










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Journal of Radiology
On-line version ISSN 2078-6778
Print version ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.18 n.2 Johannesburg 2014
http://dx.doi.org/10.4102/sajr.v18i2.668
CASE REPORTS
Juxta-articular myxoma of the wrist
Andrew J. van den Heever
Tuft and Partners Incorporated Radiologists, Cape Town, South Africa
ABSTRACT
This case report describes a juxta-articular myxoma (JAM) in an uncommon location, demonstrating an unusually aggressive local growth pattern.
Introduction
Myxomas are benign mesenchymal tumours characterised by the production of mucinous material in a scant spindle cell matrix.1 Juxta-articular myxoma (JAM) is a rare form of myxoma in the vicinity of a joint.2 JAM has an association with trauma or joint arthrosis. It is may be locally aggressive and commonly recurs after surgical excision.3
Case presentation
A 78-year-old man, with a history of colon carcinoma and gout, presented with a large mass in the thenar eminence and bilateral carpal tunnel syndrome. On clinical examination, the mass was fixed and had no inflammatory or infective features. Magnetic resonance imaging (MRI) was requested to assess the nature of the mass and exclude a neoplastic lesion.
Imaging findings
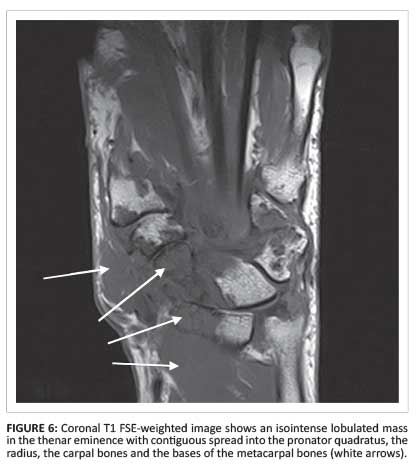
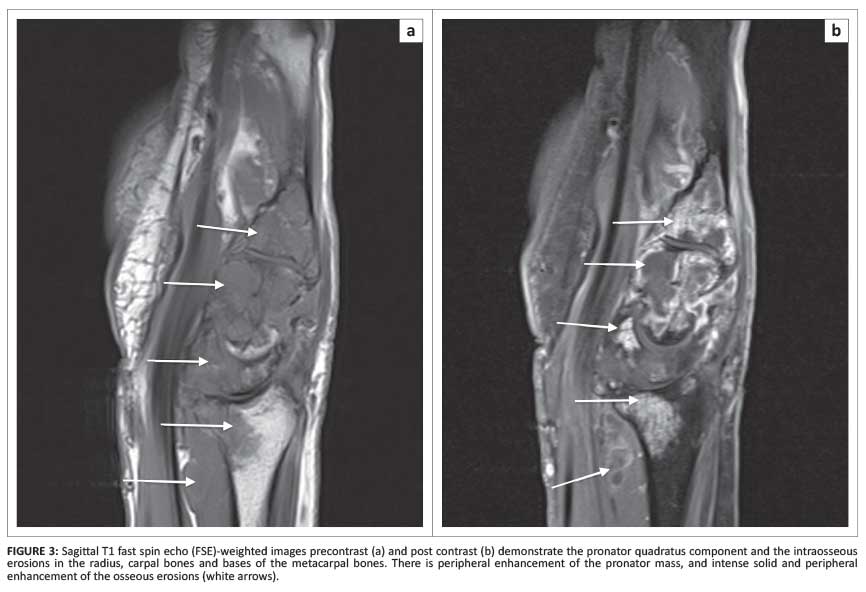
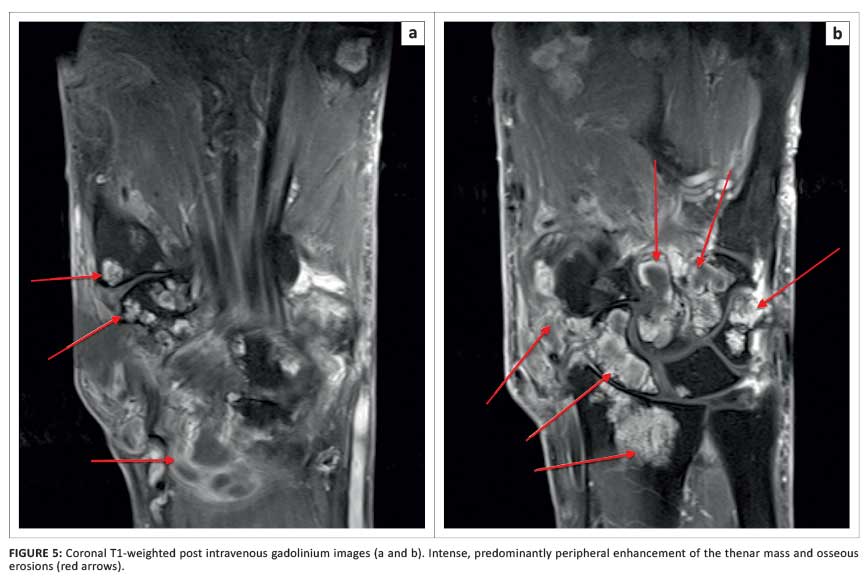
An extensive, multiseptated cystic mass was noted in the thenar eminence with infiltration around the flexor pollicis longis (FPL) and abductor pollicis brevis (APB) tendons. The mass had uniform fluid signal on proton density (PD) fat-saturated images (Figure 1 and Figure 2). Post-contrast images demonstrated enhancement of the septations with central fluid signal. Similar cystic infiltration was noted in and deep to the pronator quadratus (Figures 3b, 4, 5a and 5b).



Multiple osseous erosions involving the distal radius, the carpal bones and the metacarpal bases were observed. Prominent osseous erosion of the capitate and scaphoid was present with almost total destruction of the normal trabecular marrow. The erosions were PD hyperintense (Figure 1 and Figure 2), T1W hypointense (Figures 3a and Figure 6) and enhanced peripherally with almost uniform central fluid signal (Figures 3b, 4, 5a and 5b). The erosions were sharply marginated and corticated and there was no associated bone marrow oedema.
Tenosynovitis was noted, involving all of the extensor and flexor compartments. The median nerve, compressed in the carpal tunnel, was oedematous and swollen proximal to the carpal tunnel (Figures 3b, 4, 5a and 5b). Prominent radiocarpal and intercarpal synovitis was present. Moderate arthrosis of the radiocarpal, first carpometocarpal (CMC) and scaphotrapeziotrapezoid (STT) joints. Periarticular fluid collections, synovitis and enhancing erosions were noted in relation to the metacarpophalangeal (MCP) joints.
A diagnosis of probable gout was made, with a differential diagnosis of polyarticular inflammatory arthritis. Metastatic disease was thought unlikely.
Surgical findings
At surgery, a complex, infiltrating, locally aggressive cystic mass was confirmed (Figure 7). The thenar mass was debulked, the carpal tunnel was released and a biopsy of the synovium of the radiocarpal joint was done.

Histopathology
Histology and immunohistological staining revealed a mucin-producing mass with scant spindle cells expressing smooth muscle actin and vimentin. No features of autoimmune synovitis were present and no crystals were found. S100 and desmin staining was negative. A pathological diagnosis of JAM was made.
Clinical course
The postoperative course was initially unremarkable; however, the patient returned four months later complaining of an increase in the size of the lesion, with decreasing left hand function. A repeat MRI was performed prior to further surgery, as dramatic clinical deterioration suggested a possible infectious or malignant diagnosis.
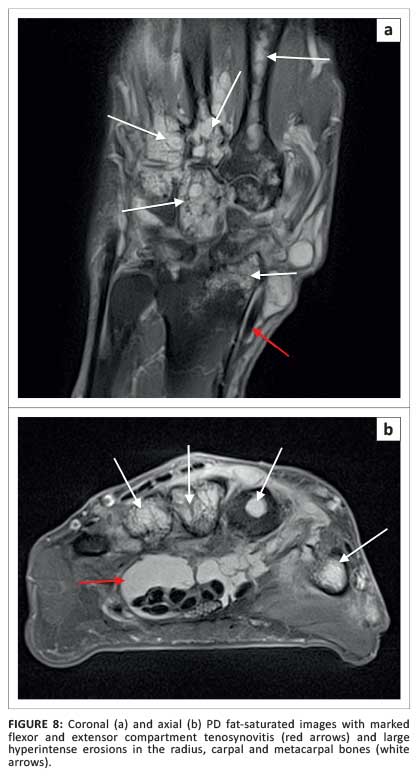
Follow-up MRI findings
The MRI showed recurrence of the thenar eminence JAM, marked progression of the erosive intraosseous components, prominent flexor and extensor tenosynovitis, and radiocarpal and intercarpal synovitis (Figure 8).
Discussion
JAM is most commonly associated with large joints, with a male preponderance. It is mostly found in the lower limbs, and is very unusual in the hand and wrist.5 JAM involves periarticular tissues including subcutaneous fat, joint capsule, tendons and rarely skeletal muscle.
The aetiology of the lesion is uncertain; however, there is an association with previous trauma and osteoarthrosis of the underlying joint.1, 6 The lesion itself is usually painless, but it may cause local mechanical symptoms. JAMs do not metastasise; however, as in this case, they can be very locally aggressive. Postoperative recurrence is seen in approximately 30% of JAMs within five years of excision.3, 4 Other types of myxoma are intramuscular, cutaneous aggressive angiomyxoma, and myxoma of the nerve sheath (neurothekeoma).3
Intramuscular myxoma is the most commonly encountered myxoma in clinical practice, occurring in the thigh, upper arm and buttock.5 The lesion is characteristically a well-circumscribed oval mass that is cystic in appearance. Intramuscular myxomas are usually solitary but may be multiple and, in this scenario, are usually associated with monostotic or polyostotic fibrous dysplasia, which is known as Mazabraud's syndrome.5
On ultrasound, the lesion may appear as a complex cystic mass (hypo- or anechoic with increased through-transmission and posterior acoustic enhancement) or may even appear solid. It is hypovascular.1 Computed tomography (CT) typically shows a lesion denser than water but less dense than muscle.8 The lesion on MRI is iso- to hypointense on precontrast T1W, inhomogeneously hyperintense on T2W, and demonstrates mild to moderate diffuse or peripheral contrast enhancement.8 Typical MRI findings also include mild perilesional oedema, owing to an incomplete fibrous capsule, and a split-fat sign as a result of adjacent muscle atrophy.8
JAM and intramuscular myxoma share the same histological characteristics, but are differentiated by lesion location and the high recurrence rate of JAM. The differential diagnosis of a lesion with imaging findings of a soft-tissue mass that mimics a cyst includes synovial cyst, bursa, ganglion, neurogenic neoplasms, myxoid liposarcomas and myxoid malignant fibrous histiocytoma (MFH).5, 7
Conclusion
JAM is a benign mesenchymal soft-tissue tumour that is a variant of myxoma, associated with large joints and joint degeneration. The present case demonstrates a histologically proven case of JAM in an unusual location, with an unusually aggressive growth pattern and prominent local tissue infiltration.
Acknowledgements
Competing interests
The author declares that they he has no financial or personal relationships that he might have inappropriately influenced him in writing this article.
References
1. Meis JM, Enzinger FM. Juxta-articular myxoma: A clinical and pathologic study of 65 cases. Hum Pathol. 1992;23(6):639-646. http://dx.doi.org/10.1016/0046-8177(92)90319-X [ Links ]
2. Allen PW. Myxoma is not a single entity: A review of the concept of myxoma. Ann Diagn Pathol. 2000;4(2):99-123. http://dx.doi.org/10.1016/S1092-9134(00)90019-4 [ Links ]
3. Fletcher JW, Watson HK, Weinzweig J. Recurrent myxoma of the hand. J Hand Surg Am. 2000;25(4):772-775. http://dx.doi.org/10.1053/jhsu.2000.9412 [ Links ]
4. Haluk OA, Merter Ozenski E, Inanc G, Serdar T. Juxta-articular myxoma of the wrist: A case report. J Hand Surg Am. 2005;30(1):165-167. http://dx.doi.org/10.1016/j.jhsa.2004.09.009 [ Links ]
5. Murphey MD, McRae GA, Fanburg-Smith JC, Temple HT, Levine AM, Abouilafia AJ. Imaging of soft-tissue myxoma with emphasis on CT and MRI and comparison of radiologic and pathologic findings. Rad. 2002;225(1):215-224. http://dx.doi.org/10.1148/radiol.2251011627 [ Links ]
6. Korver RJP, Theunissen PH, van de Kreeke WT, van der Linde MJ, Heyligers IC. Juxta-articular myxoma in a 5-year-old boy: A case report and review of the literature. Eur Radiol. 2010;20(3):764-768. http://dx.doi.org/10.1007/s00330-00901490-7 [ Links ]
7. Al-Qattan MM. Myxoma of the hand. J Hand Surg Br. 1996;21(5):690-692. http://dx.doi.org/10.1016/S0266-7681(96)80163-X [ Links ]
8. Petscavage-Thomas JM, Walker EA, Logie CI, Clarke LE, Duryea DM, Murphey MD. Soft-tissue myxomatous lesions: Review of salient imaging features with pathologic comparison. Radiograph. 2014;34(4):964-980. http://dx.doi.org/10.1148/rg.344130110 [ Links ]
 Correspondence:
Correspondence:
Andrew van den Heever
PO Box 461
Plumstead 7801
South Africa
Email:andrew.vdh@tuft.co.za
Received: 09 June 2014
Accepted: 06 Nov. 2014
Published: 11 Dec. 2014


{kind=link}
{kind=link}