










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkScientia Militaria: South African Journal of Military Studies
versão On-line ISSN 2224-0020
versão impressa ISSN 1022-8136
SM vol.50 no.3 Cape Town 2022
http://dx.doi.org/10.5787/50-3-1379
ARTICLES
A positive psychology perspective on pre-deployment fitness-for-duty evaluations for external deployments: A proposition for the South African National Defence Force
PietBester188
Stellenbosch University
ABSTRACT
The aim of this article is to introduce the reader to a psychological well-being orientation for soldiers in pre-deployment fitness-for-duty evaluations by screening for psychological risk rather than pathology. This aim is reached firstly, by discussing the existing process of pre-deployment fitness-for-duty evaluations, then conceptualising the assessment for psychological risk rather than psychopathology only, followed by linking pre-deployment assessment of fitness-for-duty evaluations to the positive psychology paradigm and proposing an integrative military model for soldiers' psychological well-being in the external deployment context. The discussion is concluded by recommendations for military decision-makers to consider this approach of psychological risk assessment as a feasible process.
Introduction
As a member state of the United Nations (UN), the African Union (AU) and the Southern African Development Community (SADC), South Africa is in the vanguard of bringing about lasting peace and stability on the continent.189 In recent years, the South African National Defence Force (SANDF) has participated in peace-support operations in various African states, such as Burundi, Sudan and the Democratic Republic of the Congo, and is currently involved in a counterterrorism operation in neighbouring Mozambique.190 The SANDF has been involved in 14 peace missions between 1999 and 2019,191 and averaged at one stage 2 300 soldiers at any given time.192 Consequently, South African (SA) soldiers deploy in the African battlespace (ABS), which can be described as an environment where soldiers are increasingly placed in asymmetric situations against opponents who are not easily identifiable and who are probably better armed and equipped, with better access to communications and technology than the SANDF.193 Various authors have reported on the changed nature of the ABS, and have confirmed the complexity and challenges resulting from these changes.194
These are complex situations, and Gouws195 emphasises that the complexities of military operations domestically and abroad require soldiers who are more resilient than ordinary citizens. Moreover, soldiers are very likely to be exposed to psychological trauma that may inflict adverse neuropsychological effects.196 The individual's ability to recover from such trauma depends on his or her previous history, his or her physiological status, and the social distress encountered.197 Furthermore, the demands of the SANDF to deploy into peacekeeping and operations other than war scenarios to satisfy UN and SADC needs on the African continent lead to an increased operational tempo for soldiers. There is thus a considerable likelihood of exposure to trauma as well as prolonged deployment periods away from home that may exceed the typical SANDF deployment duration of twelve months for peace support operations.
For these reasons, the UN has also indicated that deploying soldiers should undergo adequate medical, dental and/or psychological screening prior to deployment, implying that they should have "no psychopathology".198 It is therefore understandable that the SA cabinet decided in 1998 that SANDF soldiers should undergo health assessments that include the psychological state of soldiers199 once every two years to ensure that they are combat-ready. This decision compelled the Military Health Services (Directorate Psychology) of the SANDF to conduct mental health screening of soldiers prior to deployment.
After an initial review of the literature on psychological fitness for military operations, the SANDF Director Psychology decided to screen soldiers for general psychopathology in the pre-deployment phase.200 This is consistent with international trends to screen for pathology.201 In the absence of an SA instrument or tool for assessing pathology, the Millon Clinical Multiaxial Inventory-III was used initially. However, because of high cost and low scale reliabilities when applied to an SA population, the instrument was rejected. A decision was made to 'screen out', which implied the identification of mental health issues that could adversely affect performance as opposed to 'screening in' when candidates who meet specific criteria are sought.202 In the SA military health context, this screening process involved the so-called 'three Ds', namely disease, disorder and disability.203 Against this background, the Military Psychological Institute (MPI) embarked on a process of developing a psychopathology-based clinical measuring instrument suitable for screening a supposedly 'normal population' or 'non-psychiatric population' whose members may be highly functional in the workplace, with no known diagnosed psychological disorders.204This was further complicated by the understanding that the absence of psychopathology does not imply the presence of mental health and vice versa.205
These dynamics highlight the limitations of a restrictive medicalised framework that would tend to screen for pathology only. Utilising a purely medical model in the study of human experiences may lead one to neglect other psychological risk factors that may have a negative effect on psychological well-being (PWB) that can be identified and addressed by interventions other than psychotherapy. After all, it needs to be acknowledged that there are conditions other than medical disorders that will make a person a psychological risk for deployment. Furthermore, useful insights may be gained from employing other psychological frameworks, such as positive psychology (broadly, the study of the conditions and processes that contribute to the optimal functioning of people, groups and organisations).
Consequently, the author provides background to the current screening process, which places strong focus on screening for psychopathology. This article will compare psychopathology with psychological risk, introduce a positive psychology perspective, and propose an integrative military model for soldiers' well-being in the external deployment context as a basis for a future process of screening for deployment. This discussion will be concluded with recommendations for decision-makers in the SANDF.
The current screening process
The screening process currently employed in the SANDF is referred to as the Concurrent Health Assessment (CHA)206, whereas the broader military psychology literature refers to it as "military-fitness-for duty-evaluations".207 References to the CHA are closely linked to fitness-for-duty evaluations. The aim of these evaluations is to select those soldiers whose fitness for military duty would be sustained when operationally active, even in some extreme situations. From the perspective of military psychology, this means that soldiers can perform their operational and related duties safely and effectively, whilst maintaining a stable state of mental health state. Owing to the comprehensive nature of the process followed during the CHA, it is even possible for a soldier to be classified medically without evaluation by a so-called 'medical' or 'health board'.208 Moreover, it is important to note that the CHA process does not include post-deployment assessments, forensic assessments, security vetting assessments or medical evaluation boards. As stated above, the focus of the CHA is routine assessments209 to determine operational deployability. It is also worth noting that the SANDF prefers that, for a specific mission area, the fighting elements are deployed as an entire unit or entity, whereas the support elements are often compiled from various, often unrelated, units.
The current process requires psychological and social work assessment of the soldier preferably one week before medical assessments are due to begin, although this is not always possible in practice. Subsequent medical and dental assessments involve a pre-medical examination to obtain clinical data, other medical assessments, drawing blood to identify traces of substance abuse and HIV/Aids infection, HIV/AIDS pre-test counselling, as well as an oral health assessment by a dentist. These procedures also include the immunisation of the soldier or confirmation that immunisations are up to date and will remain up to date for the duration of the anticipated deployment period.
During the psychological assessment, soldiers complete the Psychological Risk Inventory (PRI).210 This instrument was developed by the MPI as a screening tool to assist clinical psychologists in assessing the mental health status of SANDF members when large groups of people are to be evaluated within a short period. Since conducting clinical interviews on an individual basis is extremely time-consuming and labour-intensive, the inventory serves as a cost-effective tool to identify risk factors. It is important to note that the PRI is not a diagnostic tool, but a self-report measure that attempts to identify behavioural patterns that differ significantly from a so-called normal SANDF population. When at-risk behavioural patterns are identified, findings are probed and verified by means of a clinical interview. The instrument can be administered by counselling or industrial psychologists but the clinical interview can only be done by a clinical psychologist.
According to the MPI, the PRI measures a number of primary, secondary and latent scales to assess the overall risk behaviour of soldiers in a normal population.211 The primary scales of the PRI measure whether the respondents (the soldiers in this instance) are under stress; whether they are suffering as a consequence of past trauma; and whether they display aggression (by responding in the affirmative to questions with an aggressive and/or impulsive content, for example, being irritated by others). The secondary scales refer to the measurement of withdrawal, which represents a mixture of withdrawal, anxiety and depression indicators; mood, implying behavioural indicators associated with negative mood states; dissociative traits indicative of absent-mindedness, possible depression and inability to cope with day-to-day stressors; and destructive behaviour, which is a composite scale with diverse indicators of an ineffective coping strategy. Lastly, the latent scales measure mild anxiety, indicative of constant worry and feelings of being down-hearted and/or irritated for no reason; low ego integrity, indicative of a person's ego being under pressure based on vague and non-specific complaints; and lastly, general negative behaviour. The latter is not a scale on its own, but contains items that might provide valuable information that the psychologist could use if the respondent is identified for an interview.
In addition to these scales, the questionnaire includes a risk indicator consisting of a combination of all the items related to the primary, secondary and latent scales, but excluding items relating to moderating indices. There is also a coping indicator, which serves as a moderating value that allows the psychologist to make an informed decision on the state of the respondent's coping mechanisms in relation to the risk factors reported in the test. It is worthy to note that, although the developers of the PRI did not approach the development of the inventory purposefully from a positive psychology framework per se, the words 'coping indicator' are a positive psychology concept as it focuses on the positive rather than the negative as it refers to the ability to deal with a challenge.
Those with identified risk factors are then interviewed by a psychologist, and a determination is made with respect to their health status in relation to deployability. Based on a statistical formula, about 23% of those assessed will be identified for a clinical interview.212 The psychologist then makes a decision with respect to the mental health status of the individual in relation to external operational deployability according to a colour code assigned to each individual.213 These codes are green, yellow and red and indicate the soldier's external deployability.
A green operational status indicates no restrictions on the utilisation of the individual based on the confirmed medical (health) category. Yellow status implies a temporary restriction on deployment. In this case, an intervention may enable the status to be changed to green when conditions change as a result of the intervention. For example, an obese person who is assessed as yellow status goes on a diet, loses weight and is then determined to be within the norms set by the SANDF. When a soldier has a permanent inability (irreversible condition) to deploy operationally externally, as in the case of kidney failure, red status will be attributed to him or her. During internal deployments, decisions will be based on a case-by-case assessment in relation to the nature of deployment, occupational class and the individual health profile of the soldier.
Essentially, the colour-coded system reflects a representation of the soldier's health status and is used to initiate follow-up visits to a healthcare practitioner (HCP) or interventions in respect of further treatment. As suggested above, this colour coding is done not only holistically, but also per discipline or component of the process. A person may be 'green' in terms of his or her physical health, but may be 'yellow' because of a mental health-related issue, which then will holistically make such person unsuitable for deployment, and an intervention will be required to change the person's status (colour code). All disciplines involved, such as psychology, social work, medicine and oral health, capture the interpreted results electronically and these are imported back on the Health Informatics System (HIS) of the South African Military Health Service (SAMHS) where they are accessible for a final decision to be made on a member's suitability for deployment.
Consequently, on completion of the whole process, a so-called 'confirming healthcare practitioner' (CHCP) evaluates all available information (inputs from all the disciplines involved) and determines the health status of the member. This HCP may require that additional medical information be obtained if an informed decision is not possible. Furthermore, all the information is captured on the HIS for future reference and statutory record-keeping requirements. Discipline-specific information is only available to practitioners of the discipline registered on the system and to the CHCP. For the sake of patient confidentiality, patient information is not accessible across different disciplines.214
The author's criticism against the existing screening process is that its strong reliance on the medical model leads little room for the consideration of other collateral information potentially relevant to an individual's deployability, for example, what is manifested in a person's behaviour on a day-to-day basis. Furthermore, the process is based on a self-report measure where the respondents report directly on their behaviours, beliefs, attitudes or intentions. As a result, the respondents may provide socially desirable answers, especially if they want to deploy. Although one may argue that it can be countered by response analysis through so-called 'lie scales' or 'social desirability scales', it would add up to those individuals 'red flagged' for a follow-up interview, making it time-consuming and hence burdensome. Consequently, another approach from a positive psychology perspective is suggested where the self-report data are not used alone.215 However, before conceptualising the alternative approach, it is important to contrast the concepts of psychopathology vs psychological risk.
Psychopathology versus psychological risk
Psychopathology resides within the field of clinical psychology, and refers to the study of the symptoms and causes of mental distress and various treatments for behavioural and mental disorders.216 In turn, a mental disorder can be described as a behavioural or psychological syndrome or pattern that occurs within an individual, which reflects an underlying psychobiological dysfunction, and which is associated with clinically significant distress or impairment in one or more important areas of functioning.217Pre-deployment screening with a primary focus on psychopathology may lead to the medicalisation of normal behaviour,218 and offers a restricted view of an individual's risk potential.
From a 'fitness-for-duty' perspective, an alternative approach focusing on the concept of 'psychological risk' seems attractive, as it relates better to a mental health model than to a medical or disease model. In this regard, a person who poses a potential risk from a psychological perspective may not necessarily be ill from a mental health perspective or meet the diagnostic criteria for a mental disorder. Yet, an overview of the psychology and risk-related literature yielded limited coverage of the concept of psychological risk as it might be applicable to military deployments. Nevertheless, useful insights regarding psychological risk could be gained from the fields of occupational health and safety, national security, criminology as well as literature on stress and coping.
From the perspective of occupational health and safety, psychological risk is seen as emanating from the work environment, namely poor work design or poor social context of the work, leading to physical and social outcomes, such as work-related stress, burnout or depression.219 Born and Van der Flier220 highlighted individual differences in their investigation of organisational risk and observed that there are relevant aspects related to individual differences, for instance coping styles (how people cope with the events they encounter).
From a national security perspective, Wiese221 refers to the concept of 'security risk', which suggests that, because of a person's personality traits, needs, behaviour, ideological persuasion or extreme sensitivity in terms of past deeds, he or she might be persuaded by whatever means to cooperate with an unauthorised individual or organisation to divulge secrets of his or her employer, or on his or her own accord would divulge secrets to an unauthorised individual or organisation. Based on the work of Wiese, the author of this article, who also does consulting work related to compiling a risk profile of existing or prospective employees, conceptualised the 'risk profile' of an individual as the outcome of a process to determine whether such individual poses a risk to his or her employer or prospective employer. This is based on an analysis of the personality traits, lifestyle, needs, behaviour, value system or sensitivity in terms of past deeds and whether he or she can be persuaded by whatever means to cooperate with an unauthorised individual or organisation to cause intentional or unintentional damage to his or her company or any of the clients of such company.222 This definition can be viewed as that of 'employment risk'.
McSherry223 discusses psychological risk from a mental health perspective in a criminology setting and states that it is about identifying the risk of dispositions that might lead to reoffending or to harming others. Reference is made to a combination of both a clinical (qualitatively determined risk by an expert, based on consideration of all evidence) and actuarial approach (quantitatively calculated risk factor, based on weighted variables) to decision-making in terms of psychological risk, and a number of predictor variables have been identified from the literature. These variables are:
• past violence (relying on the history of past behaviour);
• pre-existing vulnerabilities, such as early signs of antisocial traits, difficulties in peer relationships and hostility towards authority figures;
• social and interpersonal factors;
• mental illness;
• substance abuse, especially when it co-exists with mental illness;
• state of mind;
• situational triggers, such as loss, demands, expectations, confrontations, ready availability of weapons, and physical illness; and
• personality constructs.
One can also see the relationship between these pre-existing vulnerabilities and the content of the PRI scales discussed above. Moreover, in an effort to deal with a normal population, the MPI states that psychological risk "refers to the behavioural indicators of [an] ineffective coping mechanism to deal with the psychological demands of everyday life".224 The notion is that, if a person does not demonstrate the necessary coping strategies, the likelihood of the development and progression of a mental health disorder is increased if the problem is not identified and treated timeously. Taylor's description of coping strategies, as cited by the MPI, refers to the specific efforts, both behavioural and psychological, that people employ to master, tolerate, reduce, or minimise stressful events.225 These coping styles may include active, passive or avoidance coping techniques.226 There are a number of generalised and specific resources that could assist an individual when attempting to cope with various stressors.227 These include self-respect, cultural values, tradition, intelligence, view of the world and healthy behaviour. According to Antonovsky,228 these resources can be classified into eight groups, namely physical, biochemical, material, cognitive, emotional, estimation and views, interpersonal relational, as well as macrosocial and cultural. Naturally, as these resources come under threat in acute and/or prolonged stressful situations, psychological risk increases.
In the military context, the stress caused by stressful events is defined as "a non-specific number of reactions and responses of the body (mental, emotional and/or physiological) causing bodily or mental tension, strain or pressure following any demand made upon it, and designed for self-preservation".229 Stress can be either good (referred to as eustress) or bad (referred to as distress) and can be caused by internal or external forces.230
When analysing the aforementioned perspectives on psychological risk, a number of broad themes come to the fore, namely context (social, work, personal), predictive variables, coping, and outcomes. Considering these themes, and for the purpose of this discussion, psychological risk can be defined as:
[T[he sum total of the outcomes emanating from an individual's ability or inability to cope with contextual encounters as determined by predictive variables affecting that specific individual.
The context refers to, but is not limited to, the social, work and personal environments of the soldier, while the predictive variables include, but are not limited to, such individual's past behaviour, pre-existing vulnerabilities, possible history of mental illness, social and interpersonal factors, substance abuse, situational triggers, and certain personality constructs. Should a soldier deploy to a mission area in, for example Sudan, the context would be the foreign country, Sudan, with all its characteristics, such as climate, culture, population and social system, the soldier's personal circumstances at home, and his or her experience of working as a soldier as part of a team interacting with the social system in Sudan. Furthermore, within this context, coping includes both unhealthy coping behaviours, such as over- or undereating, smoking, drinking and healthy coping behaviours, such as exercising.
With a rich understanding of psychological risk and knowing that it is directly related to the outcomes of an individual's ability to cope, one may ask what the consequences or outcomes of psychological risks are, especially those that lead to unsuccessful deployment, which is in itself a negative outcome or consequence. In essence, when a soldier becomes a challenge for his or her commanders during deployment, for example, by being charged through the legal system and/or by having to be repatriated prematurely because of health or behaviour-related issues, the deployment is viewed as unsuccessful. From the above, one could infer that there are numerous psychological risk factors that are likely to contribute to unsuccessful deployment by an individual or which could at least increase the risk of having an unsuccessful deployment if the person cannot cope with such deployment. Such unsuccessful outcomes may stem from psychopathology, such as suboptimal intelligence, anxiety disorders, and adjustment disorders (i.e. a lack of adaptability), as well as related factors, such as a lack of motivation, a history of ineffectiveness, difficulties with interpersonal relationships, and failure to seek mental health assistance when needed. In view of the theory of behavioural consistency231 -which posits that past behaviour is the best predictor of future behaviour - factors related to inappropriate conduct but not necessarily associated with psychopathology could be considered as key elements of psychological risk., Such factors could include criminal behaviour, financial difficulties (which might cause stress for the individual or which might be an indicator of uncontrolled or impulsive behaviour), incidents involving substance abuse, poor performance, and even incompatibility with the military culture.
Negative outcomes therefore might not stem from psychopathology only, because psychological risk also includes other dysfunctional behaviours that cannot be diagnosed as psychopathology. Some of the typical dysfunctional work behaviours are absenteeism, substance abuse, presenteeism (functionally absent although physically at work), theft, bullying and sexual harassment.232 Unmanaged psychological risks may also lead to an inability to manage the demands of the job,233 the development of mental health problems (psychopathology), increased safety-related incidents, such as psychological and sexual harassment and third-party violence.234
Within the context of military deployment, uncontrolled individual behaviour might lead to an international incident and ultimately diplomatic embarrassment during, for example, a peace-support operation. It could also have a negative influence on unit cohesion that restricts the ability of a military force to function optimally. From a private business perspective, one could say that the outcome would be overall poor business performance; in the military it would most probably denote a failed mission.
Based on the preceding discussion one could postulate how the changed ABS may place new demands on SA soldiers. In support, Rothmann et al.235 emphasise that work has an influence on the well-being of employees and that, depending on the unique resources and demands in a specific work context, the determinants of well-being may differ in various working environments. Moreover, every occupation has its own specific risk factors regarding well-being, and the military is one of those places where the risks are higher and more than in other occupations such as, for example, a teacher. This suggests that deployment is emotionally demanding and that emotional coping is required. Content, resilient and coping soldiers are likely to function optimally.
From the above, it is clear that, while a psychological risk-based approach provides a more informed view than a psychopathology-based approach, it is still restrictive in that it focuses essentially on maladaptation in its many varied forms. It is therefore necessary to focus on and include other risk factors in the psychopathology-free majority of the population of soldiers and to assist them to live and work increasingly purposefully, become increasingly productive, and develop a sense of positive engagement and meaning during deployments specifically and in life in general. The next section will therefore provide additional insight into the positive psychology approach.
A positive psychology approach
From the discussion above, it was evident that it may be beneficial to consider elements of a positive psychology framework in the pre-deployment screening process. Various authors236 present a variety of definitions of positive psychology. After analysing some of these definitions, it is worthy to make the following observation on positive psychology: positive psychology is the application of psychological principles to real-life issues by attempting to understand the causes and consequences of optimal human functioning to help one manage and succeed in the workplace. Positive psychology is furthermore about delivering better and more compassionate health care to employees, and providing effective and engaging education in ways that optimise achievement (psychological well-being and the development of community). In essence, positive psychology is about optimal human functioning.
Archana, Ahuja and Kumar emphasise the importance of positive traits that cover character strengths and virtues, which when in combination above a certain threshold will make the person a 'good character'.237 Furthermore, within a military context, Mathews238describes positive psychology as a paradigm that provides a systematic conceptual basis and groundwork for an empirical assessment of the role of character strengths in adaptation and performance. Positive psychology is thus about efficacious adaptation and excellence in all domains of life, and therefore it has utility within the domain of military psychology where military commanders would like to command high-performing soldiers. It is, for example, for this reason that Milnic239 investigated the application of the salutogenic paradigm,2 which also falls within the field of positive psychology and which focuses on health and well-being in the field of military psychology. Others, such as Bartone, also studied hardiness, another construct related to positive psychology and which refers to a collection of personality characteristics that functions as a flexible resource during encounters with demanding life events.240
Positive psychology is not meant to replace traditional methods and models employed by military psychologists; it rather entails adding concepts and methods to the military psychologist's toolbox.241 The functionality of positive psychology in the military is further supported by Matthews242 who argues that the military is a perfect 'home' for positive psychology, as the military comprise relatively young, healthy and pathology-free individuals. In a positive psychology framework, one would consequently focus on those factors that improve and strengthen the mental health of SANDF soldiers.
In the same vein and in support of Kasser,243 the study on which this article is based, reasoned that rather than assuming that a good life is defined by the absence of psychopathology, many of the leaders in positive psychology have argued that PWB is a construct embedded in positive psychology, which should be studied in its own right.244 Positive psychology is about having a proactive stance towards achieving optimal emotional, physical and mental well-being through self-acceptance, personal growth (for example changing your mindset and become more positive), having a purpose in life, mastering the environment, autonomy, and having positive relationships with others.245Various authors246 argue that positive psychology as a discipline focuses on strengths rather than weaknesses. Furthermore, PWB has been identified as a predictor of risk behaviour247 that is closely linked to an individual's job security and career behaviour. When an individual experiences job security248 he or she is less likely to experience anxiety and stress, which will make such person more likely to control and deal with challenging situations through his or her coping mechanisms. Ruini249 observes that PWB plays a buffering role in coping with stress and a protective role in mental health. It would thus be safe to postulate that 'good' PWB will lessen psychological risk in a soldier, as conceptualised above.
From what has been stated elsewhere, one can deduce what it means for a soldier to run minimal psychological risk for deployment in the military context, but the question arises how it can be understood and applied in the PWB context. An overview of the positive psychology literature - more specifically literature dealing with PWB - highlights the work of Rothmann and Cooper,250 who designed an integrative diagnostic model for PWB in the work context. Closer analysis of this model suggests that it might be of good use in the context of fitness-for-duty evaluations in the military, especially when it is related to the abovementioned definition of psychological risk. This model was therefore explored in more detail while it was also contextualised to the military environment into what the author refers to as an integrative military model for soldiers' psychological well-being in the external deployment context.
Integrative military model for soldiers' psychological well-being in the external deployment context
Rothmann and Cooper's251 model was designed to address PWB in the work context, which in this instance, would be the military environment in general and more specifically deployments outside the borders of South Africa, also referred to as external deployments. See Figure 1 below for a graphic representation of the suggested integrative military model.
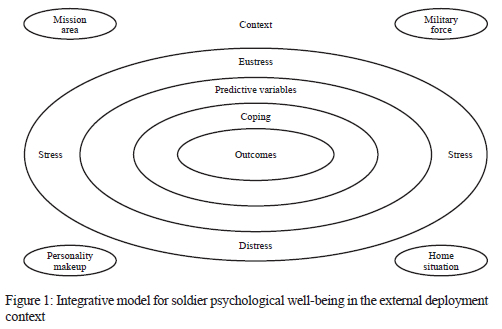
The context illustrated by the outer square in Figure 1 will typically refer to the anticipated mission area as a social system with everything related to it in combination with the physical and geopolitical characteristics of the country or deployment area, for example whether it is a desert or tropical forest, with its weather patterns and all other factors related to it. The military force (work context) includes own and opposing forces, the deploying soldier's situation back home, i.e. his or her family; the soldier's support systems; and things taking place in his or her home unit. The context will also include the psychological or personality makeup of the soldier, which would be his or her personality, psychological resources and interpersonal relationships as manifested in terms of group dynamics.
Moreover, a number of "outside forces",252 which are not part of the individual or the organisation are present and affect the context, such as social change, race, gender, social class and community, family and other environmental factors, as well as 'organisational forces', such as job demands and job resources. As different soldiers tend to react differently to the same stressor, there are also moderating forces related to the context, such as perception, job experience, self-efficacy, social support, locus of control, sense of coherence, psychological hardiness, coping and optimism that contribute uniquely to the manifestation of stress in each individual. In some cases, this will be eustress. In others, it will be distress based on the actual environment and how the individual interprets the environment in conjunction with the abovementioned stressors and other moderator variables.253 Cilliers and Flotman254 observe that distress due to non-coping manifests in negativity, emotional alienation, an increase in bureaucratic and autocratic leadership, poor decision-making and ineffective process and people management, which will all have an adverse influence on deployed forces. Individually, or in combination, these forces affect the well-being of soldiers, manifesting in physical effects, such as headaches, ulcers, insomnia and decreased immunity; psychological effects, such as anger, depression, tension and boredom; behavioural effects, such as substance abuse, overeating or undereating, and sleeplessness.255 From these forces, one can formulate predictive variables on the basis of which one can predict the outcomes in relation to the particular soldier's ability to cope with these stressors. These predictive variables can be used to make predictions in terms of soldiers' future behaviour based on present and past behaviour.
This model can be further enhanced by other theoretical models, such as the Person-Environment Fit Model and the Person-Environment-Occupation Model. The Person-Environment Fit Model focuses on how the degree of fit and the interaction between individual characteristics and their perceived environmental influence one another.256 The Person-Environment-Occupation Model demonstrates and conceptualises how a person and his or her environment and occupation (in this case, a soldier) interact dynamically over time.257 It was however beyond the scope of this study, which suggested consideration of a positive psychology approach for pre-deployment fitness for duty evaluations for external deployments. This approach can thus be viewed as still in its infancy, and limited research is available on these models in this particular context. Future research could focus on linking these models to psychological risk in the military setting.
From the discussion above, the question arises how this positive psychology-related model could be applied to the fitness-for-duty evaluation process in the SANDF. The section below presents a proposal on a process that could be followed.
Proposed pre-deployment fitness-for-duty evaluation process based on positive psychology
It is evident that in the current process, the focus is stronger on a medical model of decision-making with respect to whether a soldier is fit for duty outside South Africa than on a positive psychology model. It is therefore suggested that the proposed pre-deployment screening process should go beyond the medical model paradigm, which resulted in a stigmatised process. Instead, a positive psychology perspective that focuses on optimal functioning should be gained by adopting a comprehensive risk assessment approach centring on "the whole person" context.258 From this viewpoint, the medical process forms part of a more comprehensive process, considering the individual soldier in all his or her complexity. As a result, the broad spectrum of personal and systemic variables affecting adjustment and functioning in the deployment area could be considered. This should result in recognising risk factors that may currently be overlooked. For example, behavioural risk factors of dysfunctional behaviour, such as a tendency towards dishonesty or bullying, will not be identified through the current medical model-driven screening process.
The main idea is to obtain as much information as possible to decide whether a person is an acceptable psychological risk for external deployments. For this reason, various role players are included to become part of the pre-deployment screening team. Their main aim would be to make an informed decision on whether a particular soldier is suitable for external deployment. Such an informed decision can be made through weighing up risk and moderating factors stemming from contextual analysis of the individual's full spectrum functioning - medical, psychological, social and behavioural. In this regard, De Soir259 observes that, if a soldier's pre-deployment well-being is relatively low, it is likely to decrease further during the period of deployment.
Furthermore, it is suggested that the new decision-making process should function in the form of a panel, which is convened after the units and individuals earmarked for deployment have been identified and after all relevant medical and other information has been obtained. It is suggested that all role players in deciding on a particular soldier's fitness-for-duty or deployment be present at the panel, whether physical or virtual (for example, online with a program, such as Zoom or Microsoft Teams). This process can be easy if the required information is obtained because in most cases, a whole unit, such as an infantry battalion, will be deploying. However, it is usually the support staff (logistics, human resources, and finance) that comes from other units. In the large infantry units, it would be easy to involve immediate supervisors in the panel, but it might not be possible to involve support personnel from other units. In practice, this means that, if a specific platoon or company is deployed, the whole company and/or platoon is dealt with simultaneously at the panel. The objective of the panel is to identify those soldiers deemed to be imminently or potentially dangerous; thus, posing a risk to themselves and to others. Health information provided by healthcare practitioners (medical and psychological practitioners, social workers and other relevant medical experts) is supported by the inclusion of collateral information from command, the military legal practitioner, the spiritual guide (chaplaincy),3 and counter-intelligence personnel. The inclusion of command refers to the person's immediate superior. Budd and Harvey260refer to the inclusion of the immediate superior and senior enlisted personnel when they describe them as usually the best sources of information on a soldier's behaviour and work performance, followed by the person him- or herself, the person's records and lastly psychological testing. This process is likely to counterbalance the limitations of self-report only alluded to above.
It is furthermore suggested that the person designated to command the external deployment be the chairperson of this panel. However, care should be taken not to divulge confidential medical information regarding the soldier, but to restrict inputs to the colour code mentioned earlier. Any information that the role players think ought to be considered for the decision should be mentioned at the panel. The military law officer could, for example, confirm whether the person has a record of misconduct or whether he or she has any outstanding court cases. Based on the author's personal experience, many of the soldiers who had been repatriated from external mission areas for conduct-related issues were already a challenge for their commanders in their home country. This kind of information can be considered to obtain a holistic picture of the 'whole person', not only the medical information. In this way, individuals that already present a challenge would be excluded from external deployment because of the psychological or behavioural risk that they pose, based on the notion alluded to above, namely that past behaviour predicts future behaviour.
The proposed process introduces a new pre-deployment screening model, although it may combine existing processes, such as confirming whether a person has any outstanding legal issues that function independently from one another. In this way, all the information would be made available in one place ('under one umbrella') and an informed decision could be taken under the chairmanship of the commander who has to command the force during the external deployment.
Concerns may be duly raised about the complexity and time-consuming nature of the proposed process. However, if the data collection and analysis functions are sufficiently decentralised along functional lines, the final panel discussion could be streamlined and time-efficient. For example, suppose the key role players limit their inputs to high-level findings (clearly defined risk and moderating factors). In that case, quick decisions can be made about individuals posing little risk while more time can be allocated for deliberation on individuals where risk factors outweigh moderating factors. The benefit of an informed decision - which was not possible in the past - will turn the scale in favour of such an integrated process. Information obtained from the panel discussions can also be used to determine trends and individuals who might require interventions. It might even be possible to identify positive psychology-related interventions, such as optimistic intervention, strength-building measures, or meaning-oriented interventions261to be implemented as part of preparing the force for the particular mission.
The suggested process is theoretical in nature and still needs to be tested in practice in against the existing process and in cooperation with the prospective role players. However, theorising is a good start, and when considering that the founding father of social psychology, Kurt Lewin, surmised, "[t]here is nothing so practical as good theory",262 this statement implies that a good foundation has already been laid for a process that could possibly work. It would therefore be apt to make some recommendations to military decision-makers on the proposition to approach pre-deployment fitness-for-duty evaluations from a positive psychology perspective.
Recommendations for military decision-makers
Based on the discussion above, it is thus suggested that military decision-makers in the SANDF in general and more specifically in the SAMHS move away from the stigmatised view of psychopathology to that of psychological risk. From a positive psychology approach, psychological risk can be identified more effectively than from a medical model, and it can be approached as something more manageable, such as any other workplace safety and health risk. In this way, commanders would also have increased control over managing the risks. Nevertheless, it will remain imperative, firstly, to identify those soldiers deemed imminently or potentially dangerous to minimise the risk posed to themselves, others or the success of the mission and, secondly, to assist the members in their well-being.
The importance of the role of leadership in managing the psychological well-being of subordinates is emphasised by Rothmann and Cooper263 when they suggest that "good" leaders should initiate a process to assess the impact of the various risk factors on overall functioning at present and in the future. It is also important that leadership identify what can be done to improve the overall well-being of soldiers individually and/or as part of the 'military family' to enable them to function optimally and to be able to be utilised in the military in fulfilling its constitutional obligations.
Military decision-makers must be encouraged to initiate and support further research into pre-deployment screening processes and into coping under deployment situations with their unique stressors. It might also be possible to link such research to research on stressors in the mission area and dysfunctional behavioural patterns observed during external deployments. This could include research into identifying soldiers' existing coping mechanisms and developing programmes to improve their coping skills before and during deployments. Closely linked to these programmes is training that can be covered in employee well-being programmes that address issues, such as management of time and/or stress, self-management and coping strategies, addressing personality characteristics, such as psychological hardiness, resilience and personal effectiveness. In this way, areas for interventions, such as psychoeducation could assist in improving a soldier's general PWB. Positive psychology-based interventions can also provide effective tools for working with psychologically distressed soldiers.264 Military psychologists could thus follow a positive psychology approach in screening soldiers for deployment and could consider looking into post-deployment programmes for reintegrating soldiers into their communities and non-deployment routines, as this is essential to lay the foundation for future deployments. Positive psychology-related reintegration interventions could focus on sharing the success stories of the deployment with families, the community and unit members who did not deploy. The crux of the recommendations made to military decision-makers is to make a deliberate effort to include positive psychology into the regime of the SANDF to improve the PWB of soldiers.
Conclusion
A positive psychology approach will not mean a move away from 'selecting out' soldiers unsuitable for deployment. It is however a 'tool' in the hand of the military psychologist as the current selection instrument becomes part of a more inclusive and more informative process of considering collateral information in deciding on the suitability of individuals for external deployments. It is likely to be advantageous for the SANDF, and it will make the deploying force commander part of the decision-making process. In this way, the force commander has more information on which informed decisions can be made than in the past and more useful and succinct feedback can be given to sub-level commanders. This will give the clients of the SAMHS additional insight into the process that was followed to reach a decision, and the client (in this case, the force commander) will become part of making the decision. The client can take responsibility for assisting with the development of the affected soldier's PWB and will have a good understanding of what might be required to ensure the PWB of other soldiers as well. Furthermore, research on existing challenges in the various mission areas can be used to improve the selection process. Positive psychology elements included in a holistic approach could realise benefits for the different stages of deployment, such as the preparatory phase, the deployment and adjustment phase, as well as the preparation for reintegration once deployment has been completed.
This article does not provide a solution to military decision-makers but rather acts as an 'appetiser' for further exploration of positive psychology within the context of fitness-for-duty evaluations. It also supports the observation in a recent book on military psychology in South Africa that there is a need for a broad shift towards positive psychology and proactivity in the management of wellness in the SA military context.265 Future research can further explore the integration of the Person-Environment-Fit Model, the Person-Environment-Occupation Model and other constructs related to positive psychology, such as engagement, resilience, hardiness, organisational affective commitment, flourishing, psychological capital and well-being, to name a few. Lastly, the SANDF in general and more specifically the SAMHS Directorate Psychology will benefit from the suggested expansion of this model and approach by, for example, developing a taxonomy of stressors related to deployment and trends in morale and engagement at different stages of deployment.
2 Conceptualised by Aaron Antonovsky, the salutogenic paradigm refers to looking at health and illness not as a dichotomy but as a continuum. Salutogenesis focuses on the study of the origins of health rather than on the origins of disease.
3 This will be omitted if the person has no spiritual connection.
188 Piet Bester grew up on a farm in the Orange Free State. After matriculation, he did national service (conscription). Piet joined the South African Defence Force, attended the South African Military Academy, obtained various degrees, and completed the University of Johannesburg's Doctoral Programme: Leadership in Performance and Change. He is also a registered Industrial Psychologist and completed various military courses, including the Joint Senior Command and Staff Programme and Security and Defence Studies Programme, including a Post Graduate Diploma in the Management of Security at the University of the Witwatersrand. Piet is currently a senior lecturer at the University of Stellenbosch's Faculty of Military Science. His research interests include leadership, integrity, performance enhancement, test construction, and national security.
189 P Fabricius. "SA should first sort out its own backyard". Institute for Security Studies. 20 July 2017. <https://issafrica.org/amp/iss-today/sa-should-first-sort-out-its-own-backyard> Accessed on 30 March 2019. [ Links ]
190 AllAfrica. "Southern Africa: SADC extends military mission to Mozambique". 19 January 2022. <https://allafrica.com/stories/202201190096.html> Accessed on 20 January 2022.
191 G Martin. "SANDF peacekeeping efforts continue in Africa". defenceWeb. 14 April 2019. <https://www.defenceweb.co.za/joint/diplomacy-a-peace/sandf-peacekeeping-efforts-continue-in-africa/> Accessed on 12 May 2022. [ Links ]
192 defenceWeb. "SANDF has 2 100 soldiers deployed on peacekeeping operations". 14 April 2019. <https://www.defenceweb.co.za/sa-defence/sa-defence-sa-defence/sandf-has-2-100-soldiers-deployed-on-peacekeeping-operations/> Accessed on 12 May 2022.
193 PC Bester & JW O'Neil. "The military leadership training landscape of the South African National Defence Force as related to extreme situations". In M Hollenweger (ed), Leadership in extreme situations. Zurich: Springer, In press, 1-25.
194 H Boshoff. "African battle space and conflict". Presentation. Pretoria: Institute for Security Studies, 2009. <http://aardvarkaoc.co.za/wp-content/Conf_Aug_2009/Henri%20Boshoff%202.pdf> Accessed on 11 August 2019; I Ichikowitz. "The African battle space is not the Middle East". defenceWeb. 7 December 2017. <https://www.defenceweb.co.za/land/land-land/the-african-battle-space-is-not-the-middle-east-ichikowitz/> Accessed on 19 March 2019; N Alusala. "Managing the battle space: Women on the frontline in Eastern DRC". Institute for Security Studies. 14 January 2016. <https://issafrica.org/research/central-africa-report/managing-the-battle-space-women-on-the-frontline-in-eastern-drc> Accessed on 19 August 2019; Bester & O'Neil op cit.
195 JJ Gouws. "Military stress and resillience, post-psychological assessment: Factors affecting armed forces' resillience". In A Macintyre, D Lagace-Roy & DR Lindsay (eds), Global views on military stress and resillience. Kingston: Canadian Defence Academy Press, 2017, 113-126.
196 GL Lindenfield, G Rozelle, J Hummer, MR Sutherland & JC Miller. "Remediation of PTSD in a combat veteran: A case study". NeuroRegulation 2. 2019. 102-125. doi:10.15540/nr.6.2.102 [ Links ]
197 Ibid., pp. 102-103.
198 United Nations. Medical support manual for United Nations field operations. New York, NY: Department of Peacekeeping Operations, 1995.
199 A Neale. "Reflecting on 15 years of psychological (pre- and post-deployment) screening in the SANDF". Presentation at the 56th Annual International Military Testing Association Conference, Hamburg, 27-31 October 2014.
200 Ibid.
201 RJ Rona, KC Hyams & S Wessely. "Screening for psychological illness in military personnel". The Journal of the American Medical Association 293/10. 2005. 1257-1260. doi:10.100/Jama.293.10.1257 [ Links ]
202 FC Budd & S Harvey. "Military fitness-for-duty evaluations". In CH Kennedy & EA Zillmer (eds), Military psychology: Clinical and operational applications. London: The Guilford Press, 2006, 35-60.
203 CLM Keyes, BL Fredriksen & N Park. "Positive psychology and the quality of life". In KC Land, AC Michalos & JM Sirgy (eds), Handbook of social indicators and quality of life research. Amsterdam: Springer, 2012, 99-112.
204 Military Psychological Institute (MPI). Manual for the Psychological Risk Indicator 2.5: A psychological screening tool for concurrent health assessment. Pretoria, 2019.
205 Keys et al. op. cit., pp. 101-102.
206 South African Military Health Service (SAMHS). South African Military Health Service patient administration policy and procedures. SAMHS Order: Pat Admin 05/2002. Pretoria, 2006.
207 Budd & Harvey op. cit., p. 35
208 SAMHS op. cit., p. 8-5.
209 It is, however, important to note that the CHA is also used for entry and exit medicals and is used as the main programme for occupational health surveillance in the SANDF, although it was not initially designed for that purpose. The focus of this study is however on the use of the CHA as a pre-deployment screening process.
210 MPI op. cit., pp. 1-2.
211 Ibid., p. 16.
212 Ibid., p. 2.
213 SAMHS op. cit., p. 8-2.
214 The SANDF has different classifications of information, of which 'patient confidentiality' is a category, referring to health- (medical-) related information of an individual. The others are restricted, confidential, secret and top secret and it mainly refers to information and material.
215 KS Pedneault. The use of self-report data in psychology. 2020. <https://www.verywellmind.com/definition-of-self-report-425267> Accessed on 16 June 2022.
216 D Sue, DW Sue, DM Sue & S Sue. Essentials of understanding abnormal behavior (3 ed). Boston, MA: Cengage Learning, 2017, 2.
217 Definition adopted from the DSM-5: American Psychiatric Association. Diagnostic and statistical manual for mental disorders (5 ed). Washington, DC, 2013, 20.
218 SO Lilienfeld, SF Smith & AL Watts. "Issues in diagnosis: Conceptual issues and controversies". In WE Craighead, DJ Miklowitz & LW Craighead (eds), Psychopathology: History, diagnosis and empirical foundations. San Francisco, CA: Wiley, 2017, 1-35.
219 European Agency for Safety and Health at Work. Psychological risk and stress at work. 2019. <https://osha.europa.eu/en/themes/psychosocial-risks-and-stress> Accessed on 12 February 2019.
220 M Born & H van der Flier. "Risk management through the psychological looking glass". YouTube. Video File. 6 May 2019. <https://youtu.be/BWVY4H2pNS8> Accessed on 12 May 2019.
221 W Wiese. Presentation on espionage case studies. Pretoria: Defence Intelligence Media Centre, 1997.
222 PC Bester. Background to comprehensive profiling services. Pretoria, 2006, 1.
223 B McSherry. "Risk assessment by mental health professionals and the prevention of future violent behaviour". Trends and issues in criminal justice. Canberra: Autralian Institute of Criminology, July 2004. <http://www.aic.gov.au> Accessed on 10 August 2019.
224 MPI op. cit., p. 2.
225 Ibid.
226 KC Kalmbach & BA Moore. "Posttraumatic growth in military populations: Theory, research, and application". In U Kumar (ed.), The Routledge international handbook of military psychology and mental health. London: Routledge, 2020, 133-150.
227 J MilniC. "Salutogenic model of health, a sense of family coherence and proactive coping among adolescents". In A Pesic (ed.), Stress in military profession. Belgrade: Odbrana, 2018, 113-124.
228 Ibid., p. 114.
229 C Jacob & D Lagacé-Roy. "Military stress and resillience: Introduction to the 2017 International Military Testing Association inaugural volume." In Macintyre et al. op. cit., pp. 3-4.
230 Ibid., pp. 4-5.
231 DC Funder & CR Colvin. "Explorations in behavioral consistency: Properties of persons, situations, and behaviors". Journal of Personality and Social Psychology 60/2. 1991. 773-794.
232 I Rothmann & CL Cooper. Organizational and work psychology. London: Hodder Education, 2008, 239.
233 European Agency for Safety and Health at Work op. cit.
234 Ibid.
235 S Rothman, K Mostert & M Strydom. "A psychometric evaluation of the job demands-resources scale in South Africa". South African Journal of Industrial Psychology 32/4. 2006. 76-86.
236 S Joseph. "Preface". In S Joseph (ed.), Positive psychology in practice: Promoting human flourishing in work, health, education and everyday life. Hoboken, NJ: Wiley, 2015, xi-xiii; F Cilliers & A Flotman. "The psychological well-being manifesting among master's students in industrial and organisational psychology". SA Journal of Industrial Psychology 42. 2016. 1-1. doi: 10.4102/sajip.v42i1.1323
237 Archana, S Ahuja & U Kumar. "Shaping military leaders: Role of character strengths and virtues". In Kumar op. cit., p. 125.
238 MD Matthews. "Cognitive and non-cognitive factors in soldier performance". In JH Laurence & MD Matthews (eds), The Oxford handbook of military psychology. London: Oxford University Press, 2012, 197-217.
239 Milnic op. cit., pp. 113-124. Footnote * refers to: A Antonovsky, Health, stress and coping. San Franciso: Jossey-Bass Publishers, 1979, vii.
240 N Ferreira. "Hardiness in relation to organisational commitment in the human resource management field". SA Journal of Human Resource Management 10/2. 2012. 1-10. doi: 10.4102/sajhrm.v10i2.418
241 MD Matthews. "Towards a positive military psychology". In MD Matthews & JH Laurence (eds), Military psychology (Vol 3). London: Sage, 2012, 283-292.
242 Ibid.
243 T Kasser. "The science of values in the culture of consumption". In S Joseph (ed.), Positive psychology in practice: Promoting human flourishing in work, health, education and everyday life. Hoboken, NJ: Wiley, 2015, 83-102.
244 Cilliers & Flotman op. cit.
245 Ibid.; Rothmann & Cooper op. cit., p. 230.
246 D Arendse. "A psychological wellbeing model for South African military students". In NM Dodd, PC Bester & J van der Merwe (eds), Contemporary issues in South African military psychology. London: Routledge, 2020, 53; Kasser op. cit.; Joseph op. cit.
247 Ferreira op. cit.
248 The term 'job security' is presented here in its traditional work context, implying guaranteed employment. The opposite of job security is job insecurity, usually viewed as when a person has no guarantee of employment. However, in the context of military deployment, the insecurity may be related to aspects such as lack of role clarity, the looming unknown and uncertainty about how one's training would hold up in an unfamiliar/potentially adversarial environment. This matter warrants further investigation in future research.
249 C Ruini. Positive psychology in the clinical domains: Research and practice. Bologna: Springer, 2017, 45, 84.
250 Rothmann & Cooper op. cit., pp. 229-248: I Rothmann & CL Cooper. Work and organizational psychology. London: Routledge, 2015.
251 Rothmann & Cooper, Organizational and work psychology op. cit., pp. 229-248.; Rothmann & Cooper Work and organizational psychology op. cit.
252 Cilliers & Flotman op. cit.; S Rothman & CL Cooper. Work and organizational psychology (3 ed). Routledge: New York, 2021, p. 228.
253 This relates to Murray's need press model, which describes two types of classifications of environmental stimuli that impact an individual's behaviour. The first is alpha press, which is the actual environment, and the second is beta press, which is how the environment is perceived by that individual. These presses in combination with human needs determine the individual's behaviour. S Hirata & DL Fisher. "Re-activating the learning environment research in environmental psychology". The Japanese Journal of Environmental Psychology 1/1. 2013. 27-37; H Murray. Explorations in personality. New York, NY: Oxford University Press, 2008.
254 Cilliers & Flotman op. cit.
255 Rothmann & Cooper, Organizational and work psychology op. cit., pp. 236-237.
256 V Parkash. "Stress experiences and abilities to cope". In Kumar op. cit., p. 355.
257 M Law, B Cooper, S Strong, D Stewart, P Rigby & L Letts. "The person-environment- occupation model: A transactive approach to occupational performance". Canadian Journal of Occupational Therapy 1. 1996. 102-125. doi: 10.1177%2F000841749606300103
258 Bloom Leadership. "6 areas of whole person development: Professional". 2017. <http://www.bloomleaders.com/blog/2017/1/25/6-areas-of-whole-person-development-professional Accessed on 20 August 2019; W Henderson. "Security clearance: The whole-person concept". ClearanceJobs. 2010. <https://news.clearancejobs.com/2010/12/27/security-clearance-the-whole-person-concept/> Accessed on 20 August 2019; O Boe, KK Wooley & J Durkin. "Choosing the elite recruitment, assessment and selection in law enforcement tactical teams and military special forces". In PJ Sweeney, MD Matthews & PB Lester (eds), Leadership in dangerous situations: A handbook for the armed forces, emergency services, and first responders. Annapolis, MD: Naval Institute Press, 2011, 333-349.
259 E de Soir. "Psychological adjustment after military operations: The utility of postdeployment decompression for supporting health readjustment". In SV Bowles & PT Bartone (eds), Handbook of military psychology: Clinical and organizational practice. Cham: Springer, 2017, 89-103.
260 Budd & Harvey op. cit.
261 There are many more than suggested here. See for example MR Crowdhury. "19 best positive psychology interventions + how to apply them". PositivePsychology. N.d. <https://positivepsychology.com/positive-psychology-interventions/> Accessed on 20 February 2020.
262 P Marsden. "Nothing so practical as good theory: Syzgy's Mark Ellis on social commerce". digitalwellbeing.org. N.d. <https://digitalwellbeing.org/nothing-so-practical-as-good-theory-syzygys-mark-ellis-on-social-commerce/> Accessed on 17 August 2019.
263 Rothmann & Cooper, Organizational and work psychology op. cit., p. 238.
264 Matthews op. cit., 2012. Military psychology (Vol 3)., p. 285.
265 N Dodd, J van der Merwe & P Bester. "Conclusion". In Dodd et al. op. cit., p. 235.

