










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Journal of Radiology
versión On-line ISSN 2078-6778
versión impresa ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.24 no.1 Johannesburg 2020
http://dx.doi.org/10.4102/sajr.v24i1.1767
ORIGINAL RESEARCH
Hysterosalpingographic evaluation of human immunodeficiency virus-infected and uninfected infertile women
Dolongo C. OnyangungaI; Jagidesa MoodleyII
IDepartment of Radiology, School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa
IIWomen's Health and HIV Research Unit, Department of Obstetrics and Gynaecology, School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Hysterosalpingography (HSG) is an outpatient fluoroscopy-guided procedure that evaluates the uterine cavity and fallopian tube patency in infertile women. Its cost-effective use is being challenged with the human immunodeficiency virus (HIV) burden in KwaZulu-Natal, which characteristically affects multiple organs.
OBJECTIVES: The aim of this study was to describe the HSG findings in a group of HIV-infected and uninfected infertile women.
METHOD: This was a retrospective study conducted over a 4-year period (2012-2016) in which the HSG images and reports of 178 infertile patients from records of the Radiology Department were re-reviewed for abnormalities of the cervix, uterus and fallopian tubes. Their clinical data and radiological findings were entered into a pre-coded data sheet and analysed.
RESULTS: The frequency of HIV infection amongst patients with infertility was found to be 32.6%. Forty-four patients were on antiretroviral therapy at the time of the HSG examination, whereas three had not yet started treatment. From the 178 HSG reports, 109 (61.2%) were abnormal. Tubal pathologies were the most common abnormalities, accounting for 79 of the 109 cases and was higher in HIV-infected women than in HIV-uninfected women (p = 0.001). Uterine filling defects were demonstrated in 13 of the 109 cases. There were two cases of cervical abnormalities.
CONCLUSION: The study demonstrated that tubal abnormalities were the most common findings amongst infertile women undergoing HSG and occurred predominantly in HIV-infected patients.
Keywords: hysterosalpingography; infertility; HIV; sexually transmitted diseases; fallopian tubes; radiology.
Introduction
Infertility is defined as the incapacity of a couple at reproductive age to conceive after regular and unprotected sexual intercourse within 2 years.1 It may be classified as primary infertility for a couple who never conceived or secondary infertility when occurring after a previous pregnancy.
Infertility remains a serious health concern with sociocultural implications, particularly in women of African ancestry.2 In Africa, 30% - 40% of couples present with infertility.3 The major cause of infertility in South Africa (SA) is sexually transmitted disease, which leads to genital tract pathology including endometritis and salpingitis, complicated by tubal mucosal damage and blockage. The human immunodeficiency virus (HIV) epidemic in SA over the last three to four decades has compounded the impact of sexually transmitted infections on infertility.4,5,6 However, treatment of HIV infection has been reported to reduce infertility rates.7,8
A variety of imaging techniques including hysteroscopy, ultrasonography (US), hysterosalpingography (HSG) and pelvic magnetic resonance imaging (MRI) are available to evaluate the patency of the female genital tract for the investigation of infertility. The unavailability of expertise and the costs of imaging techniques, such as MRI and diagnostic laparoscopy, make HSG the most commonly used first-line imaging technique for evaluating female infertility in district and most regional hospitals in SA.
To the best of our knowledge, there are no local reports on HSG findings in HIV-infected women with infertility. This is of importance for the KwaZulu-Natal province, which carries the highest burden of the HIV pandemic, with rates of approximately 37% in antenatal attendees.9 Therefore, the aim of this study was to report on HSG findings in a setting of high HIV infection rates.
Methods
Study design
This was a descriptive, retrospective study covering a 4-year period, from 01 January 2012 to 31 December 2016, in the Radiology Department of a Central Hospital in Durban, KwaZulu-Natal. The radiological information system of the hospital was used to obtain the relevant clinical records and imaging findings of patients referred for HSG as part of an infertility work-up during the study period. Each included patient had prior US of the pelvis and laboratory tests for ovulation. Hysterosalpingography was performed according to standard protocols, with the images reviewed by both a gynaecologist and a radiologist.10 The final reports were documented by the radiologist. The report and final images were archived in a Radiology Information Database. For the purpose of this study, both the reports and the images were re-reviewed by the author, a registrar in radiology, and by a specialist radiologist with 4 years of experience.
The socio-demographic and clinical information was recorded on a structured data sheet. The documentation of the HIV status was considered absolute criteria for inclusion. We considered the risk factor profile of women with secondary infertility as well.11 Women with incomplete clinical information, other proven causes of infertility and a history of tuberculosis or records of anti-tuberculosis treatment were excluded from the study.
All statistical analysis was performed using Statistical Package for the Social Sciences (SPSS version 25, IBM Corp, 2017). The results were expressed as mean and standard deviation. The Z-test was used for the difference between means. A p-value of < 0.05 was considered statistically significant.
Results
The records of 178 infertile women with complete information who underwent HSGs were retrieved. The mean (standard deviation [s.d.]) age and duration of infertility of the patients were 33.3 ± 4.7 years and 5.64 ± 4.1 years, respectively. Amongst them, 64.6% had primary infertility and 35.4% had secondary infertility. Hysterosalpingography reports were normal in 38.8% (69/178) of patients, whilst the remaining 61.2% patients (109/178) had at least one abnormal HSG finding. Subgroup analysis showed that 120 (67.4%) women were HIV-uninfected and 58 (32.6%) were HIV-infected. Forty-four patients were on antiretroviral therapy at the time of HSG examination, whereas three had not yet started treatment. The demographic and clinical profiles of the infertile women are presented in Tables 1 and 2.
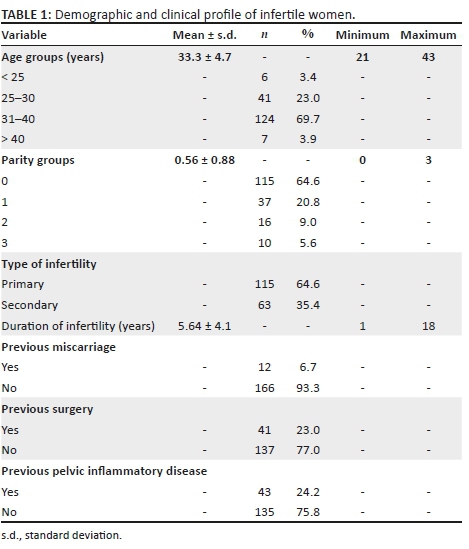
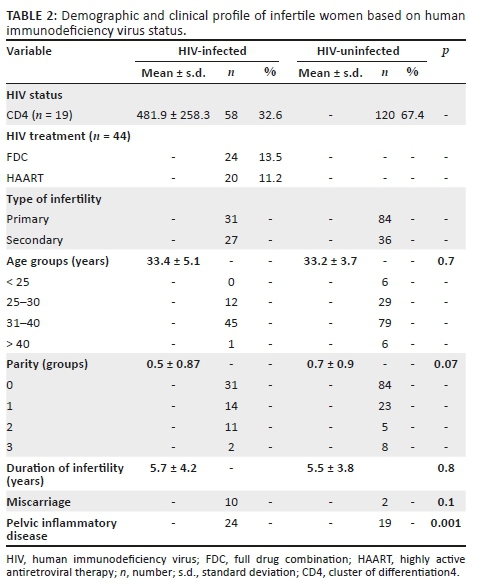
Of the 41 women who had previous pelvic surgery, 27 were HIV-uninfected and 14 were HIV-infected. The association with HIV infection was significant (p = 0.047). Forty-three (24.2%) women provided a history of pelvic inflammatory disease (PID) and 24 (55.81%) of those were HIV-infected. Pelvic inflammatory disease and HIV were also significantly associated (p = 0.001).
Sixty-three patients presented with secondary infertility before undergoing HSG. Previous caesarean delivery was performed in 29 of these patients presenting with uterine and/or tubal abnormalities at HSG. Human immunodeficiency virus infection was more frequent in the caesarean delivery group than in the vaginal delivery group (p = 0.000).
Tubal pathologies were the most common abnormalities and accounted for 79/109 (72.5%) of the abnormal findings. They presented as bilateral occlusions or unilateral tubal occlusions with hydrosalpinx. The next most common abnormality was seen in the uterine cavity, with 13 filling defects. The majority (14) of filling defects were confirmed on pelvic US as air bubbles and not considered as a pathology; 10 were submucosal fibroids and three were congenital uterine malformations. There was one uterine synechia. Cervical pathologies included elongated cervix and stenosed cervix, where the procedure was then abandoned.
Ten HIV-infected patients (17.2%) had more than one documented cause of infertility. Tubal pathologies were the only cause of infertility that was significantly associated with HIV infection (p = 0.001). The HSG findings are presented in Table 3.

Discussion
The main findings of this study showed that a substantial proportion of patients who had HSGs were HIV-infected (32.6%). The study confirmed a smaller number of HIV-infected infertile women <25 years old and a larger proportion between 25 and 40 years of age. Although infertility affects all reproductive ages, it was also not documented in any HIV-uninfected patients less than 25 years of age. In a similar study conducted by Heis et al.,12 the overall mean age was 31.5 years (s.d. 5.9 years), with maximum occurrence at 18-46 years and a mean (s.d.) infertility duration of 4 ± 3.4 years. Panti13 reported a mean age of 28.9 ± 6.5 years and a mean duration of infertility of 7.47 ± 1.6 years. Chen and Walker14 reported that the age-specific fertility rates of HIV-infected women are reduced as compared to uninfected women, except for those in the 15-19 years age range where fertility is said to be higher based on reports from many countries.
In this study, the incidence of primary infertility was higher than that of secondary infertility, which is in accordance with other studies.13,14,15 However, contradictory findings where secondary infertility was more common than primary infertility have also been documented.6,16 We did not find any significant statistical association between the duration of infertility and HIV.
The frequency of HIV infection in the study was 32.6%. This prevalence rate is much higher than previous reported values from Gabon (9.3%),17 Tanzania (18.2%)17 and SA (20%).18 The high rates of HIV are probably because KwaZulu-Natal has the highest HIV burden in SA; the rate amongst antenatal attendees is 37%.8
It should be noted that 25% of the HIV-infected infertile women in this study had not initiated anti-retroviral (ARV) treatment. Although no side effects or adverse events of HSG were noted in the study for both infected and uninfected women, the study was not designed to evaluate the complications in HIV-infected women following HSG. This might be regarded as a limitation of the study. It is plausible that any invasive procedure of the female genital tract in HIV-infected women may cause infective complications. This needs further investigation and it seems intuitive that gynaecologists initiate ARVs prior to any investigations for infertility. We only found one study in the current literature that has evaluated HSG procedures in HIVpatients.19
The results of this study revealed that 38.8% of the patients had normal HSGs; however, our finding is lower than the 49.2% reported previously in a similar study in Nigeria.8 This may be related to the HIV burden in the study sample. Other studies have recorded 16.6% and 29.1% of normal findings.13,20,21
Tubal factor infertility was seen in 79.3% of our HIV-infected patients. Some HIV-infected patients (6.2%) had more than one documented cause of infertility. Tubal factor was the only cause of infertility that was significantly associated with HIV infection (p = 0.001). Yahya et al.7 reported tubo-peritoneal factor as the most common cause of infertility (seen in 81% of HIV-infected patients) and the association as statistically significant, with a p-value of 0.048. Similarly, Adegoke et al.8 reported that tubo-peritoneal abnormalities were more common amongst infertile women infected with HIV as compared to those without HIV infection. Adesiyun et al.4 also reported a study on HSG and found that distal tubal occlusion with hydrosalpinx was mainly associated with HIV infection.
Limitations of the study
There was no follow-up of the patients to monitor any long-term complications related to the procedure. Furthermore, there was no record of the duration or initiation of ARV regimen. Many patients were excluded from the study because of a history of tuberculosis or anti-tuberculosis treatment, even though there was a concurrent positive medical history of HIV. It is important to note that the infertile women were investigated without examining their spouses; thus, it could be that their infertility is related to their partners. This is a major limitation of this study.
Conclusion
This study has shown that HSG remains an important diagnostic tool in the evaluation of the infertile women, particularly in public-sector health facilities in SA, where there is a lack of equipment, technology and expertise. Hysterosalpingograms are cheap, quick and easily accessible. We demonstrated that tubal abnormalities were the most common findings amongst infertile women undergoing HSG, occurring predominantly in HIV-infected patients.
Acknowledgements
The authors would like to thank Prof. D.P. Ramaema, Head of Radiology Department at Inkosi Albert Luthuli Central Hospital, who gave access to their Data Base System.
Competing interests
The authors have declared that no competing interests exist.
Authors' contributions
All authors contributed equally to this work.
Ethical consideration
Approval for the study was granted by the Bioethics Research Committee (BE: 406/17), University of KwaZulu-Natal, the Postgraduate Education Committee, Hospital management and the KwaZulu-Natal Department of Health.
Funding Information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.WHO. Reproductive health indicators for global monitoring. Report of the second interagency meeting. WHO/RHR/01.19. Geneva: World Health Organization, Department of Reproductive Health and Research; 2001 [ Links ]
2.Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med. 2012;9(12):1001356. https://doi.org/10.1371/journal.pmed.1001356 [ Links ]
3.Leke RJ, Oduma JA, Bassol-Mayagoitia S, Bacha AM, Grigor KM. Regional and geographical variations in infertility: Effects of environmental, cultural, and socioeconomic factors. Environ Health Perspect. 1993;101(2):73-80. https://doi.org/10.1289/ehp.93101s273 [ Links ]
4.Adesiyun AG, Ameh C, Eka A. Hysterosalpingographic tubal abnormalities and HIV infection among black women with tubal infertility in sub-Saharan Africa. Gynecol Obstet Investig. 2008;66(2):119-122. https://doi.org/10.1159/000128600 [ Links ]
5.Lash MM, Yaghamee A, Strohsnitter W, Lalwani S. Association between secondary infertility and fallopian tube obstruction on hysterosalpingography. J Reprod Med. 2008;53(9):677-680. [ Links ]
6.Mazzuca P, Caruso A, Caccuri F. HIV-1 infection, microenvironment and endothelial cell dysfunction. New Microbiol, 2016;39(3):163-173. [ Links ]
7.Yahya A, Adesiyun A, Olorukooba AA. Seroprevalence and clinical correlates of human immunodeficiency virus infection among women with infertility in North-Western Nigeria. Trop J Obstet Gynaecol. 2018;35(2):177-183. https://doi.org/10.4103/TJOG.TJOG_17_18 [ Links ]
8.Adegoke AA, Anthony E, Olumide AB, Folake O, Idowu AA. Hysterosalpingographic tubal abnormalities in retroviral (HIV) positive and negative infertile females. J Clin Diagn Res. 2013;7(1):35-38. https://doi.org/10.7860/JCDR/2012/4938.2664 [ Links ]
9.National Department of Health. Saving mothers 2011-2013: Sixth report on confidential enquiries into maternal deaths in South Africa. Fact sheet. Pretoria: National Committee for Confidential Enquiry into Maternal Deaths, Department of Health Republic of South Africa; 2015. [ Links ]
10.Chapman S, Nakielny R. Chapter 6: Aids to radiological procedures. In: Watson N, Jones H, editors. Chapman & Nakielny's guide to radiology procedures. 4th ed. London: Elsevier, 2001; p. 175-180. [ Links ]
11.Dhont N, Luchters S, Muvunyi C, et al. The risk factor profile of women with secondary infertility: An unmatched case-control study in Kigali, Rwanda. BMC Womens Health. 2011;11:32. https://doi.org/10.1186/1472-6874-11-32 [ Links ]
12.Heis M, Amarin Z, Ibrahim AY, Obeidat N, Obeidat B, Omari M. Uterine and tubal anatomical abnormalities in infertile women: Diagnosis with routine hysterosalpingography prior to selective laparoscopy. SA J Radiol. 2011;15(4):121-122. https://doi.org/10.4102/sajr.v15i4.354 [ Links ]
13.Panti AA, Sununu YT. The profile of infertility in a teaching hospital in North West Nigeria. Sahel Med J. 2014;17(1):7-11. https://doi.org/10.4103/1118-8561.129145. [ Links ]
14.Chen WJ, Walker N. Fertility of HIV-infected women: Insights from demographic and health surveys. Sex Transm Infect. 2010;86(2):22-27. https://doi.org/10.1136/sti.2010.043620 [ Links ]
15.Khetmalas SM, Kathaley MH. A study evaluation of tubal factors of infertility by hysterosalpingography and diagnostic laparoscopy. MVP J Med Sci. 2016;3(1):11-17. https://doi.org/10.18311/mvpjms/2016/v3/i1/722 [ Links ]
16.Okafor CO, Okafor CI, Okpala OC, Umeh E. The pattern of hysterosalpingography findings in women being investigated for infertility in Nnewi, Nigeria. Niger J Clin Pract. 2010;13(3):264-267. [ Links ]
17.Favot I, Ngalula J, Mgalla Z, Klokke AH, Gumodaka B, Boerma JT. HIV infection and sexual behavior among women with infertility in TANZIANIA: A hospital-based study. Int J Epidemiol. 1997;26(2):414-419. https://doi.org/10.1093/ije/26.2.414 [ Links ]
18.Statistics South Africa. Midyear population estimates 2017 [homepage on the Internet]. Department: Statistics South Africa Republic of South Africa. [cited 2017 Dec. 12] Available from: https://www.stassa.gov.za [ Links ]
19.Nwankwo NC, Akani CI. Pattern of hysterosalpingography in patients with infertility in Port Harcourt. West Afr J Radiol. 2005;12(1);15-19. https://doi.org/10.4314/wajr.v12i1.34200 [ Links ]
20.Elsie KM, Rosemary KB, Structural finding at hysterosalpingography in patients with infertility at private clinics in Kampala, Uganda. Afr Health Sci. 2004;4(3):178-181. [ Links ]
21.Onwuchekwa CR, Oriji VK. Hysterosalpingography pattern of infertility in women of reproductive age. J Hum Reprod Sci. 2017;10(3):178-184. https://doi.org/10.4103/jhrs.JHRS_121_16 [ Links ]
 Correspondence:
Correspondence:
Dolongo Onyangunga
dolongocarine@gmail.com
Received: 03 July 2019
Accepted: 14 Jan. 2020
Published: 24 Mar. 2020

