










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkCurationis
versión On-line ISSN 2223-6279
versión impresa ISSN 0379-8577
Curationis vol.37 no.1 Pretoria ene. 2014
http://dx.doi.org/10.4102/curationis.v37i1.1184
ORIGINAL RESEARCH
Using a simulated patient to transfer patient-centred skills from simulated practice to real patients in practice
Yolinda Uys; Ina Treadwell
University of Limpopo, Medunsa Campus, South Africa
ABSTRACT
BACKGROUND: Simulation in healthcare education is common practice. Although this teaching strategy increases patient safety, it is not proven to enhance patient-centred care in practice. Simulated patients are used to teach communication skills and to contribute to the authenticity of the simulation. Could this enhanced authenticity help bridge the gap from simulated practice to practice with live patients where patient-centredness is of crucial importance?
OBJECTIVE: This study's objective was to determine whether students who acquired a skill in simulation using a simulated patient displayed more patient-centredness in practice than students who used a mannikin.
METHOD: A pre-experimental, post-test-only design with a comparison group was used. The population sample comprised all second-year B.Cur. students (N = 36) at a tertiary institution, who were divided into two cohorts. Cohort 1 was trained to administer an intramuscular injection using a simulated patient with a strap-on injectable device, whilst cohort 2 used an injection model. All participants were assessed on their procedural skills as well as patient-centred care whilst administering an injection to a patient in hospital. A comparison was made of mean scores for patient-centred care rendered by the two cohorts.
RESULTS: Fisher's exact test revealed that the mean score for patient-centredness of cohort 1 (88%) was significantly higher (p = < 0.001) than that of cohort 2 (74%).
CONCLUSION: Using a simulated patient to teach administration of an intramuscular injection enhanced students' patient-centredness when performing the procedure in practice. Recommendations include making use of a bigger sample and including a pre-test the next time research of this nature is carried out.
Introduction
Simulated training in health care is aimed at providing interactive experiences to develop skills, critical thinking and the capability to solve complex clinical problems (Reilly & Spratt 2007:544). Simulation in healthcare education and simulation learning experiences using low-fidelity mannikins is common practice. This teaching strategy increases patient safety, but has not been proven to enhance patient-centred care in practice. Simulated patients (SPs) are used to teach communication skills and to contribute to the authenticity of the simulation. Could this enhanced authenticity in teaching help bridge the gap from simulated practice to practice with live patients, where patient-centredness is of crucial importance?
Problem statement
Since the use of new technology has provided health education with mannikins of increased high-fidelity, it makes the learning scenario appear quite real. The use of high-fidelity mannikins will suspend incredulity in the learning experience (Rodgers 2007:13). Standardised patients are real-life people acting as patients, and it is suspected that they enhance the authenticity of the learning experience. The problem statement is thus to determine whether the use of SPs as a teaching strategy is conducive to fostering patient-centredness in practice.
Aim
This study aimed to determine whether students who acquired the skill of administering an intramuscular injection (IMI) in simulation, using an SP with a strap-on injectable device, displayed more patient-centredness when performing the skill in real practice than students who used an injection model.
Background
Simulation and mannikins have been used since World War II (Sanford 2010:1006), and such teaching strategies are used to enhance skills, develop clinical decision making and critical thinking. Nursing education must deliver competent graduates who are sufficiently skilled and will render safe patient care (Hughes 2008:23) Graduates must display patient-centredness in their physical, emotional, and cultural support of the family and patient. Sensitivity for the preferences of the individual must be a priority (Lewis 2009:1). The challenge to provide graduates with all of the abovementioned competencies and skills compels educators to compare ways of teaching. This study provides a comparison of two clinical teaching strategies.
Trends
Although research on effectiveness and outcomes when using simulators and simulations in nursing education is limited, the use of simulation as a teaching strategy is common practice (Sanford 2010:1006). Students acquire and refine their skills in a safe environment to optimise clinical outcomes (Patow 2007:1). Simulations provide a less threatening environment for practising skills required for accurate and safe patient care (Sanford 2010:1006).
Research objectives
- Teaching/learning of administration of an IMI by using either an SP with a strap-on injectable device (cohort 1) or an injection model (cohort 2).
- Assessment of both cohorts' performances (including patient-centred care) in administering IMIs to live patients.
- Comparison of assessment results for patient-centred care in cohort 1 and cohort 2.
Definition of key concepts
Patient-centred care is essential to providing high-quality care, and envelops several different attributes and behaviours. These include physical comfort and emotional support as well as handling patients as persons in the context of their own social worlds, who are listened to, informed, respected and involved in their own care (Hughes 2008:3).
Simulated patients (SPs) are characters portrayed by actors for the purposes of teaching, practising, and assessing clinical skills.
Standardised patients are SPs that present repetitive, realistic portrayals of the same patient scenario in a similar, standardised manner by using the exact same opening line and same scenario for every student (Hanna & Fins 2006:265).
A simulation model is a static replication of a part of the human body that provides no interactivity but is suitable for training students in a certain task. The degree of fidelity is the trueness to life of the teaching experience (Poikela & Poikela 2012:53).
Contribution to the field
This study can contribute evidence to support the use of SPs in simulated training of procedural skills to enhance students' patient-centred skills when carrying out tasks in practice. The authors support a teaching strategy using SPs to enhance patient-centred care.
Literature review
Patient-centredness, leading to positive patient outcomes and fewer complaints, is regarded as one of the core values in all healthcare professions. This approach results in patients' emotional state being much more positive as they experience sharing of power, being treated as a person and being able to create a therapeutic alliance with a healthcare provider (Hudson et al. 2011:155).
Since person-centred care equates to quality care, a philosophy that centres on patient-centredness must be fostered whilst students are trained and whilst they are in the clinical setting. The focus should not only be on the patients' healthcare needs (Manley, Hills & Marriot 2011:36).
Patient safety is undeniably the most important benefit when training healthcare students in simulation. Simulation is especially effective in the development of skills that require hand-eye coordination and ambidextrous manoeuvres. Not only is the performance much improved, but also teamwork, communication skills and confidence (Patow 2007:1-2). According to Buckley and Gordon (2011:716, 719) patient outcomes can be improved by using high-fidelity mannikins in the clinical training of students.
There are many other types of teaching strategies that can be utilised in the clinical training of students, such as human cadavers, which provide realistic simulations where anatomy can be studied. However, patient- centeredness cannot be taught with cadavers. Audio simulations can be used to teach the auscultation sound in the heart and lungs. Patients in the clinical setting provide realistic scenarios, but patient safety must be considered as a high priority, and inexperienced students preferably start off in the simulation laboratory first (Rodgers 2007:11).
Using SPs when patient-centeredness is at stake, such as in psychiatry, has been indicated to be extremely valuable (Eagles et al.2007:188). Patient-centeredness is regarded as one of the core values in all medical professions, and proves positive outcomes and fewer complaints from patients. Simulation training in nursing is beneficial, and the use of simulators and/or mannikins and SPs is aimed at ensuring the competency of students before encountering real-life patients (Wilson et al. 2005:56, 57).
Human SPs are real-life people used to portray a patient. They present repetitive, realistic portrayals of the same patient scenario in a standardised manner by using the exact same opening line and scenario for each student. The SP accurately simulates an actual patient by incorporating appropriate body language and personality characteristics, creating a realistic environment conducive to teaching and evaluating the patient-centred care model critical to today's healthcare practice (Gerzina 2012).
The use of an SP in simulation can enhance the safety of patients, since students get the exposure to real-life situations without posing any risk to real patients. This teaching strategy provides a safe learning environment to the student and gives them the opportunity to work and interact with responding patients without feeling that their incorrect decisions or actions will harm the patient. Including the SP as an integral part of the training team will not only enhance authenticity, but also promote social interaction, group dynamics and collective negotiating skills through communication.
There is consensus that person-centred care equates with quality care. A philosophy that centres on patient- centeredness must be fostered whilst students are trained and in the clinical setting, and not only focus on the patients' healthcare needs (Manley et al. 2011: 36). SPs could be used to teach patient-centred care and assist healthcare professionals in developing vitally important traits and skills (Gerzina 2012) such as social interaction and communication. SPs add value to the learning because of the reality-based nature of the learning experience, with which the students of today can relate, and which they could prefer (Parker & Myrick 2011:81).
Further advantages of using SPs, as discussed by Durham and Alden (2008:3-231), include opportunities for students to participate and to be the drivers of their own learning. This is consistent with the adult learning theory. It also enhances communication with the patients and their family members as well as with the interdisciplinary team members. Skills and procedures are practised in an authentic situation and students become aware of the effect of their actions on patients (Hughes 2008:3-232).
The display of patient-centred care can be measured by adding items representing the major constructs in patient-centred care to an objective structured clinical examination (OSCE) checklist (Wilkerson et al. 2010:86).
Simulation-based teaching is a satisfactory basis for acquiring procedural skills. Interpersonal skills - which are essential components of carrying out a clinical procedure on a conscious patient - can, however, be ignored (Kneebone et al. 2006:1107).
The objective in creating any simulation experience is to achieve a high degree of fidelity, implying a close replication of the real-life, human situation (Aldrich 2012:117). Fidelity to the real clinical situation helps students to react as they would in a real-life scenario. Using SPs to enhance the fidelity or authenticity of the learning experience has been indicated as extremely valuable when patient-centredness is at stake (Eagles et al. 2007:189). Parker and Myrick (2011:74) concur that SPs add value since it is a reality-based learning experience.
Research design and method
A pre-experimental post-test-only design with a comparison group was used in this study (Burns & Grove 2009:216). Participants were allocated to two cohorts: cohort 1 was trained to administer an IMI using an SP with a strap-on injectable device, whilst cohort 2 was trained using an injection model. Patient-centred care was included in the teaching of both cohorts.
On completion of the training both cohorts were observed and objectively assessed on their procedural skills and patient-centred care whilst administering IMI to patients in the hospital. Post-test scores were calculated and compared to determine the difference in patient-centred care between the two cohorts. This study did not include any pre-testing, and therefore any difference between the two cohorts prior to the study was unknown.
Population and sampling
The population sample comprised B.Cur. (N = 36) nursing students. Numbers were given to participants that were listed alphabetically to form the sampling frame, and the top 50% were allocated to cohort 1 and the remaining 50% to cohort 2. The nursing students were in their second year of training. Administration of an IMI is part of their practical skills training during their second year. Patient-centred care had been incorporated into all the teaching of practical skills since their first year of study. Both the psychomotor and patient-centred skills were observed and assessed.
Data collection
A checklist was developed based on a tested checklist used for assessing administration of an IMI in the Skills Centre. Since the display of patient-centred care can be measured by adding items representing the major constructs in patient-centred care to an OSCE checklist (Wilkerson et al. 2010:57), actionable attributes of patient-centredness were identified through a literature review and added as items. These items were based on current evidence and consensus review by the researchers and two facilitators involved in teaching procedural and clinical communication skills. The attributes presented five core values of patient-centred care (Table 1) that healthcare professionals should provide: physical comfort, emotional support (Hughes 2008:22), being listened to, informed, respected and involved in one's own care (Epstein & Street 2011:100).

Structured observation, a very systematic method, was used in this study (Cohen, Manion & Morrison 2011:459). The developed checklist was used to assess each participant on administering an IMI to a patient in a hospital ward. The psychomotor and patient-centred items were dichotomously scored on separate forms as 'done' or 'not done'. Fourteen checklist items presenting actionable attributes of patient-centredness, as seen in Table 1, were added to the tool used for assessing students' procedural skill in administering an IMI.
The items (attributes) presented five core values of patient-centred care that healthcare professionals should provide, as defined in the literature (Hughes 2008:22; Epstein & Street 2011:100). The checklist was developed by the researchers based on current evidence and consensus review.
Data analysis
The data from the checklists were captured in Excel spreadsheets and the 'done' responses were summarised by percentages. The average percentages for the patient-centred items for cohorts 1 and 2 were compared using Fisher's exact test.
Results
The average of the total scores for patient-centred care was 88% for cohort 1, who trained with an SP, and 74% for cohort 2, who trained on a mannikin. Cohort 1 therefore performed significantly better (p < 0.001) than cohort 2.
A comparison of the cohorts' assessed five core values revealed that cohort 1 did significantly better (p < 0.05) than cohort 2 in showing respect by acknowledging the patient, ensuring a comfortable position after the procedure, and rendering emotional support by allaying the patient's fears (Table 2).
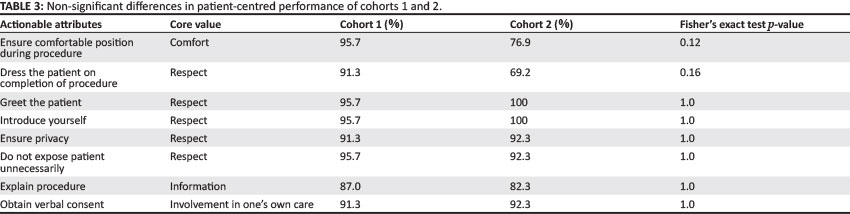
Table 3 reveals that although the difference was not significant, cohort 1 students performed better in ensuring the patient's comfort during the procedure and showing respect by dressing the patient upon completion of the procedure. Students did well on the remaining checklist items (attributes), and there was only a slight difference in other aspects of showing respect (greeting the patient, introducing themselves, ensuring privacy, avoiding unnecessary exposure of the patient), informing the patient (explaining the procedure) and involving the patient in their own care by obtaining verbal consent.
Ethical considerations
The research proposal for this study was approved by the Medunsa Research Ethics Committee.
Potential benefits and hazards
There were no hazards involved in the research. The students had to perform the procedure as part of their curricular activities. Since participation was voluntary, participants were made aware of being entitled to withdraw from the study if they so wished. The whole of the second-year B.Cur. group was selected, and in doing so fairness was ensured by allowing all members of the group to participate. To ensure ethical fairness the group in total was given the opportunity to practice the IMI on SPs before their final summative assessment at the end of the year. This was done after the execution of data collection for this research.
Informed consent
Written informed consent was obtained from participants to take part in this study and to allow publication of the results. No harm was done to students or patients in this study.
Data protection
Scores were recorded on separate checklists; those for the patient-centred skills were anonymous and only marked as cohort 1 or 2. Confidentiality was ensured by filing the anonymous checklists separately from the injection checklists that identified students. Confidentiality was further ensured by the researcher personally managing the data collection instruments.
Trustworthiness
Reliability
Inter-rater reliability was addressed by having two raters scoring the same individual and comparing their results. This was done until the two raters were sure that they understood the assessment document and corresponded in their assessment. Correlation coefficients were not determined.
Validity
The lecturer who taught the procedure was not involved in the participants' assessments, since this could pose a threat to the internal validity if the assessor was closely involved with the participants prior to the assessments (Cohen et al. 2011:209).
Content validity was considered by matching the content of the assessment sheet with the characteristics of patient-centred care as per the literature. For the purpose of validity a pilot study was carried out to ensure that the observed skills for patient-centred care were suitable, comprehensive and fit the goal of the research. The pilot study was done with four clinical specialists, who conveyed consensus on the checklist items. The clinical specialists were part of the Nursing Department in the specific tertiary institution and part of a team of six; the pilot sample thus consisted of more than 50% of this population.
The pilot study revealed one concept that was debated; all of the other concepts and questions on the assessment document were agreed upon. The concept that was discussed was whether 'Allay fears of the patient' should be included or not. The reasoning was that it could place the focus on fears, which have a negative connotation even if the patient would not necessarily have any fears. It was decided to include it as students should be made aware of the irrationality and/or the reality of some patients' fears.
Discussion
Outline of the results
The study aimed to determine whether students who acquired a skill in simulation using an SP (cohort 1) displayed more patient-centredness in practice than students who used a simulation model (cohort 2). The patient-centredness of cohort 1 was found to be significantly better than the students who trained on a model. This indicates that including an SP in a simulation scenario becomes more authentic, patient-centred and more natural, making the student aware of the feelings, insecurities and fears of the patient.
Bearnson and Wiker (2005) explored the use of SPs in the training of nursing students, and concluded that SPs enhance both teaching and evaluating. They further pointed out the benefit of use of SPs as a medium for safe and effective experiential learning.
The literature reveals results of various studies that prove that training with SPs is beneficial to improve interpersonal skills and knowledge (Triola et al. 2006:424). Educators today should realise that the use of SPs compared to traditional teaching strategies is an innovative, didactic method that enhances the authenticity of the learning experience.
SPs can be utilised in a number of learning and assessment scenarios, such as in OSCEs. The use of SPs gives the educator the freedom to incorporate creative components into the learning experience. The patients' culture, socio-economic and religious background, to name a few, can be portrayed by SPs, which emphasises the value of using SPs in training (Triola et al. 2006:426).
Practical implications
The integration of SPs in training on nursing skills is of great importance, especially for the enhancement of patient-centred skills. Engagement with the SP will enhance the students'sensitivity towards patient-centred care.
Limitations of the study
The small number of participants, who were selected non-randomly, limits generalisation of the results. In some instances the researcher's involvement in the event can alter the situation and bias the results. Two independent assessors recorded the observation data to limit possible bias. They were orientated on their role prior to data collection. They were also requested to refrain from providing emotional or physical support which could impact on the data, without compromising the safety of the patient (as this should always be the priority) (Burns & Grove 2009:445). The methodological limitation of not carrying out a pre-test should be taken into consideration, as it now cannot be known whether the results were due to the intervention or some other confounding factors. Not determining the correlation coefficient could also be considered a limitation in this study.
Recommendations
Patient-centred skills should be integrated into all practical teaching strategies to enhance the quality of patient care. Students' patient-centredness could be fostered by using well-trained SPs to enhance the authenticity and humanisation of simulations. For future research studies use of a larger sample is suggested, as well as including a pre-test. Random sampling should be used in future research.
Conclusion
The study compared two ways of teaching clinical skills, one using an SP, and the other using a mannikin. In this pre-experimental, post-test-only design two cohort groups were trained, and all participants were assessed on their procedural skills and patient-centred care.
The significance of the study was reflected in the results. The display of patient-centredness by students trained in a procedure using an SP was significantly better than that of students trained on a simulation model. It can therefore be concluded that the use of SPs in training on nursing skills will enhance patient-centred care.
Acknowledgements
The authors would like to thank skills facilitators K. Kgasi and M. Randa who did the assessments of the students, and statistician Prof. H.S. Schoeman who analysed the data. M. Theron trained the students.
Competing interests
The authors declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
Y.U. (University of Limpopo) developed the proposal and the article, and I.T. (University of Limpopo) contributed to the proposal development and writing of the article.
References
Aldrich, C., 2012, 'Why educational simulations? Designs to develop competence plus conviction', Inside Learning Technologies & Skills 1, 117-118, 121. [ Links ]
Bearnson, C.S. & Wiker, K.M., 2005, 'Human patient simulators: A new face in Baccalaureate nursing education at Birgham Young University', Journal of Nursing Education 44(9), 421-425. [ Links ]
Buckley, T. & Gordon, C., 2011, 'The effectiveness of high fidelity simulation on medical-surgical registered nurses ability to recognise and respond to clinical emergencies', Nurse Education Today 31(7), 716-721. http://dx.doi.org/10.1016/j.nedt.2010.04.004 [ Links ]
Burns, N. & Grove, S.K., 2009, The practice of nursing research. Appraisal, synthesis, and generation of evidence, 6th edn., Elsevier, Cape Town. [ Links ]
Cohen, L. Manion, L. & Morrison, K., 2011, Research methods in education, 7th edn., Sage Publications, London. [ Links ]
Durham, C.F. & Alden, K.R., 2008, 'Enhancing patient safety in nursing education through patient simulation', in R.G. Hughes (ed.),Patient safety and quality: An evidence-based handbook for nurses, AHRQ Publication No. 8-0043, Rockville. [ Links ]
Eagles, J.M., Calder, S.A., Wilson, S., Murdoch, J.M. & Sclare, P.D., 2007, 'Simulated patients in undergraduate education in psychiatry',Psychiatric Bulletin 31, 187-190. http://dx.doi.org/10.1192/pb.bp.106.010793 [ Links ]
Epstein, R.M. & Street, R.L., 2011, 'The values and value of patient-centred care', Annals of Family Medicine 9(2), 100-103. http://dx.doi.org/10.1370/afm.1239 [ Links ]
Gerzina, H., 2012, Standardized patients: Teaching patient-centred care for more than 25 years, Northeast Ohio Medical University, viewed 01 October 2012, from http://www.neomed.edu/media-library/story-bank/standardized-patients-teaching-patient-centered-care-for-more-than-25-years [ Links ]
Hanna, M. & Fins, J.J., 2006, 'Power and communication: Why simulation training ought to be complemented by experiential and humanist learning', Academic Medicine 81(3), 265-270. http://dx.doi.org/10.1097/00001888-200603000-00016 [ Links ]
Hudson, C., Fortin, M., Haggerty, J.L., Lambert, M. & Poitras, M.E., 2011, 'Measuring patients' perceptions of patient-centred care: A systematic review of tools for Family Medicine', Annuals of Family Medicine 9(2), 155-164. http://dx.doi.org/10.1370/afm.1226 [ Links ]
Hughes, R.G., 2008, Patient safety and quality: An evidence-based handbook for nurses, AHRQ Publication No. 8-0043, Rockville. [ Links ]
Kneebone, R., Nestel, D., Yadollahi, F., Brown, R., Nolan, C., Durack, J., Brenton, H., Moulton, C., Archer, J. & Darzi, A., 2006, 'Assessing procedural skills in context: Exploring the feasibility of an integrated procedural performance instrument (IPPI)', Medical Education40(11), 1105-1114. http://dx.doi.org/10.1111/j.1365-2929.2006.02612.x [ Links ]
Lewis, S., 2009, An introduction to what it is and how to achieve it, viewed 10 February 2012, from http://www.medworxx.com/patient-centered-care-an-introduction-to-what-it-is-and-how-to-achieve-it-discussion-paper-for-the-saskatchewan-ministry-of-health [ Links ]
Manley, K., Hills, V. & Marriot, S., 2011, 'Person-centred care: Principle of nursing practice', Nursing Standard 25(31), 35-37. http://dx.doi.org/10.7748/ns2011.04.25.31.35.c8431 [ Links ]
Parker, B. & Myrick, F., 2011, 'The grounded theory method: deconstruction and reconstruction in human patient simulator context',International Journal of Qualitative Methods 10(1), 73-82. [ Links ]
Patow, C.A., 2007, Advancing medical education and patient safety through simulation learning, Patient Safety & Quality Healthcare, March/April 2005, viewed 17 July 2012, from http://www.psqh.com/marapr05/simulation.html [ Links ]
Poikela, E. & Poikela, P., 2012, Towards Simulation Pedagogy Developing Nursing Simulation is a European Network, Kopijyvä Oy.Jyväskylä, Povaniemi. [ Links ]
Reilly, A. & Spratt, C., 2007, 'The perceptions of undergraduate student nurses of high-fidelity simulation-based learning: A case report from the University of Tasmania', Nurse Educator Today 27, 542-550. http://dx.doi.org/10.1016/j.nedt.2006.08.015 [ Links ]
Rodgers, D.L., 2007, High-fidelity patient simulation: A descriptive White Paper report, Healthcare Simulation Startegies, Charleston, West Virginia. [ Links ]
Sanford, P.G., 2010, 'Simulation in nursing education: a review of research', Qualitative Report 15(4), 1006- 1011. [ Links ]
Triola, M., Feldman, H., Kalet, A.L., Zabar, S., Kachur, E.K., Gillespie, C., Anderson, M., Griesser, C. & Lipkin, M., 2006, 'A randomized trial of teaching clinical skills using virtual and live standardized patients', Journal of General and Internal Medicine 21, 424-429. http://dx.doi.org/10.1111/j.1525-1497.2006.00421.x [ Links ]
Wilkerson, L., Fung, C.C., May, W. & Elliott, D., 2010, 'Assessing patient-centred care: One approach to health disparities education',Journal of General Internal Medicine 25(2), 86-90. http://dx.doi.org/10.1007/s11606-010-1273-5 [ Links ]
Wilson, M., Sheperd, I., Kelly, C. & Pitzner, J., 2005, 'Assessment of a low fidelity human patient simulator for the acquisition of nursing skills', Nurse Education Today 25, 56-57. http://dx.doi.org/10.1016/j.nedt.2004.10.004 [ Links ]
 Correspondence:
Correspondence:
Yolinda Uys
PO Box 142
Medunsa 0204
South Africa
Email: yolinda.uys@ul.ac.za
Received: 31 May 2013
Accepted: 17 July 2014
Published: 25 Nov. 2014


{kind=link}
{kind=link}