










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Childhood Education
On-line version ISSN 2223-7682
Print version ISSN 2223-7674
SAJCE vol.10 n.1 Johannesburg 2020
http://dx.doi.org/10.4102/sajce.v10i1.836
ORIGINAL RESEARCH
Prevalence of possible developmental coordination disorder among Grade 1 learners in low socio-economic environments in Mangaung, South Africa
Alretha Margaretha du PlessisI; Monique de MilanderI; Frederick Francois CoetzeeI; Mariette NelII
IDepartment of Exercise and Sport Sciences, University of the Free State, Bloemfontein, South Africa
IIDepartment of Biostatistics, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Developmental coordination disorder (DCD) affects motor skills and consequently has an impact on the performance in daily living activities of learners with this impairment.
AIM: The aim of this study was to determine the prevalence of possible DCD in Grade 1 (Gr. 1) learners in a low socio-economic environment in Mangaung, South Africa.
SETTING: The study was conducted in the Mangaung Metro, Motheo District, Free State Province. Gr. 1 learners, 6-8 years old (n = 242), from a low socio-economic environment attending Quintile 1-3 schools were randomly selected for assessment.
METHODS: The Movement Assessment Battery for Children-2nd edition (MABC-2) was used to identify learners with possible DCD. Furthermore, results were compared with regard to gender.
RESULTS: Of the 242 learners, 9.9% were identified with possible DCD. With regard to gender, 10.5% of boys and 9.3% of girls showed signs of possible DCD. No significant difference (p = 0.9439) has been found between boys and girls.
CONCLUSION: The prevalence of possible DCD among Gr. 1 learners in this setting was higher than that in previously reported studies in other low and high socio-economic environments of South Africa. Further research is required to establish the full extent of possible DCD within learners living in low socio-economic environments.
Keywords: developmental coordination disorder (DCD); Movement Assessment Battery for Children-2nd edition (MABC-2); motor skills; children; learners; socio-economic environment; prevalence.
Introduction
Developmental coordination disorder (DCD) can be defined as motor performances that are substantially below the expected levels of the child's ability, considering the child's chronological age and previous opportunities for gaining skills (American Psychiatric Association [APA] 2013). Furthermore, DCD is defined as a neuro-motor developmental disorder, which includes a 'significant delay in the acquisition and execution of coordinated motor skills as expected for the child's chronological age and opportunities for learning' (APA 2013; Blank et al. 2012). The definition clearly states that DCD is a motor skill disorder, which influences a child's activities during daily routines, learning performance and coordinated skill development.
The diagnosis of DCD is based on its description in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) (APA 2013). Learners may only be diagnosed with DCD if the learner meets the four diagnostic criteria determined by the APA (APA 2013). The following criteria are used:
-
Achievement and execution of coordinated motor skills are significantly below the expected performance according to the individual's chronological age and measured intelligence.
-
The deficits in criteria A interfere with the individual's activities of daily living, for example, self-care and self-maintenance, including academic performance.
-
The difficulties are not because of a general medical condition (such as cerebral palsy, hemiplegia or muscular dystrophy) and do not meet the criteria for pervasive developmental disorder.
-
If mental retardation is present, the motor difficulties are in excess of those usually associated with it (APA 2013; De Souza 2015).
However, the literature clearly states that the prevalence of DCD will be referred to as possible DCD, suspected DCD or at risk for DCD if all four DSM-5 criteria have not been used (Alesi, Pecoraro & Pepi 2019; Delgado-Lobete et al. 2019; Lingam et al. 2009; Valentini, Clark & Whitall 2015). For this reason, the term possible DCD was used in this study. De Souza (2015) conducted a systematic review regarding the four criteria to diagnose DCD and identified the Movement Assessment Battery for Children-2nd edition (MABC-2) as the most frequently used tool to assess criterion A, the Developmental Coordination Disorder Questionnaire (DCDQ) for criterion B and no specific instrument for criteria C and D. However, according to Blank et al. (2012), the European Academy of Childhood Disability (EACD) recommends that a medical practitioner should rule out criteria C before a diagnosis can be made and criteria D should be kept in mind if mental retardation is present.
The DSM-5 and previous researchers identified DCD in 5% - 6% of school-aged learners worldwide (APA 2013; Cairney & Streiner 2011; Goyen & Lui 2009; Rivard et al. 2014) between 6 and 12 years of age (Barnhart et al. 2003). It can therefore be ranked as one of the most common neuro-motor developmental disorders among school-aged learners (Lingam et al. 2010). The prevalence of DCD is well documented and varies within different countries and according to the diagnostic criteria used to identify this condition (Cardoso, Magalhães & Rezende 2014; De Milander, Coetzee & Venter 2014; Tsiotra et al. 2006; Valentini et al. 2012). In some countries, the incidence of DCD is high. In southern Brazil, 19.9% of learners between 4 and 12 years of age were identified with possible DCD (Valentini et al. 2012). These findings were similar to those in earlier research reporting that 16.6% of learners aged 7-11 years in a high socio-economic environment in Japan had DCD (Miyahara et al. 1998). Tsiotra et al. (2006) reported that in Greece, 19% of learners with a mean age of 11.3 years were identified with possible DCD. On the contrary, a low prevalence of DCD ranging between 0.8% and 4.3% was also reported among 7-8-year-old learners in Brazil (Cardoso et al. 2014) and 0.8% of Indian learners between 6 and 15 years of age (Girish, Raja & Kamath 2016) living in different socio-economic environments.
With regard to previous research in South Africa, De Milander et al. (2014) found a prevalence of 15% of possible DCD among 6-8-year-old learners in Bloemfontein, South Africa. Similar results were reported by Venter, Pienaar and Coetzee (2015), who found that DCD occurred in 11.3% of learners aged 3-5 years in the North West Province, South Africa. However, another study in the North West Province on learners aged 8-10 in different socio-economic environments identified a lower prevalence of possible DCD (6.3%) (Pienaar & Kemp 2014). In addition, a more recent study in the North West Province of South Africa on learners with a mean age of 10.05 years reported that 21.3% of the learners in the sample were identified with DCD. It is, however, important to note that this was a longitudinal study, and data were collected in 2013 (De Waal, Pienaar & Coetzee 2018).
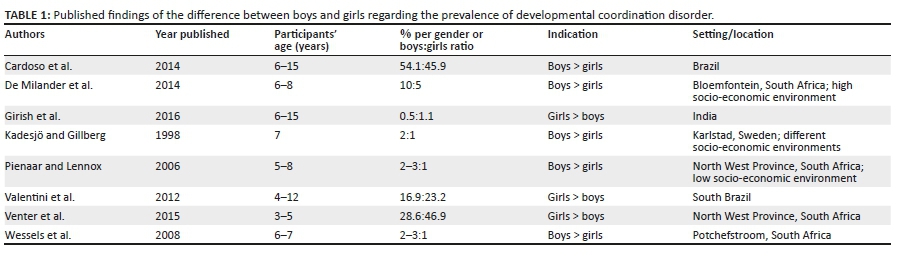
Different results regarding the prevalence of DCD in gender have also been found. According to Lingam et al. (2009) and Pienaar and Lennox (2006), the prevalence of DCD is higher in boys than in girls. The DSM-5 (APA 2013) and Lingam et al. (2009) further suggested boy-girl ratios ranging from 2:1 to 7:1. Table 1 shows the comparison of the prevalence of DCD among boys and girls as reported previously from different studies. It is clear that contradicting results regarding the prevalence of DCD among boys and girls have been found. In addition, limited data on the prevalence of DCD in various socio-economic environments are available (Valentini et al. 2015).
Low socio-economic environments in South Africa are found in townships, inner cities and peri-urban areas (Ndebele 2015). These areas are identified on the basis of poverty, income, education, environmental factors, working conditions and health conditions (Isaacs-Martin 2015; Narsai et al. 2013; Pappin et al. 2015; Pienaar & McKay 2014). According to Senekal et al. (2015), learners and educators living in these environments have fewer opportunities and activities such as sport, playground spaces, equipment and extramural physical activities. Learners living in low socio-economic environments experience motor difficulties and developmental deficits in comparison with learners of the same age from more privileged environments (Pienaar 2004; Pienaar, Labuschagne & Peens 2007). Research conducted in South Africa by Cloete, Pienaar and Coetzee (2006) on 10-12-year-old learners and De Waal et al. (2018) on 10-year-old learners found that learners from low socio-economic environments had a high tendency to have DCD and showed motor skill difficulties. Even though motor skill difficulties are apparent in learners with DCD, no two learners with this disorder are the same and therefore experience different secondary problems.
Secondary problems associated with DCD are physical performance, such as impaired strength and flexibility (Batey et al. 2014; Rihtman, Wilson & Parush 2011; Wuang, Su & Su 2012) and increased obesity (Rihtman et al. 2011; Tsiotra et al. 2006). Learners may show difficulty in academic performance (Cantell, Smyth & Ahonen 2003) and completing activities of daily living (Cairney et al. 2012; Zhu et al. 2010), which include activities such as dressing themselves (home activities), writing and reading (school activities) and play activities, for example, ball skills and balance (Asonitou et al. 2012; Edwards et al. 2011; Schoemaker, Smits-Engelsman & Jongmans 2003). These secondary problems result in emotional and social problems, such as low self-esteem and poor social acceptance (Missiuna et al. 2006). Other problems related to DCD are difficulties with fine motor skills (Zwicker, Missiuna & Boyd 2009), visual impairments (Gomez & Sirigu 2015), attention deficit hyperactivity disorder (ADD/ADHD) and speech or language impairments (Gaines & Missiuna 2007; Missiuna 2003). Because of these difficulties (fine motor, visual and speech impairment), it is important to identify learners with DCD at an early stage.
According to our knowledge, limited research on the prevalence of DCD in different socio-economic environments in South Africa has been conducted. The aim of the study was to determine the prevalence of possible DCD among Grade 1 (Gr. 1) learners living in low socio-economic environments in Mangaung, Motheo District, Free State Province, South Africa, and to establish whether a significant difference between boys and girls could be observed.
Methodology
Study design
Grade 1 learners between 6 and 8 years of age, living in low socio-economic environments in Mangaung, Motheo District, South Africa, were the target population for this study. This research was an empirical study that focussed on a quantitative approach to collect data. The cross-sectional design included one testing procedure to determine the prevalence of possible DCD and differences between boys and girls. The sample for the study was established by obtaining a list of schools in the Motheo District from the Department of Education in the Free State Province.
The sample size was further determined by considering: (1) the duration of administering the measuring instrument MABC-2; (2) the number of trained postgraduate students in Human Movement Science at the University of the Free State in Bloemfontein, specialising in Kinderkinetics (further referred to as movement specialists), with sufficient training and experience to administer the test battery; (3) the school hours; and (4) the budget. A poverty classification from the National Census data was used to determine the classification of schools in different quintiles (Pauw 2005). For example, Quintile 1 schools in each province cater for the poorest 20% of learners, compared with Quintile 4 and 5 schools representing high socio-economic populations (Van Den Berg 2015). From the list of schools in the province, the Motheo District represented approximately 378 schools. There were 33 Quintile 1-3 schools and 3940 Gr. 1 learners in these schools. Ten schools were randomly selected on the criteria that included: representation of Quintile 1-3 public schools and being within a 30 km radius from Bloemfontein, to ensure that the researcher and movement specialists could reach the schools.
Participants
Participants included Gr. 1 learners, 6-8 years of age, who were representative of the population living in low socio-economic environments in Mangaung. These learners were classified into Quintile 1-3 schools that are no-fee schools to make education affordable for poor learners, based on low income, unemployment and parents' level of literacy (Collinridge 2013). Ten schools were selected to take part in the study, of which two schools were Quintile 1 and 2 schools, respectively, and eight were Quintile 3 schools. Using proportional sampling, 400 learners were included in the study. The sample size per school was determined by using random sampling.
Consent forms were sent to the parents of the 400 learners, of which 242 (response rate 60.5%) learners' parents consented to their children's participation in the study. The consent forms included questions regarding the child's health. Parents were asked to indicate according to a tick box if their child suffered from any medical condition or illness and/or severe neurological problem that has been diagnosed by a medical practitioner.
The DSM-5 criteria proposed by the APA (2013) for DCD were partially met concerning criteria A, C and D. The EACD recommended using the MABC-2 as an assessment tool to determine criterion A (Blank et al. 2012) and was therefore used in this study. The EACD further indicated that the Developmental Coordination Disorder Questionnaire'07 (DCDQ'07) is recommended to be used as the assessment tool to determine criterion B (Blank et al. 2012). However, the DCDQ'07 has not been translated, adapted and validated in the home language (Sesotho) of this population in South Africa and could not be used as a valid instrument in this study; therefore, criterion B was excluded. To conduct criteria C and D, the exclusion criteria comprised learners who had serious neurological or intellectual disabilities or conditions such as epilepsy, ADD/ADHD, autism spectrum disorder, visual problems, hearing problems, cancer and/or physical disability.
Using information obtained from the parents, none of the participants met these exclusion criteria. However, the researcher was not able to involve a medical doctor to diagnose general medical conditions (criterion C) in the participating learners in this study. As criteria B and C were not fully met, it could not be alluded that the learner had DCD (Barba et al. 2017), and therefore the learners were referred to as having possible DCD if they fell below the 16th percentile in the MABC-2 performance test. Further exclusion criteria comprised (1) learners falling outside the age range of 6-8 years and (2) parents indicating that they were relocating. The principle researcher (AdP) captured data from the MABC-2 electronically on a Microsoft Excel spreadsheet.
Measuring instrument
Learners were identified with possible DCD using the MABC-2. The MABC-2 is a standardised performance test used to identify learners with motor difficulties. The chosen items of the performance test are aimed to be relevant to all cultural backgrounds. Although previous research has reported differences between learners from different cultures on particular items, no radical changes have been reported (Henderson, Sugden & Barnett 2007). Furthermore, the performance test's psychometric properties have not been established for the South African population, and a revised MABC-2 Performance Test for South Africa is not available. Therefore, no adjustment of the MABC-2 Performance Test was made for this study. Lastly, no assessment tool for South African children exists, and therefore the MABC-2 Performance Test was used. Both the original MABC performance test and the revised MABC-2 have been used successfully in research conducted in South Africa (De Milander, Coetzee & Venter 2016; Wessels, Pienaar & Peens 2008).
To use the MABC-2 for learners of various ages, the test consists of age band 1 (3-6 years), age band 2 (7-10 years) and age band 3 (11-16 years). For the purpose of this study, age bands 1 and 2 were used. The age bands consist of eight age-specific test items, grouped under three components, namely (1) manual dexterity (three test items), (2) aiming and catching (two test items) and (3) balance (three test items) (Henderson et al. 2007). Each test item was clearly demonstrated by a movement specialist, followed by a practice trial and two official test trials. The second trial was administered only if the first trial had not been completed in the correct way, or if the learner had not completed the test within the correct amount of time for his or her age group. Administration of the test battery lasted approximately 30 minutes per learner.
The best trial of each item is used and known as the raw score. The raw score of each item is converted to an item standard score. An item standard score is available for each age group between 3 and 16 years. The standard score is provided every 6 months for learners between 3 and 4 years (3 years 0 months, 3 years 6 months, etc.) and every year for learners between 5 and 16 years (5 years 0 months, 6 years 0 months, etc.). Standard scores and percentiles were further calculated for manual dexterity, aiming and catching as well as balance (Henderson et al. 2007). The standard score demonstrates that the higher the standard score, the better the Gr.1 learner performed, whereas the percentile indicated the percentage that the learner scored less than or equal to the raw score. Furthermore, the percentile was classified according to specific cut-off scores and interpreted through a traffic light system. The green zone (> 15th percentile) indicated performance in a normal range and was classified as no motor difficulty (non-DCD category), the amber zone (6th-15th percentile) indicated that a learner was at risk and should be monitored carefully, with the classification of moderate motor difficulty (risk for DCD category). The red zone (≤ 5th percentile) was an indication of definite motor difficulty (serious DCD category). Possible DCD was identified in the Gr. 1 learners if they fell below the 16th percentile.
The MABC-2 is a valid and reliable test with reliabilities of r = 0.77 for manual dexterity, r = 0.84 for aiming and catching and r = 0.73 for balance when the test was conducted in the United Kingdom on learners between the age of 3-16 years (Henderson et al. 2007). The total test score indicated a reliability of r = 0.80 according to Henderson et al. (2007), and an even higher reliability (r = 0.97) in a more recent study on 6-12-year-old learners in Taiwan (Wuang et al. 2012).
Statistical analysis
Descriptive statistics, namely frequencies and percentages, were calculated for categorical data, and medians and ranges for numerical data. The prevalence of Gr. 1 learners with possible DCD was determined and described by means of 95% confidence interval (CI). The total number of learners identified either with or without DCD, further separated into boys and girls in both groups, was determined. The learners were compared per gender by means of the chi-square test, or when necessary the Fisher's exact test for small samples, for categorical data. A probability level of 0.05 or less (p ≤ 0.05) was accepted to indicate statistical significance.
Ethical consideration
Learners were recruited after approval from the provincial Department of Basic Education and the Health Sciences Research Ethics Committee (UFS-HSD2017/1363) at the University of the Free State was obtained. The headmasters of each school and the parents or legal guardians of the learners completed an informed consent form and gave permission for their child to participate in the study. The learners agreed to take part by completing an assent form.
The learners agreed to take part by completing an assent form. The MABC-2 Performance Test was conducted by 11 trained movement specialists. All movement specialists underwent extensive training that included a minimum of 8 hours preparatory training and at least 6 hours of in-field training. To guarantee consistency within the study, each movement specialist conducted one subtest item. Testing took place during school hours in the second term and was conducted over a period of one month. The parents of the learners were provided with a feedback report regarding their child's motor proficiency results as well as exercises to address the problem, if necessary. The hard copies of each learner's data sheets were stored in a locked safety cabinet by the principal investigator. The electronic data on the computer were stored by using a protective password, which can only be accessed by the principal investigator.
Results
Table 2 displays the frequency distribution of the total sample in terms of gender and age. In total, 242 Gr. 1 learners participated in the study, with the group being composed of an approximately equal number of boys and girls. The majority of the learners were 6 years of age (n = 174; 71.9%). The median age was 6.66 years (range 6.0-8.75 years).

Table 3 displays the results according to the percentile cut-off values of the MABC-2. In total, 90.1% of the learners (n = 218) fell in the group above the 15th percentile, which identified them within the non-DCD group, whereas 9.9% of the learners (n = 24) scored equal or below the 15th percentile, indicating possible DCD. With regard to gender, the percentage of boys with possible DCD was similar to the girls (10.5% and 9.3%, respectively). The 95% CI for the prevalence of DCD is further illustrated in Table 3.
Table 4 shows the distribution of the total group of learners within the three MABC-2 subtests, with 27.7% of learners' scores for manual dexterity indicating possible DCD, opposed to their scores for aiming and catching (5.0% of learners) and balance (8.7% of learners). Of the total group, 72.3% fell in the non-DCD group for manual dexterity, 95.0% for aiming and catching and 91.3% for balance. The results indicated that the learners struggled more with the fine motor component of the MABC-2 performance test.

In Table 5, the differences between boys and girls with possible DCD are shown for the total test score and the individual MABC-2 subtests. No statistically significant differences between the boys' and girls' scores on the total test score (p = 0.9439) and the different subtests were observed (manual dexterity, p = 0.26; aiming and catching, p = 0.16; balance, p = 1.0).
Discussion
The aim of this study was to determine the prevalence of possible DCD in Gr.1 learners between the age of 6 and 8 years, living in low socio-economic environments in the Motheo District of Mangaung, South Africa, and compare the findings of boys and girls participating in the study. To the authors' knowledge, this is the first study to assess the prevalence of possible DCD in the low socio-economic environment in Mangaung, which adds to the limited information on the prevalence of possible DCD in South Africa as a whole, especially with regard to low socio-economic environments. Consequently, comparison of this study with previous research on the prevalence of DCD in low socio-economic environments was restricted.
In this study, 9.9% of Gr. 1 learners were identified with possible DCD, and according to the parents, there was no medical DCD diagnosis before. Research in different countries, such as Israel (Engel-Yeger, Rosenblum & Josman 2010) and Brazil (Valentini et al. 2015), found a high prevalence of possible DCD in low-income families and socio-economic environments. Research conducted by Prinsloo and Pienaar (2003) in the North West Province of South Africa in a low socio-economic environment, supported these findings and indicated a low occurrence of DCD in 7- to 8-year-old learners. In addition, a more recent study in the same province indicated that the prevalence of possible DCD in a low (38.7%) and high (40.9%) socio-economic environment was similar (Venter et al. 2015).
However, when using the 5th percentile as cut-off score for severe DCD with the MABC-2 performance test, it was noted that the high socio-economic environment had a higher incidence (22.7%) than the low socio-economic environment (3.2%) (Venter et al. 2015). Furthermore, another study in the North West Province identified 429 of 645 learners (10-12 years) with possible DCD when using the MABC-2. In addition to Venter et al. (2015), Cloete et al. (2006) reported that the lower the socio-economic environment, the lower the MABC scores. Therefore, it is clear that conflicting results regarding possible DCD in socio-economic environments may be found.
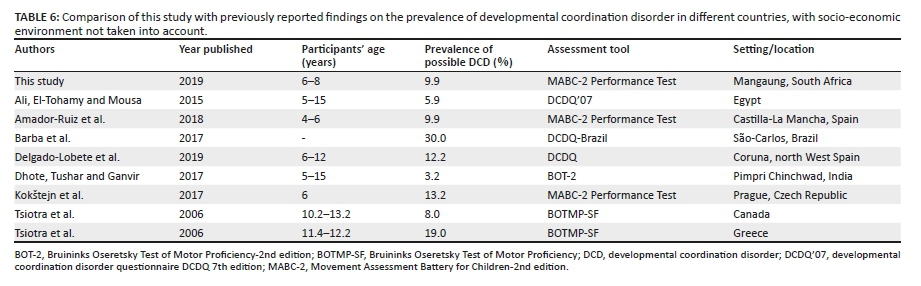
Delgado-Lobete et al. (2019) were of the opinion that the difference in the prevalence rates of DCD depended on the assessment used to identify and/or diagnose DCD. Previous research found results that were similar to those in this study by making use of the DSM-4 and/or DSM-5 and considering only one of the criteria. These findings are summarised in Table 6, and a comparison of the findings of this study with previously reported findings on studies where the socio-economic status of the participants had not been indicated is shown.
Hua et al. (2014) used all four criteria of the DSM-4 with 3-6-year-old learners from China and reported similar results (8.9%) compared with those in this study (9.9%). However, Lingam et al. (2009) indicated a very low prevalence of 1.8% when conducting a large cohort study of learners between 7 and 8 years of age in the United Kingdom. From the literature it is clear that findings vary extensively, even when the full DSM-5 criteria have been applied. It is furthermore important to note the discrepancies in the literature with regard to research conducted in South Africa where no socio-economic environment has been stated. Although De Milander et al. (2014) indicated that 12-15% of 6-8-year-old learners in Bloemfontein could have possible DCD, a very low incidence (1.6%) was reported in Gr.1 learners by Pienaar and Kemp (2014) in the North West Province, South Africa.
With regard to gender, the prevalence of DCD in this study indicated no statistically significant differences (p = 0.9439) between boys (10.5%) and girls (9.3%), showing a boy-to-girl ratio of 1:1. Similar results were reported by Cairney et al. (2005) and Dewey et al. (2002), where no differences between 12- and 14-year-old boys and girls were reported. Comparable findings of a study on Italian learners were reported (Alesi et al. 2019). On the contrary, Delgado-Lobete et al. (2019) indicated that the prevalence of DCD among boys was higher than in girls (16.2% and 8.6%, respectively). Similar to Delgado-Lobete et al. (2019), Gillberg (2003) reported a boy-to-girl ratio of 3-5:1, although Carslaw (2011) found an even higher boy-girl ratio of 9:1. These studies provided evidence of a higher prevalence of DCD in boys than in girls. Research conducted in South Africa showed results that were contrary to this study. Pienaar and Lennox (2006) found a boy-girl ratio of 2-6:1 in a North West Province study, and De Milander et al. (2014) found a boy-girl ratio of 1.6:1 in Bloemfontein. In addition, another study in the North West Province found that mostly girls were identified with possible DCD (Venter et al. 2015).
It has been reported that boys were at greater risk for DCD than girls (Wade & Kazeck 2018), and girls outperformed boys with regard to their overall motor proficiency (Pienaar & Kemp 2014). Amador-Ruiz et al. (2018), however, argued that the occurrence of DCD could be influenced by the tool used to evaluate the learners. Boys tend to be more skilful with ball activities, which increases their aiming and catching performance, whereas girls perform better on fine motor skills (Cardoso & Magalhães 2009). Furthermore, it has been suggested that factors such as cultural differences might have an impact on motor skill abilities (Blank et al. 2012), and also socio-demographic variables (Delgado-Lobete et al. 2019), and should be considered before evaluating a learner for possible DCD.
Disadvantaged educational, social and family circumstances are one of the main reasons for low socio-economic conditions in South Africa and could contribute to a lack of motor skill proficiencies and experience (Isaacs-Martin 2015; Narsai et al. 2013; Pappin et al. 2015; Pienaar & McKay 2014). Tsiotra et al. (2006) concluded that lifestyle differences, such as neighbourhood, environment and culture, should be taken into account when identifying motor skill difficulties or possible DCD. Barba et al. (2017) and Valentini et al. (2015) supported the argument of Tsiotra et al. (2006), confirming that a low socio-economic environment and family status are risk factors for DCD and increase the risk for motor skill difficulties.
Conclusion
The prevalence of DCD among Gr. 1 learners in low socio-economic environments in the Motheo District of the Free State Province is high in comparison with previously reported South African findings. This finding highlights the need to identify learners as early as possible and enhance motor competencies to prevent further motor skill difficulties. Screening tools for the identification of possible DCD, such as the MABC-2 Checklist and the DCDQ'07, should be investigated in low socio-economic environments to increase early identification to assist these learners. Although it has been found that the prevalence of DCD may be higher among boys, the difference in gender ratio has been reported in recent studies to be decreasing. Although socio-economic status might be a reason for a higher prevalence of DCD, limited research has been conducted in South Africa. Given the contradicting prevalence of DCD in this study and other studies in South Africa, it is clear that the prevalence of DCD in South Africa, especially with regard to low socio-economic status, is unknown and not fully identified, warranting further research in this area. Furthermore, it is important to make use of all four criteria of the DSM-5 when identifying DCD and ensure early identification to establish timely intervention. Finally, it is important to evaluate the role that socio-economic situations play on the development of DCD in learners.
This study increased our knowledge of the importance to establish the prevalence of DCD in all provinces of South Africa to ensure a thorough knowledge of the occurrence of this disorder. Furthermore, increased awareness of prevalence of DCD in South Africa can assist in treating this disorder at an earlier stage by means of appropriate interventions. These interventions will contribute to improved motor proficiency levels in learners necessary for activities of daily living in addition to the school environment. Lastly, increasing the awareness of DCD in South Africa, especially in low socio-economic environments, increases our ability to attend to this disorder in future by means of implementing strategies for teachers to improve learners' motor abilities.
Limitations
Although the research was performed on a randomly selected sample, only one province and one district in South Africa were included in the study. Therefore, the findings could not provide a comprehensive reflection of the actual prevalence of possible DCD in all the low socio-economic environments of South Africa. It is therefore recommended that a larger sample group should be used in other parts of low socio-economic environments in South Africa to further investigate the prevalence of possible DCD.
It has to be noted further that DCD studies within various socio-economic environments are limited, and therefore, the results of this study could not be used to make comparisons or evaluate differences. Furthermore, it should be kept in mind that the daily living activities of the learners in this study could not be established and was therefore a limitation. It is probable that several learners with possible DCD in this study might have a functionality challenge at home, but because of the language challenge parents were not able to complete a standardised questionnaire such as the DCDQ'07 and the MABC-2 checklist.
Lastly, criteria C and D of the DSM-5 were assessed by using feedback from parents and did not follow the recommendations of the EACD by making use of a medical doctor to ensure that physical and neurological disorders were not present, as well as a psychological evaluation to confirm that cognitive and intellectual problems were absent. Although limitations were recognised in the present study, the opportunity was created to evaluate more learners and establish the extent of DCD in learners living in low socio-economic environments.
Acknowledgements
The authors thank Dr Daleen Struwig, medical writer/editor, Faculty of Health Science, University of the Free State, for technical and editorial preparation of the manuscript and the 2018 Kinderkinetics Honours students at the UFS, for assistance with data collection.
Competing interests
The authors declare that they have no financial or personal relationships which may have inappropriately influenced them in writing this article.
Authors' contributions
A.M.d.P. was the main researcher reporting on her PhD study and the primary author of the article. M.d.M was the supervisor of the study and contributed to the article by providing guidance regarding structure and content. F.F.C. was the co-supervisor of the study and provided guidance on writing of the manuscript. M.N. was the biostatistician involved in the study and gave input during the planning and analysis of the study. All the authors approved the final version of the article.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability statement
Data are available from the corresponding author on request.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
Alesi, M., Pecoraro, D. & Pepi, A., 2019, 'Executive functions in kindergarten children at risk for developmental coordination disorder', European Journal of Special Needs Education 34(3), 285-296. https://doi.org/10.1080/08856257.2018.1468635 [ Links ]
Ali, H.A.A., El-Tohamy, A.M. & Mousa, A., 2015, 'Prevalence of developmental coordination disorder in Egyptian children', Trends in Applied Sciences Research 11(1), 1-11. https://scialert.net/abstract/?doi=tasr.2016.1.11 [ Links ]
Amador-Ruiz, S., Gutierrez, D., Martínez-Vizcaíno, V., Gulíaz-González, R., Pardo-Guijarro, M.J. & Sánchez-López, M., 2018, 'Motor competence levels and prevalence of developmental coordination disorder in Spanish children: The Movi-Kids Study', Journal of School Health 88(7), 538-546. https://doi.org/10.1111/josh.12639 [ Links ]
American Psychiatric Association, 2013, Diagnostic and statistical manual of mental disorders, 5th edn., American Psychiatric Association, Washington, DC.
Asonitou, K., Koutsouki, D., Kourtessis, T. & Charitou, S., 2012, 'Motor and cognitive performance differences between children with and without developmental coordination disorder (DCD)', Research in Developmental Disabilities 33(4), 996-1005. https://doi.org/10.1016/j.ridd.2012.01.008 [ Links ]
Barba, P.C.D.D., Luiz, E.M., Pinheiro, R.C. & Lourenco, G.F., 2017, 'Prevalence of developmental coordination disorder signs in children 5 to 14 years in São Carlos', Motricidade 13(3), 22-30. https://doi.org/10.6063/motricidade.10058 [ Links ]
Barnhart, R.C., Davenport, M.J., Epps, S.B. & Nordquist, V.M., 2003, 'Developmental coordination disorder', Physical Therapy 83(8), 722-731. [ Links ]
Batey, C.A., Missiuna, C.A., Timmons, B.W., Hay, J.A., Faught, B.E. & Cairney, J., 2014, 'Self efficacy toward physical activity and the physical activity behaviour of children with and without developmental coordination disorder', Human Movement Science 36(1), 258-271. https://doi.org/10.1016/j.humov.2013.10.003 [ Links ]
Blank, R., Smits-Engelsman, B., Polatajko, H. & Wilson, P., 2012, 'European Academy for Childhood Disability (EACD): Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (long version)', Developmental Medicine and Child Neurology 54(1), 54-93. https://doi.org/10.1111/j.1469-8749.2011.04171.x [ Links ]
Cairney, J., Hay, J., Faught, B., Mandigo, J. & Flouris, A., 2005, 'Developmental coordination disorder, self-efficacy toward physical activity, and play: Does gender matter?', Adapted Physical Activity Quarterly 22(1), 67-82. https://doi.org/10.1123/apaq.22.1.67 [ Links ]
Cairney, J., Kwan, M.Y., Hay, J.A. & Faught, B.E., 2012, 'Developmental coordination disorder, gender, and body weight: Examining the impact of participation in active play', Research in Developmental Disabilities 33(5), 1566-1573. https://doi.org/10.1016/j.ridd.2012.02.026 [ Links ]
Cairney, J. & Steiner, D.L., 2011, 'Using relative improvement over chance (RIOC) to examine agreement between tests: Three case examples using studies of developmental coordination disorder (DCD) in children', Research in Developmental Disabilities 32(1), 87-92. https://doi.org/10.1016/j.ridd.2010.09.001 [ Links ]
Cantell, M.H., Smyth, M.M. & Ahonen, T.P., 2003, 'Two distinct pathways for developmental coordination disorder: Persistence and resolution', Human Movement Science 22(4-5), 413-431. https://doi.org/10.1016/j.humov.2003.09.002 [ Links ]
Cardoso, A.A. & Magalhães, L.C., 2009, 'Bilateral coordination and motor sequencing in Brazilian children: Preliminary construct validity and reliability analysis', Occupational Therapy International 16(2), 107-121. https://doi.org/10.1002/oti.273 [ Links ]
Cardoso, A.A., Magalhães, L.C. & Rezende, M.B., 2014, 'Motor skills in Brazilian children with developmental coordination disorder versus children with motor typical development', Occupational Therapy International 21(4), 176-185. https://doi.org/10.1002/oti.1376 [ Links ]
Carslaw, H., 2011, 'Developmental coordination disorder', Innovait 4(2), 87-90. https://doi.org/10.1093/innovait/inq184 [ Links ]
Cloete, E., Pienaar, A.E. & Coetzee, M., 2006, 'Lae fisieke aktiwiteit se varband met ontwikkelingskoördinasieversteuring: Thusa Bana-studie', South African Journal of Research in Sport, Physical Education and Recreation 28(1), 13-27. https://doi.org/10.4314/sajrs.v28i1.25928 [ Links ]
Collinridge, L., 2013, Schools quintile system to change, viewed 03 March 2019, from http://:www.corruptionwatch.org.za/schools-quintile-system-to-change/.
Delgado-Lobete, L., Santos-Del-Riego, S., Pértega-Díaz, S. & Montes-Montes, R., 2019, 'Prevalence of suspected developmental coordination disorder and associated factors in Spanish classrooms', Research in Developmental Disabilities 86(1), 31-40. https://doi.org/10.1016/j.ridd.2019.01.004 [ Links ]
De Milander, M., Coetzee, F.F. & Venter, A., 2014, 'Developmental coordination disorder in grade 1 learners', African Journal for Physical Health Education, Recreation and Dance 20(3), 1075-1085. [ Links ]
De Milander, M., Coetzee, F.F. & Venter, A., 2016, 'Prevalence and effect of developmental coordination disorder on learning-related skills of South African grade one children', South African Journal for Research in Sport, Physical Education and Recreation 38(2), 49-62. [ Links ]
De Souza, T.D.F., 2016, Especificidade e Sensibilidade do Questionário de Transtorno do Desenvolvimento da Coordenação - Brasil para crianças de 8 a 10 anos, Master's dissertation [abstract in English], Universidade Federal de São Carlos, São Carlos, viewed 24 February 2020, from https://repositorio.ufscar.br/handle/ufscar/7283 [ Links ]
De Waal, E., Pienaar, A.E. & Coetzee, D., 2018, 'Gender differences in academic achievement of children with developmental coordination disorder', South African Journal of Childhood Education 8(1), a515. https://doi.org/10.4102/sajce.v8i1.515 [ Links ]
Dewey, D., Kaplan, B.J., Crawford, S.J. & Wilson, B.N., 2002, 'Developmental coordination disorder: Associated problems in attention, learning and psychosocial adjustment', Human Movement Science 21(5-6), 905-918. https://doi.org/10.1016/S0167-9457(02)00163-X [ Links ]
Dhote, N.S., Tushar, J.P. & Ganvir, S., 2017, 'Age wise prevalence of developmental coordination disorder in school going children in west India', International Archives of Integrated Medicine 4(4), 1-7. [ Links ]
Edwards, J., Berube, M., Erlandson, K., Haug, S., Johnstone, H., Meagher, M. et al., 2011, 'Developmental coordination disorder in school-aged children born very preterm and/or at very low birth weight: A systematic review', Journal of Developmental and Behavioural Pediatrics 32(9), 678-687. https://doi.org/10.1097/DBP.0b013e31822a396a [ Links ]
Engel-Yeger, B., Rosenblum, S. & Josman, N., 2010, 'Movement assessment battery for children (M-ABC): Establishing construct validity for Israeli children', Research in Developmental Disabilities 31(1), 87-96. https://doi.org/10.1016/j.ridd.2009.08.001 [ Links ]
Gaines, R. & Missiuna, C., 2007, 'Early identification: Are speech/language-impaired toddlers at increased risk for developmental coordination disorder?', Child Care, Health and Development 33(3), 325-332. https://doi.org/10.1111/j.1365-2214.2006.00677.x [ Links ]
Gillberg, C., 2003, 'Deficits in attention, motor control, and perception: A brief review', Archives of Disease in Childhood 88(10), 904-910. https://doi.org/10.1136/adc.88.10.904 [ Links ]
Girish, S., Raja, K. & Kamath, A., 2016, 'Prevalence of developmental coordination disorder among mainstream school children in India', Journal of Pediatric Rehabilitation Medicine 9(2), 107-116. https://doi.org/10.3233/PRM-160371 [ Links ]
Gomez, A. & Sirigu, A., 2015, 'Developmental coordination disorder: Core sensori-motor deficits, neurobiology and etiology', Neuropsychologia 79(Pt B), 272-287. https://doi.org/10.1016/j.neuropsychologia.2015.09.032 [ Links ]
Goyen, T.A. & Lui, K., 2009, 'Developmental coordination disorder in "apparently normal" school children born extremely preterm', Archives of Disease in Childhood 94(4), 298-302. https://doi.org/10.1136/adc.2007.134692 [ Links ]
Henderson, S.E., Sugden, D.A. & Barnett, A.L., 2007, Movement Assessment Battery for Children-2 (MABC-2), 2nd edn., The Psychological Corporation/Harcourt Brace and Company Publishers, London.
Hua, J., Jin, H., Gu, G., Liu, M., Zhang, L. & Wu, Z., 2014, 'The influence of Chinese one-child family status on developmental coordination disorder status', Research in Developmental Disabilities 35(11), 3089-3095. https://doi.org/10.1016/j.ridd.2014.07.044 [ Links ]
Isaacs-Martin, W., 2015, 'Issues of race, ethnicity, socioeconomic position and spatial acknowledgement in South Africa: How spatial access and expression still perpetuate notions of difference, separation and uncertainty amongst the South African coloured population', International Journal of African Renaissance Studies 10(1), 120-140. https://doi.org/10.1080/18186874.2015.1050219 [ Links ]
Kadesjö, B. & Gillberg, C., 1998, 'Attention deficits and clumsiness in Swedish 7-year-old children', Developmental Medicine and Child Neurology 40(12), 796-804. https://doi.org/10.1111/j.1469-8749.1998.tb12356.x [ Links ]
Kokštejn, J., Musálek, M., Št'astný, P. & Golas, A., 2017, 'Fundamental motor skills of Czech children at the end of the preschool period' Acta Gymnica 47(4), 193-200. https://doi.org/10.5507/ag.2017.024 [ Links ]
Lingam, R., Golding, J., Jongmans, M., Hunt, L., Ellis, M. & Emmond, A., 2010, 'The association between developmental coordination disorder and other developmental traits', Pediatrics 126(5), e1109-1118. https://doi.org/10.1542/peds.2009-2789 [ Links ]
Lingam, R., Hunt, L., Golding, J., Jongmans, M. & Edmond, A., 2009, 'Prevalence of developmental coordination disorder using the DSM-IV at 7 years of age: A UK population based study', Pediatrics 123(4), e693-e700. https://doi.org/10.1542/peds.2008-1770 [ Links ]
Missiuna, C., 2003, Children with developmental coordination disorder: At home and in the classroom, viewed 30 July 2019, from http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.504.7511&rep=rep1&type=pdf.
Missiuna, C., Gaines, B., Souchie, H. & McLean, J., 2006, 'Parental questions about developmental coordination disorder: A synopsis of current evidence', Paediatric Child Health 11(8), 507-512. https://doi.org/10.1093/pch/11.8.507 [ Links ]
Miyahara, M., Tsujii, M., Hanai, T., Jongmans, M., Barnett, A., Henderson, S.E. et al., 1998, 'The Movement Assessment Battery for Children: A preliminary investigation of its usefulness in Japan', Human Movement Science 17(4-5), 679-697. https://doi.org/10.1016/S0167-9457(98)00018-9 [ Links ]
Narsai, P., Taylor, M., Jinabhai, C. & Stevens, F., 2013, 'Variations in housing satisfaction and health status in four lower socio-economic housing typologies in the eThekwini Municipality in KwaZulu-Natal', Development Southern Africa 30(3), 367-385. https://doi.org/10.1080/0376835X.2013.817304 [ Links ]
Ndebele, M., 2015, 'Socio-economic factors affecting parents' involvement in homework: Practices and perceptions from eight Johannesburg public primary schools', Perspectives in Education 33(3), 72-91. [ Links ]
Pappin, M., Marais, L., Sharp, C., Lenka, M., Cloete, J., Skinner, D. et al., 2015, 'Socio-economic status and socio-emotional health of orphans in South Africa', Journal of Community Health 40(1), 92-102. https://doi.org/10.1007/s10900-014-9903-1 [ Links ]
Pauw, K., 2005, 'A profile of the Free State Province: Demographics, poverty, inequality and unemployment', Provide Project Background Paper Series 1(4), 1-25. https://doi.org/10.22004/ag.econ.15616 [ Links ]
Pienaar, A.E., 2004, 'Developmental co-ordination disorder in an ethno-racially diverse African nation: Should norms of the MABC be adjusted?', Journal of Human Movement Studies 47(1), 75-92. [ Links ]
Pienaar, A.E. & Kemp, C., 2014, 'Motor proficiency profile of grade 1 learners in the North West Province of South Africa: NW-child study', South African Journal for Research in Sport, Physical Education and Recreation 36(1), 167-182. [ Links ]
Pienaar, A.E., Labuschagne, G.M. & Peens, A., 2007, 'Motor and sensory development of 5-6-year-old children in poor socio-economic circumstances: Thusano-study', African Journal for Physical, Health Education, Recreation and Dance (special edition) Supplement (September), 304-320.
Pienaar, A.E. & Lennox, A., 2006, 'Die effek van 'n motoriese intervensieprogram gebaseer op 'n geïntegreerde benadering vir 5- tot 8-jarige plaaswerkerkinders met DCD: Flagh-studie', South African Journal for Research in Sport, Physical Education and Recreation 28(1), 69-83. https://doi.org/10.4314/sajrs.v28i1.25932 [ Links ]
Pienaar, R. & McKay, T.M., 2014, 'Mapping socio-economic status, geographical location and matriculation pass rates in Gauteng, South Africa', Perspectives in Education 32(1), 101-119. [ Links ]
Prinsloo, A. & Pienaar, A.E., 2003, 'Prevalence of developmental coordination disorder and influences of physical activity levels and body composition on the children of farm workers: Flagh-study', African Journal for Physical, Health Education, Recreation and Dance 9(1), 151-164. https://doi.org/10.4314/ajpherd.v9i1.46318 [ Links ]
Rihtman, T., Wilson, B.N. & Parush, S., 2011, 'Developmental of the Little Developmental Coordination Disorder Questionnaire for preschoolers and preliminary evidence of its psychometric properties in Israel', Research in Developmental Disabilities 32(4), 1378-1387. https://doi.org/10.1016/j.ridd.2010.12.040 [ Links ]
Rivard, L., Missiuna, C., McCauley, D. & Cairney, J., 2014, 'Descriptive and factor analysis of the Developmental Coordination Disorder Questionnaire (DCDQ'07) in a population-based sample of children with and without developmental coordination disorder', Child Care, Health and Development 40(1), 42-49. https://doi.org/10.1111/j.1365-2214.2012.01425.x [ Links ]
Schoemaker, M.M., Smits-Engelsman, B.C. & Jongmans, M.J., 2003, 'Psychometric properties of the Movements Assessment Battery for Children-Checklist as a screening instrument for children with a developmental co-ordination disorder', British Journal of Education Psychology 73(3), 425-441. https://doi.org/10.1348/000709903322275911 [ Links ]
Senekal, M., Seme, Z., De Villiers, A. & Steyn, N.P., 2015, 'Health status of primary school educators in low socio economic areas in South Africa', BMC Public Health 15(1), 186. https://doi.org/10.1186/s12889-015-1531-x [ Links ]
Tsiotra, G.D., Flouris, A.D., Koutedakis, Y., Faught, B.E., Nevill, A.M., Lane, A.M. et al., 2006, 'A comparison of developmental coordination disorder prevalence rates in Canadian and Greek children', Journal of Adolescent Health 39(1), 125-127. https://doi.org/10.1016/j.jadohealth.2005.07.011 [ Links ]
Valentini, N.C., Clark, J.E. & Whitall, J., 2015, 'Developmental co-ordination disorder in socially disadvantaged Brazilian children', Child Care, Health and Development 41(6), 970-979. https://doi.org/10.1111/cch.12219 [ Links ]
Valentini, N.C., Coutinho, M.T.C., Pansera, S.M., Dos Santos, V.A.P., Veira, J.L.L., Ramalho, M.H. et al., 2012, 'Prevalence of motor deficits and developmental coordination disorders in children from South Brazil' [article in Spanish], Revista Paulista Pediatria 30(3), 377-384. https://doi.org/10.1590/S0103-05822012000300011 [ Links ]
Van Den Berg, S., 2015, 'What the Annual National Assessments can tell us about learning deficits over the education system and the school career', South African Journal of Childhood Education 5(2), 28-43. https://doi.org/10.4102/sajce.v5i2.381 [ Links ]
Venter, A., Pienaar, A.E. & Coetzee, D., 2015, 'Extent and nature of motor difficulties based on age ethnicity, gender and socio-economic status in a selected group of three- to five-year-old children', South African Journal for Research in Sport, Physical Education and Recreation 37(3), 169-183. [ Links ]
Wade, M.G. & Kazeck, M., 2018, 'Developmental coordination disorder and its cause: The road less travelled', Human Movement Science 57(1), 489-500. https://doi.org/10.1016/j.humov.2016.08.004 [ Links ]
Wessels, Y., Pienaar, A.E. & Peens, A., 2008, 'Geslags- en rasverskille by 6- en 7-jarige kinders met ontwikkelingskoördinasieversteurings ("DCD") in leerverwante vaardighede en ADHD: Navorsings- en oorsigartikel', Tydskrif vir Geesteswetenskappe 48(4), 493-504. [ Links ]
Wuang, Y., Su, J. & Su, C., 2012, 'Reliability and responsiveness of the Movement Assessment Battery for Children Second Edition Test in children with developmental coordination disorder', Developmental Medicine and Child Neurology 54(2), 160-165. https://doi.org/10.1111/j.1469-8749.2011.04177.x [ Links ]
Zhu, J.L., Obel, C., Basso, O. & Olsen, J., 2010, 'Parental infertility and developmental coordination disorder in children', Human Reproduction 25(4), 908-913. https://doi.org/10.1093/humrep/deq010 [ Links ]
Zwicker, J.G., Missiuna, C. & Boyd, L.A., 2009, 'Neural correlates of developmental coordination disorder: A review of hypotheses', Journal of Child Neurology 24(10), 1273-1281. https://doi.org/10.1177/0883073809333537 [ Links ]
 Correspondence:
Correspondence:
Alretha du Plessis
20268319@nwu.ac.za
Received: 12 Dec. 2019
Accepted: 08 June 2020
Published: 07 Sept. 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}