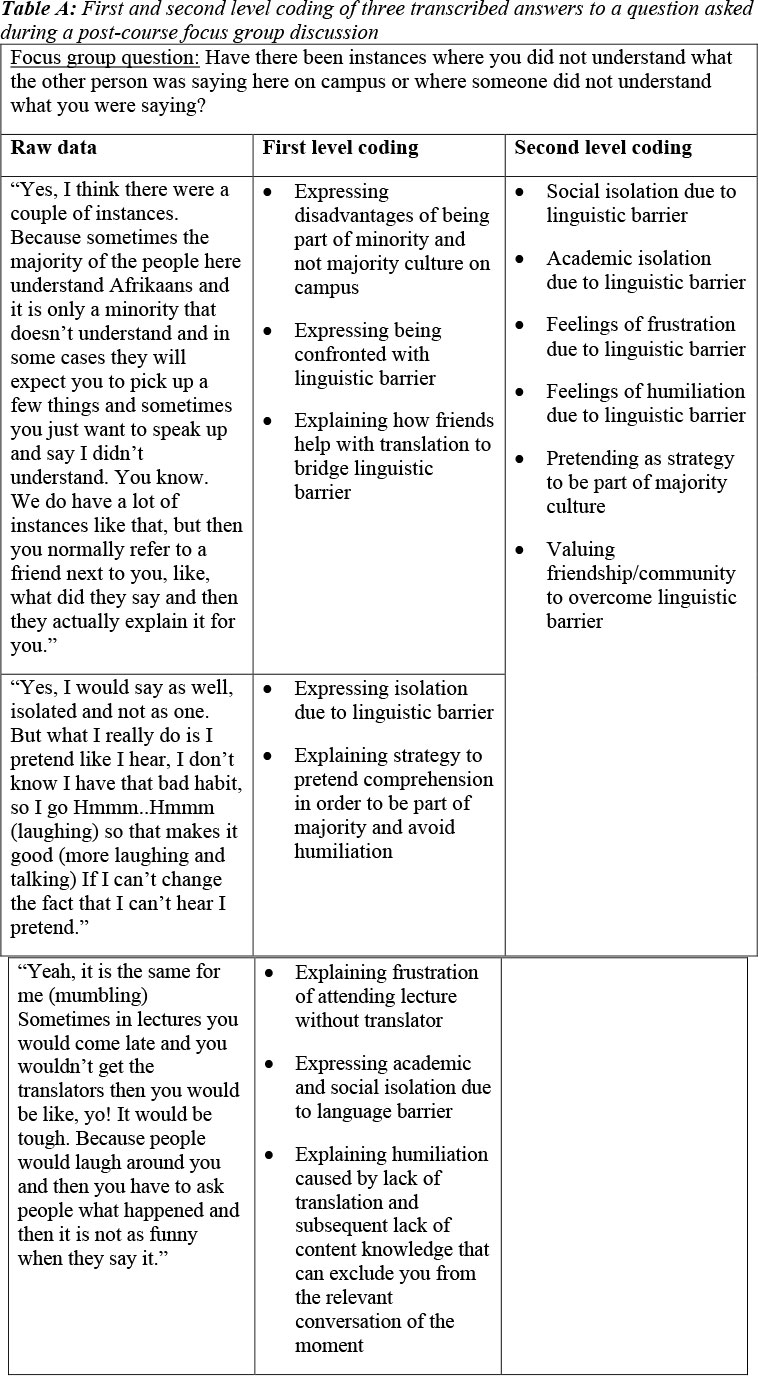
The analysis outlined in Table A shows that students are expressing the challenges they are experiencing, such as linguistic and cultural barriers, as well as the impact of these two factors on academic acculturation. They are also suggesting positive alternatives.
Table B demonstrates how a question from the post-course questionnaire has been analysed and coded:

Table C below demonstrates how the results shown in Tables A and B have been conceptualised to indicate how students managed positive changes in spite of a challenging context so that they could progress towards a positive sense of self as first-year medical students. The concepts used have here been evaluated in line with existing research with a focus on the process of developing a new identity as medical pre-professionals. See 5.1 Discussion and Table 6 for a detailed consideration and final table with coded results.



{kind=link}