










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Journal of Radiology
versão On-line ISSN 2078-6778
versão impressa ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.19 no.1 Johannesburg 2015
http://dx.doi.org/10.4102/sajr.v19i1.634
ORIGINAL ARTICLE
A comparative cost analysis of picture archiving and communications systems (PACS) versus conventional radiology in the private sector
Indres Moodley; Sivani Moodley
Health Outcomes Research Unit, Department of Public Heath Medicine, University of KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: Radiology is rapidly advancing, with a global transition to digital imaging technology to improve productivity and enhance communication. The major challenge confronting radiology practices is to demonstrate cost savings and productivity gains when a picture archiving and communication system (PACS) is established
AIM: To undertake an incremental cost analysis of PACS compared with conventional radiology to determine productivity gains, if any, at two private hospitals in Durban
METHOD: An incremental cost analysis for chest radiographs,, computed tomography and magnetic resonance imaging brain scans with and without contrast were performed. The overall incremental cost for PACS in comparison with a conventional radiology site was determined. The net present value was also determined to evaluate the capital budgeting requirements for both systems
RESULTS: The incremental cost of both capital and the radiology information system for installing PACS shows an expected increase. The incremental PACS image cost shows a reduction
CONCLUSION: The study provides a benchmark for the cost incurred when implementing PACS. It also provides a decision framework for radiology departments that plan to introduce PACS and helps to determine the feasibility of its introduction
Introduction
Radiology is rapidly advancing with the introduction of new technologies. Globally, a transition to digital imaging technology and picture archiving and communication systems (PACS) is rapidly transforming radiology. Until recently, conventional radiology based on screen-film technology dominated all radiology departments. However, many radiology departments have since introduced PACS, an electronic system that is used in radiology to transfer, archive, store and retrieve digital images and produce reports. PACS and digital radiography (DR) have the potential to bring about a major change in radiology workflow. Patients benefit from reduced waiting times, whilst radiology practices benefit from increased productivity with a reduction in staffing costs.
The purpose of the present study is to undertake a cost analysis of a PACS system in comparison with conventional radiology in two private sector radiology departments in Durban. The study focuses on the incremental costs of introducing PACS with digital radiology versus conventional radiology. It is important that decision-makers have information regarding the financial impact of PACS, to allow appropriate budget planning for radiology departments in South African hospitals. The study will also assist in understanding the financial implications of PACS in terms of efficiency gains in human resource allocation and the potential subsequent reduction in overall health care costs.
Background
Table 1 shows differences in systems and processes between Hospital A and Hospital B. Hospital A removed the conventional film or screen radiography unit and replaced it with a conventional radiography and DR radiology unit. Both sites had used a similar radiology information system (RIS) which existed prior to the implementation. The only difference for Hospital A was linking the Digital Imaging and Communications in Medicine (DICOM) modality work list to the radiology modalities. The darkroom and processing unit was removed in Hospital A to accommodate a server room. Both hospitals retained their laser film processors. Printing of the report and film for distribution for Hospital B remained the same; however, Hospital A had installed web access throughout the hospital as well as a compact disc (CD) burner for distribution of patient images.

Both Hospital A and Hospital B had one darkroom assistant at the time of implementation. The assistant from Hospital A was transferred to another department within the radiology group and would not be replaced if she left.
Hospital A had been operating with a fully installed PACS for two years. PACS introduction involved training staff who still had to continue regular work, which created pressure for them during the training phase of the implementation. Teething problems were experienced during this phase, such as incorrect scanning of referring documents, mismatch of images owing to incorrect accession numbers used by the radiographers, and cancelling of accounts. Troubleshooting with the assistance of the PACS and application specialist was done as problems arose because many problems could not be anticipated before implementation. All major and minor workflow issues had been rectified at the time of the present study. Paper printouts were given to patients on request for hard-copy images. The laser printer was kept on site for emergency purposes and for special requests.
Methods
The study was undertaken at two private hospitals in Durban, KwaZulu-Natal Province (Hospital A and Hospital B). Hospital A has 400 beds and Hospital B has 270. Both hospitals have dedicated specialist wards. The study population comprised all walk-in patients attending the radiology department for chest radiographs, magnetic resonance imaging (MRI) and computed tomography (CT) brain scans for a period of one month (August 2009) as well as all radiographers working in these departments.
Data for the cost analysis were obtained from the accounting departments of each hospital. Costs attributable to radiology services were determined for personnel, equipment, consumables, and utility and maintenance costs. Costs of procedures were obtained from the electronic billing system at both the hospitals. For the purposes of comparison, the costs of all procedures were determined using medical aid rates.
The time taken for the different types of studies using either conventional radiology or PACS were obtained from radiographers by means of questionnaires. A pilot study consisting of 10 radiographers was conducted to ensure there was no ambiguity in the questionnaires before they were administered.
Waiting time sheets were self-administered by all walk-in patients for chest, CT and MRI brain procedures. This information was cross-referenced to the data recorded on the RIS at both sites.
Questionnaires were used to determine radiographers' work experience, actual times for examination taken with PACS and conventional radiology methods, any problems experienced with PACS, and any suggestions that could assist in implementing PACS. Data obtained from the time sheets were verified with those recorded on the RIS.
The total number of procedures was determined for the month of August (31 days). The cost per procedure (chest radiograph, CT and MRI brain scans) was then determined. Personnel salaries were weighted according to the time taken to undertake each step of the procedure. Consumables and materials needed for each procedure were also added to make up the final cost. Water, electricity, cleaning services, maintenance of the building and security were included in the monthly rental costs for both sites. Costs for chest radiographs, CT and MRI brain scans were extrapolated to annual costs, and the monthly cost for each procedure was then calculated.
The maintenance of the building was included in the rental cost. The cost of equipment and furniture was calculated using replacement values as well as their lifespan. For computers and furniture, average lifespan is 3-5 years depending on usage. For all other equipment and mainframe computers, the South African Revenue Service's (SARS) depreciation allowance of 5 years was used and 2 years for software depreciation.1
Income after tax was calculated on the gross income after allowance for wear and tear. Net income was calculated after deducting income tax at 28%.
The net present value (NPV) takes into account cash flows over a period of time, discount rates and the lifetime of the project. The NPV for conventional radiology workflow methods was compared to that of PACS. Productivity gains were added from the PACS NPV values to show the NPV with the total cost savings for chest radiographs and CT and MRI brain scans.
The formula for calculating NPV is:
Where:
NPV = net present value
CF t = the cash flow in period t
r = discount rate
N = number of periods.
The NPV calculation in the above formula can be described as the present value of an investment's expected cash inflows minus the costs of acquiring the investment. NPV calculations are used to analyse acquisitions or future capital costs.
Ethical considerations
Ethical approval for the study was obtained from the Biomedical Research Ethics Committee of the Nelson R. Mandela School of Medicine (reference number EXP003/06).
Results
Capital costs of PACS and conventional radiography
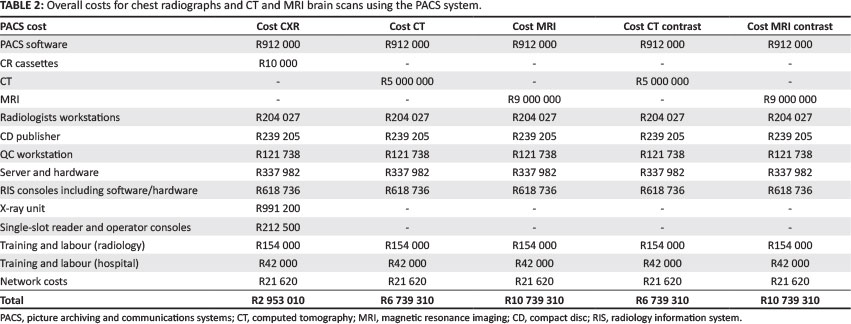
The capital costs of PACS and conventional X-ray equipment are shown in Table 2. The capital costs for PACS included software, computers, digital X-ray equipment, CT and MRI scanners compatible with DICOM, wide-screen monitors and 17-inch monitor screens for radiologists, computed radiography (CR) cassettes, CD printer, UPS, single slot reader, operator consoles for radiographers and training costs.
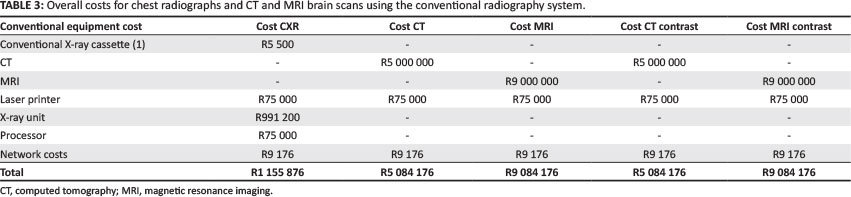
Table 2 and Table 3 show each cost item used for the calculation of the capital cost of PACS and conventional radiography for chest radiographs and CT and MRI brain scans with and without contrast. An important aspect noted in the tables is that the implementation of PACS incurs greater capital cost for all three procedures than conventional radiography systems.
Table 4 shows a detailed imaging cost for PACS. Weighted labour costs required to produce a radiograph were included as well as the costs of each consumable to produce the radiograph. The labour costs for radiographers were used to calculate the minimum (one radiographer) and maximum (two radiographers) total costs. Operating costs included maintenance (building and equipment), utilities and services excluding service level agreements.

The imaging costs for producing images by conventional radiography methods are shown in Table 5. Radiographer labour costs were used to calculate the minimum and maximum total costs. Operating costs included maintenance (building and equipment), utilities and services, excluding the service level agreement.

Table 6 shows the overall incremental imaging costs for PACS v. conventional X-rays. A decrease in imaging cost for PACS compared with conventional radiology was observed. Chest radiographs and MRI brain scans with PACS showed a substantial cost saving on a single examination image cost. A moderate cost saving of 5% and 14.2% was seen for CT brain scans (with and without contrast, respectively). However, a more substantial cost saving of 27% was seen for chest radiographs whilst MRI brain scans (with and without contrast) decreased by 22% and 15% respectively.

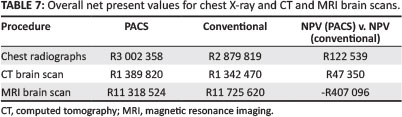
The capital costs allocated for radiology equipment (conventional radiography (cassettes, cassette reader and X-ray unit), CT, MRI), computer hardware (reception PCs, consoles for radiographer and radiologists, CD publisher, server, quality control PC, network costs) as well as RIS and PACS were weighted according to the number of patients per examination procedure. Income after tax was used in determining the NPV. The individual NPVs for both systems, though not significantly different, were positive, indicating that both systems were equally profitable.
The overall NPVs for PACS and conventional methods, including the difference between both systems, is shown in Table 7.
Productivity gains
All salaries (radiographers, radiologists, PACS administrators and darkroom assistants) were weighted according to the number of chest radiographs and CT and MRI brain scans undertaken. Because private hospital salary scales were deemed to be confidential, the radiologist's salary was taken from the National Department of Health salary scales and is probably a conservative estimate. Following the introduction of PACS, a decrease in the number of radiologists on site from five to three was noted, signifying productivity gains for the practice. The cost savings of two radiologists for a year was in the range of R1 833 000 to R3 665 000. There was no decrease in radiographer staff numbers at the time of the study. However, it was noted over a period of time that, when radiographers left, fewer were replaced.
Table 8 shows the NPV values for chest radiographs' and CT and MRI brain scans' productivity gains over a five-year forecast period.

Productivity gains were weighted for the time spent by a radiologist to diagnose and report a procedure. The NPV for chest radiographs and CT and MRI brain scans after five years was positive, showing a net productivity gain. In the present study, the project timeline was assumed to be five years. The timeline is based on the expected useful life of current hardware, software systems and procedure technologies.
Time and motion study for PACS vs. conventional radiology
A time and motion study determined the time taken to capture patients' details onto the RIS until the report was produced; this provided the total waiting time for patients. PACS waiting times showed a reduction owing to reduced report waiting times for all three procedures (Figures 1-3).


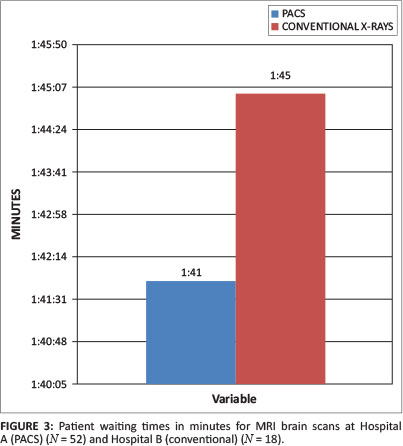
The results shown in Figures 1-3 reveal that both sites performed the same number of procedures for chest radiographs and CT brain scans, except for Hospital A where more MRI brain scans were performed. Compared with conventional radiography, chest radiographs and CT and MRI brain scans using the PACS site were completed in less time; this could provide added advantage to hospitals with PACS as the potential exists to increase patient throughput.
User satisfaction survey
A total of 16 radiographers from Hospital A were given the opportunity to participate in the present study, with 81% of them returning their self-administered questionnaires. The results show that all the radiographers had a year or more PACS experience in a completely filmless and paperless environment. All (100%) staff who participated in the study preferred the new PACS system over the conventional system. Further interrogation of their responses showed that a large proportion (46%) of the radiographers preferred PACS because they found the system to be fast and efficient. About 23% observed that time efficiencies were possible with PACS. A small proportion (8%) of the radiographers felt that PACS was easier to use than conventional radiology methods.
Discussion
The present study compared the cost of introducing PACS with conventional radiology. PACS is fast becoming the method of choice for both local and international radiologists. The recent application of digital technology to radiology has not only eliminated the need for producing X-ray film and paper-based reports but also improved patient workflow in radiology departments. Referring doctors are now able to make a more rapid diagnosis owing to the quick and easy access to radiological images and reports via the electronic system. Radiologists are able to increase diagnostic accuracy thanks to the accessibility via PACS of previous studies. PACS can increase the productivity of a radiology department and lead to positive financial outcomes, depending on various other factors such as the vendor used and location of the radiology department. However, careful financial consideration must be applied.
The implementation of PACS requires a major capital investment initially, with a total cost that must include RIS. Where a radiology department has an existing RIS and digital equipment, as is becoming the norm as equipment is replaced, the additional cost would then be only for the acquisition of PACS. The present study did not take into consideration the building modifications needed when implementing PACS. In this study, those aspects were minor: the server room and radiographer and radiologist workspace needed some modifications and requirements to be met.
The findings presented here suggest that the incremental capital costs for implementing PACS are greatest when new digital X-ray equipment and PACS are purchased at the same time, as in the case of Hospital A. This option may not apply to all radiology practices as X-ray equipment costs are often fully paid off before PACS is purchased. Pratt et al.2 suggest that when a hospital is committed to implementing CR equipment regardless of implementing PACS, or if the CR equipment is already installed, it would result in a positive financial effect on the cost analysis because the implementation of CR can be regarded as a sunk cost. The implementation of CR or DR equipment before the introduction of PACS could prove to be a cost-effective method for radiology practices and reduce the need for a large capital outlay at one time.
Hospital A required hardware and software as well as labour costs for implementation and training. These initial costs account for the greater capital investment needed for PACS. With the introduction of PACS in Hospital A, the radiographer and radiologists required client computers. For the radiologists, additional diagnostic monitors were also needed. These costs were not incurred in Hospital B (conventional radiography) as the radiographer and radiologist made use of referral letters and printed radiographs.
Both Hospital A and Hospital B with RIS required a local area network (LAN) to be set up. However, the layout of the network in Hospital A was more complicated as it involved linking reception, radiographer and radiologist. Hospital A was able to reduce these costs by using the existing IT department to configure and establish this network. The LAN cost incurred in Hospital A was far greater than that of Hospital B owing to the increased need to network the entire radiology department in Hospital A. The cost incurred for the hospital network was not included in the present study as the hospital had taken responsibility to configure and maintain this network for the referral doctors.
Although the initial capital outlay for PACS is high, there are other financial benefits in its use. The incremental image costs for chest radiographs and CT and MRI brain scans are less than the incremental RIS and capital costs. Incremental image production costs in all the PACS radiology departments showed a cost saving for all three procedures. These findings are consistent with previous findings on PACS costings.2,3,4,5
The image cost savings and related consumable costs are one of the positive aspects to implementing PACS.
While the NPV for MRI brain scans was negative, a positive NPV value was found for chest radiographs and CT brain scans. The findings for MRI brain scans were not similar to previous studies as a positive NPV value for PACS was obtained.2,6,7,8 The reason for this difference could be the volume of patients seen at the practice, which offsets the costs; however, it could also indicate that different examination procedures yield different NPV values.2,6,7,8
Other major direct cost savings derived from PACS arose in staffing and operational costs, which showed a reduction in cost for chest radiographs and CT and MRI brain scans. The predominant gain seen with PACS is the productivity gain. A reduction from five radiologists to three resulted in cost savings to Hospital A owing to both PACS and the central work list. Wide area network (WAN) cost was not included as it was implemented after this study was completed. The radiology department was now able to decrease the need for additional radiologists as well as re-allocate radiologists for a newer venue and annual leave. This cost saving had a positive effect on the NPV value for chest radiographs and CT brain scans. It was also observed that, over the period of the study, radiographers were not always replaced upon their departure, thus reducing the number of radiographers currently working in the department. The need for darkroom assistants was eliminated and, in Hospital A, they were relocated to the distribution section of radiology. However, the additional cost of a PACS administrator was incurred in Hospital A.
The results presented in the present study show that, whilst PACS incurs a greater initial capital cost than conventional radiology methods, there are downstream cost savings in human resources and image production. To determine the true costing of PACS, both monetary and non-monetary benefits need to be considered. Mweli9 points out an interesting aspect on non-monetary costs, in that, for patients, the benefit of implementing PACS is immediate, whilst the benefit to a radiology practice is in the long term. Mweli9 also states that the benefits to patients are indirect and can only be seen downstream of the value process.3,8
Radiologists are now able to immediately access the images, patient referring letter and history, thus reducing the time to clear their work lists. The workload on radiologists is eased via even distribution of work. Consequently, reporting backlogs can be avoided and patients' report turnaround time can be improved. At Hospital A, it was later found that with the introduction of further workflow enhancements within PACS, a radiologist could work at any practice or venue and report a case anywhere with PACS facilities; for example, a central work list. There was also a moderate improvement in report waiting times for patients who opted to wait for their radiographs, as these can now be transmitted electronically to the requesting doctor. The productivity gains from PACS show that with the decrease in times, the potential exists to increase the number of patients, providing an increase in profitability. The referring doctor also benefits as patient images are available for viewing at the same time as their interpretation by the radiologist. Referring doctors can now benefit through faster turnaround times for patient diagnosis as images are immediately accessible to them and treatment of patients can be expedited.
The radiographers' experience with PACS was shown to be positive owing to improvements in the working environment. Radiographers who are the end users are important in making any system work successfully, especially in a PACS environment. Radiographer productivity gains were not evaluated in the present study. However, in the self-administered questionnaire, they reported improved speed and efficiency of workflow with PACS. The new system made the working environment easier for some radiographers by eliminating slow and tedious processes used in conventional radiology. Some of the initial disadvantages of using PACS are downtime owing to initial errors and computer glitches during the setup phase; however, these arise only in the first few months of implementation. Once this phase is over, very few incidents occur, and onsite assistance is available at all times.
In the present study, one of the radiology practices with PACS has seen productivity gains owing to the reduced need for an onsite radiologist, thus contributing to cost savings. However, both radiology departments have seen the opportunity to enhance workflow by introducing remote reporting, voice recognition and tele-radiology through the introduction of PACS technology.
PACS could potentially be of benefit to the proposed national health insurance scheme by reducing the number of radiologists required and image processing costs, whilst containing costs, thereby eliminating compromise in the quality of patient care.10,11
Costing a new investment such as PACS is a key factor in controlling the high spend on health care in South Africa. However, radiology practices need to evaluate PACS technology in terms of both its monetary and non-monetary benefits before coming to an implementation decision.
The present study could be used to inform other practices contemplating the introduction of PACS. It should be noted that a return of investment might not be seen in the short-term; further cost benefit studies would be required to evaluate this. However, the benefits to the practice, radiologists, referring physicians and patients in terms of time and efficiency are more immediate.
Acknowledgements
This article is an objective production by the authors. Where applicable, the research work or material from various academic scholars and sources has been acknowledged and reported accurately.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
References
1. South African Revenue Services. Wear and tear or depreciation allowance [homepage on the internet] c2010 [cited 10 January 2012]. [ Links ] Available from: http://www.sars.gov.za/home.asp?pid=55888
2. Pratt HM, Langlotz CP, Feingold ER, Schwartz JS, Kundel HL. Incremental cost of department wide implementation of a picture archiving and communication system and computer radiography. Radiology. 1998;206:245-252. http://dx.doi.org/10.1148/radiology.206.1.9423679 [ Links ]
3. Becker SH, Arenson RL. Costs and benefits of picture archiving and communication systems. J Am Med Inform Assoc. 1994;1:361-371. http://dx.doi.org/10.1136/jamia.1994.95153424 [ Links ]
4. Huda W, Honeyman JC, Frost MM, Staab EVA. Cost analysis of computed radiography and picture archiving and communication systems in portable radiography. J Digit Imaging. 1996;9:39-14. http://dx.doi.org/10.1007/BF03168567 [ Links ]
5. Reddy AS, Loh S, Kane RA. Budget variance analysis of a department wide implementation of a PACS at a major academic medical center. J Digit Imaging. 2006;19:66-71. http://dx.doi.org/10.1007/s10278-006-0852-9 [ Links ]
6. Duerinchkx AJ, Kenagy JJ, Grant EG. Cost analysis of PACS: Fact or fiction. Medical Imaging. 1999;253. http://dx.doi.org/10.1117/12.352752 [ Links ]
7. Fang YC, Yang M, Hsueh YS. Financial assessment of a picture archiving and communication system implemented all at once. J Digit Imaging. 2006;19:44-51. http://dx.doi.org/10.1007/s10278-006-0632-6 [ Links ]
8. Hilsenrath PE, Smith WL, Berbaum KS, Franken EA, Owen DA. Analysis of the cost effectiveness of PACS. AJR. 1991;156:177-180. http://dx.doi.org/10.2214/ajr.156.1.1898556 [ Links ]
9. Mweli, T. An exploratory business case for radiology information system (RIS) - A South African firm level analysis [dissertation for Master of Business Administration]. Pretoria: University of South Africa; 2010. [ Links ]
10. Economist Intelligence Unit. Healthcare and pharmaceuticals report South Africa - Market data at a glance. [ Links ] [homepage on the internet] c2012 [cited 26 April 2012]. Available from: http://store.eiu.com/article.aspx?.productid=1557096955
11. Masombuka S. NHI plan now on a roll. The Times. 23 March 2012. Available from: http://www.timeslive.co.za/local/2012/03/23/nhi-plan-now-on-a-roll [ Links ]
 Correspondence:
Correspondence:
Indres Moodley
Private Bag X7
Congella 4013
Durban
South Africa
Email: moodleyi15@ukzn.ac.za
Received: 10 May 2014
Accepted: 22 Dec. 2014
Published: 31 Mar. 2015


{kind=link}
{kind=link}