










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Journal of Radiology
versão On-line ISSN 2078-6778
versão impressa ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.26 no.1 Johannesburg 2022
http://dx.doi.org/10.1016/s2352-4642(18)30173-1
CASE REPORT
A rare case of tuberous sclerosis complex-associated renal cell carcinoma
Humphrey MapurangaI; Bianca Douglas-JonesII; Danelo du PlessisIII; Camilla E. le RouxI; Christel du BuissonIV; Shahida MoosaII
IDepartment of Radio-Diagnosis, Faculty of Medical Imaging and Clinical Oncology, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa
IIDepartment of Medical Genetics, Division of Molecular Biology and Human Genetics, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa
IIIDepartment of Surgery, Division of Urology, Faculty of Medicine and Health Sciences, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa
IVDepartment of Paediatrics and Child Health, Paediatric Nephrology, Faculty of Medicine and Health Sciences, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa
ABSTRACT
Renal cell carcinoma is rarely described in paediatric patients with tuberous sclerosis complex. This report describes a case of an 11-year-old male with tuberous sclerosis-associated renal cell carcinoma.
Keywords: tuberous sclerosis complex; renal cell carcinoma; paediatric; neuro-cutaneous; hamartomas.
Introduction
Tuberous sclerosis complex (TSC) is one of a large heterogeneous group of neurocutaneous syndromes with characteristic involvement of structures derived from embryologic neuro-ectoderm, and a prevalence of 1 in 6000-10 000 persons. The disease is characterised by slow-growing hamartomas with multisystem involvement being typical.
Tuberous sclerosis complex is an autosomal-dominant disorder, caused by heterozygous variants in one of the two genes: TSC1, which encodes for hamartin (located on chromosome 9q34), or TSC2, which encodes for tuberin (located on chromosome 16p13.3). Hamartin and tuberin act together as tumour suppressors and are components of the mammalian target of rapamycin (mTOR) signalling pathway.1,2
A clinical diagnosis of TSC is established if the individual has (1) two major clinical criteria, (2) one major and two or more minor criteria, or (3) the identification of a pathogenic variant in either TSC1 or TSC2 on genetic testing. Major criteria include multiple angiofibroma (≥ 3), cardiac rhabdomyoma, cortical dysplasias including tubers and white matter migration lines, hypomelanotic macules (≥ 3 mm of > 5 mm in diameter), lymphangioleiomyomatosis, retinal nodular hamartomas, shagreen patches, subependymal giant cell astrocytomas, subependymal nodules and ungual fibromas. Minor features include 'confetti' lesions on the skin, dental enamel pits, intraoral fibromas, multiple renal cysts, non-renal hamartomas and retinal achromic patches.
Angiomyolipomas (AMLs) are the most common renal lesions associated with TSC and are present in 75% - 80% of patients. Renal cell carcinomas (RCCs) are very rare in patients with TSC (1% - 4%) (2). Moreover, the average age of diagnosis of RCC in patients with TSC is 30 years, with the youngest TSC-associated RCC reported in a 6-month-old girl.3 The clear cell, papillary and chromophobe RCC subtypes have been described in association with TSC.1,4 Renal cysts and oncocytomas may also occur.1,4
This report describes a unique case of an 11-year-old boy with confirmed TSC-associated RCC and highlight his management.
Patient presentation
An 11-year-old boy was referred to paediatric nephrology at Tygerberg Hospital with a clinical concern of hypertension following a seizure at his local hospital. He had a history of generalized tonic-clonic seizures from the age of three years. The seizure episodes were managed and controlled with sodium valproate. At presentation, he was fully awake and alert but persistently hypertensive with a blood pressure higher than the 95th percentile for his height, age and gender.
The patient was examined by a medical geneticist, and the clinical diagnosis of TSC was made, based on fulfillment of two major criteria: (1) > 3 hypomelanotic macules of > 5 mm in diameter, and (2) facial angiofibromas, in addition to further TSC-related features, like multiple 'confetti' skin lesions on his neck and chest and the clinical suspicion of multiple renal cysts. Based on the cystic kidneys, a contiguous gene deletion involving both TSC2 and PKD1 on chromosome 16p13.3 was considered as part of the differential molecular diagnosis, in addition to variants in TSC1 or TSC2.
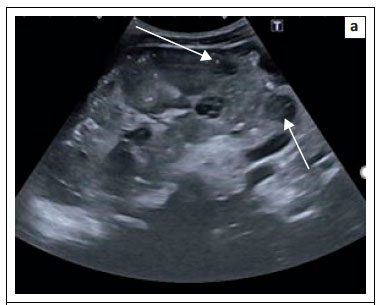
Initial imaging evaluation at our institution included renal ultrasound, which demonstrated multiple bilateral mild to markedly hypoechoic cortical masses (Figure 1a and b). Magnetic resonance imaging (MRI) of the brain and abdomen was subsequently performed.
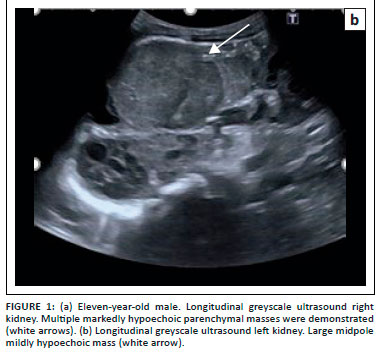
Brain imaging demonstrated T2-weighted hypointense subependymal nodules (Figure 2a and b) with a subependymal giant cell astrocytoma (Figure 2a to d). Fluid-attenuated inversion recovery (FLAIR) demonstrated multiple hyperintense cortical tubers (Figure 2c) and hyperintense white matter radial bands (Figure 2e). No retinal hamartomas were identified.
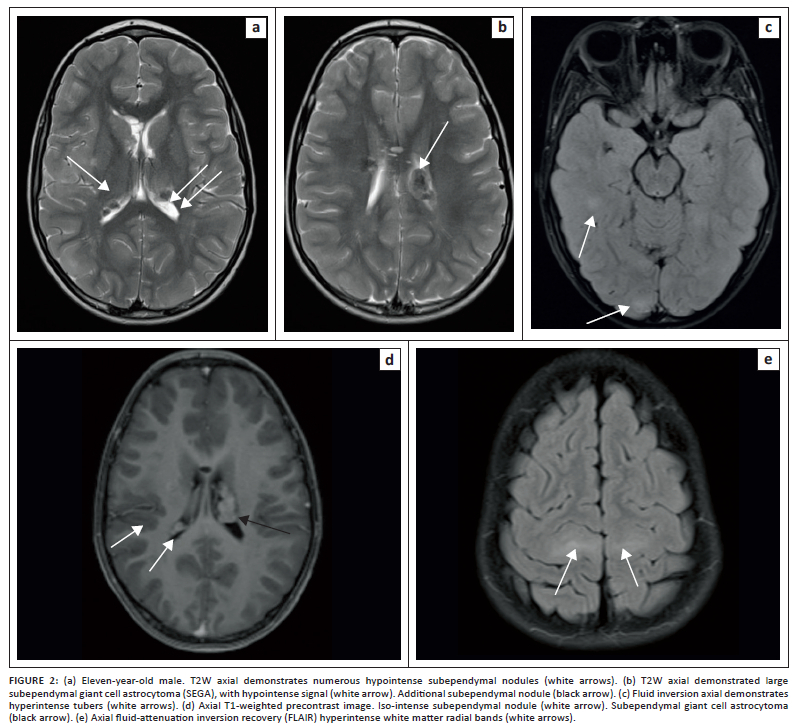
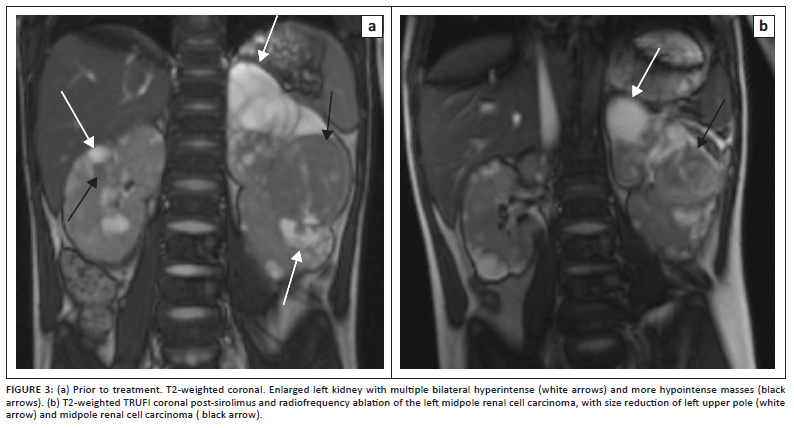
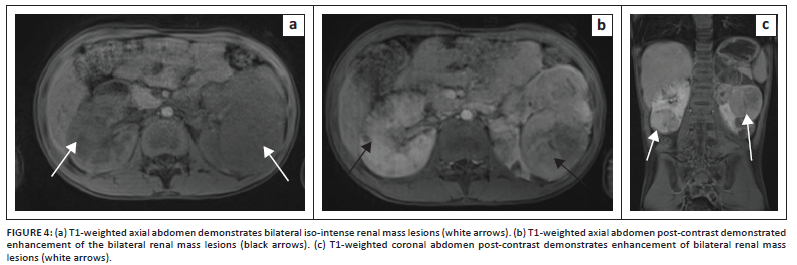
Abdominal MRI demonstrated numerous bilateral renal cortical T2-weighted hypo to hyperintense (Figures 3a and b), T1-weighted hypointense mass lesions (Figure 4a). Fat suppression failed to demonstrate fat content (not shown). Post-contrast enhancement of bilateral renal mass lesions was seen. (Figure 4b and c). Time of flight MRI imaging of the abdominal aorta and renal arteries excluded renal artery stenosis (not shown). A radiological guided biopsy of the left midpole lesion was performed and confirmed tuberous sclerosis-associated RCC of the left kidney.
No concrete evidence of cardiac abnormalities, specifically rhabdomyomas, was found on echocardiogram.
Testing, management and outcome
Genetic testing was performed in a stepwise manner. First, a chromosomal microarray was done and excluded the presence of a contiguous gene deletion on chromosome 16p13.3. The next step in testing was a TSC gene panel (Invitae, United States [US]), which included sequencing and deletion/duplication analysis of TSC1 and TSC2. This showed a pathogenic variant in TSC2 (c.5238_5255del; p.His1746_Arg1751del), which is a known pathogenic variant and definitively confirms the diagnosis.
The patient was started on sirolimus (a oral mTOR inhibitor) to treat his central nervous system (CNS) lesions. Due to the absence of demonstrable fat on MRI, a renal biopsy of the left midpole lesion was performed, which confirmed the diagnosis of tuberous sclerosis-associated RCC of the granular eosinophilic and macrocystic subtype.
The renal nephrometry score of the left midpole lesions was 11p, indicating a high complexity. Given the complexity and number of lesions, nephron sparing surgery was deemed too high a risk. We performed percutaneous ultrasound-guided microwave ablation (Emprint Ablation System, Medtronic) to treat the lesions in the left kidney, average wattage of 50 W and ablation time 6 min 30 s per lesion. Technical success was confirmed at post-ablation MRI (Figure 3b). Interval microwave ablation of the right renal lesions will be performed. The patient did not experience any post-ablation complications.
Discussion
This patient had obvious features of TSC including, seizures due to underlying brain abnormalities, typical skin lesions, and hypertension as the presenting sign of underlying renal anomalies. With the identification of a pathogenic variant in TSC2, his condition was molecularly confirmed and enabled accurate genetic counselling. Up to two-third of patients with TSC have the condition due to a de novo (new) mutation. The risk to his offspring of inheriting the TSC2 variant is 50%.
Renal lesions occur in 50% - 80% of patients with TSC, with AMLs being the most common (75% - 80%). Angiomyolipomas may be classified according to fat content into lipid rich, lipid poor and lipid absent.5 Renal cysts may also be identified in patients with TSC.4 While most RCCs occur sporadically, 3% - 5% are associated with hereditary syndromes, like Von-Hippel Lindau (VHL) disease, hereditary papillary RCC, and Birt-Hogg-Dubé (BHD) syndrome which is the most common. Renal cell carcinoma is very rare in TSC (< 3% of patients) and even rarer in the paediatric population (average age is 30 years).4
Treatment principles for these patients are cancer control, rather than cure, while preserving renal function. RCC develops metastatic potential as the size increases, and if individual tumour size can be kept below 3 cm - 7 cm in maximal diameter, the risk of metastases is estimated at less than 4%. Treatment should be nephron sparing, either surgical or using ablative therapy.6,7
Everolimus, an oral mTOR inhibitor, is effective in treating TSC-associated lesions, not only in the kidney, but also in the CNS; however, it is not recommended for the treatment of non-metastatic RCC.8,9
Renal cysts or polycystic kidney disease can develop in patients with TSC. As opposed to renal AMLs, renal cysts occur in younger children. Although renal cysts are generally asymptomatic, they can more frequently cause subsequent hypertension with rapid progression to end-stage renal failure.10,12 Thus, screening and treating hypertension and proteinuria, as well as preserving renal tissue, with the use of mTOR inhibitors, and sparing of renal tissue are advocated.11,13
Conclusion
Microwave ablasion of selected cases of TSC-associated RCC, in conjunction with Everolimus, is a cornerstone of treatment for renal and central nervous system lesions in TSC.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
H.M. was the primary author; C.E.l.R and S.M. provided overall guidance in article preparation and write up. C.d.B. and D.d.P contributed equally to the case, providing clinical input and patient management details. S.M. and B.D.-J. assessed the patient, made the clinical diagnosis and interpreted the genetic test results.
Ethical considerations
Ethical clearance to conduct this study was obtained from Stellenbosch University Health Research Ethics Committee (Number C21/11/039). Consent for case publication was obtained from the guardian, the patient's mother.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1. Yang P, Cornejo KM, Sadow PM, et al. Renal cell carcinoma in tuberous sclerosis complex. Am J Surg Pathol. 2014;38(7):895-909. https://doi.org/10.1097/PAS.0000000000000237 [ Links ]
2. Verine J, Pluvinage A, Bousquet G, et al. Hereditary renal cancer syndromes: An update of a systematic review. Eur Urol. 2010;58:701-710. https://doi.org/10.1016/j.eururo.2010.08.031 [ Links ]
3. Breysem L, Nijs E, Proesmans W, Smet MH. Tuberous sclerosis with cystic renal disease and multifocal renal cell carcinoma in a baby girl. Pediatr Radiol. 2002;32(9):677-680. https://doi.org/10.1007/s00247-002-0765-9 [ Links ]
4. Northtup H, Krueger DA, International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Paediatr Neurol. 2013;49(4):243-254. [ Links ]
5. Song S, Park BK, Park JJ. New radiologic classification of renal angiomyolipomas. Eur J Radiol. 2016;85(10):1835-1842. https://doi.org/10.1016/j.ejrad.2016.08.012 [ Links ]
6. Pavlovich CP, Schmidt LS. Searching for the hereditary causes of renal-cell carcinoma. Nat Rev Cancer. 2004;4:381-393. https://doi.org/10.1038/nrc1364 [ Links ]
7. Gupta GN, Peterson J, Daryanani KA, et al. Oncologic outcomes of partial nephrectomy for multifocal renal cell carcinoma with tumors greater than 4 cm. J Urol. 2010;184:59-63. [ Links ]
8. Lechuga L, Franz DN. Everolimus as adjunctive therapy for tuberous sclerosis complex-associated partial-onset seizures. Expert Rev Neurother. 2019;19(10):913-925. https://doi.org/10.1080/14737175.2019.1635457 [ Links ]
9. Alsidawi S, Kasi PM. Exceptional response to everolimus in a novel tuberous sclerosis complex-2 mutation-associated metastatic renal-cell carcinoma. Cold Spring Harb Mol Case Stud 2018;4:1-7. https://doi.org/10.1101/mcs.a002220 [ Links ]
10. Nair N, Chakraborty R, Mahajan Z, Sharma A, Sethi SK, Raina R. Renal manifestations of tuberous sclerosis complex. J Kidney Cancer VHL. 2020;7(3):5-19. https://doi.org/10.15586/jkcvhl.2020.131 [ Links ]
11. Rakowski SK, Winterkorn EB, Paul E, Steele DJ, Halpern EF, Thiele EA. Renal manifestations of tuberous sclerosis complex: Incidence, prognosis, and predictive factors. Kidney Int. 2006;70(10):1777-1782. [ Links ]
12. Crino PB. The tuberous sclerosis complex. N Engl J Med. 2006;355:345-356. https://doi.org/10.1056/NEJMra055323 [ Links ]
13. Janssens P, Van Hoeve K, De Waele L, et al. Renal progression factors in young patients with tuberous sclerosis complex: A retrospective cohort study. Pediatric Nephrol. 2018;33(11):2085-2093. https://doi.org/10.1007/s00467-018-4003-6 [ Links ]
 Correspondence:
Correspondence:
Camilla le Roux
camilla.leroux@gmail.com
Received: 23 Jan. 2022
Accepted: 23 Mar. 2022
Published: 20 May 2022
Project Research Registration:
Project Number: 23549


{kind=link}
{kind=link}
{kind=link}