










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Childhood Education
versión On-line ISSN 2223-7682
versión impresa ISSN 2223-7674
SAJCE vol.11 no.1 Johannesburg 2021
http://dx.doi.org/10.4102/sajce.v11i1.930
ORIGINAL RESEARCH
The ability of teachers to identify Grade 1 learners in low socio-economic environments with possible developmental coordination disorder
Aletta M. du PlessisI; Monique de MilanderI; Frederik F. CoetzeeI; Mariette NelII
IDepartment of Exercise and Sport Sciences, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIDepartment of Biostatistics, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Early identification of learners in low socio-economic environments with possible developmental coordination disorder (DCD) is important. Although various screening tools are available, it is unclear whether teachers can use the movement assessment battery for children - second edition checklist (MABC-2 checklist) to identify learners with possible DCD.
AIM: To establish teachers' ability to identify Grade 1 learners in low socio-economic environments with possible DCD.
SETTING: The study was conducted in the Mangaung Metro, Motheo District of the Free State Province, South Africa. Grade 1 learners aged 6-8 years (n = 200) from a low socio-economic environment attending quintile one to three schools were randomly selected for assessment. Twenty-nine teachers participated in the study.
METHODS: Kinderkineticists identified learners with possible DCD (displaying motor skills far below the child's age) by means of the MABC-2 performance test. The teachers used the MABC-2 checklist to identify possible DCD. The convergent validity of the MABC-2 performance test and checklist was compared.
RESULTS: The convergent validity between the MABC-2 performance test and the MABC-2 checklist indicated a kappa (k) coefficient of 0.17, indicating a slight agreement between the performance test and the checklist. Overall, the specificity was 58% (105/180), and the sensitivity was 85% (17/20).
CONCLUSION: Teachers could effectively identify learners with possible DCD. However, they demonstrated a low ability to identify learners without possible DCD when using the MABC-2 checklist. It is therefore recommended that the performance test should be used in conjunction with the checklist to obtain the most reliable results.
Keywords: developmental coordination disorder (DCD); movement assessment battery for children - second edition (MABC-2); checklist; teachers; motor skills; children; learners; low socio-economic environment; prevalence.
Introduction
Developmental coordination disorder (DCD) in children has become a constant concern in the last two decades (Blank et al. 2012; Geuze & Börger 1993; Schoemaker et al. 2006). When children are diagnosed with DCD, they experience low motor skill abilities without the evidence of a neurological disorder and cannot be related to a general medical difficulty such as cerebral palsy or a pervasive development disorder (American Psychiatric Association [APA] 2013; Kadesjö & Gillberg 1998; Visser 2003). The low motor skill abilities of these children are significant to the extent that these interfere with their social competence, academic performance and physical development, leading to problems with completing activities of daily living (Blank et al. 2012; Lingam et al. 2009). Therefore, DCD involves motor skill difficulties that have a negative influence on children's performances during daily activities.
Difficulties in performing daily activities include home activities (dressing themselves), play activities (ball skills and balance) and academic skills, such as writing and reading (Asonitou et al. 2012; Edwards et al. 2011). Secondary effects associated with DCD include social problems such as psychosocial challenges (Karras et al. 2019; Pratt & Hill 2011; Sylvestre et al. 2013) and low self-esteem (Missiuna et al. 2006, 2014; Zwicker et al. 2012), whilst physical challenges include lower cardiorespiratory fitness (Aertssen et al. 2018; Cairney et al. 2017), low strength and flexibility (Batey et al. 2014; Smits-Engelsman, Jelsma & Ferguson 2017) and increased obesity (Philips et al. 2016; Rihtman, Wilson & Parush 2011). A significant matter of concern is that DCD has been described as one of the most common motor neurological developmental disorders in school-aged children (Zwicker et al. 2018) and is present in 5% - 6% of school-aged children worldwide (APA 2013). The reported incidence of DCD could be influenced by the assessment tool used to identify motor skill difficulties and possible DCD (Amador-Ruiz et al. 2018).
Terms such as possible DCD, suspected DCD or at risk for DCD have been used in research studies where a complete diagnostic assessment of DCD has not been conducted (Alesi, Pecoraro & Pepi 2019; Delgado et al. 2019; Lingam et al. 2009; Valentini, Clark & Whitall 2015). The APA (2013) proposed that the Diagnostic Statistical Manual of Mental Disorders fifth edition (DSM-5) should be taken into consideration before the diagnosis of DCD can be made. In order to determine criterion A (execution of coordinated motor skills significantly lower than the child's chronological age) and criterion B (deficits in criterion A interferes with the child's daily activities) of DSM-5, an evaluation of motor proficiency abilities of the child and how this has an influence on daily living activities should be conducted (APA 2013; Blank et al. 2019; Van Waelvelde et al. 2007). Criterion C states that the onset of the motor difficulties should occur in the child's early developmental period and criterion D states that the motor difficulties experienced are not because of intellectual, visual or other neurological impairments (APA 2013). Criteria C should be ruled out by a medical practitioner and criteria D should be kept in mind if a neurological impairment exists (Blank et al. 2012).
Using norm-referenced tests, such as the movement assessment battery for children - second edition performance test (MABC-2 performance test) (Henderson, Sugden & Barnett 2007) and the Bruininks-Oseretsky test of motor proficiency - second edition (BOT-2) (Missiuna et al. 2011), to measure a child's motor proficiency is required for accurate assessment of motor skills. However, these tests have been labelled as time-consuming, having long waiting lists for children to be evaluated and being financially out of reach for children living in low socio-economic environments (Junaid et al. 2000; Schoemaker et al. 2006; Van der Walt, Plastow & Unger 2020). An alternative approach is to make use of questionnaire-based assessments (Dimitropoulou et al. 2019).
The Motor Observation Questionnaire for Teachers (Van Dellen, Vaessen & Schoemaker 1990), the MABC original and second edition checklist (MABC-2 checklist) (Henderson et al. 2007) and the Developmental Coordination Disorder Questionnaire'07 (DCDQ'07) (Wilson et al. 2009) have previously been used as questionnaire-based assessments. Faught et al. (2008) were of the opinion that screening children's motor skill abilities by making use of questionnaires was more useful and put emphasis on the important role that teachers play in identifying difficulties with motor skills. The importance of more research regarding the input from schools with the main focus on teachers to identify children with motor difficulties has been emphasised (Barnett 2008:114; Missiuna et al. 2011). Teachers have the ability to observe learners in various situations, for example, during academic learning activities and play time (Faught et al. 2008; Larkin & Rose 2005). Asunta et al. (2017) elaborated on the importance of a suitable screening tool for teachers for early identification of learners with motor skill difficulties.
Although the MABC-2 checklist can be used by teachers, uncertainties have been raised regarding the suitability of the screening tool for the identification of motor skill difficulties (Barnett 2008; Peters & Henderson 2008), and disagreement continues whether teachers and therapists can identify the same children with motor skill difficulties and possible DCD when this screening tool is used (Missiuna et al. 2011; Schoemaker et al. 2008). Table 1 shows the total percentages of motor skill difficulties identified in children by teachers (using the MABC original and second edition checklist) which were also identified with the performance test. For example, in Table 1, Schoemaker et al. (2012) reported that class teachers identified 26 (41%) of the 64 children by the performance test with motor skill difficulties. Only two studies were found in South Africa in the Free State province. The class teachers were able to identify 46.5% of the children with motor difficulties who were also identified with motor difficulties using the MABC-2 performance test in the one study (De Milander, Coetzee & Venter 2016), whereas another study by the same authors indicated an ability of 35.6% (De Milander, Du Plessis & Coetzee 2019). Both studies indicated a low ability of teachers to identify motor difficulties. Both of these studies were conducted in high socio-economic environments. The only other study to the authors' knowledge on the MABC checklist in South Africa was the earlier study on 94 children (9-12 years) in the North West province with the aim to determine whether class teachers are reliable to use the MABC checklist as a screening tool for DCD; however, the teachers only completed two of the sections of the checklist and the focus was on the reliability of the teachers and the convergent validity was not provided (Lombard & Pienaar 2003).
Table 1 demonstrates a variation in the results where some results show a meagre ability of class teachers to correctly identify children with motor difficulties using the MABC original and second edition checklist and some show a very high ability ranging from 14.3% (Junaid et al. 2000) to 85% (Schoemaker, Smits-Engelsman & Jongmans 2003). Therefore, controversy exists regarding the efficacy of using the checklist as a screening tool for motor difficulties. Furthermore, Table 1 emphasises the limited availability of studies regarding the second edition of the MABC, studies in low socio-economic environments, studies in low-to-middle-income countries and research findings in South Africa. Therefore, more research should be conducted.
South Africa has incongruent socio-economic classes that can influence assessment tools and therapists' availability to conduct these assessments in different populations (Pienaar 2004). Low socio-economic environments are found in townships, the inner city and peri-urban areas of South Africa (Ndebele 2015) and are identified when observing poverty, income, education, environmental factors, working conditions and health conditions in these areas (Isaacs-Martin 2015; Narsai et al. 2013; Pappin et al. 2015; Pienaar & McKay 2014). The considerable diversity of socio-economic classes in South Africa has led to unequal educational opportunities for learners (Graven 2013). Consequently, the South African government has categorised public schools into five quintiles ranging from non-fee paying schools to fee-paying schools to allocate financial resources to specific schools (Graven 2013; Hall & Giese 2008; Ogbonnaya & Awuah 2019).
In South Africa, many children living in low socio-economic environments experience low motor skill abilities (Pienaar & Kemp 2014) because of limited opportunities to practice fundamental motor skills (Ferguson, Naidoo & Smits-Engelsman 2015; Gallahue & Ozmun 2006) and may therefore be identified with possible DCD (Hardy et al. 2012; Uys & Pienaar 2010; Valentini et al. 2015). Furthermore, the children living in low socio-economic environments are not adequately motivated to develop fundamental motor skills and in many cases, insufficient instructions and limited physical education opportunities for the development of these skills are provided (Barnett et al. 2016; Gallahue & Ozmun 2006; Pienaar & Kemp 2014). Pienaar, Barhorst and Twisk (2013) found in their study on 812 children living in the North West Province of South Africa that learners in quintile one to three schools performed poorly in perceptual-motor development skills and required additional help with these skills. Research in low socio-economic environments of the Western Cape found that fewer opportunities and activities are available for children and educators living in these environments (Senekal et al. 2015). Motor proficiency challenges could have a negative influence on young children's academic skills and their interest in sport participation (Pienaar & Kemp 2014).
Although the literature is available regarding children's motor skill abilities, research in low socio-economic environments in South Africa is still limited (De Waal, Pienaar & Coetzee 2018; Pienaar & Kemp 2014; Uys & Pienaar 2010). Uys and Pienaar (2010) reported in their study on 69 children between 4 and 71 months that the children from lower socio-economic environments had lower motor development abilities than children from the higher socio-economic environment. In accordance, De Waal et al. (2018) and Pienaar and Kemp (2014) reported higher tendencies of possible DCD in children (8-10 years old & 6-7 years old) from low socio-economic environments in the Zeerust District of South Africa and the North West Province.
Consequently, it is vital to investigate the motor skill abilities of learners living in low socio-economic environments in South Africa and to ensure appropriate identification methods of possible DCD for these children. The priority is to determine if teachers can be used in the school community to identify physical features in children that can indicate possible DCD using a screening tool (De Milander et al. 2016). If teachers can identify motor difficulties, they will be able to support children who experience motor difficulties. Teachers can refer children with motor difficulties to formal neurodevelopmental evaluation by a multidisciplinary team, if necessary (Blank et al. 2019). To determine if teachers can play a valuable role, it was essential to determine if the MABC-2 checklist could be used effectively by teachers to identify learners with possible DCD and whether teachers were competent when using the checklist, which constituted the aim of this study. Therefore, the completed MABC-2 checklist (teachers) will be compared to the MABC-2 performance test results (Kinderkineticists in training) of the children.
Methodology
Study design
An empirical study with a cross-sectional design was conducted and focused on a quantitative research method to collect data. Participants of this study included learners and class teachers. The target population was Grade 1 learners between 6 and 8 years of age and the class teachers of these learners. The Grade 1 learners lived in low socio-economic environments in Mangaung, Motheo District, in the Free State Province of South Africa. The cross-sectional design included one assessment tool consisting of two parts. The one part included a standardised testing procedure to identify the prevalence of possible DCD, and the second part comprised a screening checklist to identify the prevalence of possible DCD. The standardised test was completed by trained postgraduate students of Exercise and Sport Sciences (information redacted to maintain the integrity of the review process) specialising in Kinderkinetics (further referred to as movement specialists) and the checklist was completed by the class teachers of the participating learners.
The sample size was determined by including quintile one to three public primary schools within a 30 km radius from Bloemfontein in the Motheo District, Free State Province. A 30 km radius was selected to ensure that the principal investigator and the movement specialists could reach the schools. Quintile one schools are in the most economically disadvantaged geographical areas, whereas quintile five schools are in the most affluent geographical areas (Graven 2013; Hall & Giese 2008). Quintiles one to three schools are the non-fee-paying schools, and according to Ogbonnaya and Awuah (2019), the learners in these schools demonstrate low levels of achievement. The sample size was further determined by considering (1) the duration of administering the MABC-2 performance test and checklist, (2) the number of movement specialists to administer the test, (3) the physical education periods and (4) the budget. A list of schools was obtained from the provincial Department of Basic Education in the Motheo District, from which a random selection was made to finalise the study population. There were 33 quintile one to three schools in the Motheo District within a 30 km radius from Bloemfontein; a total of 3940 Grade 1 learners attended the schools. Using proportional sampling, a total of 10 primary schools were randomly selected, of which two were quintile one and two schools, respectively, and eight were quintile three schools. Within the 10 schools, there were a total of 1179 Grade 1 learners. Using proportional sampling, a total of 400 learners were invited. The sample size per school was determined using random sampling. Limited schools in quintile one and two categories were available within a 30 km radius from Bloemfontein, which formed part of the study's inclusion criteria. Therefore, more quintile three schools were identified.
Participants
The principals of the 10 primary schools were invited to participate in the research study and asked to consider providing permission for the Grade 1 learners in the school and their teachers to participate in the study, to which all the principals agreed. After the principals provided permission, information about the study was sent to the children's parents/legal guardians. Proportional sampling was used to determine the number of learners that should be included, and random sampling was used to determine the sample size per school (Etikan & Bala 2017). The information letters provided to the parents regarding the study included the consent form. The sample consisted of 400 learners.
Of the 400 children in the sample, 242 parental consent forms were returned to the different schools, giving a response rate of 60.5%. These learners also provided assent to participate in the study. Of the 242 learners, 124 (51.2%) were boys and all the children were living in low socio-economic environments in Mangaung. Most learners were 6 years of age (n = 174; 71.9%) with a mean age of 6.66 years (range 6.0-8.75 years). A total of 29 teachers agreed to participate in the study.
The following exclusion criteria were applied for the learners: if learners fell outside the age range of 6-8 years, if their parents indicated that they were relocating and if parents indicated that a medical practitioner diagnosed learners with conditions that included epilepsy, attention deficit and/or hyperactivity disorder (ADD/ADHD), autism spectrum disorder, visual problems, hearing problems, cancer and/or physical disability. The following exclusion criteria applied to the teachers. Teachers were only excluded if they did not want to participate in the study anymore and if they were a relative of one of the learners who participated in the study or if the researcher felt it is in the teacher's best interest not to participate.
Procedure
Two hundred and forty-two Grade 1 learners were tested using the MABC-2 performance test. The lower the score obtained on the MABC-2 performance test, the lower the child's motor coordination skills. Learners were identified with possible DCD when their results fell at or below the 15th percentile on the MABC-2 performance test and within the amber and red zone. For the purpose of this study, the criteria of the DSM-5 were partially met. Learners were categorised as having possible DCD if their motor coordination skills were far below their chronological age when using the MABC-2 performance test (criterion A of the DSM-5). The MABC-2 checklist was used to determine if the performance of activities during daily living was influenced if the child experienced motor skill difficulties (criterion B of the DSM-5). The MABC-2 checklist was completed by the teachers as language barriers could have limited the opportunity for parents to complete the checklist. The influence of motor coordination difficulties on academic performance was not evaluated in this study. The parents indicated on the consent form if the child had any general medical condition and/or intellectual impairment, although a confirmatory diagnosis by a medical doctor could not be obtained because of time constraints and expenses.
The 29 class teachers were requested to complete the MABC-2 checklist. Instructions and demonstrations on the completion of the MABC-2 checklist were provided by the principal investigator to each schools' head of the department (HOD) of the Grade 1 class teachers. The HOD provided the class teachers with instructions, as received from the principal investigator, on how to complete the MABC-2 checklist. The HOD received the instructions because the teachers themselves had teaching responsibilities and were not available for the principal investigator's information session. The information to the HOD included (1) the observation of the learner in the classroom, during physical education classes and on the playground, (2) what to do when the teacher was unable to answer one of the questions and (3) the content and rating of the checklist with regard to sections A, B and C. The teachers had 1 month to complete the checklists. No information was provided to the teachers about the learners' level of motor skills and the findings of the MABC-2 performance test.
The interpretation of the scores of the MABC-2 checklist differs from the performance test. The higher the scores obtained with the MABC-2 checklist, the lower the motor coordination skills of the learners. Learners were identified with possible DCD when they performed at or above the 85th percentile and fell within the amber and red zone. The final sample was determined after the teachers completed the MABC-2 checklist of each participating learner. Learners' checklists were excluded if more than one value was missing. Out of the 242 checklists completed by the teachers, 200 were used in the final analysis.
Measuring instruments
The MABC-2 is composed of three components, (1) a standardised performance test that directly involves the child and can be completed by professionals such as research psychologists, occupational therapists, movement specialists and physiotherapists, (2) a checklist that can be completed by an adult such as parents, teachers and professionals (psychologists, occupational therapists and physiotherapists) and (3) an ecological approach manual to guide intervention for children experiencing motor skill difficulties (Henderson et al. 2007). For the purpose of this study, the standardised performance test and the checklist were used according to the developers' prescriptions and guidelines (Henderson et al. 2007). Previous research has proven the successful use of the MABC-2 in the South African setting (De Milander et al. 2019; De Waal et al. 2018).
Movement assessment battery for children - second edition performance test
The MABC-2 performance test provides for the testing of three age groups, each with their own individual assessment form and activities, and are called age bands. (Henderson et al. 2007). The age bands are divided into 3-6 years (age band one), 7-10 years (age band two) and 11-16 years (age band three) (Henderson et al. 2007). For this study, age bands one and two were used. The learners were required to complete eight motor tasks grouped within three subtests: manual dexterity, balance and aiming and catching (Henderson et al. 2007). Each task was demonstrated to the learner by the movement specialist, where the learner had one practice trial, followed by two trials that were formally evaluated. If the learner was not able to correctly complete the first formal trail or complete the trial within the time frame allocated for the age band, the learner was required to conduct the second formal trial. The learner's performance was evaluated by making use of seconds or number of correct catches. The scores were recorded as raw scores and converted to an item standard score. The sum of the item standard scores provided the general standard score and percentile for each subtest and for the total score. A percentile equal to or lower than five identifies the learner with definite motor skill difficulties (red zone), a percentile score of 6-15 puts the learner in the at-risk or moderate motor skill difficulty category (amber zone) and a percentile score above 15 classifies the learner with no motor skill difficulties (green zone). The MABC-2 is a valid and reliable test. Manual dexterity shows a reliability of r = 0.77, aiming and catching have a reliability of r = 0.84 and the reliability for balance is r = 0.73 (Henderson et al. 2007). The total test score indicates the reliability of r = 0.80, according to Henderson et al. (2007), and even higher reliability (r = 0.97) has been reported (Wuang, Su & Su 2012).
Movement assessment battery for children - second edition checklist
The MABC-2 checklist consists of three sections of which sections A and B (30 items) focus more on motor and movement aspects, whereas section C (13 items) includes other aspects that might influence a child's motor movements (Henderson et al. 2007). Section A measures 'movement in a static and predictable environment' and is divided into three subsections, namely 'self-care skills, classroom skills, and physical exercise (PE)/recreational skills'. Section B measures 'movement in a dynamic and unpredictable environment' and is divided into 'self-care/classroom skills, ball skills, and PE/recreational skills'. The class teacher rated each learner's performance regarding each item listed in the individual sections. The teacher used a four-point scale to indicate how well the learner performed in the different skills. The scale includes 0 - very well, 1 - just OK, 2 - almost and 3 - not close (Henderson et al. 2007). If the teacher did not complete one item in a specific section, the four completed items in the section determined what the score for the empty item would be. If the scores were consistently positive, the learner was allocated a one; if it is consistently negative, the learner was allocated a two. The score results were then added up and a total motor score was interpreted by the red, amber and green of the traffic light system. The higher the total motor score, the weaker the performance, which is in contrast with the MABC-2 performance test. The green zone indicates 'no motor difficulty' with a cut-off point of <85th percentile; amber indicates 'at risk or moderate motor difficulty', indicating percentiles between 85 and 94 and red shows 'definite motor difficulty' with a percentile indication of ≥ 95th percentile. The checklist took approximately 15 min per learner to complete. According to Schoemaker et al. (2012) and Schoemaker et al. (2003), the discriminative validity of the original MABC checklist has been established. Research regarding the reliability of the second edition of the MABC checklist is limited (Brown & Lalor 2009). In addition, the reliability of the original MABC checklist was found to be useful (Shoemaker et al. 2003). Research on the MABC-2 checklist confirmed that the internal consistency was strong (Shoemaker et al. 2012).
To determine if teachers had the competence to identify Grade 1 learners in low socio-economic environments with possible DCD, the results of the MABC-2 checklist were compared with the results of the MABC-2 performance test and the convergent validity was determined. Learners with a score on the 15th percentile and lower (red and amber zone) with the MABC-2 performance test and on the 85th or higher percentile (red and amber zone) for the MABC-2 checklist were referred to as the possible DCD group, which included learners with severe and moderate motor difficulties. The moderate and severe motor difficulties are grouped to categorise children in a possible DCD group and a without DCD group (De Waal et al. 2018). Children below the 15th percentile are categorised as possible DCD because their motor coordination skills are below average (Alesi et al. 2019).
Statistical analysis
Data from the results of the MABC-2 performance test and the checklist were recorded electronically on a Microsoft Excel spreadsheet by the principal researcher (A.d.P.). A statistician was consulted and conducted the statistical analysis. The data were analysed using a statistical analysis software package, SAS version 9.4 (SAS Institute Inc., Cary, NC, United States). Descriptive statistics, namely frequencies and percentages, were calculated for categorical data, and medians and percentiles for numerical data. Bowker's test for symmetry was calculated for paired categorical data as more than two discrete outcomes were measured. The difference in the total score was calculated and compared using the signed-rank test.
The agreement between the results of the MABC-2 performance test and the MABC-2 checklist was determined by means of the kappa (k) coefficient and 95% confidence interval (CI) for k. Values lower than 0 indicated no agreement, 0.00-0.20 slight agreement, 0.21-0.40 fair agreement, 0.41-0.60 moderate agreement, 0.61-0.80 substantial agreement and 0.81-1.00 as an almost perfect agreement (Landis & Koch 1977). Diagnostic test statistics were calculated where amber and red were combined as one discrete outcome. Sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios were calculated.
Ethical considerations
Learners were recruited after permission for the study had been obtained from the provincial Department of Basic Education. The Health Sciences Research Ethics Committee (HSREC; reference number UFS-HSD2017/1363) at the University of the Free State provided ethical approval to conduct this study. The principal of each school, teachers of the participating learners and the parents or legal guardians of the learners provided consent for the children to participate in the study by completing an informed consent form. The learners provided assent. The information letters and consent forms were provided in the languages most commonly spoken in the region, namely English and Sesotho. The information letters and explanation to the participants stipulated that participation was not compulsory and should a participant wish to withdraw, they were allowed to do so at any time during the study. The learners and teachers were treated according to the ethics guidelines of the Faculty of Health Sciences, University of the Free State. Data collection took place during the second term of the school year. The principal investigator stored all the data sheets in a locked safety cabinet and the data on the computer were stored by using a protective password.
Results
Table 2 presents the frequency distribution of the total sample in terms of gender and age. Two hundred (N = 200) Grade 1 learners between the age of 6 and 8 years participated in the study, with an equal distribution of boys and girls (n = 101, 50.5%; n = 99, 49.5%, respectively). The median age was 6.7 years, ranging between 6.0 and 8.1 years.
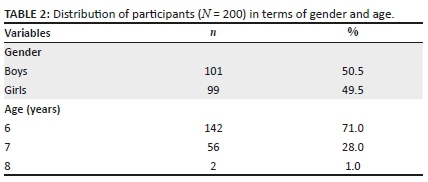
Table 3 shows the number of learners identified with and without possible DCD as determined by the movement specialists using the MABC-2 performance test and the teachers completing the MABC-2 checklist. In order to categorise the learners into a possible DCD group, the cut-off scores of the amber and red zones were combined. Therefore, the non-DCD group comprised learners with a percentile score of above the 15th percentile (>15), and the possible DCD group are learners with a percentile score of lower or equal to the 15th percentile (≤ 15) for the MABC-2 performance test. In addition, the checklist's non-DCD group represented a percentile score of below 85, and the possible DCD group's score was at or above the 85th percentile. The movement specialist identified more learners (n = 180; 90.0%) in the non-DCD group than the teachers, who identified 108 (54.0%) learners. The teachers mis-identified learners with possible DCD by identifying 92 (46.0%) learners with possible DCD. However, only 20 (10.0%) learners were identified by the movement specialist with possible DCD.
Table 4 shows the inter-rater agreement between the MABC-2 performance test and the MABC-2 checklist with cut-off scores for each category of the MABC-2, namely definite motor skill difficulties (≤ 5 percentile), moderate motor skill difficulties (6th-15th percentile) and no motor skill difficulties (> 15th percentile). A slight agreement was found (k = 0.1362). Of the seven learners identified by the movement specialist with moderate motor difficulties, none were identified by the teachers using the checklist. Eleven of the 13 learners identified with severe motor difficulties were similarly identified by the teachers by means of the MABC-2 checklist.
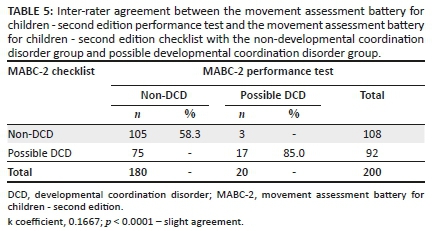
Table 5 illustrates the agreement with cut-off scores divided into a non-DCD group (>15th percentile) and possible DCD group (≤ 15th percentile). The k coefficient used to determine the convergent validity of the MABC-2 performance test and the MABC-2 checklist indicated a slight agreement, with k = 0.1667. The low agreement between the two tests demonstrated that the movement specialist and the teacher did not identify the same learners with and without motor difficulties.
In Table 6, the MABC-2 performance test and MABC-2 checklist are presented for sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio and the negative likelihood ratio. The predicted standards when using the 15th percentile as cut-off scores with the MABC-2 are 80% sensitivity and 90% specificity (APA 1985). In this study, the sensitivity was 85%, indicating a high ability of the class teachers to correctly identify learners in Grade 1 with possible DCD. The specificity was 58%, indicating that the teachers found it difficult to identify the absence of motor skill difficulties when using the MABC-2 checklist.
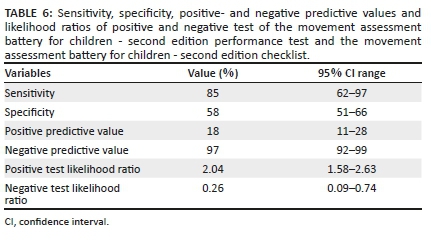
The positive predictive value indicated the probability that the learners who were identified with possible DCD truly had possible DCD. The probability of possible DCD in this study was 18%, indicating a low probability that the learners who were identified with possible DCD truly had possible DCD. The negative predictive value is the probability that the learners in the non-DCD category certainly did not have possible DCD. The probability of non-DCD was 97%, indicating that these learners certainly did not have possible DCD.
Discussion
This study aimed to determine whether class teachers of Grade 1 learners living in low socio-economic environments were able to identify these learners with possible DCD by completing the MABC-2 checklist. The convergent validity (agreement of the MABC-2 performance test and checklist) was determined in order to establish the ability of the teachers.
A sensitivity of 85% was found in this study, showing that of the 20 learners identified with possible DCD with the MABC-2 performance test, 17 learners were also identified by means of the teacher-completed MABC-2 checklist. These results demonstrated a high ability of the teachers to identify learners with possible DCD and were correlated with the findings of Schoemaker et al. (2003). Schoemaker et al. (2003) reported that a study in the Netherlands on 184 children 6-11 years of age found a sensitivity of 85% when using the original MABC performance test conducted by physiotherapists and the checklist completed by classroom teachers.
Our findings on sensitivity were contrary to other research on the original MABC that found lower sensitivities. A sensitivity of 44% on 98 children (mean age 107.4 months) was reported in a study when the MABC performance test was executed by occupational therapists and the checklists completed by the physical education teachers (Green et al. 2005). Ellinoudis et al. (2009) established a sensitivity of 27.1% in a study on 330 Greek children when evaluated with the original MABC checklist completed by the physical education teachers and the performance test by professionals trained in the assessment of children. Junaid et al. (2000) reported an even lower sensitivity of 14.3% in a study on 103 Canadian children (mean age 8 years) when evaluated with the MABC performance test by physical therapists and the checklist completed by the teachers. Junaid et al. (2000) further explained that of the 14 learners identified with DCD by means of the original MABC performance test, only two learners were identified by using the MABC checklist. Ellinoudis et al. (2009), as well as Piek and Edwards (1997), concluded that teachers had a low ability to identify motor skill difficulties in learners, when using the original MABC checklist and were therefore unable to identify learners with possible DCD. The opinion of Ellinoudis et al. (2009) and Piek and Edwards (1997) was in contrast with the findings of the current study, where the indication of teachers to have the ability to identify learners with possible DCD, when using the second edition MABC-2 checklist, was high (85%).
Schoemaker et al. (2012) put emphasis on the contradicting findings of this study when using the MABC-2, and reported a sensitivity of 41% in a study on 383 Belgium children 5-8 years of age, where teachers completed the MABC-2 checklist and therapists completed the MABC-2 performance test. They further reported that of the 64 learners with possible DCD with the MABC-2 performance test, only 26 (40.6%) were identified by means of the checklist (Schoemaker et al. 2012). Dimitropoulou et al. (2019) recently determined 52.7% sensitivity in a study on 584 Greek children when evaluated with the MABC-2 checklist completed by teachers. Comparing the research findings of Dimitropoulou et al. (2019) with the current study, the greater ability of the teachers to identify possible DCD by means of the MABC-2 checklist (85.0%) was evident. In another study conducted in the Free State Province in South Africa by De Milander et al. (2016), a sensitivity of 46.5% was reported when the checklist was completed by teachers. Their study included 323 children (5-8 years), where Kinderkineticists conducted the performance test.
In this study, we determined a specificity of 58%, which indicated the following: of the 180 learners identified by the MABC-2 performance test without DCD, only 105 were identified without possible DCD with the MABC-2 checklist completed by the teachers. This finding demonstrated that the teachers had a low ability to identify learners without DCD. The results are supported by Schoemaker et al. (2003). Their findings reported a specificity of 66% with the original MABC performance test and checklist. In addition, several authors reported higher specificities when using the original MABC and the MABC-2 performance test and checklist, ranging from 70% to 88% (De Milander et al. 2016; Dimitropoulou et al. 2019; Green et al. 2005; Shoemaker et al. 2012). Their findings suggested that teachers and/or parents who completed the checklist had a high ability to identify individuals without possible DCD (De Milander et al. 2016; Dimitropoulou et al. 2019; Green et al. 2005; Shoemaker et al. 2012), and were in contrast with the findings of the current study. Junaid et al. (2000) found an even higher specificity when using the original MABC. They reported that out of the 89 learners identified without DCD with the performance test, 87 (97.8%) were also evaluated without DCD with the checklist (Junaid et al. 2000). Their results contradict the current study's findings. One of the reasons for the low specificity in this study might be that class teachers have not been formally trained to identify and observe motor skills, and might therefore observe more children with motor difficulties instead of realising that it was part of their normal motor development. Furthermore, it would be more ideal to make use of physical education teachers with more in-depth knowledge of motor skills to determine if motor skills are on par or absent.
The convergent validity of this study between the MABC-2 performance test and the MABC-2 checklist completed by the class teachers was indicated by a k coefficient of 0.17. The convergent validity, therefore, demonstrated a slight agreement and the results correlated well with research conducted in a high socio-economic environment in Bloemfontein, Free State Province, with a k coefficient of 0.11 (De Milander et al. 2016). Similar results were reported by Ellinoudis et al. (2009) and Green et al. (2005) when using the original MABC performance test and checklist, with a k coefficient of 0.14 (14%). The agreement found in the current study was lower than that by Dimitropoulou et al. (2019) and Schoemaker et al. (2012) with the MABC-2 performance test and checklist, who reported an agreement of 0.28. In addition, more moderate agreements were found when using the original MABC, with k coefficients of 0.44 (Schoemaker et al. 2003) and 0.51 (Junaid et al. 2000), respectively.
Schoemaker et al. (2003) were of the opinion that both the MABC performance test and the MABC checklist should be used, and if the learner failed both the evaluations, they could be identified with possible DCD. The authors further mentioned that the MABC checklist should identify all children with possible DCD, after which the MABC performance test should be conducted to confirm the diagnosis (Schoemaker et al. 2003). This argument was later supported by Ellinoudis et al. (2009), putting emphasis on the statement that if the MABC checklist is used, the MABC performance test must further be conducted to confirm the diagnosis. Considering the results of the current study, the views of Ellinoudis et al. (2009) and Schoemaker et al. (2003) could be seen to be meaningful to determine possible DCD, and the problem of incorrectly identifying learners with possible DCD might then be eliminated. The current study, therefore, supports the view that the MABC-2 checklist should not be used independently.
A possible reason for the low agreement between the MABC-2 performance test and the MABC-2 checklist could be that the class teachers indicated that they do not present structured physical education classes to the learners because of unavailable space or limited time. Teachers indicated to the principal investigator that they are not qualified, physical educators. They therefore did not have the experience of observing learners performing movement activities outside the classroom. Piek and Edwards (1997) and Schoemaker et al. (2008) supported this point of view, as they were of the opinion that class teachers did not experience children in a changing environment and were not part of physical education classes, which could cause a disadvantage on how to evaluate motor skills in children. Another reason could be that teachers do not have sufficient knowledge about DCD (Dimitropoulou et al. 2019) and this could have an effect on how they evaluate motor behaviours and motor proficiency executions. Netelenbos (2005) further explained that a screening tool specifically observes the motor skill abilities of a child in daily living activities, whereas a motor test conducted by a movement specialist evaluates underlying motor skill abilities, and could therefore be an explanation for the low agreement observed in the current study. Further reasons might be the socio-economic environment. The learners were from a low socio-economic environment attending quintile one to three schools. The MABC-2 checklist might therefore not be suitable for this population because of the lack of apparatus, opportunities and facilities. Although the MABC-2 checklist completed by teachers of Grade 1 learners living in a low-socioeconomic environment could be used to identify learners with possible DCD, it should not be the only assessment tool used and teachers might wrongfully identify learners with possible DCD, who might not have this problem.
Conclusion
We found a slight agreement (0.17) of convergent validity between the MABC-2 performance test and the MABC-2 checklist completed by teachers. Although we showed that the teachers were able to use the MABC-2 checklist to identify possible DCD in learners (sensitivity), the study further established that the ability of the teachers to accurately identify learners without possible DCD (specificity) was low. Teachers have therefore identified learners who do not have possible DCD, confirmed by the movement specialist, as having possible DCD when using the MABC-2 checklist. Based on the results and findings, it would therefore not be recommended to only use the MABC-2 checklist by teachers to identify possible DCD. Furthermore, other assessment tools should be considered.
The prevalence of possible DCD as determined by the MABC-2 performance test has been reported to be high in low socio-economic environments. Some children living in these low socio-economic environments in South Africa have motor development delays and limited opportunity to develop motor skills (Kahts, Du Randt & Venter 2017; Pienaar & Kemp 2014). It was further evident that teachers could not identify learners living in low socio-economic environments with possible DCD, and it is therefore important to raise awareness of limited or unfitting screening tools available for teachers in a low socio-economic environment to identify learners with possible DCD. Venter, Pienaar and Coetzee (2015) emphasised the importance of early screenings for motor difficulties to identify possible DCD. They further explained that the results of a child's motor skills are important for teachers, day care personnel and other professionals who work with children with motor skill problems (Venter et al. 2015). According to Pienaar and Kemp (2014), more strategies should be developed to create more awareness of motor skill problems. If an assessment is not provided, early intervention cannot take place.
This study has the potential to raise awareness of possible DCD and to motivate the public school services to raise awareness of children having limited access and experience of participation in motor activities, as well as the lack of assessment services for DCD. The motor difficulties experienced by these learners highlight the importance of early identification to prevent further problems and provide adequate interventions or support. It is essential for the Department of Basic Education to put more emphasis on the importance of screening and execution of motor skills, as motor development plays a very important part in the complete development of a child.
Limitations
The sample size of this research study was small and further research on a larger sample is recommended. Furthermore, the study was conducted in only one province and one district and should be expanded to other provinces for a broader view and improved results on the national prevalence of possible DCD amongst Grade 1 learners. A larger sample group of different quintile schools and teachers in other parts of South Africa within low socio-economic and high socio-economic communities should be investigated. The MABC-2 checklist is based on a UK population, which should be taken into account when evaluating South African children for possible motor skill deficits. Despite the limitations, awareness of evaluating teachers' role in identifying possible DCD, especially in low socio-economic environments, has been created. The research can motivate more in-depth studies to assist children with low motor skill abilities earlier. Suppose all the children wrongfully identified with possible DCD by the teachers, they should be referred for further assessment by therapists. In that case, an overload of the therapists' capacity can occur or be costly for the parents from these low socio-economic environments. Therefore more research strategies are required for assessment options.
Acknowledgements
The authors would like to acknowledge Dr Daleen Struwig, medical writer/editor, Faculty of Health Science, University of the Free State, for technical and editorial preparation of the manuscript. The authors also acknowledge the 2018 Kinderkinetics Honours students at the University of the Free State for assistance with data collection.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this research article.
Authors' contributions
A.M.d.P. was the principal researcher reporting on her PhD study and the primary author of the article. M.d.M. was the supervisor of the study and contributed to the article by guiding structure and content. F.F.C. was the co-supervisor of the study and guided writing of the manuscript. M.N. was the biostatistician involved in the study and gave input during the study's planning and analysis. All the authors approved the final version of the article.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
Data are available from the corresponding author, A.M.d.P., upon reasonable request.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
Aertssen, W., Bonney, E., Ferguson, G. & Smits-Engelsman, B., 2018, 'Subtyping children with developmental coordination disorder based on physical fitness outcomes', Human Movement Science 60, 87-97. https://doi.org/10.1016/j.humov.2018.05.012 [ Links ]
Alesi, M., Pecoraro, D. & Pepi, A., 2019, 'Executive functions in kindergarten children at risk for developmental coordination disorder', European Journal of Special Needs Education 34(3), 285-296. https://doi.org/10.1080/08856257.2018.1468635 [ Links ]
Amador-Ruiz, S., Gutierrez, D., Martínez-Vizcaíno, V., Gulíaz-González, R., Pardo-Guijarro, M.J. & Sánchez-López, M., 2018, 'Motor competence levels and prevalence of developmental coordination disorder in Spanish children: The Movi-Kids study', Journal of School Health 88(7), 538-546. https://doi.org/10.1111/josh.12639 [ Links ]
American Psychological Association (APA), 1985, Standards for educational and psychological tests, American Psychiatric Association, Washington, DC.
American Psychiatric Association (APA), 2013, Diagnostic and statistical manual of mental disorders, 5th edn., American Psychiatric Association, Washington, DC.
Asonitou, K., Koutsouki, D., Kourtessis, T. & Charitou, S., 2012, 'Motor and cognitive performance differences between children with and without developmental coordination disorder (DCD)', Research in Developmental Disabilities 33(4), 996-1005. https://doi.org/10.1016/j.ridd.2012.01.008 [ Links ]
Asunta, P., Viholainen, H., Ahonen, T., Cantell, M., Westerholm, J., Shoemaker, M.M. et al., 2017, 'Reliability and validity of the Finnish version of the motor observation questionnaire for teacher', Human Movement Science 53, 63-71. https://doi.org/10.1016/j.humov.2016.12.006 [ Links ]
Barnett, A.L., 2008, 'Motor assessment in developmental coordination disorder: From identification to intervention', International Journal of Disability, Development and Education 55(2), 113-129. https://doi.org/10.1080/10349120802033436 [ Links ]
Barnett, L.M., Lai, S.K., Veldman, L.C., Hardy, L.L., Cliff, D.P., Morgan, P.J. et al., 2016, 'Correlates of gross motor competence in children and adolescents: A systematic review and meta-analysis', Sports Medicine 46(11), 1663-1688. http://doi.org/10.1007/s40279-016-0495-z [ Links ]
Batey, C.A., Missiuna, C.A., Timmons, B.W., Hay, J.A., Faught, B.E. & Cairney, J., 2014, 'Self efficacy toward physical activity and the physical activity behaviour of children with and without developmental coordination disorder', Human Movement Science 36, 258-271. https://doi.org/10.1016/j.humov.2013.10.003 [ Links ]
Blank, R., Barnett, A.L., Cairney, J., Green, D., Kirby, A., Polatajko, H. et al., 2019, 'International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder', Developmental Medicine and Child Neurology 61(3), 242-285. https://doi.org/10.1111/dmcn.14132 [ Links ]
Blank, R., Smits-Engelsman, B., Polatajko, H. & Wilson, P., 2012, 'European academy for childhood disability (EACD): Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (long version)', Developmental Medicine and Child Neurology 54(1), 54-93. https://doi.org/10.1111/j.1469-8749.2011.04171.x [ Links ]
Brown, T. & Lalor, A., 2009, 'The movement assessment battery for children second edition (MABC-2): A review and critique', Physical and Occupational Therapy in Pediatrics 29(1), 86-103. https://doi.org/10.1080/01942630802574908 [ Links ]
Cairney, J., Veldhuizen, S., King-Dowling, S., Faught, B.E. & Hay, J, 2017, 'Tracking cardiorespiratory fitness and physical activity in children with and without motor coordination problems', Journal of Science and Medicine in Sport 20, 380-385. https://doi.org/10.1016/j.jsams.2016.08.025 [ Links ]
De Milander, M., Coetzee, F.F. & Venter, A., 2016, 'Teachers' ability to identify children with developmental coordination disorder', African Journal for Physical Activity and Health Sciences 22(4:1), 990-1005. [ Links ]
De Milander, M., Du Plessis, A.M. & Coetzee, F.F., 2019, 'Identification of developmental coordination disorder in grade 1 learners: A screening tool for parents and teacher', South African Journal for Research in Sport, Physical Education and Recreation 41(2), 45-49. [ Links ]
De Waal, E., Pienaar, A.E. & Coetzee, D., 2018, 'Gender differences in academic achievement of children with developmental coordination disorder', South African Journal of Childhood Education 8(1), a515. https://doi.org/10.4102/sajce.v8i1.515 [ Links ]
Delgado-Lobete, L., Santos-Del-Riego, S., Pértega-Díaz, S. & Montes-Montes, R., 2019, 'Prevalence of suspected developmental coordination disorder and associated factors in Spanish classrooms', Research in Developmental Disabilities 86, 31-40. https://doi.org/10.1016/j.ridd.2019.01.004 [ Links ]
Dimitropoulou, D., Evaggelinou, C., Kourtessis, T., Mouratidou, K., Tsigili, N. & Ellinoudis, T., 2019, 'Concurrent validity of the movement assessment battery for children checklist-2: A Greek population-based study', European Psychomotricity Journal 11(1), 19-38. [ Links ]
Edwards, J., Berube, M., Erlandson, K., Haug, S., Johnstone, H., Meagher, M. et al., 2011, 'Developmental coordination disorder in school-aged children born very preterm and/or at very low birth weight: A systematic review', Journal of Developmental and Behavioural Pediatrics 32(9), 678-687. https://doi.org/10.1097/DBP.0b013e31822a396a [ Links ]
Ellinoudis, T., Kyparisis, M., Gitsas, K. & Kourtesis, T., 2009, 'Identification of children age 7-12 with developmental coordination disorder by physical education teachers using the test "movement assessment battery for children"', Hellenic Journal of Physical Education & Sport Science 29(3), 288-306. [ Links ]
Etikan, I. & Bala, K., 2017, 'Sampling and sampling methods', Biometrics & Biostatistics International Journal 5(6), 215-217. https://doi.org/10.15406/bbij.2017.05.00149 [ Links ]
Faught, B.E., Cairney, J., Hay, J., Veldhuizen, S., Missiuna, C. & Spironello, C.A., 2008, 'Screening for mortor coordination challenges in learners using teacher ratings of physical ability and activity', Human Movement Science 27(2), 177-189. https://doi.org/10.1016/j.humov.2008.02.001 [ Links ]
Ferguson, G.D., Naidoo, N. & Smits-Engelsman, B.C.M., 2015, 'Health promotion in a low-income primary school: Children with and without DCD benefit, but differently', Physical and Occupational Therapy in Pediatrics 35(2), 147-162. https://doi.org/10.3109/01942638.2015.1009230 [ Links ]
Gallahue, D.L. & Ozmun, J.C., 2006, Understanding motor development, 6th edn., McGraw-Hill, New York, NY.
Geuze, R. & Börger, H., 1993, 'Children who are clumsy: Five years later', Adapted Physical Activity Quarterly 10(1), 10-21. https://doi.org/10.1123/apaq.10.1.10 [ Links ]
Graven, H., 2013, 'Poverty, inequality and mathematics performance: The case of South Africa's post-apartheid context', ZDM Mathematics Education 46(7), 1039-1049. https://doi.org/10.1007/s11858-013-0566-7 [ Links ]
Green, D., Bishop, T., Wilson, B.N., Craword, S., Hooper, R., Kaplan, B. et al., 2005, 'Is questionnaire-based screening part of the solution to waiting lists for learners with developmental coordination disorder?', British Journal of Occupational Therapy 68(1), 2-10. https://doi.org/10.1177/030802260506800102 [ Links ]
Hall, K. & Giese, S., 2008, 'Addressing quality through school fees and school funding', in S. Pendlebury, L. Lake & C. Smith (eds.), South African child gauge 2008/2009, pp. 35-40, Children's Institute, UCT, Cape Town.
Hardy, L.L., Reinten-Reynolds, T., Espinel, P., Zask, A. & Okely, A.D., 2012, 'Prevalence and correlates of low fundamental movement skill competency in children', Pediatrics 130(2), e390-e398. https://doi.org/10.1542/peds.2012-0345 [ Links ]
Henderson, S.E., Sugden, D.A. & Barnett, A.L., 2007, Movement assessment battery for children-2 (MABC-2), 2nd edn., The Psychological Corporation/Harcourt Brace and Company Publishers, London.
Isaacs-Martin, W., 2015, 'Issues of race, ethnicity, socio-economic position and spatial acknowledgement in South Africa: How spatial access and expression still perpetuate notions of difference, separation and uncertainty amongst the South African coloured population', International Journal of African Renaissance Studies 10(1), 120-140. https://doi.org/10.1080/18186874.2015.1050219 [ Links ]
Junaid, K., Harris, S.R., Fulmer, A. & Carswell, A., 2000, 'Teachers' use of the MABC checklist to identify children with motor difficulties', Pediatric Physical Therapy 12, 158-163. https://doi.org/10.1097/00001577-200001240-00003 [ Links ]
Kadesjö, B. & Gillberg, C., 1998, 'Attention deficits and clumsiness in Swedish 7-year-old children', Developmental Medicine and Child Neurology 40(12), 796-804. https://doi.org/10.1111/j.1469-8749.1998.tb12356.x [ Links ]
Kahts, S.A., Du Randt, R. & Venter, D.J.L., 2017, 'Fundamental movement skill proficiency of South African girls from a lower socio-economic community', South African Journal for Research in Sport, Physical Education and Recreation 39(3), 41-56. [ Links ]
Karras, H.C., Morin, D.N., Gill, K., Izadi-Najafabadi, S. & Zwicker, J.G., 2019, 'Health-related quality of life of children with developmental coordination disorder', Research in Developmental Disabilities 84, 85-95. https://doi.org/10.1016/j.ridd.2018.05.012 [ Links ]
Landis, J.R. & Koch, G.G., 1977, 'The measurement of observer agreement for categorical data', Biometrics 33(1), 159-174. https://doi.org/10.2307/2529310 [ Links ]
Larkin, D. & Rose, E., 2005, 'Assessment of developmental coordination disorder', in D.A. Sugden & M.E. Chambers (eds.), Children with developmental coordination disorder, pp. 135-154, Whurr Publishers Ltd., London.
Lingam, R., Hunt, L., Golding, J., Jongmans, M. & Edmond, A., 2009, 'Prevalence of developmental coordination disorder using the DSM-IV at 7 years of age: A UK population based study', Pediatrics 123(4), e693-e700. https://doi.org/10.1542/peds.2008-1770 [ Links ]
Lombard, I. & Pienaar, A.E., 2003, 'Reliability of class teachers using the MABC checklist for DCD screening', Journal of Human Movement Studies 45(2), 163-186. [ Links ]
Missiuna, C., Cairney, J., Pollock, N., Campbell, W., Russell, D.J., Macdonald, K. et al., 2014, 'Psychological distress in children with developmental coordination disorder and attention-deficit hyperactivity disorder', Research in Developmental Disabilities 35(5), 1198-1207. https://doi.org/10.1016/j.ridd.2014.01.007 [ Links ]
Missiuna, C., Cairney, J., Pollock, N., Russell, D., Macdonald, K., Cousins, M. et al., 2011, 'A staged approach for identifying children with developmental coordination disorder form the population', Research in Developmental Disabilities 32(2), 549-559. https://doi.org/10.1016/j.ridd.2010.12.025 [ Links ]
Missiuna, C., Gaines, B., Souchie, H. & McLean, J., 2006, 'Parental questions about developmental coordination disorder: A synopsis of current evidence', Paediatric Child Health 11(8), 507-512. https://doi.org/10.1093/pch/11.8.507 [ Links ]
Narsai, P., Taylor, M., Jinabhai, C. & Stevens, F., 2013, 'Variations in housing satisfaction and health status in four lower socio-economic housing typologies in the eThekwini Municipality in KwaZulu-Natal', Development Southern Africa 30(3), 367-385. https://doi.org/10.1080/0376835X.2013.817304 [ Links ]
Ndebele, M., 2015, 'Socio-economic factors affecting parents' involvement in homework: Practices and perceptions from eight Johannesburg public primary schools', Perspectives in Education 33(3), 72-91. [ Links ]
Netelenbos, B., 2005, 'Teachers's ratings of gross motor ability suffer from low concurrent ability', Human Movement Science 24, 116-137. https://doi.org/10.1016/j.humov.2005.02.001 [ Links ]
Ogbonnaya, U.I. & Awuah, F.K., 2019, 'Quintile ranking of schools in South Africa and learners' achievement in probability', Statistics Education Research Journal 18(1), 106-119. http://www.stat.auckland.ac.nz/serj [ Links ]
Pappin, M., Marais, L., Sharp, C., Lenka, M., Cloete, J., Skinner, D. et al., 2015, 'Socio-economic status and socio-emotional health of orphans in South Africa', Journal of Community Health 40(1), 92-102. https://doi.org/10.1007/s10900-014-9903-1 [ Links ]
Peters, J.M. & Henderson, S.E., 2008, 'Understanding developmental coordination disorder and its impact on families: The contribution of single case studies', International Journal of Disability, Development and Education 55(2), 97-111. https://doi.org/10.1080/10349120802033410 [ Links ]
Philips, E., Chirico, D., Cairney, J., Hay, J., Faught, B.E. & O'Leary, D.D., 2016, 'Arterial stiffness in children with and without probable developmental coordination disorder', Research in Developmental Disabilities 59, 138-146. https://doi.org/10.1016/j.ridd.2016.07.011 [ Links ]
Piek, J.P. & Edwards, K., 1997, 'The identification of children with developmental coordination disorder by class and physical education teachers', British Journal of Educational Psychology 67(Pt 1), 55-67. https://doi.org/10.1111/j.2044-8279.1997.tb01227.x [ Links ]
Pienaar, A.E., 2004, 'Developmental coordination disorder in an ethno-racially diverse African nation: Should norms or the MABC be adjusted?', Journal of Human Movement Studies 47, 75-92. [ Links ]
Pienaar, A.E., Barhorst, R. & Twisk, J.W.R., 2013, 'Relationships between academic performance, SES school type and perceptual-motor skills in first grade South African learners: NW-CHILD study', Child: Care, Health and Development 40(3), 370-378. https://doi.org/10.1111/cch.12059 [ Links ]
Pienaar, A.E. & Kemp, C., 2014, 'Motor proficiency profile of grade 1 learners in the North West Province of South Africa: NW-child study', South African Journal for Research in Sport, Physical Education and Recreation 36(1), 167-182. [ Links ]
Pienaar, R. & McKay, T.M., 2014, 'Mapping socio-economic status, geographical location and matriculation pass rates in Gauteng, South Africa', Perspectives in Education 32(1), 101-119. [ Links ]
Pratt, M.L. & Hill, E.L., 2011, 'Anxiety profiles in children with and without developmental coordination disorder', Research in Developmental Disabilities 32(4), 1253-1259. https://doi.org/10.1016/j.ridd.2011.02.006 [ Links ]
Rihtman, T., Wilson, B.N. & Parush, S., 2011, 'Developmental of the little developmental coordination disorder questionnaire for preschoolers and preliminary evidence of its psychometric properties in Israel', Research in Developmental Disabilities 32(4), 1378-1387. https://doi.org/10.1016/j.ridd.2010.12.040 [ Links ]
Schoemaker, M.M., Flapper, B.C.T., Reinders-Messelink, H.A. & De Kloet, A., 2008, 'Validity of the motor observation questionnaire for teachers as a screening instrument for children at risk for developmental coordination disorder', Human Movement Science 27(2), 190-199. https://doi.org/10.1016/j.humov.2008.02.003 [ Links ]
Schoemaker, M.M., Flapper, B.C.T., Verheij, N.P., Wilson, B.N., Reinders-Messelink, H.A. & De Kloet, A., 2006, 'Evaluation of the developmental coordination disorder questionnaire as a screening instrument', Developmental Medicine and Child Neurology 48(8), 668-673. https://doi.org/10.1017/S001216220600140X [ Links ]
Schoemaker, M.M., Niemeijer, A., Flapper, B.C.T. & Smits-Engelsman, B.C.M., 2012, 'Validity and reliability of the movement assessment battery for children-2 checklist for children with and without motor impairments', Developmental Medicine and Child Neorology 54(4), 368-375. https://doi.org/10.1111/j.1469-8749.2012.04226.x [ Links ]
Schoemaker, M.M., Smits-Engelsman, B.C. & Jongmans, M.J., 2003, 'Psychometric properties of the movements assessment battery for children-checklist as a screening instrument for children with a developmental coordination disorder', British Journal of Education Psychology 73(3), 425-441. https://doi.org/10.1348/000709903322275911 [ Links ]
Senekal, M., Seme, Z., De Villiers, A. & Steyn, N.P., 2015, 'Health status of primary school educators in low socio economic areas in South Africa', BMC Public Health 15, 186. https://doi.org/10.1186/s12889-015-1531-x [ Links ]
Smits-Engelsman, C.M., Jelsma, D. & Ferguson, G.D., 2017, 'The effect of exergames on functional strength, anaerobic fitness, balance and agility in children with and without motor coordination difficulties living in low-income communities', Human Movement Science 55, 327-337. https://doi.org/10.1016/j.humov.2016.07.006 [ Links ]
Sylvestre, A., Nadeau, L., Charron, L., Larose, N. & Lepage, C., 2013, 'Social participation by children with developmental coordination disorder compared to their peers', Disability and Rehabilitation 35, 1814-1820. https://doi.org/10.3109/09638288.2012.756943 [ Links ]
Uys, L. & Pienaar, A.E., 2010, 'Die fisieke en motoriese ontwikkeling van voorskoolse kinders vanuit verskillende sosio-ekonomiese onstandighede, Thusano-studie', South African Journal for Research in Sport, Physical Education and Recreation 32(2), 131-144. [ Links ]
Valentini, N.C., Clark, J.E. & Whitall, J., 2015, 'Developmental coordination disorder in socially disadvantaged Brazilian children', Child Care, Health and Development 41(6), 970-979. https://doi.org/10.1111/cch.12219 [ Links ]
Van Dellen, T., Vaessen, W. & Schoemaker, M.M., 1990, 'Clumsiness: Definition and selection of subjects', in A.F. Kalverboer (ed.), Developmental biopsychology, pp. 135-152, The University of Michigan Press, Ann Arbor, MI.
Van der Walt, J., Plastow, N.A. & Unger, M., 2020, 'Prevalence of motor skill impairment among Grade R learners in the West Coast District of South Africa', South African Journal of Education 40(1), Art. #1667. https://doi.org/10.15700/saje.v40n1a1667 [ Links ]
Van Waelvelde, H., Peersman, W., Lenoir, M. & Smits-Engelsman, B.C.M., 2007, 'Convergent validity between two motor tests: Movement-ABC and PDMS-2', Adapted Physical Activity Quarterly 24(1), 59-69. https://doi.org/10.1123/apaq.24.1.59 [ Links ]
Venter, A., Pienaar, A.E. & Coetzee, D., 2015, 'Extent and nature of motor difficulties based on age ethnicity, gender and socio-economic status in a selected group of three- to five-year-old children', South African Journal for Research in Sport, Physical Education and Recreation 37(3), 169-183. [ Links ]
Visser, J., 2003, 'Developmental coordination disorder: A review of research on subtypes and comorbidities', Human Movement Science 22(4-5), 479-493. https://doi.org/10.1016/j.humov.2003.09.005 [ Links ]
Wilson, B.N., Crawford, S.G., Green, D., Roberts, G., Aylott, A. & Kamplan, B.J., 2009, 'Psychometric properties of the revised developmental coordination disorder questionnaire', Physical and Occupational Therapy in Pediatrics 29(2), 182-202. https://doi.org/10.1080/01942630902784761 [ Links ]
Wuang, Y., Su, J. & Su, C., 2012, 'Reliability and responsiveness of the movement assessment battery for children second edition test in children with developmental coordination disorder', Developmental Medicine and Child Neurology 54(2), 160-165. https://doi.org/10.1111/j.1469-8749.2011.04177.x [ Links ]
Zwicker, J.G., Missiuna, C., Harris, S.R. & Boyd, L.A., 2012, 'Developmental coordination disorder: A review and update', European Journal of Paediatric Neurology 16(6), 573-581. http://doi.org/10.1016/j.ejpn.2012.05.005 [ Links ]
Zwicker, J.G., Suto, M., Harris, S.R., Vlasakova, N. & Missiuna, C., 2018, 'Developmental coordination disorder is more than a motor problem: Children describe the impact of daily struggles on their quality of life', British Journal of Occupational Therapy 81(2), 65-73. https://doi.org/10.1177/0308022617735046 [ Links ]
 Correspondence:
Correspondence:
Aletta du Plessis
20268319@nwu.ac.za
Received: 19 Aug. 2020
Accepted: 14 Dec. 2020
Published: 19 Apr. 2021


{kind=link}
{kind=link}
{kind=link}