










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Journal of Radiology
versão On-line ISSN 2078-6778
versão impressa ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.20 no.1 Johannesburg 2016
http://dx.doi.org/10.4102/sajr.v20i1.940
REVIEW ARTICLE
http://dx.doi.org/10.4102/sajr.v20i1.940
Paediatric interventional radiology
Gulraiz Chaudry
Division of Interventional Radiology, Boston Children's Hospital, United States
ABSTRACT
Paediatric interventional radiology (IR) is a rapidly developing subspecialty, seeking to meet the increasing demand for image-guided minimally invasive procedures. The wide range of procedures performed and the conditions treated reflect the varying ages and complexity of the patient population. This article reviews the various interventional procedures performed and the unique challenges faced in paediatric IR. Conditions, such as vascular anomalies, that are primarily treated by paediatric interventional radiologists are highlighted. The requirements for establishing a paediatric IR practice are reviewed, as are the challenges facing the future development of the specialty.
Introduction
Paediatric interventional radiology (IR) is a young but rapidly expanding subspecialty. The use of image guidance for performing some minimally invasive procedures was first suggested in the 1970s, but the range and complexity of procedures performed by paediatric interventionalists principally expanded in the 1980s and 1990s.1 The field was initially slow to develop due to limited training in performing image-guided procedures in children and the challenge of adapting equipment and techniques for use in small children.2 Recently, however, the need for paediatric IR has been recognised at local and national levels, with increased funding and provision of training programs. The field has now developed beyond offering an alternative to more invasive surgical techniques by introducing new and innovative therapy that has transformed the treatment of many patients.
Paediatric interventional radiology procedures
The range of procedures performed in paediatric institutions often reflect local or institutional practice and availability of interventionalists. Box 1 summarises the types of procedures commonly performed by paediatric IR physicians, although the numbers of these procedures performed can vary significantly between institutions, particularly if traditionally performed by non-radiologists.
Vascular access
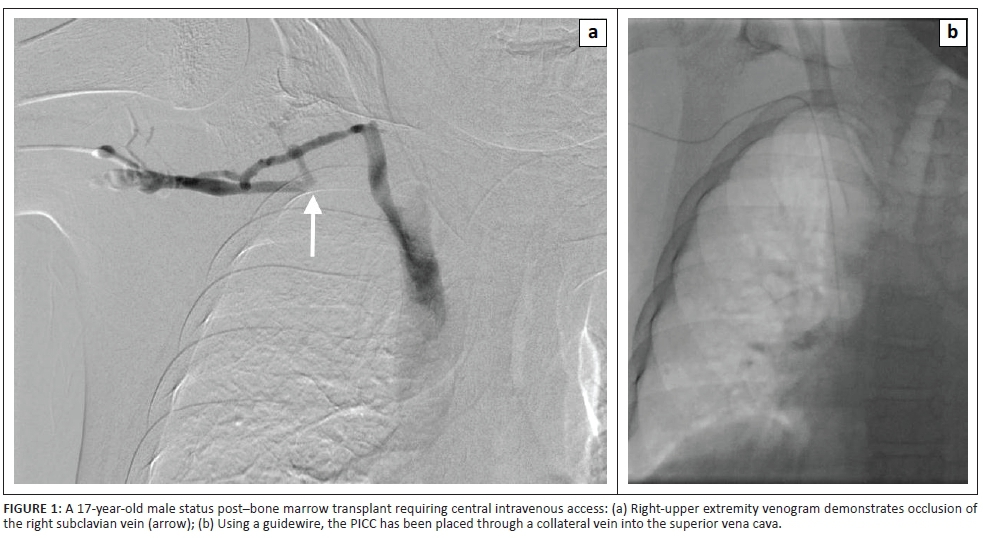
Sonographic guidance and interventional procedures have long been shown to offer the most reliable and safe method of central venous access.2Improvements in sonographic technology and types of machines available have resulted in increasing use of sonography for vascular access by non-radiologists, including vascular access teams and intensive care units. Interventional radiologists, however, generally possess a greater level of expertise in catheter placement and management of complications, including management of venous stenosis (Figure 1). Active involvement of IR departments in interdisciplinary vascular access teams ensures that children receive the access (peripherally inserted central catheter [PICC], central venous catheter, port-a-cath, etc.) that most appropriately addresses their clinical needs.2
Biopsy
Percutaneous image-guided needle biopsy is now the standard for solid organ biopsies in most institutions. The most commonly biopsied organs are the kidneys and liver, with the biopsies performed percutaneously under sonographic guidance. This technique has been demonstrated to be safe and effective with high diagnostic yield and very low complication rate.3 Transjugular liver biopsies are not commonly performed as these can be particularly challenging in smaller children and often yield small and fragmented samples.
Image-guided needle biopsies of suspected tumours has also increased in recent years (Figure 2). The vast majority of solid organ tumours can be biopsied with sonography alone, with CT and fluoroscopic guidance reserved for bone and lung tumours.2 The use of a coaxial technique allows multiple cores to be obtained through a single puncture and allows the tract to be embolised, reducing the risk of tumour seeding and haemorrhage.2,3,
Drainage
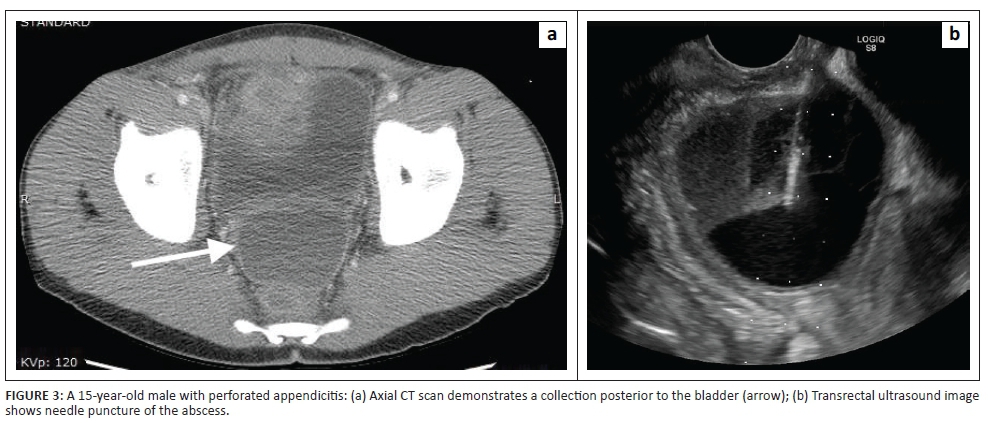
Percutaneous drainage of abdominal abscesses is the standard in children. Early surgery in cases of perforated appendicitis with abscess formation is associated with increased morbidity due to haemorrhage, infection and adhesion formation. Interventional techniques, including percutaneous and transrectal drainage of pelvic abscesses, significantly decrease the complication rates in these children (Figure 3).4 Aspiration and drainage of ascites and pleural effusions can be safely performed with sonographic guidance, even in the smallest infants. Placement of pigtail drains into empyemas and lung abscesses is safe and effective and offers a minimally invasive alternative to video-assisted thoracoscopic surgery (VATS), with similar success rates.5
Enteric access and intervention
Percutaneous image-guided retrograde or anterograde placement of gastrostomy and gastrojejunostomy tubes is now the standard in some large paediatric institutions, although there remains considerable local variability in practice. Radiologic percutaneous gastrostomy tube placement is a safe and minimally invasive way of providing enteral nutrition in children of all sizes, including infants with significant coexisting morbidities such as cardiac disease.6 Maintenance and exchange of gastrojejunostomy tubes are also commonly performed by interventional radiologists, as skills with guidewires and catheters greatly facilitate accurate positioning of post-pyloric feeding tubes.
Image-guided tumour therapy
Paediatric interventional oncology remains a small part of the paediatric IR practice when compared to adults. This is primarily due to the relative rarity of paediatric cancers, and the fact that standardised treatment protocols are determined by cooperative oncology groups. In addition, the extra protection afforded to children as a vulnerable population limits the introduction of new treatments and devices.7 Standardised treatment regimens have increased the 5-year survival rate to over 80% in many solid tumours, but occasionally regional interventional tumour therapy is utilised to increase the effectiveness of existing treatment or for palliation.8
Bland embolisation with coils, liquid agents or particles is occasionally required, such as in cases of rapidly involuting congenital haemangiomas of the liver, with cardiac decompensation resulting from arteriovenous shunting. Intra-arterial chemotherapy and radioembolisation have also been used in a small percentage of cases of hepatoblastoma or hepatocellular carcinoma.8
The most common ablative procedure performed in children is radiofrequency ablation of osteoid osteoma. Using fluoroscopy and/or CT, the nidus of the osteoid osteoma is accessed and a radiofrequency probe inserted to ablate the nidus (Figure 4). This can often result in immediate improvement of the chronic pain experienced by these children. Other ablative modalities, such as cryoablation, have also been more recently introduced to treat conditions such as desmoids and fibroadipose vascular anomalies.
Angiography and intervention
Improvements in non-invasive vascular imaging in recent years have resulted in decreased need for catheter angiography as a diagnostic tool. In our institution, like many others, arteriography is predominantly performed as a precursor to further interventions such as angioplasty and embolisation. The safety and efficacy of renal angioplasty has been established in children with refractory hypertension secondary to renal artery stenosis.9
Non-operative management is the standard of care in children with blunt solid organ trauma. However, as with adults, transcatheter arterial embolisation can play a key role in the treatment of traumatic injuries when conservative observation has failed, providing effective control of haemorrhage with a low complication rate.10
Catheter-directed thrombolysis
Catheter-directed thrombolysis (CDT) is considered to be the treatment of choice in children with extensive deep venous thrombosis.11 Indications include Paget-Schroetter disease (thoracic outlet syndrome) (Figure 5), May-Thurner syndrome, iliofemoral and Inferior vena cava (IVC) thrombosis. An IVC filter can also be placed in selective cases, followed by a combination of local thrombolysis through an infusion catheter and mechanical thrombectomy. A variety of devices can be used for the latter technique, including Angiojet rheolytic system (Possis Medical, Minneapolis, MN) or the Trellis-8 (Bacchus Vascular, Santa Clara, CA) and Arrow-Trerotola devices (Arrow International, Reading, PA).
Catheter-directed arterial thrombolysis is also indicated in a select group of patients, helping restore flow towards end organs and threatened limbs.
Vascular anomalies
Vascular anomalies can be broadly classified into tumours and malformations. Tumours can spontaneously involute or respond to medical therapy. In contrast, malformations usually require invasive treatment. Over the past 20 years, the treatment of vascular anomalies has been revolutionised by the use of interventional techniques, which now form the primary method of treatment in the majority of malformations.12 However, the care of these patients should be directed by an interdisciplinary team to ensure optimal treatment for individual patients. In our institution, all cases are directed through the vascular anomalies centre with physicians from 14 different specialties providing input if required.
Slow-flow (venous and lymphatic) malformations are predominantly treated with percutaneous sclerotherapy, with the choice of sclerosant determined by the type of malformation (Figure 6). Arteriovenous malformations are fast-flow anomalies consisting of a network of vessels forming a nidus, which connects arteries and veins without an intervening capillary network. These malformations can be technically challenging to treat, requiring a combination of arterial and venous intervention. Transvenous embolisation of large dominant draining veins offers the best hope of a successful outcome.12
Combined vascular anomalies syndromes, such as Klippel-Trenaunay syndrome and CLOVES syndrome (Congenital Lipomatous Overgrowth, Vascular Malformations, and Epidermal Nevi [and spinal and/or skeletal anomalies]), are sometimes associated with persistence of embryonic superficial veins, such as the lateral marginal vein (of Servelle). These veins are typically incompetent and can become significantly enlarged over the course of childhood; in addition to pain, these are also associated with a significantly increased risk of thromboembolism. Endovenous laser ablation of these veins in childhood can obliterate these, promoting the development of the deep venous system.13 Bleeding or leaking lymphatic vesicles are also common in these children, which can be photoevaporated with CO2 laser.
Biliary interventions
Biliary interventions in children are most commonly performed to manage complications of hepatic transplantation. Less common indications include cholangitis, cholecystitis or traumatic biliary leaks. Percutaneous transhepatic cholangiography is often the first step, with a peripheral duct accessed under sonographic guidance. This can be followed by angioplasty of ductal stenosis or internal-external biliary drainage (Figure 7). Gangrenous cholecystitis may necessitate transhepatic cholecystostomy drain placement. Percutaneous biliary drainage can also be used to divert biliary flow and allow healing of a biliary leak.14
Genitourinary interventions
In addition to renal biopsies, the most common Genitourinary (GU) intervention is placement of percutaneous nephrostomy tubes. Indications include posterior urethral valves, pyelo-ureteric junction obstruction, pyonephrosis and renal calculi. The procedures are predominantly performed under a combination of sonographic and fluoroscopic guidance. Occasionally, the anterograde placement of ureteric stents is also required following nephrostomy tube placement.1
Conclusions and the future of paediatric interventional radiology
The future of paediatric IR appears to be bright. Children's hospitals are increasingly recognising the necessity of having appropriately trained paediatric interventional radiologists. The main challenges to the growth of the specialty are the availability of dedicated paediatric IR fellowships and standardisation of training. Given the significant variability in local practice, trainees completing a fellowship can currently emerge with a strikingly different set of skills depending on the training hospital.15 In the future, it is likely that a specific set of skills will be mandated for all trainees completing fellowships, which may require elective time spent at other children's hospitals or adult institutions.
The key to creating a successful IR division lies in having the right number and mix of essential personnel. An IR team should include a radiation technologist (radiographer) with an understanding of optimal ways to reduce radiation in children, a paediatric nurse comfortable with administering sedation, a nurse practitioner and/or physician assistant and an anaesthesiologist comfortable with the particular demands of paediatric IR procedures. Inadequate facilities, including sharing of rooms with other specialties, can often hinder the development of IR in a hospital; dedicated commitment by department and hospital administrators is therefore required.
The experience at our institution and other children's hospitals has been that once a safe and reliable service can be provided and relationships developed with other specialties, IR can become an integral part of any children's hospital.
Acknowledgements
Competing interests
The author declares that he has no financial or personal relationships which may have inappropriately influenced him in writing this article.
References
1. Roebuck D. Paediatric interventional radiology. Pediatr Radiol. 2009;39 Suppl 3: 491-495. http://dx.doi.org/10.1007/s00247-009-1245-2 [ Links ]
2. Barnacle AM. Interventional radiology in infancy. Early Hum Dev. 2014;90(11): 787-790. http://dx.doi.org/10.1016/j.earlhumdev.2014.08.017 [ Links ]
3. Govender P, Jonas MM, Alomari AI, et al. Sonography-guided percutaneous liver biopsies in children. AJR Am J Roentgenol. 2013;201(3):645-650.http://dx.doi.org/10.2214/AJR.12.9802 [ Links ]
4. Brown C, Kang L, Kim ST. Percutaneous drainage of abdominal and pelvic abscesses in children. Semin Intervent Radiol. 2012;29(4):286-294.http://dx.doi.org/10.1055/s-0032-1330062 [ Links ]
5. Hogan MJ, Coley BD. Interventional radiology treatment of empyema and lung abscesses. Paediatr Respir Rev. 2008;9(2):77-84; quiz 84.http://dx.doi.org/10.1016/j.prrv.2007.12.001 [ Links ]
6. Sy K, Dipchand A, Atenafu E, et al. Safety and effectiveness of radiologic percutaneous gastrostomy and gastro jejunostomy in children with cardiac disease. AJR Am J Roentgenol. 2008;191(4):1169-1174. http://dx.doi.org/10.2214/AJR.07.3655 [ Links ]
7. Hoffer FA. Interventional oncology: The future. Pediatr Radiol. 2011;41 Suppl 1: S201-6. http://dx.doi.org/10.1007/s00247-011-1990-x [ Links ]
8. Roebuck DJ. Paediatric interventional oncology. Canc Imag. 2010;10(1A):S27-34. http://dx.doi.org/10.1102/1470-7330.2010.9089 [ Links ]
9. Kari JA, Roebuck DJ, McLaren CA, et al. Angioplasty for renovascular hypertension in 78 children. Arch Dis Child. 2015;100(5):474-478.http://dx.doi.org/10.1136/archdischild-2013-305886 [ Links ]
10. Vo NJ, Althoen M, Hippe DS, Prabhu SJ, Valji K, Padia SA. Pediatric abdominal and pelvic trauma: Safety and efficacy of arterial embolization. J Vasc Interv Radiol. 2014;25(2):215-220. http://dx.doi.org/10.1016/j.jvir.2013.09.014 [ Links ]
11. Kukreja K, Vaidya S. Venous interventions in children. Tech Vasc Interv Radiol. 2011;14(1):16-21. http://dx.doi.org/10.1053/j.tvir.2010.07.005 [ Links ]
12. Alomari A, Dubois J. Interventional management of vascular malformations. Tech Vasc Interv Radiol. 2011;14(1):22-31.http://dx.doi.org/10.1053/j.tvir.2010.07.006 [ Links ]
13. King K, Landrigan-Ossar M, Clemens R, Chaudry G, Alomari AI. The use of endovenous laser treatment in toddlers. J Vasc Interv Radiol. 2013;24(6): 855-858. http://dx.doi.org/10.1016/j.jvir.2012.12.023 [ Links ]
14. Racadio JM, Kukreja K. Pediatric biliary interventions. Tech Vasc Interv Radiol. 2010;13(4):244-249. http://dx.doi.org/10.1053/j.tvir.2010.04.007 [ Links ]
15. Lord DJ. The practice of pediatric interventional radiology. Tech Vasc Interv Radiol. 2011;14(1):2-7. http://dx.doi.org/10.1053/j.tvir.2010.07.002 [ Links ]
 Correspondence:
Correspondence:
Gulraiz Chaudry
gulraiz.chaudry@childrens.harvard.edu
Received: 16 Sept. 2015
Accepted: 07 Apr. 2016
Published: 29 June 2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}