










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Journal of Radiology
versão On-line ISSN 2078-6778
versão impressa ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.19 no.2 Johannesburg 2015
http://dx.doi.org/10.4102/sajr.v19i2.899
ORIGINAL RESEARCH
The role of cardiac CT angiography in the pre- and postoperative evaluation of tetralogy of Fallot
Ebrahim BanderkerI; Elias PretoriusII; Rik de DeckerIII
IDepartment of Diagnostic Radiology, Red Cross War Memorial Children's Hospital, University of Cape Town, South Africa
IIDepartment of Diagnostic Radiology, Tygerberg Hospital, Stellenbosch University, South Africa
IIIDivision of Cardiology, Department of Paediatrics and Child Health, Red Cross War Memorial Children's Hospital, University of Cape Town, South Africa
ABSTRACT
Tetralogy of Fallot (TOF) is the first described and most common cyanotic congenital heart anomaly that generated the first successful surgical palliation procedure and definitive intracardiac repair. Classical TOF comprises the four typical features of right ventricular outflow tract obstruction (RVOTO), right ventricular hypertrophy (RVH), ventricular septal defect (VSD) and aortic dextroposition. Complex forms of the condition include TOF associated with absent pulmonary valve and TOF with pulmonary atresia (TOF-PA) with or without major aortopulmonary collateral arteries (MAPCAs). The pathophysiological understanding that the tetrad is basically the sequel of a singular abnormality of infundibular malformation, with anterior deviation of the infundibular septum, had major surgical consequences that improved survival. Diagnostic and functional imaging play a key role in the clinical and surgical management of patients with TOF. We revisit the role of traditionally employed imaging modalities (echocardiography and cardiac catheterisation) only briefly as these remain within the domain of cardiology practice. The emphasis of the present review is to outline the role of cardiac computed tomographic angiography (CTA) in the evaluation of TOF, with special reference to the technical considerations and best practice recommendations. Cardiovascular magnetic resonance imaging (CMR) is addressed only in passing, as this service is not currently available at our institution.
Introduction
Maude Abbott, variously known as the 'Queen of Canadian Cardiology' and 'The Beneficent Tornado', first coined the now familiar term of tetralogy of Fallot (TOF) in 1924.
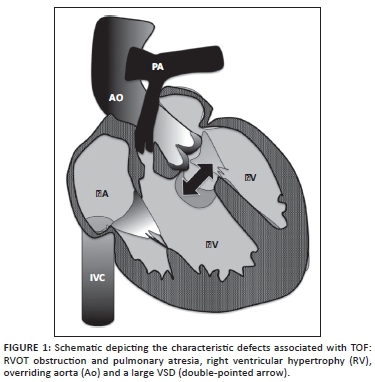
The earliest reports of the anomaly are, however, attributed to Niels Stensen (1671), Edouard Sandifort (1777) and William Hunter (1784), amongst many others. Etienne-Louis Arthur Fallot published five serialised reports in the Marseille Medical in 1888 in which he described his now famous 'blue malady'. Whilst Fallot described the classical tetrad of pulmonary outflow tract obstruction, ventricular septal defect (VSD), aortic override and right ventricular hypertrophy (RVH) (Figure 1), Stella Van Praagh in 1970 attributed the anomaly to a single defect of pulmonary valve and subpulmonary infundibular malformation, the so-called 'monology of Stensen'.1 The diagnostic and surgical consequences of this realisation have resulted in improved long-term patient survival.
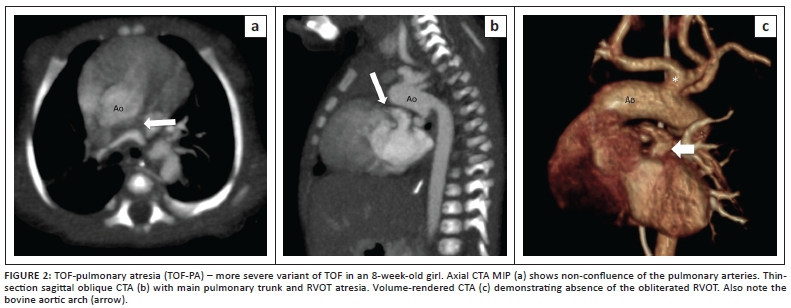
The era of clinicophysiological understanding in cardiology, between 1940 and 1970, drew special attention to the need for accurate imaging of the complex and variable pulmonary blood flow that exists in the more severe form of TOF such as tetralogy of Fallot with pulmonary atresia (TOF-PA) (Figure 2).
Imaging modalities used in TOF
The objectives of imaging are addressed in Box 1.
Whilst diagnostic paradigms for the evaluation of congenital heart disease (CHD) may be institution specific, echocardiography remains the primary diagnostic modality of choice worldwide.2 Echocardiography has wide appeal on account of its accessibility, portability, favourable cost, lack of harmful radiation and extensive experience of use. Serious limitations relate mainly to the small acoustic window that sometimes precludes the evaluation of certain anatomical structures such as the ascending aorta, right ventricle (RV) size and function, aberrant coronary anatomy, pulmonary arteries and major aortopulmonary collateral arteries (MAPCAs). Ancillary diagnostic tests are requested in the small number of cases where echocardiography fails to answer specific questions.
The role of cardiac catheterisation as the gold-standard modality for the assessment of intra-cardiac pressures, coronary artery anatomy, branch pulmonary arteries and MAPCAs is well established. Its invasive nature, prolonged sedation-anaesthesia, high cost and ionising radiation burden, however, limit its utility to a carefully selected number of cases, including instances where catheter-based intervention such as balloon dilatation and stenting of the pulmonary arteries or right ventricular outflow tract (RVOT) is anticipated.
Cardiovascular magnetic resonance imaging (CMR) offers significant advantages over the traditional imaging modalities of echocardiography and X-ray angiography, providing detailed assessment of cardiac and extra-cardiac morphology, functional analysis (RV size and function, pulmonary valve competence, pulmonary arterial flow) without radiation or iodinated contrast agents, and is suitable for numerous longitudinal follow-ups. In resource-limited environments such as ours it is expensive, however, the imaging times are long (requiring lengthy sedation and anaesthesia), and the post-processing is time-consuming. Other disadvantages include artefacts from non-MR-compatible implants, poor evaluation of lungs and airways, and the risk of nephrogenic systemic sclerosis with gadolinium-based products.
The role of cardiac CT angiography in TOF
Overview
Modern-generation multi-detector computed tomography (MDCT) allows fast imaging with very short acquisition times (often within a single breath hold) that translates into superior spatial and temporal resolution from diminished motion artefact. Its widespread availability in institutions that perform cardiac surgery offers greater accessibility at relatively reduced cost compared with CMR. Flexibility in CT protocols based on patient age, suspected cardiac defect, anticipated type of surgical repair, level of patient co-operation and the need for functional assessment further adds to its appeal. Strategies for radiation dose sparing, via carefully selected paediatric adaptive CT protocols, have gone a long way to alleviating radiation-related anxieties. Whilst its utility in the structural and functional assessment of the heart is without doubt, cardiac CT angiography (CTA) has its principle strength in the evaluation of the extra-cardiac anatomy. Its complementary use with echocardiography frequently obviates the need for invasive cardiac catheterisation of the haemodynamically unstable infant. The objectives of imaging in TOF are most often more than adequately satisfied with echocardiography alone,2 and cardiac CTA should only be employed as an ancillary tool for specific indications.
Cardiac CTA protocols
Patient preparation
The procedure is precluded and contra-indicated by iodine allergy. The laterality of the aortic arch needs to be established from the echocardiography report so as to determine the opposite cubital fossa for intravenous access. A large-bore peripheral IV cannula, at least a 22G, should be used to accommodate the large-volume, high-pressure contrast injection. A 20G cannula is preferred when the patient is >3 years of age or if ECG-synchronised CT is planned. Pharmacological heart rate manipulation using beta blockade is sometimes necessary in ECG-gated studies (see later). Preparations for sedation or anaesthesia should be made as per local protocol. Medical personnel skilled in the management of cardiac emergencies must accompany the patient.
Contrast agents
A volume of 2 ml/kg bodyweight of non-ionic iodinated contrast agent is administered through a large bore IV cannula at a rate of 2 ml/second via a power injector. A right arm injection is preferred in a known left-sided aortic arch. We employ a bolus tracking technique with the region of interest (ROI) placed within the descending thoracic aorta, at the level of the carina, and scan threshold set at 150 Hounsfield units (HU). Scan trigger after a fixed delay of 12 seconds for a peripheral line or 8 seconds for a central line, can also be used but is less favored.3 A volume of 10 ml - 15 ml of contrast saline solution (50% dilution) is utilised in a bolus chasing technique to dilute contrast within the right heart and improve contrast within the cardiac chambers.
Non-ECG-synchronised and ECG-synchronised cardiac CT
Non-ECG synchronised CT
Non-gated CT combined with echocardiography is sufficient in the structural and functional evaluation of most congenital heart conditions. Thicker detector collimation and a pitch of greater than 1 (typically 1-1.5) allows fast acquisition at the expense of superior spatial resolution. The evaluation of small cardiac defects and the coronary structures is further compromised by motion artefact. It has, however, been reported that 82% of the origins and proximal segments of the coronary arteries are in fact evaluable with non-ECG-synchronised CT.4 Furthermore, the radiation dose, defined by the dose length product, is typically less than 1 mSv.3
ECG-synchronised CT Prospective gating
This technique utilises unique cone beam reconstruction5 following 'step-and-shoot' non-spiral data acquisition with an effective pitch of 1. Imaging occurs during a user-selected brief period of the R-R interval, that is radiation exposure only during specifically determined periods of diastole. Hence the imaging is forward looking (prospective) and based on R-wave timing. Heartbeat irregularities are compensated for using 'padding' - the addition of an imaging window around the anticipated beam-on time. Image quality is enhanced during this technique by the fact that there is no table motion during imaging.
The disadvantages of prospective gating include longer acquisition time - for a 64-slice MDCT, the 4 cm table motion during the beam-off time takes about 1 second every alternate beat - resulting in greater propensity for motion artefact. Single sector gating is also limited to heart rates less than 75 BPM. Imaging during a small portion of the R-R interval does not allow functional assessment related to wall motion, valve motion or the calculation of ejection fractions.
Retrospective gating
Retrospective gating, on the other hand, employs spiral scanning with table motion and uses a low pitch (typically 0.2-0.26), resulting in over scanning. The imaging is hence gapless. The technique uses backward measurement of the R-wave and the beam is turned on throughout the R-R interval. This allows functional assessment.
Despite employing radiation dose-sparing techniques such as beam intensity modulation (see later), radiation dose to the patient is in the order of 8-19 mSv.6 Superior image quality with artefact-free visualisation of the coronary arteries, even at elevated heart rates, comes at the expense of increased radiation. Retrospective gating increases radiation exposure by 77% over prospectively gated studies.6 Two further studies have shown the radiation burden to increase by 50% and 83% respectively.7,8
Strategies for radiation dose reduction
Radiation-sparing techniques must always be fastidiously implemented, in accordance with the broader principles of ALARA (as low as reasonably achievable) and the 'image gently' campaign, as advocated by the South African Society of Paediatric Imaging (SASPI). The lifetime cumulative radiation dose is of particular importance in vulnerable children with genetic-, sex- and age-related increased radiation susceptibility. In the domain of congenital heart disease imaging, where longitudinal follow-up may be lifelong, radiation consciousness assumes even greater significance.
The process ensues with the appropriate selection of CT protocols where the lowest possible radiation is employed without losing detail. Functional cardiac CT is not a priority as function is most often adequately determined at echocardiography. ECG-synchronised cardiac CT should only be performed in very specific indications such as when detailed coronary artery anatomy beyond its origins is needed. Even then, prospective gating should be preferred.
The need for repeat studies must also be carefully considered, as echocardiography is most often sufficient.
Radiation dosage is directly proportional to the volume of patient scanned. Meticulous attention to Z-axis (cranio-caudal length) limits, to incorporate only the anatomy of interest and relevant adjacent structures, can result in a radiation dose saving of 0.7 mSv per centimeter.3 Fine-tuning of kVp and tube current according to paediatric adaptive protocols based on body weight will also result in dose reduction.
ECG-based tube current modulation3 is a technique used to diminish radiation dose when retrospective ECG-synchronisation is required for functional imaging. Reduced current of between 4% and 20% is used outside of the pulsing window for morphological assessment that occurs at about 70% of the R-R interval. Left ventricle (LV) functional assessment is still possible. Slower heart rates are better for gated ECG as the optimal pulsing window for morphological imaging is heart-rate dependent.3 Tube current modulation during retrospective ECG-synchronisation CT can result in up to 64% reduction in radiation dosage.9
Pre- and postoperative evaluation of TOF
TOF is one of the earliest described cyanotic congenital heart conditions and, despite a long history of both palliative and definitive surgical repair, uniform successful outcomes remain elusive. Surgical techniques underpinned by a better understanding of post-TOF repair physiology have demonstrated improved outcomes. A departure from the traditional quest for elimination of the 'undesirable' right ventricular outflow tract obstruction, at the expense of free pulmonary regurgitation, has resulted in an avoidance of long-term complications such as RV dilatation and consequent RV and LV dysfunction.10
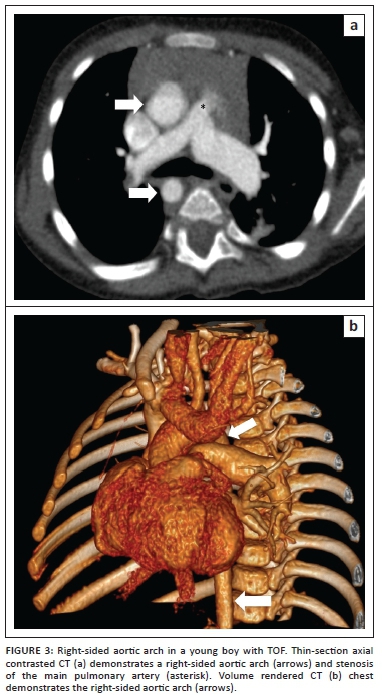
Preoperative imaging is directed at confirmation of the diagnosis and differentiation of TOF from other common mixing disorders such as a common arterial trunk, transposition of the great vessels with a ventricular septal defect or a double-outlet right ventricle (DORV). Further goals of preoperative imaging are to establish the severity of the primary anatomical lesion, the associated anomalies and the degree of functional disturbance, that in turn dictate appropriate timing of surgical intervention - either definitive early repair or a staged approach following initial palliation. The surgical approach itself may be altered by anatomical relationships of cardiac, coronary and extra-cardiac structures, such as a right-sided aortic arch (Figure 3), MAPCAs and variant coronary anatomy.11 The debate around timing of surgery and the multitude of institutional preferences of surgical approach is beyond the scope of the present paper.
In his presentation entitled 'The essential echocardiographic features of tetralogy of Fallot',2 Norman H. Silverman very eloquently illustrates the comprehensive role of echocardiography in the pre-operative evaluation of TOF. The four features of TOF as well as the pulmonary valve morphology, main and branch pulmonary arteries, proximal coronary anatomy, aortic arch anatomy and even aortopulmonary collateral arteries can all be adequately identified at echocardiography in skilled and experienced hands.
Cardiac CTA provides the ideal alternative to invasive and potentially hazardous cardiac catheterisation when the limitations of echocardiography fail to meet the goals of imaging.12 Box 2 illustrates the indications for preoperative cardiac CTA in TOF.
Branch pulmonary arteries and MAPCAs
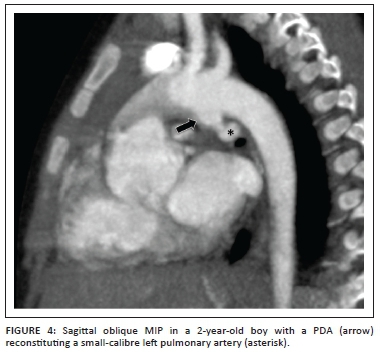
The variability in surgical management of TOF is frequently because of the diverse arrangement of the pulmonary arterial anatomy and the source of pulmonary artery blood supply. TOF with pulmonary atresia (TOF-PA) is a more severe variant that accounts for 20.3% of TOF13 where the arrangement of the pulmonary arteries may vary from well-formed, confluent pulmonary arteries (pulmonary arteries in free communication) supplied by the patent ductus arteriosus (Figure 4), to absence of the pulmonary valve and the native pulmonary arteries, with MAPCAs providing all the pulmonary supply. The anatomy of the native pulmonary arteries and vessels of supply must be clearly established in order to plan corrective surgery.11
The most frequent arrangement is where the pulmonary arteries are confluent but hypoplastic, with flow into them supplied by MAPCAs.
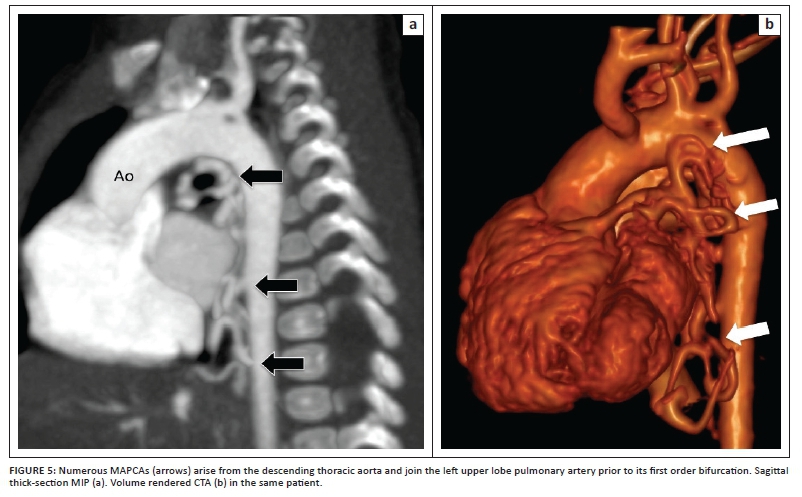
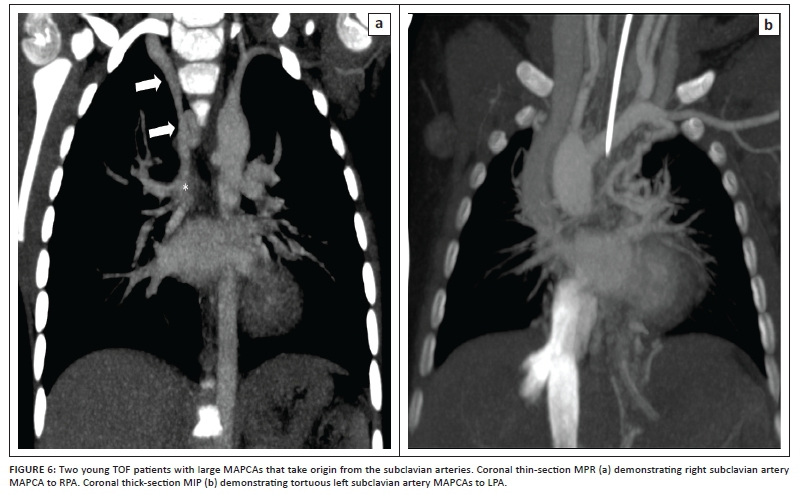
MAPCAs most frequently arise from the descending thoracic aorta (Figure 5) but can also take origin from the ascending aorta and the head and neck vessels (subclavian artery most commonly) (Figure 6) and even from the coronary arteries or from the infra-diaphragmatic supply.
Complete absence of the native pulmonary arteries (non-confluent) with absent antegrade flow of blood from the RV to the pulmonary arteries is much less common. Large calibre, hypertensive MAPCAs are then the only source of supply, necessitating early surgical intervention.
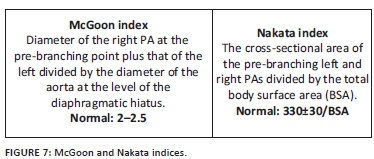
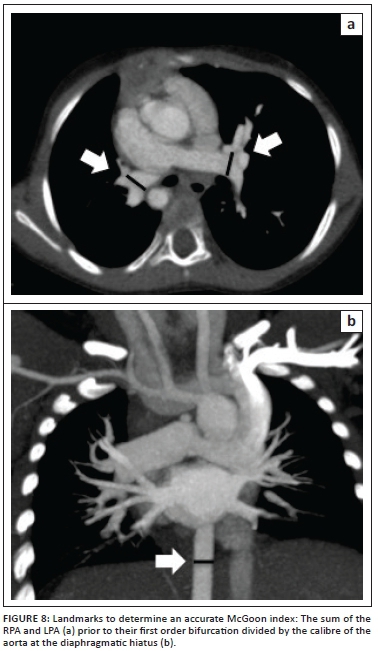
Cardiac CTA, with its multi-planar and three-dimensional reconstruction capabilities, allows accurate depiction of pulmonary artery anatomy, MAPCAs and the aorta at the level of the diaphragm. These features allow calculation of the McGoon index and the Nakata index (Figure 7) to quantitate the degree of pulmonary artery hypoplasia. The McGoon index is the preferred index in our institution and is used post-palliation (central shunt, classic or modified Blalock-Taussig shunt, Brock procedure or stent) to guide definitive repair and VSD closure when it exceeds 1.6-1.8.
Complex coronary arteries
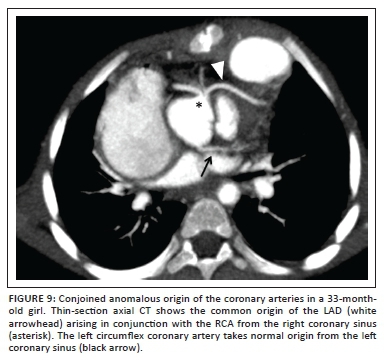
Coronary artery anomalies in TOF have an incidence of 5% - 12%13 and, whilst they in themselves do not present any risk of ischaemia or sudden death, surgical morbidity and mortality are significantly increased when they cross the RVOT. When undiagnosed, these vessels are at significant risk of surgical injury during right ventriculotomy or RVOT repair. The most frequently encountered coronary artery anomaly is left anterior descending (LAD) or accessory LAD arising from the right coronary artery (RCA) or right sinus of Valsalva14 (Figure 9) that crosses the RVOT to reach the anterior interventricular groove. The second-most common anomaly seen in most studies is that of a single coronary ostium from one of the sinuses of Valsalva (left, right or non-coronary sinus); these may or may not traverse the RVOT.
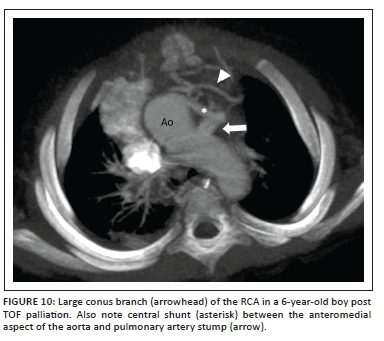
Single or double enlarged conus arteries that take origin from the RCA (Figure 10) and a RCA that arises from the LCA, are further common anomalies that can present a serious hazard at the time of surgery.
Surgical repair can be successfully contemplated even in the presence of a major coronary artery anomaly, provided that the surgeon is made aware thereof. In most instances, proximal coronary anatomy is effectively and reliably demonstrated at echocardiography15 except in instances of previous palliation, late TOF repair or reoperation resulting in a suboptimal acoustic window, or where the coronary arteries pursue an intramyocardial course.
Cardiac CTA, when ECG synchronised (see section above entitled 'Cardiac CTA protocols'), is an alternative non-invasive modality of high diagnostic performance and accuracy, to demonstrate coronary artery origins, their course and spatial relationships to adjoining structures.
Evaluation of previous palliation
TOF repair involves closure of the VSD and augmentation of the RVOT. The technique for VSD closure is relatively standard whilst RVOT relief is variously achieved, depending on the severity of the lesion. The two procedures may occur simultaneously, or VSD closure may only take place post palliation.
Blalock-Taussig and central shunts
Systemic to pulmonary artery shunting procedures are well recognised interim surgical interventions, performed to augment pulmonary bloodflow prior to definitive corrective repair, to improve cyanosis, symptoms and general quality of life. Despite the trend towards single reparative operations, physiological and anatomical conditions (hypoplastic pulmonary arteries, coronary anomalies crossing the RVOT, avoidance of a conduit in a small RVOT) may preclude early definitive repair. Several types of palliative shunts have been described since the classic Blalock-Taussig (CBT) procedure of 1945, many of which have fallen out of favour (such as Potts and Waterston shunts) owing to subsequent pulmonary hypertension.
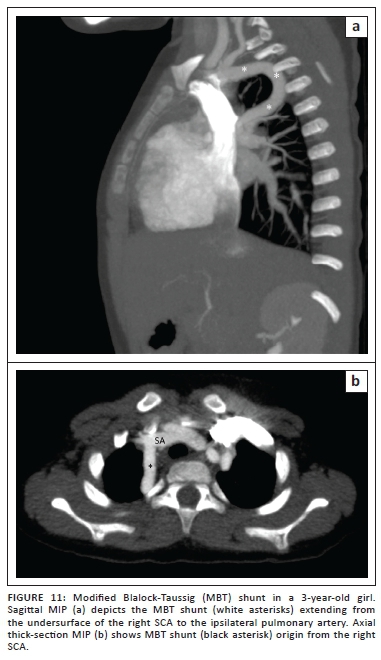
The modified Blalock-Taussig (MBT) shunt (Figure 11) directs blood from the subclavian artery opposite the aortic arch to the pulmonary artery via a PTFE or Goretex conduit graft rather than an end-to-side anastomosis of the ligated and divided native subclavian artery of the CBT shunt. Improved patency rates and ease of subsequent closure, favour the use of these shunts in our institution.
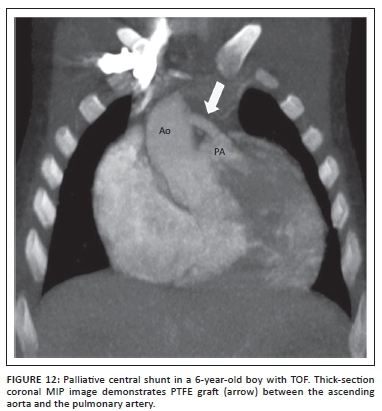
Central shunts using PTFE interposed between the ascending aorta and the main pulmonary artery are also in use. Where echocardiography may be challenging, CTA is once again perfectly suited to establish shunt anatomy and patency (Figure 12).
Pulmonary artery distortion owing to previous palliative shunting in older children lost to follow-up is elegantly displayed at CTA as an alternative to invasive angiography.
Brock procedure, RVOT and pulmonary artery stents
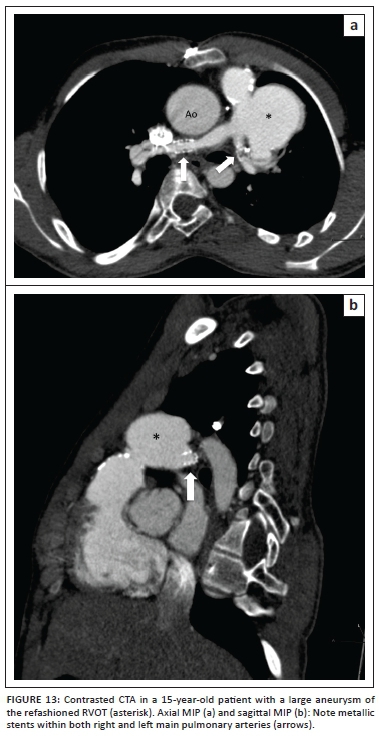
The effectiveness of the Brock procedure (RVOT relief without VSD closure) can also be effectively demonstrated via CTA. The Brock procedure is performed when the McGoon index is unfavourable and does not allow closure of the VSD at the time of RVOT relief. Pulmonary artery and RVOT stent patency and its related complications (Figure 13) are well documented at CTA and obviate the need for repeat angiography.
Restenosis of the pulmonary outflow tract
Infundibulectomy is reserved for cases of mild to moderate obstruction of the RVOT with an adequate pulmonary valve annulus. The hypertrophic muscle is resected via a transatrial-transpulmonary (TA-TP) approach without significant disruption of the pulmonary valve. Persistent or recurrent RVOT obstruction is a known consequence of this procedure, and serial imaging studies may be needed to assess the need for further surgical or catheter-based intervention.
Pulmonary outflow tract aneurysm
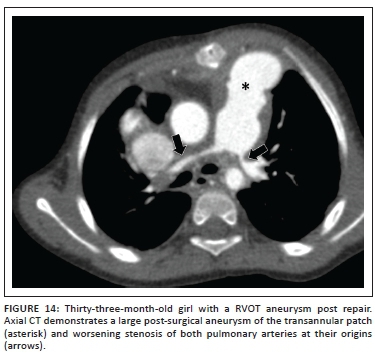
When the RVOT stenosis is more severe or involves the pulmonary valve annulus, a trans-annular patch repair, using treated pericardium or synthetic material to approximate the margins of the incision, is performed. The trans-annular anterior approach is associated with a variable amount of pulmonary valve insufficiency, resulting in eventual long-term RV dysfunction when excessive. Residual RVOT stenosis is implicated in the pathogenesis of the well-documented post repair complication of RVOT aneurysm (Figures 13-14). The ventriculotomy aneurysm may be complicated by the rare formation of intraluminal thrombus.16
RV-pulmonary artery conduit stenosis
The rare, severe variant of TOF-PA associated with atresia of the pulmonary valve or pulmonary artery is repaired by way of a Rastelli operation whereby a synthetic or biological conduit (homograft) is interposed between the RVOT and pulmonary arteries, which might have required prior augmentation. Conduit complications arise from stenosis at the anastomosis site, degenerative conduit stenosis itself and/or regurgitation of the conduit valve. In many instances, CTA is superior to echocardiography in assessing these stenosed conduits, owing to the aliasing that can occur with Doppler flow.
Restenosis of the pulmonary arteries
Recurrent or residual stenosis of the main or branch pulmonary arteries can occur regardless of the type of surgery employed to relieve the RVOT obstruction (Figure 14). Serial imaging of the arteries may be needed to ascertain when intervention is required.
Conclusion
Echocardiography remains the principal imaging modality of choice in the investigation of CHD, including tetralogy of Fallot.
Comprehensive single-modality investigation to address all the structural and functional queries preoperatively is often not achievable. CTA, in a resource-limited environment, can be used judiciously to complement the echocardiographic findings. The growing role of CMR and CTA as the preferred adjunctive tests to echocardiography is related to a simultaneous proportional decline in the use of invasive angiography.12
Competing interests
The authors declare that they have no financial or personal relationships which may have inappropriately influenced them in writing this article.
Authors' contributions
E.B. (University of Cape Town) is the principal author of this article. E.P. (Stellenbosch University) is responsible for the editing of the images and literature review. R.d.D. (University of Cape Town) acted in a clinical advisory role.
References
1. Van Praagh R. The first Stella van Praagh memorial lecture. Pediatric Cardiac Surgery Annual. Beverly: American Association for Thoracic Surgery; 2009; p. 19-38. [ Links ]
2. Silverman NH. The essential echocardiographic features of tetralogy of Fallot. Cardiol Young. 2013;23:871-882. PMID: 24401261, http://dx.doi.org/10.1017/S1047951113001704 [ Links ]
3. Stinn B, Stoltzmann P, Fornaro J, et al. Technical principles of computed tomography in children with CHD. Insights Imaging. 2011;2:349-356. http://dx.doi.org/10.1007/s13244-011-0088-1 [ Links ]
4. Goo HW, Yang DH. Coronary artery visibility in free breathing young children with CHD on cardiac 64-slice CT: Dual-source ECG-triggered sequential scan vs. Single-source non-ECG-synchronized spiral scan. Paediatr Radiol. 2010;40:1670-1680. http://dx.doi.org/10.1007/s00247-010-1693-8 [ Links ]
5. Desjardins B, Kazerooni EA. ECG-gated cardiac CT. Am J Roentgenol. 2004;182:993-1010. http://dx.doi.org/10.2214/ajr.182.4.1820993 [ Links ]
6. Shuman WP, Branch KR, May JM, et al. Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: Comparison of image quality and patient radiation dose. Radiology. 2008; 248:431-437. PMID: 18552312, http://dx.doi.org/10.1148/radiol.2482072192 [ Links ]
7. Hsieh J, Londt J, Vass M, Li J, Tang X, Okerlund D. Step-and-shoot data acquisition and reconstruction for cardiac X-ray computed tomography. Med Phys. 2006;33:4236-4248. PMID: 17153402, http://dx.doi.org/10.1118/1.2361078 [ Links ]
8. Earls JP, Berman EL, Urban BA, et al. Prospectively gated coronary CT angiography versus retrospectively gated helical technique. Radiology. 2008;246:742-753. PMID: 18195386, http://dx.doi.org/10.1148/radiol.2463070989 [ Links ]
9. Weustink AC, MolletNR, Pugliese F, et al. Optimal electrocardiographic pulsing windows and heart rate: Effect on image quality and radiation exposure. Radiology. 2008;248:792-798. PMID: 18710975, http://dx.doi.org/10.1148/radiol.2483072098 [ Links ]
10. Karl TR. Tetralogy of Fallot: Current surgical perspective. Ann Pediatr Cardiol. 2008;1:93-100. http://dx.doi.org/10.4103/0974-2069.43873 [ Links ]
11. Prieto LR. Management of tetralogy of Fallot with pulmonary atresia. Images Paediatr Cardiol. 2005;7:24-42. [ Links ]
12. Han BK, Lesser AM, Vezmar M, et al. Cardiovascular imaging trends in congenital heart disease. J Cardiovasc Comput Tomogr. 2013;7:361-366. PMID: 24331931, http://dx.doi.org/10.1016/j.jcct.2013.11 [ Links ]
13. Van Ferenz C, Rubin JD, McCarter RJ, et al. Congenital heart disease: Prevalence at livebirth. Am J Epidemiol. 1985;121:31-36. PMID: 3964990. [ Links ]
14. Kervancioglu M, Tokel K, Varan B, Yildirim SV. Frequency, origins and courses of anomalous coronary arteries in 607 Turkish children with tetralogy of Fallot. Cardiol J. 2011;18:546-551. PMID: 21947991. [ Links ]
15. Jureidini SB, Appleton RS, Nouri S. Detection of coronary artery abnormalities in tetralogy of Fallot by two-dimensional echocardiography. J Am Coll Cardiol. 1989;14:960-967. PMID: 2794284, http://dx.doi.org/10.1016/0735-1097(89)90473-7 [ Links ]
16. Peer SM, Bhat PSS, Furtado AD, Chikkatur R. Right ventricular outflow tract aneurysm with thrombus. Interact Cardiovasc Thorac Surg. 2012;14:488-490. http://dx.doi.org/10.1093/icvts/ivr151 [ Links ]
 Correspondence:
Correspondence:
Ebrahim Banderker
Department of Diagnostic Radiology
Red Cross War Memorial Children's Hospital Kliptown Road
Rondebosch 7700, South Africa
ebanderker@iafrica.com
Received: 12 June 2015
Accepted: 14 Oct. 2015
Published: 17 Dec. 2015


{kind=link}
{kind=link}
{kind=link}