










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Journal of Radiology
On-line version ISSN 2078-6778
Print version ISSN 1027-202X
S. Afr. J. radiol. (Online) vol.18 n.2 Johannesburg 2014
http://dx.doi.org/10.4102/sajr.v18i2.709
CASE REPORTS
Humeral avulsion of the glenohumeral ligament: The J sign
Pieter J. Oberholzer
Department of Radiology, University of Pretoria, South Africa
ABSTRACT
The lesion resulting from humeral avulsion of the glenohumeral ligament (HAGL) is an important cause of anterior glenohumeral instability and can be seen in isolation or combination with an antero-inferior labral complex lesion. A conclusive magnetic resonance imaging diagnosis is aided when either a joint effusion is present or a contrast arthrography of the shoulder is performed.It is important to be familiar with the J sign as it represents contrast leaking through the defect in the lateral attachment of the joint capsule.
Introduction
The musculotendinous structures of the rotator cuff and almost all the shoulder muscles maintain the stability of the glenohumeral joint.1 Humeral avulsion of the glenohumeral ligament (HAGL) is a less frequent cause of anterior instability than the classic Bankart lesion. The HAGL lesion may appear in patients with anterior stability, with or without association of an anterior labral tear. Magnetic resonance imaging (MRI) is essential in preoperative detection of a HAGL lesion. The 15° oblique radiograph view in the anterior plane of the shoulder (Garth view) demonstrates only the variant bony HAGL lesion.2 Intra-articular fluid (joint effusion) or the introduction of contrast medium (arthrography) is necessary to identify a HAGL lesion on MRI.
Case report
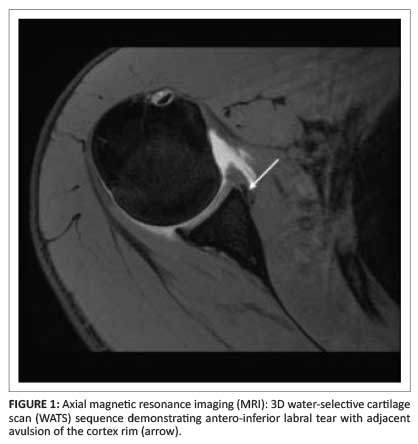
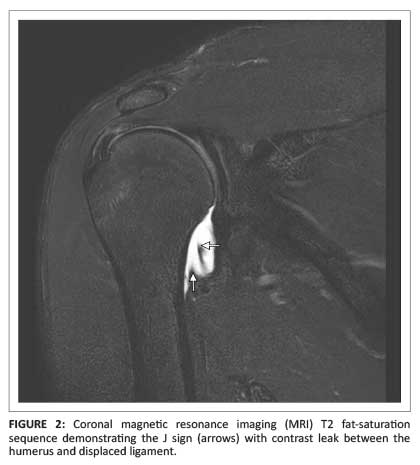
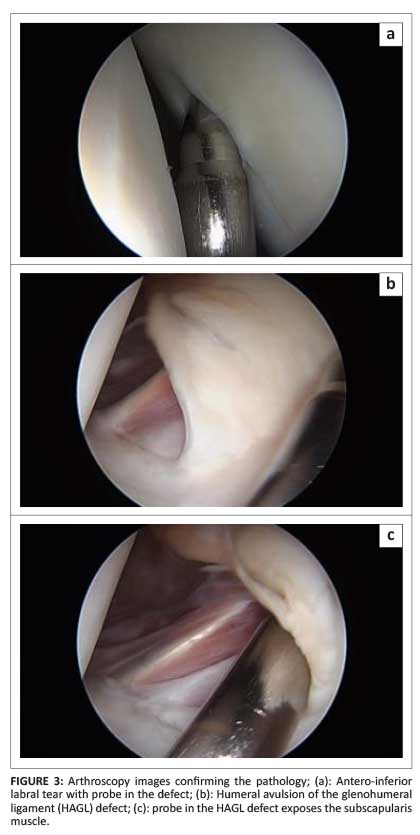
A 16-year-old rugby player, with a four-month history of injury to his right shoulder, presented with anterior glenohumeral instability. MRI was requested to assess the labrum and anterior capsule. The MRI arthrogram demonstrated an antero-inferior labral tear with adjacent avulsion of the cortical rim of the glenoid (Figure 1). A coronal T2W fat-saturation sequence showed the typical J sign caused by contrast leaking between the humerus and the displaced ligament (Figure 2). The findings were confirmed on arthroscopy (Figure 3). The inferior glenohumeral ligament (IGHL) in the patient was retracted and very tight at arthroscopic examination. He underwent open surgical repair, where part of the subscapularis muscle was used to close the defect.
Discussion
HAGL and anterior instability
The IGHL consists of an anterior and a posterior band with the axillary pouch interposed. The medial attachment, at the antero-inferior and postero-inferior glenoid margin, forms part of the labral complex, which is the main anterior stabiliser of the shoulder. The IGHL has a U-shaped appearance with the lateral attachment at the anatomic neck of the humerus. Intra-articular fluid or contrast medium is necessary for evaluation of the IGHL-labral complex. When detachment of the ligament from the humerus (infero-medially) occurs, fluid leaks between the humerus and the torn ligament or capsule, and the U-shaped capsule develops a J-shaped appearance.
Tears of the IGHL can also involve the midportion of the ligament or the glenoid attachment. This involvement, with or without associated labral tears, leads to anterior instability and predisposes to recurrent subluxation and dislocation.
Teaching point
Look for the J sign (HAGL lesion) on coronal MRI sequence when there is a history of anterior shoulder instability.
Conclusion
The humeral attachment of the joint capsule and IGHL are important stabilisers of the antero-inferior glenohumeral joint. This area is an important checkpoint when there is a history of anterior shoulder instability. It is important to be familiar with the J sign as it suggests an IGHL humeral attachment tear.
Acknowledgements
I thank Drs S.A. Peach, M.D. Velleman and S. Miller, and M. Robbertse and D. Coetzee, for their contributions.
Competing interests
The author declares that he has no financial or personal relationship(s) that may have inappropriately influenced him in writing this article.
References
1. Stoller DW. Magnetic resonance imaging in orthopaedics and sports medicine, volume 2. 3rd edn. Philadelphia: Lippincott Williams & Wilkens, 2007; p. 1324-1352. [ Links ]
2. Carlson CL. The 'J' sign. Radiology. 2004;232(3):725-726. http://dx.doi.org/10.1148/radiol.2323021239 [ Links ]
 Correspondence:
Correspondence:
Pieter Oberholzer
Private Bag X24270
Gezina 0031
South Africa
Email: oberp@mweb.co.za
Received: 04 Aug. 2014
Accepted: 29 Oct. 2014
Published: 05 Dec. 2014

