










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Journal of Radiology
On-line version ISSN 2078-6778
Print version ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.21 n.2 Johannesburg 2017
http://dx.doi.org/10.4102/sajr.v21i2.1230
CASE REPORT
Unusual complication and successful high-dose chemotherapy treatment of advanced Burkitt's lymphoma in an adult HIV-positive patient
Henrietta W.H. McGrathI; Alexander FitzhughI; Maria JavedI; Neesha RockwoodII; Farhat KazmiI
IDepartment of Radiology, Chelsea and Westminster Hospital, United Kingdom
IIDepartment of Infectious Diseases and HIV, Chelsea and Westminster Hospital, United Kingdom
ABSTRACT
Adult Burkitt's lymphoma emerged as an AIDS-defining condition in the 1980s. We describe a case of HIV-associated adult Burkitt's lymphoma diagnosed and treated with high-dose chemotherapy in our institution, complicated by unusual bilateral renal vein tumour thrombi and tumour lysis syndrome. We believe this unique case highlights the need for early recognition of current and potential complications on staging computed tomography imaging, as well as successful use of a high-dose chemotherapy regimen.
Introduction
Burkitt's lymphoma is a highly proliferative B-cell neoplasia first described as a childhood illness endemic to malaria areas of Africa. Following the emergence of HIV in the 1980s, its significance as an AIDS-defining condition was soon recognised with a far more aggressive natural history, and its significance as an AIDS-defining condition was demonstrated.
HIV-associated lymphomas remain a significant cause of morbidity and mortality, especially within sub-Saharan Africa, and familiarity with imaging findings is essential in suggesting the initial diagnosis, identifying complications and assessing response to treatment. We present a case of adult Burkitt's lymphoma with advanced disease.
Case report
A 49-year-old man presented near cardiac-arrest with a 4-week history of weight loss, night sweats, back pain and difficulty walking.
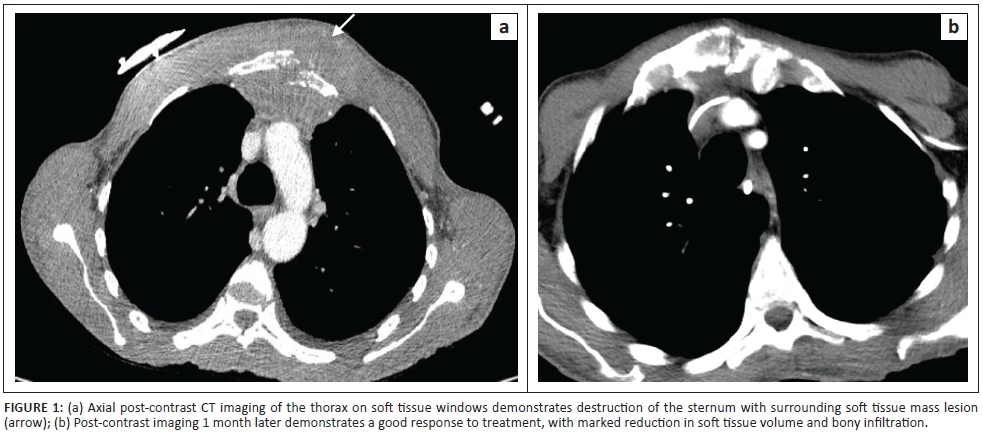
He was cachectic (42 kg), with massive hepatomegaly and a large sternal soft tissue mass (Figure 1). Blood tests demonstrated acute renal failure (creatinine 168 µmol/L, lactate 22 mmol/L, calcium 2.84 and phosphate 3.1 mmol/L).
A new HIV-1 diagnosis was made (CD4 lymphocyte count 3 cells/µL, viral load 912 376 copies/mL). Epstein-Barr viral titres were 21 620 500 copies/mL.
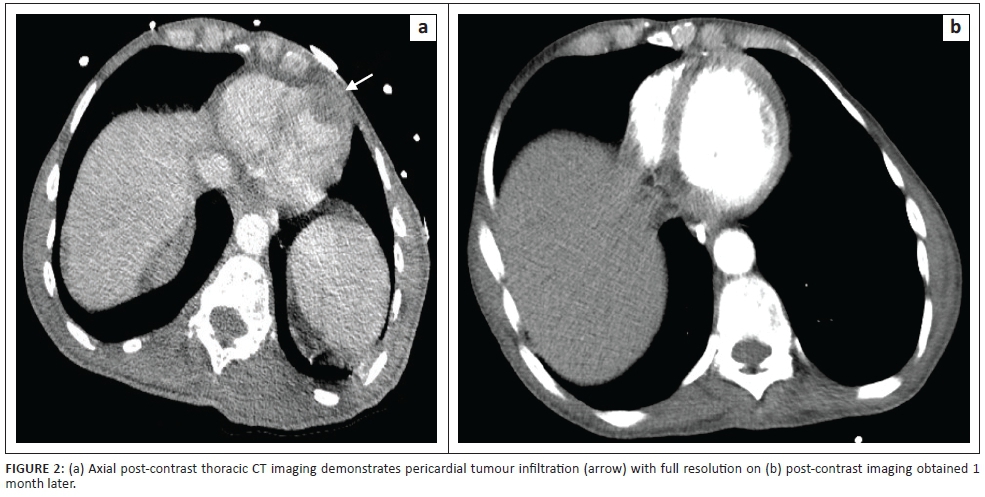
Computed tomography (CT) suggested Burkitt's lymphoma with disease affecting the lungs, heart (Figure 2), sternum, liver, vertebrae and kidneys with bilateral renal vein tumour thrombi. Biopsy of the sternal mass demonstrated diffuse lymphoid infiltrates of skeletal muscle in a starry sky pattern, in keeping with Burkitt's lymphoma.
The patient was commenced on antiretroviral therapy including Descovy and Dolutegravir, with a Rituximab-CODOX-M/IVAC chemotherapy regimen.1
His initial management was complicated by tumour lysis syndrome,2 pseudomonas bacteraemia and cytomegalovirus infection of the gastrointestinal tract, all successfully treated.
Subsequent CT imaging revealed an excellent treatment response, regression of extensive hepatic and renal infiltration and resolution of bilateral renal vein tumour thrombi, allowing anticoagulation to be discontinued.
Discussion
First reported in 1958, Burkitt's lymphoma can be usefully subdivided into endemic, sporadic (without geographical limitation) and immunodeficiency-associated. Predominantly a disease of childhood (representing 40% of paediatric non-Hodgkin's lymphomas3), Burkitt's lymphoma represents fewer than 5% of lymphoma affecting adults and carries a worse prognosis with advancing age (5-year survival between 50% and 65% without central nervous system [CNS] involvement at presentation3). Our patient presented at the age of 49 with CT-stage IV HIV-associated immunodeficient Burkitt's lymphoma, with a high lactate on admission, an additional poor prognostic marker (2-year survival of 63% vs. 86% of patients with a normal serum lactate level).3
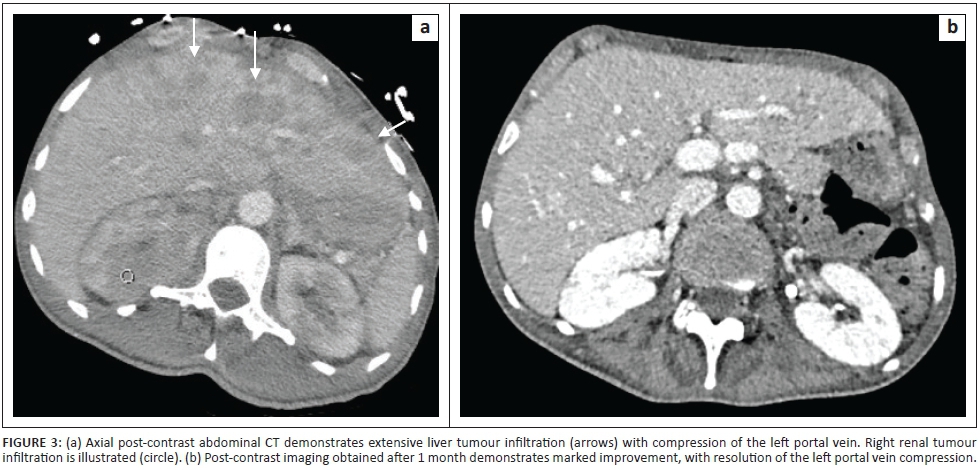
While tissue diagnosis remains essential, CT staging (using both St Jude/Murphy's and Ann Arbor scoring systems4) guides treatment. Early recognition of extensive intra-abdominal involvement [renal and hepatic (Figure 3)] helped the clinicians anticipate and promptly treat tumour lysis syndrome. Most centres commence treatment within 24 h - 48 h, and CT should not delay pursuit of a tissue diagnosis or treatment.
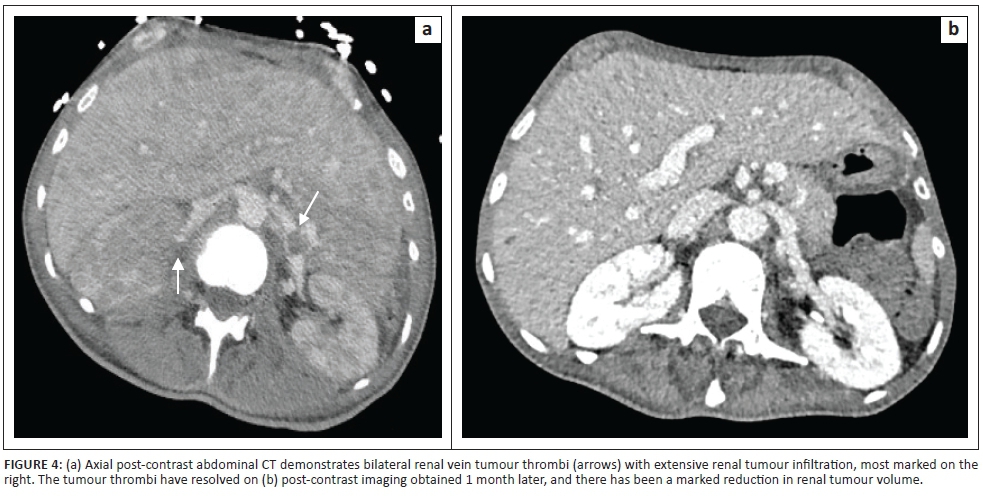
Bilateral renal vein tumour thrombosis is an uncommon complication, not typically seen in lymphoma, necessitating anticoagulation (Figure 4).5,6 CT confirmed resolution, allowing a return to thromboprophylaxis alone.
Disease confined to the abdomen is described in 50%,7 usually hepatosplenomegaly which may be observed on ultrasound. Abdominal and pelvic CT is beneficial for further characterisation and better demonstrates potential involvement of the distal small bowel, caecum and appendix.8
Involvement of the central nervous system heralds a poor prognosis (5-year survival drops to < 30%); our patient underwent CT and magnetic resonance imaging (MRI) brain which did not demonstrate CNS disease. Bilateral cavernous sinus involvement has been described in an immunocompetent individual with confirmed Burkett's lymphoma,9 diagnosed using CT and multi-parametric MRI; although the patient responded to first line cyclophosphamide-vincristine chemotherapy, CNS disease recurred and the patient died after 11 months.
Involvement of the distal urinary tract, testicular involvement, pancreatic disease and jaw involvement has been described in adults. Positron emission tomography-computed tomography (PET-CT) has been utilised to identify additional sites of disease, with a low false negative rate. However, a high false positive rate has been noticed within the immunosuppressed population attributed to concurrent opportunistic infections.
Conclusion
We have described the imaging findings of Burkitt's lymphoma affecting an immunodeficient adult, emphasising the need for prompt diagnosis. CT delineated our patient's disease, subsequently confirming an excellent response to high-dose chemotherapy, and identified current (renal vein tumour thrombus) and potential complications (tumour lysis syndrome). Radiologists should employ alternative modalities (ultrasound and MRI) to investigate extra-abdominal disease foci where clinically appropriate.
Acknowledgements
Competing interests
The authors declare they have no personal or financial relationship which may have influenced them in writing this article.
Authors' contributions
H.W.H.M., A.F. and N.R. wrote the case report. M.J. assisted with radiological images and editing. F.K. supervised the case report.
References
1. Alwan F, He A, Montoto S, et al. Adding rituximab to CODOX-M/IVAC chemotherapy in the treatment of HIV-associated Burkitt lymphoma is safe when used with concurrent combination antiretroviral therapy. AIDS. 2015;29(8):903-910. https://doi.org/10.1097/QAD.0000000000000623 [ Links ]
2. Wilson FP, Berns JS. Tumor lysis syndrome: New challenges and recent advances. Adv Chronic Kidney Dis. 2014;21(1):18-26. https://doi.org/10.1053/j.ackd.2013.07.001 [ Links ]
3. Divine ́M, Casassus P, Koscielny S, et al. Burkitt lymphoma in adults: A prospective study of 72 patients treated with an adapted pediatric LMB protocol. Ann Oncol. 2005;16:1928-1935. https://doi.org/10.1093/annonc/mdi403 [ Links ]
4. Perkins AS, Friedberg JW. Burkitt lymphoma in adults. Am Soc Haematol. 2008; 341-348. https://doi.org/10.1182/asheducation-2008.1.341 [ Links ]
5. Wagner JR, Honig SC, Siroky MB. Non-Hodgkin's lymphoma can mimic renal adenocarcinoma with inferior vena caval involvement. Urology. 1993;42(6):720-723; discussion 723-724. https://doi.org/10.1016/0090-4295(93)90543-J [ Links ]
6. Samlowski EE, Dechet C, Weissman A, Samlowski WE. Large cell non-Hodgkin's lymphoma masquerading as renal carcinoma with inferior vena cava thrombosis: A case report. https://doi.org/ [ Links ]
7. Molyneux EM, Rochford R, Griffin B, et al. Burkitt's lymphoma. Lancet. 2012;379:1234-1244. https://doi.org/10.1016/S0140-6736(11)61177-X [ Links ]
8. Satishchandra H, Sridhar AS, Pooja BP. Imaging of Burkitt's lymphoma-abdominal manifestations. J Cancer Res Ther. 2013;9(1):128-130. https://doi.org/10.4103/0973-1482.110383 [ Links ]
9. Boukobza M, Brouland J-P. Burkitt's lymphoma with bilateral cavernous sinus involvement: A case report. 2016;2016(2016), Article ID 253994. https://doi.org/10.5171/2016.253994 [ Links ]
 Correspondence:
Correspondence:
Henrietta McGrath
henrietta.mcgrath@chelwest.nhs.uk
Received: 03 June 2017
Accepted: 17 Aug. 2017
Published: 14 Nov. 2017


{kind=link}
{kind=link}
{kind=link}
{kind=link}