










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of HIV Medicine
On-line version ISSN 2078-6751
Print version ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.24 n.1 Johannesburg 2023
http://dx.doi.org/10.4102/sajhivmed.v24i1.1508
ORIGINAL RESEARCH
Confronting the human papillomavirus-HIV intersection: Cervical cytology implications for Kenyan women living with HIV
James M. KangetheI, II, III; Stephen GichuhiIV; Eddy OdariV; Jillian PintyeVI; Kenneth MutaiIII; Leila AbdullahiVII; Alex MaiyoVIII; Marianne W. MureithiII, IX
IConsortium for Advanced Research Training in Africa (CARTA), Nairobi, Kenya
IIDepartment of Medical Microbiology and Immunology, Faculty of Health Sciences, University of Nairobi, Kenya
IIIComprehensive Care Center for HIV, Kenyatta National Hospital, Nairobi, Kenya
IVDepartment of Ophthalmology, Faculty of Health Sciences, University of Nairobi, Nairobi, Kenya
VDepartment of Medical Microbiology, Faculty of Health Sciences, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
VIDepartment of Biobehavioral Nursing and Health Informatics, University of Washington, Seattle, United States of America
VIIResearch and Policy Development, African Institute for Development Policy, Nairobi, Kenya
VIIICenter for Virus Research, Kenya Medical Research Institute, Nairobi, Kenya
IXKAVI Institute of Clinical Research, Faculty of Health Sciences, University of Nairobi, Nairobi, Kenya
ABSTRACT
BACKGROUND: High-risk human papillomavirus (HR-HPV) is the primary cause of cervical cancer, leading to over 311 000 global deaths, mainly in low- and middle-income countries. Kenyan women living with HIV (WLHIV) face a disproportionate burden of HR-HPV.
OBJECTIVES: We determined the prevalence of HR-HPV infections and their association with cervical cytology findings among Kenyan WLHIV.
METHOD: We conducted a cross-sectional study among WLHIV attending the HIV care and treatment clinic at the Kenyatta National Hospital (KNH), Kenya's national referral hospital. Study nurses collected a cervical sample with a cytobrush for HR-HPV genotyping using Gene Xpert® assays and HPV Genotypes 14 Real-TM Quant V67-100FRT. Bivariate analysis explored the associations.
RESULTS: We enrolled 647 WLHIV (mean age of 42.8 years), with 97.2% on antiretroviral therapy (ART) and 79% with a suppressed viral load (< 50 copies/mL plasma). The prevalence of any and vaccine-preventable HR-HPV was 34.6% and 29.4%, respectively, with HPV 52 being the most common genotype (13.4%). Among WLHIV with HR-HPV infections, 21.4% had abnormal cervical cytology. Women with multiple HR-HPV infections were more likely to have abnormal cytology compared to those with single HR-HPV infections (34.9 vs 9.3%, adjusted odds ratio [aOR] = 6.2, 95% confidence interval [CI]: 2.7-14.1, P = 0.001). Women with HR-HPV infection (single or multiple) were more likely to be on the second-line ART regimen compared to those without HR-HPV infections (53.1% vs 46.7%, aOR = 2.3, 95% CI: 1.3-4.1, P = 0.005.
CONCLUSION: Among WLHIV at KNH, abnormal cytology was common and more frequent among women with multiple HR-HPV infections.
Keywords: high-risk human papillomavirus; cervical cytology; cervical cancer; women living with HIV; antiretroviral therapy; Kenya.
Introduction
Cervical cancer is one of the AIDS-defining cancers and is ranked fourth among the most common cancers affecting women worldwide.1,2 In the year 2020, over 550 000 incidental cases of cervical cancer were reported, with a staggering 90% of these cases and 300 000 cervical cancer-related deaths occurring in low-income countries.3 Persistent infection with high-risk human papillomavirus (HR-HPV) types is responsible for more than 70% of global cervical cancer cases, with varying prevalence rates of HR-HPV infections observed among different countries.4,5 In a global context, eastern, western and southern African regions exhibit the highest incidence rates of cervical cancer, with age-standardised rates of 34.5, 33.7, and 26.8 cases per 100 000 populations, respectively. In Kenya, the annual incidence rate of cervical cancer is 15 cases per 100 000 women, and the corresponding annual mortality rate is 12 deaths per 100 000 women.6 This substantial disease burden can largely be attributed to insufficient access to screening services and suboptimal screening uptake rates, stemming from limited knowledge or apprehensions regarding cervical cancer and HR-HPV screening among women. Other factors that have led to a high HR-HPV disease burden include low vaccine coverage and high rates of HIV and HPV co-infection as well as limited access to screening services.7,8
The persistence of HR-HPV infections can result in the development of cervical lesions. Pre-cervical cancer lesions and cervical cancer lesions are most frequently observed in women aged 30 years and above,9 indicating that the infection occurs earlier in life and progresses slowly to cancer. Metaplastic changes in the endocervix continue to occur throughout a woman's lifetime, with the period of greatest activity coinciding with the highest risk of HPV infection during puberty and the first pregnancy. Metaplastic changes gradually decline after menopause.10,11 Precancerous stages or pre-invasive precursor lesions are graded based on cytological examination and include atypical squamous cells of undetermined significance (ASCUS), low-grade squamous intraepithelial lesions (LSIL), high-grade squamous intraepithelial lesions (HSIL), and invasive cervical cancer (ICC).12,13,14
Women living with HIV are at a disproportionate risk of acquiring HR-HPV infections, harbouring multiple HR-HPV infections, and developing persistent infections that can result in abnormal cervical lesions due to their compromised immune status.15,16 In contrast, HR-HPV infections in HIV-negative women may be cleared in some individuals by the stable cell-mediated immune system or tend to regress.17 Although antiretroviral therapy (ART) has been associated with a decrease in the incidence of other AIDS-defining cancers, its impact on cervical lesions remains unclear. In HIV-infected women, cervical lesions and the progression to malignancy tend to occur at an earlier age (around 20-25 years) when there is immunosuppression and when other competing health factors are present. Due to the presence of multiple HR-HPV infections, invasive malignancies may progress more quickly to unusual locations and respond poorly to therapies. Additionally, the risk of recurrence from latent and sanctuary sites is high, resulting in a poor prognosis.18 The prevalence of HR-HPV infections among WLHIV on ART and resulting cervical cytology patterns remains unclear in low-income settings, with some studies reporting no effects of ART on cervical cancer.19
Primarily, cervical cancer is preventable through the vaccination of young girls aged 9-14 years with the HPV vaccine. The secondary prevention strategy for cervical cancer prevention is through cervical cancer screening among women aged 30 years and above, which has been implemented.20,21,22 However, annual reports indicate sustained cervical cancer incidental and mortality rates among WLHIV in the ART era in sub-Saharan Africa (SSA).6 The development of three different HPV vaccines that are strongly efficacious against some HR-HPV types offers protection against cervical infections caused by the HR-HPV genotypes in the vaccines as well as HPV-associated cancers and condylomas. The synergy between primary and secondary prevention efforts of cervical cancer among WLHIV is still unclear. One of the most neglected aspects of the potential effect of prophylactic vaccines in SSA is the evaluation of existing screening practices and existing HR-HPV genotypes. There may be unique challenges and considerations for this population regarding HPV vaccination and screening.6 Women living with HIV have a higher risk of developing HPV-related cancers due to their compromised immune systems, which may limit the effectiveness of the HPV vaccine.17 Furthermore, WLHIV may experience barriers to accessing both HPV vaccination and cervical cancer screening services due to stigma, discrimination, and limited healthcare resources.23 Therefore, it is crucial to consider these factors when implementing HPV vaccination and cervical cancer screening programmes for WLHIV.24
The World Health Organization (WHO) recommends novel approaches to increase the uptake and utilisation of cervical cancer screening and fast-track same-day 'test and treat' algorithms for WLHIV.25 The algorithm involves screening WLHIV for HR-HPV using a point-of-care HPV DNA molecular rapid platform, and, if the test is positive, performing visual inspection with acetic acid (VIA) and treating precancerous lesions with cryotherapy on the same day.25 HR-HPV DNA testing has been utilised as a screening and triage test due to its increased sensitivity.26,27 The algorithm can help to identify and treat precancerous lesions before they progress to cancer. The same-day treatment approach can also improve patient satisfaction and reduce the burden of multiple clinic visits. However, there are also potential barriers to implementing the 'test and treat' algorithm. One of the main challenges is the lack of trained healthcare providers and infrastructure in many low- and middle-income countries where the burden of HIV and cervical cancer is highest. The algorithm also requires reliable electricity, equipment, and supplies for HR-HPV DNA point-of-care consumables and cryotherapy, which may not be available in some settings.28 There is also a need for community engagement and education to increase awareness and uptake of cervical cancer screening among WLHIV.
There is limited information on the epidemiology of the current HR-HPV infections among WLHIV and the associated cervical cytology patterns in the ART era in SSA. With the increased risk of cervical abnormalities among WLHIV in Kenya and the further development of cervical cancer, there is an urgent need to invest more in interventions targeting HR-HPV genotype screening and prevention. These interventions largely require HR-HPV genotypes and cytological patterns data for effective implementation. Currently, there are no comprehensive insights into the prevalence rates and distribution of HR-HPV infections and their correlation with cervical cytology among Kenyan WLHIV enrolled for care and treatment.
Materials and methods
Study design and population
This cross-sectional study recruited WLHIV aged 18 years and above attending the ART clinic at Kenyatta National Hospital (KNH) from June 2021 to March 2022. Those who were willing to participate consented and were counselled on the benefits of cervical cancer screening. The study excluded the following participants: pregnant women, history of previous total hysterectomy, radiotherapy or chemotherapy, those currently menstruating, and those with abnormal vaginal bleeding.
Study site and procedures
Kenyatta National Hospital is the largest tertiary health facility in Kenya, with a bed capacity of 1800 and a bed occupancy rate of 90% - 95%. The ART clinic at KNH was established 20 years ago for the prevention and treatment of HIV and associated morbidities in men and women including adolescents and children. On average, the ART clinic offers services to nearly 10 000 clients, with the highest proportion being women. Cervical cancer screening commenced 12 years ago as part of integrated service for HIV care for WLHIV at the ART clinic. Trained nurses performed routine annual visual inspections with acetic acid or Lugols iodine (VIA or VILI). Women found to be positive are offered cryotherapy or loop electrosurgical excision (LEEP), depending on the accessibility to the transformation zone, by the gynaecologists upon referral to gynaecological specialised clinic at KNH. Cytological screening and HPV genotyping of high-risk types are not routinely done for patients.
In this study, eligible WLHIV were offered initial partial HPV testing using Gene Xpert® (Cepheid, Sunnyvale, California, United States [US]), and cytology smears were prepared for examination by a trained cyto-screener in the cytology laboratory at KNH. The additional individual HPV genotyping was done using HPV Genotypes 14 Real-TM Quant V67-100FRT (SACACE Biotechnologies®, Italy). Briefly, the study procedure involved face-to-face interviews after written informed consent was obtained. The interview covered sociodemographic, behavioural and sexual characteristics, history of HIV diagnosis, investigation, and treatment. Afterward, each participant was examined by a trained research nurse at the ART clinic, including a general physical and pelvic examination. In the lithotomy position, a nurse passed a sterile Cusco speculum to visualise the cervix, and a cytobrush was inserted into the endocervix and rotated 360 degrees twice. Part of the sample collected was used to prepare a slide for cytological assessment and the remaining samples were sent to the laboratory for HPV genotyping. The nurse also reviewed the HIV electronic medical records (EMR) of each participant and copied relevant information into the data collection form.
All participants had post-test counselling, irrespective of the HPV test and cervical cytology results. Women that had abnormal cytology using ASCUS classification (ASCUS: LSIL, HSIL, ICC) were referred to a gynaecologist for further evaluation and treatment based on KNH guidelines.
Sampling procedure
All eligible participants at the ART clinic were informed as a group about the study before the commencement of the clinic session. Women that signified intention to participate in the study had further discussions with a research assistant individually on the study objectives and procedure. At each clinic session, a sampling frame was generated from a list of all eligible women in attendance. We used a simple random sampling technique to select eligible women from the sampling frame. In this technique, random numbers generated from Excel were used to select women before consent was taken.
Biological sample storage and analysis
The slide for the cervical spear was prepared by the oncology-trained nurse using the standard protocol of KNH for Papanicolaou smear preparation. The prepared slides were shipped to the cytopathology laboratory for staining and reading by a cytopathologist. The results were interpreted using the Bethesda system.14 The leftover smear sample in the brush was placed in a PreservCyt solution (Hologic Corp, Marlborough, Massachusetts, US) and taken to the laboratory for HPV detection of high-risk HPV types (16, 18, 45, and 11 other HR-HPVs) using the Xpert HPV platform (Cepheid, Sunnyvale, California, US). Thereafter, advanced individual HR-HPV genotyping was conducted. First, the DNA was extracted using a QIAamp DNA Mini Kit in accordance with the manufacturer's protocol (Qiagen, Crawley, United Kingdom [UK]). The HPV detection was done, and specific genotypes were then identified and interpreted using the HPV Genotypes 14 Real-TM Quant V67-100FRT kit (SACACE Biotechnologies®, Italy).
Data collection and analysis
Data collected were entered into the ODK tool kit and exported as a CSV file before importing into SPSS® version 23.0 (IBM Corp., Armonk, New York, US). Descriptive statistics were presented in frequencies and proportions for categorical variables and mean or median for continuous variables. The primary outcome of this study was the presence or absence of abnormal cervical cytology readings (LSIL, HSIL, and ICC). Bivariate analysis was also done to explore the association between sociodemographic, clinical characteristics, and lifestyle characteristics with having normal or abnormal cytology using Chi-square test of associations, after which a multivariate logistic regression model was built to adjust for potential confounders.
Results
Enrollment process
As depicted in Figure 1, among the 1080 WLHIV initially approached, 171 were deemed ineligible and 262 of the approached women declined to participate, citing time constraints, while others refrained from providing their reasons for non-participation. Consequently, a total of 647 WLHIV provided their consent and actively engaged in the study.

Social demographics, sexual and behaviour characteristics of the participants
Participant characteristics are shown in Table 1, the mean age of the participants was 42.8 years (standard deviation [s.d.]: 8.7) and the majority (40.5%) were aged from 35 years to 44 years. The mean age for sexual debut was 18.3 years (s.d.: 3.0) and 43% of the women had three or more children. Only 29.3% of the respondents were on a family planning method. Almost half of the respondents (43.4%) reported a history of sexually transmitted infection (STI) treatment in their sexual lifetime and 68.5% of the participants had a sexual partner currently or in the last 6 months. Most of the respondents (91.6%) had only one sexual partner and 46.7% of these sexual partners were HIV sero-reactive (HIV-concordant sexual partners). The majority of the participants (85.3%) reported that their sexual partners were circumcised. Only 1.1% of the participants were vaccinated against HPV.

An analysis of the clinical characteristics of the participants
As shown in Table 2, the majority of the participants (33.8%) were diagnosed with HIV when they were aged between 35 and 39 years. Viral load was suppressed (HIV-1 RNA viral load < 50 copies/mL plasma) in 79%, 12.3% had low-level viraemia (50 copies/mL - 999 copies/mL plasma) and 8.8% were unsuppressed (≥ 1000 copies/mL plasma). Approximately 37% of the participants had an absolute CD4 cell count of < 200 cells/µL. Almost all the participants (97.2%) were on ART, with 87.6% being on a dolutegravir-based regimen and 7.8% on second-line ART. Only 1.1% of the participants were HPV vaccinated. A few of the participants (20.9%) had missed their HIV clinical appointments and 25.5% had missed taking their daily ART at least once in the last 12 months.

Overview of the overall prevalence of HR-HPV infections among WLHIV
The prevalence of any and vaccine-preventable HR-HPV was 34.6% and 29.4%, respectively. As shown in Figure 2, the highest HR-HPV infection was type 52 (13.4%), followed by the types (in descending order): 16 (9.9%), 56 (9.6%), 18 (8.2%), 35 (7.7%), 51 (5.4%), 58 (4.5%), 68 (4.0%), 45 (3.6%), 66 (3.3%), 31 (2.9%), 33 (2.3%), 39 (2.2%), and 59 (1.7%).
Prevalence of HR-HPV among WLHIV across different age categories
Based on age categories, WLHIV aged less than 25 years had the highest rate of HR-HPV infections (46.7%) followed by those aged 35-44 years (36.6%). Those aged 55 years and above had the lowest rate of infection (26.6%), as shown in the Appendix.
Examining the pattern of abnormal cervical cytology among WLHIV having HR-HPV infections
Out of the 224 WLHIV having HR-HPV infections, 21.4% had abnormal cervical cytology. Of those with abnormal cytology, 56% had ASCUS, 12% had LSIL, 19% had HSIL and 13% had ICC, as shown in Figure 3.

The relationship between cervical cytology and HR-HPV infections among WLHIV
Among WLHIV with normal cervical cytology, the most dominant HR-HPV genotype was HPV 52 (30.7%). Participants having ASCUS had HR-HPV type 56 as the most detected genotype (81.5%), those with LSIL had HR-HPV 16 dominating (66.7%), and HR-HPV 31 dominated in HSIL (66.7%). Women living with HIV with cervical cancer had HR-HPV type 16 and 52 equally dominating (50% each), as shown in Table 3.
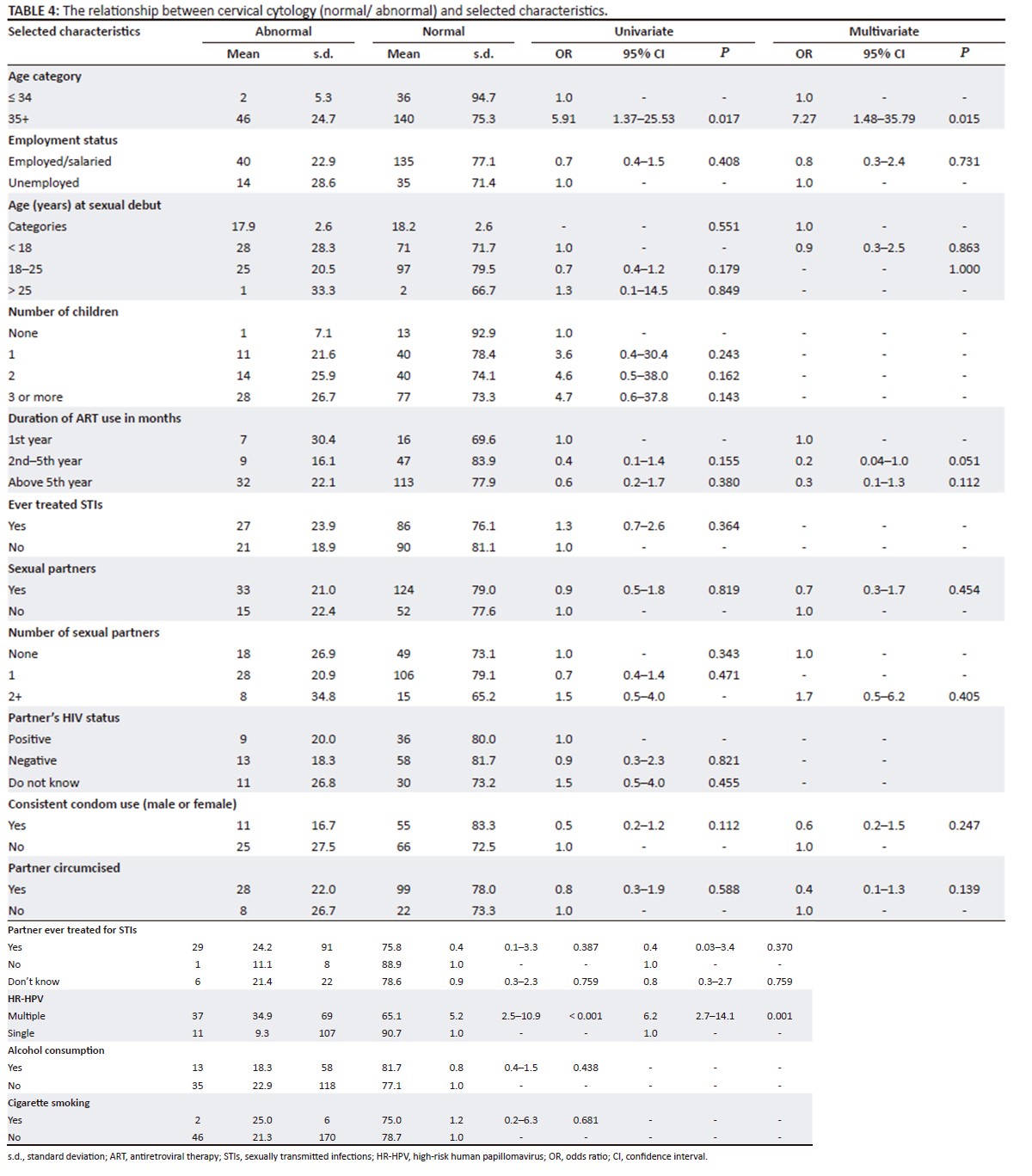
The relationship between cervical cytology (normal/abnormal) and selected characteristics
Participants aged 35 years and above were more likely to have abnormal cytology (24.7% vs 5.3%, adjusted odds ratio [aOR] = 7.27, 95% CI: 1.48-35.79, P = 0.015). Women living with HIV with multiple HR-HPV infections were more likely to have abnormal cytology as compared to those with single HR-HPV infections (34.9% vs 9.3%, aOR = 6.2, 95% CI: 2.7-14.1, P = 0.001). No other risk factor was significantly associated with abnormal cytology, as shown in Table 4.
Association between HIV-related characteristics and HR-HPV infections among WLHIV
Women living with HIV having HR-HPV infection (single or multiple) were more likely to be on second-line ART regimen compared to those without HR-HPV infection (53.1% vs 46.7%, aOR = 2.3, 95% CI: 1.3-4.1, P = 0.005).
Discussion
HPV is the most prevalent STI worldwide and is a well-known risk factor for the development of cervical cancer, especially in WLHIV.29 Antiretroviral therapy has been shown to reduce the incidence of other AIDS-defining cancers in WLHIV, but the prevalence of HR-HPV infections in this population is still a significant concern.6 In this current study, we aimed to investigate the prevalence of HR-HPV infections in WLHIV enrolled in ART care and their correlation with cervical cytology patterns. The prevalence of HR-HPV infections in our participants was 34.6%, which is lower than the prevalence reported in other studies conducted in SSA, which ranged from 54% to 81%.16,30 The difference in the prevalence of HR-HPV infections might be explained by the groups examined in earlier research that included WLHIV who had established cervical cancer.16,31,32 We enrolled participants without any cervical abnormalities, and the prevalence of HR-HPV infections was detected through screening. A high proportion (21.4%) of the participants with HR-HPV infections in our study were discovered to have different types of cervical abnormalities. This finding emphasises the importance of regular cervical cancer screening in WLHIV.
We found that HPV 52 was the most common HR-HPV genotype (13.4%), followed by types 16 (9.9%) and 18 (8.2%), while HPV 59 was the least prevalent (1.7%). Notably, types 16, 18 and 45 were not dominant in this study, a trend observed in other studies among WLHIV and the general population in the region.33,34 This finding is notable because these three HPV types are the most oncogenic and are responsible for the majority of cervical cancer cases worldwide. The lower prevalence of types 16, 18 and 45 in our study may be due to regional differences in HPV prevalence or differences in the population studied, differences in the sample size, and laboratory methods used for HR-HPV testing.26 Additionally, it is plausible that the prevalence of distinct HR-HPV genotypes exhibits temporal variations due to shifts in sexual practices or variances in HPV vaccination rates across diverse populations.8 The immune status of the WLHIV participants may have played a role in the different distribution of HR-HPV genotypes observed in this study. This highlights the need to focus on other HR-HPV infections in addition to types 16, 18, and 45 in WLHIV enrolled for ART care.
Previous studies in Kenya have also reported a high prevalence of HR-HPV 52 and 35.34,35 Cervical abnormalities from additional HR-HPVs have received little attention in low-income settings, indicating the importance of individual genotyping of all HR-HPV types and implementation point-of-care molecular screening in the same-day screen-and-treat strategy for cervical cancer screening among WLHIV. Screening for a limited subset of HR-HPV genotypes may not optimally identify those at risk of infection and cervical lesion development. According to the findings of this research, WLHIV face a heightened vulnerability to contracting multiple HR-HPV infections, such as HPV 52 and other HR-HPV genotypes that are not safeguarded by the existing Cervarix or quadrivalent Gardasil HPV vaccines offered in Kenya. Given these circumstances, there is a pressing requirement to initiate HPV vaccination using Gardasil-9, which has demonstrated comparable or superior efficacy against seven HR-HPV types.36,37,38
This study found that young WLHIV aged < 25 years had the highest prevalence of HR-HPV infection (46.7%). This increased prevalence among young women may be due to their heightened susceptibility to HR-HPV as a result of early sexual debut and increased sexual activity. Though not statistically significant in this study, participants who had their first sexual debut before 18 years of age were more likely to have HR-HPV infections as compared to others. Similar findings were reported by Guthrie et al. among WLHIV in discordant relationships in Kenya.34 While HR-HPV infections among young women may regress with time due to viral transience, persistence or latency may also occur, which could increase the risk of developing cervical cancer over time.39 These findings suggest the need for targeted interventions to address the high prevalence of HR-HPV infections among young WLHIV, particularly those aged less than 25 years. Such interventions should focus on promoting safe sexual practices, HPV vaccination, early detection and treatment of HR-HPV infections, and related conditions, such as abnormal cervical cytology. Therefore, ongoing monitoring and screening for HR-HPV infections and related conditions are critical for the long-term health of WLHIV, especially those in the younger age group. In addition, it was observed that among WLHIV aged 35 years and over, there is an increased prevalence of abnormal cytology in the presence of HR-HPV infections. The heightened occurrence of abnormal cytology can be attributed to the persistent and reactivated state of latent HR-HPV infections, which were acquired during earlier sexual activity. Therefore, it is inadequate to rely solely on HPV vaccination as an intervention to eliminate HR-HPV infections and cervical cancer. It is imperative to implement adequate routine cervical cancer screening, as emphasised by the Ministry of Health and Cubie and Campbell, to enable timely detection and management of cervical cancer in this vulnerable population.40,41
The immunocompromised state of WLHIV makes them susceptible to HR-HPV infections with increased persistence, leading to a higher incidence of cervical lesions compared to HIV-negative women. Kelly et al.,15 in their study among WLHIV in South Africa and Burkina Faso, demonstrated this vulnerability. Our study also found abnormal cytology in 21.4% of WLHIV with detectable HR-HPV infections, of which 68% were low-grade precancerous lesions and 32% were high-grade pre-cancer lesions. However, the prevalence of cervical lesions in our study was lower than that reported by Guthrie et al.34 in their study of WLHIV in discordant relationships in Kenya. Importantly, it is worth noting that spontaneous regression of cervical lesions is common in over 75% of women, and thus, these lesions should be viewed as reflective of an infection rather than a disease stage or progression. This implies that the interpretation of cervical lesions should be done carefully to prevent stigmatisation, anxiety, and fear among the screened women. Furthermore, clearance of HR-HPV infections should also be approached with caution since it may be misinterpreted as an inability of the screening method used to detect existing HPV infections, as Krings et al. emphasised.42
In the context of WLHIV, the co-occurrence of multiple HR-HPV infections is frequently observed. The findings of this study demonstrate a significant correlation between the presence of multiple HR-HPV infections and abnormal cervical cytology. This outcome is consistent with a prior investigation conducted in South Africa, which evaluated WLHIV with cervical intraepithelial neoplasia and found a similar association.16 Menon et al., in their study conducted in Western Kenya, demonstrated a 2.3-fold higher prevalence of cervical lesions in individuals with multiple HR-HPV infections compared to those with a single HR-HPV infection.19 This finding provides evidence to support the hypothesis that the presence of multiple HR-HPV infections increases the risk of developing pre-cervical cancer lesions if HR-HPV infections do not regress. The coexistence of multiple HR-HPV infections may lead to a higher HR-HPV viral load, increased persistence of the virus, and increased oncogenic potential, resulting in an increased likelihood of developing cervical lesions.19 Taken together, these results underscore the importance of vigilant monitoring for the presence of multiple HR-HPV infections among WLHIV, as they may serve as a predictor for the development of cervical lesions if they do not regress naturally or are managed promptly. The South African study further reported that participants with multiple HR-HPV infections were found to exhibit inadequate responses to therapy. This highlights the urgent need for increased investment in HR-HPV vaccinations, particularly among eligible girls, to prevent the occurrence of multiple infections. This recommendation aligns with the findings of a study conducted by Haque and colleagues, which reviewed insights and solutions for the elimination of HR-HPV infections and cervical cancer in SSA.43 The implementation of comprehensive vaccination programmes targeting multiple HR-HPV types has the potential to substantially reduce the burden of cervical cancer in this region. In the current study, only 1.1% of the participants had been vaccinated for HPV. This is similar to previous research conducted in Kenya on the uptake of the HPV vaccine, which reported poor uptake of the vaccine (33% for the first dose and 16% for the second dose). The poor uptake was associated with lack of awareness and education about the virus. In addition, their study also found that only 30% of parents had heard of the HPV vaccine, and only 13% had knowledge of its purpose. This lack of knowledge and awareness can lead to misconceptions about the vaccine and, ultimately, low uptake. To address this barrier, public education campaigns and community outreach programmes could be implemented to increase knowledge and awareness about the HPV vaccine.44 Cultural beliefs and practices have also been identified as barriers to HPV vaccine uptake in Kenya. Some parents believe that the HPV vaccine could encourage sexual promiscuity among their daughters, which goes against their cultural values. Additionally, some parents believe that the HPV vaccine is not necessary because their daughters are not sexually active.45 In addressing this barrier, it is important to engage with local communities and involve cultural leaders in public education campaigns. The cost of the vaccine has also been identified as a barrier to HPV vaccine uptake in Kenya for adolescent girls aged >14 years. Many parents do not have health insurance and are not able to access the vaccine through the national immunisation programme.46 It may be necessary to explore alternative financing mechanisms, such as public-private partnerships or donor funding, to increase access to the vaccine. Fear of side effects is another barrier to HPV vaccine uptake in Kenya. Some parents are concerned about the safety of the HPV vaccine and are worried about potential side effects, including the future fertility impacts on young girls. This fear can lead to low uptake of the vaccine, despite its proven effectiveness.47
Despite the decreasing incidence of other AIDS-defining cancers, HR-HPV infections and cervical lesions have not shown a similar decline among WLHIV who are using ART.48 Specifically, our study found that 22.1% of the participants had been on ART for more than five years and had abnormal cervical cytology results. These findings highlight the ongoing need for continued research and interventions to address the complex health needs of WLHIV, including the potential for co-infections and comorbidities such as HPV-related conditions. In the present study, there was also no significant association between unsuppressed viral load and HR-HPV infections. This denotes that there was no relationship between HR-HPV infections or abnormal cervical cytology, and poor HIV treatment outcomes indicated by the unsuppressed viral load. Contrary to our findings, other studies reported that women on ART for a shorter period and those with unsuppressed HIV viral loads were associated with increased HR-HPV infections and cervical abnormalities.15 In 2017, the WHO recommended immediate ART initiation, regardless of the WHO clinical stage or CD4 count.49 Thus, women on ART have an increased life expectancy due to less competing risk of dying from opportunistic infections. Due to the improved cell-mediated immune status leading to prolonged life, incidences of HR-HPV infections, persistence, and later development to cervical lesions could be on the rise.50
The acquisition of new HR-HPV infections among WLHIV may be linked to having multiple sexual partners, according to research conducted by Brown and Weaver.51 Although we found there was no statistical association between the number of sexual partners and HR-HPV infection rates in the overall population, 34.8% of the respondents had two or more sexual partners, which could have led to increased HR-HPV infections and abnormal cytology. Other studies have also reported a higher risk of HR-HPV infections among individuals with multiple sexual partners, such as Okunade et al. and Wencel-Wawrzeńczyk et al.52,53 The present study found that condom use was not significantly associated with either HR-HPV infections or abnormal cytology. However, lack of condom use in conjunction with multiple sexual partners have been linked to an increased risk of STIs such as HR-HPV infections with progression to abnormal cytology. A study conducted among women of reproductive age in Gambia reported an increased risk of HPV infections among participants with multiple sexual partners and those who did not use condoms.39 These findings suggest that interventions aimed at reducing the number of sexual partners and promoting condom use may be effective in reducing the risk of acquiring new HR-HPV infections among WLHIV.
Alcohol consumption and cigarette smoking have also been linked to new HR-HPV infections and persistence, as noted in research conducted by Soh et al.54 Smoking has been shown to impair the function of Langerhans cells, which act as immune cells in the cervical region, thus increasing the vulnerability of smoking women to HR-HPV infections. This was observed in studies conducted by Skinner et al.55 and Mayaud et al.8 In the present study, approximately 18.3% of the participants with abnormal cytology were using alcohol, and 25% smoked cigarettes. However, these lifestyle factors were not statistically significant. Tobacco-associated carcinogens have also been found in the genital tract of women and may act as co-factors for the development of cervical lesions, particularly in the presence of other coexisting factors such as HIV infection and alcohol consumption.56,57
Lifestyle-related factors, such as early initiation of sexual intercourse, cigarette smoking, and promiscuity, have been found to increase the risk of HR-HPV infections and progression to cervical lesions in alcoholic women.58,59,60 This suggests that interventions targeting these risk factors could be effective in reducing the incidence and persistence of HR-HPV infections and associated complications.
One of the strengths of this study is the inclusion of a relatively large sample of WLHIV with factors associated with HR-HPV infections and cervical cytology. However, it is important to acknowledge certain limitations of our study. Firstly, it was limited to WLHIV who are currently receiving ART and, therefore, the findings may not apply to women who are not on ART. According to Kenya Ministry of Health data, 96.6% of WLHIV who know their status in Kenya are currently on ART and therefore our sample is representative of most WLHIV in this setting. Additionally, since this was a facility-based study, the results may not be representative of the general population, where ART use may be less common. Without ascertaining any reason why, over 200 eligible women declined enrollment. The decliners were younger, aged 18-22 years. We were not able to send WLHIV with HR-HPV for histology or colposcopy, although participants with abnormal cytology were referred to the gynae-oncology clinic for further management and follow-up. Exploring the relationship between histology or colposcopy findings and HPV positivity among WLHIV would be an intriguing area to investigate further. Such research could provide insights into the diagnostic utility of combining these modalities and help optimise screening and management strategies for cervical abnormalities. We also suggest conducting future investigations to establish a correlation between multizonal HPV disease and WLHIV who initiate ART with a low CD4 count.
Conclusion
This study found that more than one-third of WLHIV had HR-HPV infections. There was a strong correlation between the presence of abnormal cervical cytology and having multiple HR-HPV infections, regardless of ART duration, CD4 count and behavioural factors. It is noteworthy that HR-HPV genotypes 52 and 35 were found to have a higher prevalence, emphasising the importance of considering all HR-HPV genotypes in cervical cancer prevention, management, and elimination efforts. Furthermore, a majority of respondents with HR-HPV infections exhibited ASCUS. Overall, this study underscores the importance of ongoing monitoring and screening for HR-HPV infections and related conditions for the long-term health of WLHIV.
Acknowledgements
The authors express their gratitude to the Medical Research, Training and Innovation Department at KNH for technical support during the study. Technical guidance and support during the data collection phase from Jerusha Malubi and Lydi Ivita are also acknowledged. The study participants are appreciated for their substantial support.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in conducting this research study and writing this article.
Authors' contributions
The study was conceptualised and designed by J.M.K., S.G., E.O., J.P., K.M. and M.M. Data collection was conducted in the field by J.M.K. and A.M. Data analysis was performed by J.M.K., K.M, J.P., S.G., E.O. and M.M. All authors contributed to the manuscript's development, reviewed and edited it, and gave their final approval.
Ethical considerations
Ethical approval (P552/10/2020) was obtained from the Kenyatta National Hospital - University of Nairobi Ethics and Research Committee (KNH-UoN ERC) in February 2021 for studies involving human participants. Procedures complied with institutional and national research committee ethical standards, as well as the 1964 Helsinki Declaration and its subsequent revisions or equivalent ethical guidelines.
Funding information
This research study and J.M.K., a graduate research fellow, were supported by the Consortium for Advanced Research Training in Africa (CARTA), which is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No. G-19-57145), Sida (Grant No:54100113), Uppsala Monitoring Center, Norwegian Agency for Development Cooperation (Norad), and by the Wellcome Trust [reference no. 107768/Z/15/Z] and the UK Foreign, Commonwealth & Development Office, with support from the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) programme. The statements made and views expressed are solely the responsibility of the Fellow. Additionally, the study was supported by the Union for African Population Studies (UAPS)- AFRES DATA Programme and the HIV Research Trust.
Data availability
The data sets utilised and evaluated during the present investigation can be obtained from J.M.K., the corresponding author, upon reasonable request.
Disclaimer
The authors are solely accountable for the statements made and opinions expressed, and they do not represent an official stance of the institution or funder.
References
1.Clifford GM, Franceschi S, Keiser O, et al. Immunodeficiency and the risk of cervical intraepithelial neoplasia 2/3 and cervical cancer: A nested case-control study in the Swiss HIV cohort study. Int J Cancer. 2016;138(7):1732-1740. https://doi.org/10.1002/ijc.29913 [ Links ]
2.World Health Organization. Comprehensive cervical cancer control [homepage on the Internet]. 2014 [cited 2023 Mar 28]; p. 366-378. Available from: http://apps.who.int/iris/bitstream/10665/144785/1/9789241548953_eng.pdf?ua=1 [ Links ]
3.Arbyn M, Simon M, Peeters E, et al. 2020 List of human papillomavirus assays suitable for primary cervical cancer screening. Clin Microbiol Infect. 2021;27(8):1083-1095. https://doi.org/10.1016/j.cmi.2021.04.031 [ Links ]
4.De Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob Health. 2020;8(2):e180-e190. https://doi.org/10.1016/S2214-109X(19)30488-7 [ Links ]
5.Stelzle D, Tanaka LF, Lee KK, et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob Health. 2021;9(2):e161-e169. https://doi.org/10.1016/S2214-109X(20)30459-9 [ Links ]
6.Ermel A, Tonui P, Titus M, et al. A cross-sectional analysis of factors associated with detection of oncogenic human papillomavirus in human immunodeficiency virus-infected and uninfected Kenyan women. BMC Infect Dis. 2019;19(1):1-8. https://doi.org/10.1186/s12879-019-3982-7 [ Links ]
7.Gatumo M, Gacheri S, Sayed AR, Scheibe A. Women's knowledge and attitudes related to cervical cancer and cervical cancer screening in Isiolo and Tharaka Nithi counties, Kenya: A cross-sectional study. BMC Cancer. 2018;18(1):745. https://doi.org/10.1186/s12885-018-4642-9 [ Links ]
8.Mayaud P, Boily M, Brock PM, Brisson M, Drolet M. Evidence of synergistic relationships between HIV and Human Papillomavirus (HPV): Systematic reviews and meta-analyses of longitudinal studies of HPV acquisition and clearance by HIV status, and of HIV acquisition by HPV status. Geneva: Wiley; International AIDS Society; 2018. [ Links ]
9.Liu Y, Ang Q, Wu H, et al. Prevalence of human papillomavirus genotypes and precancerous cervical lesions in a screening population in Beijing, China: Analysis of results from China's top 3 hospital, 2009-2019. Virol J. 2020;17(1):1-10. https://doi.org/10.1186/s12985-020-01383-1 [ Links ]
10.Deng H, Hillpot E, Mondal S, Khurana KK, Woodworth CD. HPV16-immortalized cells from human transformation zone and endocervix are more dysplastic than ectocervical cells in organotypic culture. Sci Rep. 2018;8:15402. https://doi.org/10.1038/s41598-018-33865-2 [ Links ]
11.Doorbar J, Gri H. Re fi ning our understanding of cervical neoplasia and its cellular origins. Papillomavirus Res. 2019;7:176-179. https://doi.org/10.1016/j.pvr.2019.04.005 [ Links ]
12.Mane A, Nirmalkar A, Risbud AR, Vermund SH, Mehendale SM, Sahasrabuddhe VV. HPV genotype distribution in cervical intraepithelial Neoplasia among HIV-infected women in Pune, India. PLoS One. 2012;7(6):e38731. https://doi.org/10.1371/journal.pone.0038731 [ Links ]
13.Cubie HA. Diseases associated with human papillomavirus infection. Virology. 2013;445(1-2):21-34. https://doi.org/10.1016/j.virol.2013.06.007 [ Links ]
14.Pangarkar MA. The Bethesda System for reporting cervical cytology. Cytojournal. 2022;19:28. https://doi.org/10.25259/CMAS_03_07_2021 [ Links ]
15.Kelly HA, Sawadogo B, Chikandiwa A, et al. Epidemiology of high-risk human papillomavirus and cervical lesions in African women living with HIV/AIDS: Effect of anti-retroviral therapy. AIDS. 2017;31(2):273-285. https://doi.org/10.1097/QAD.0000000000001301 [ Links ]
16.Taku O, Mbulawa ZZA, Phohlo K, Garcia-Jardon M, Businge CB, Williamson AL. Distribution of human papillomavirus (HPV) genotypes in HIV-negative and HIV-positive women with cervical intraepithelial lesions in the Eastern Cape Province, South Africa. Viruses. 2021;13(2):1-14. https://doi.org/10.3390/v13020280 [ Links ]
17.Liu G, Mugo NR, Bayer C, et al. Impact of catch-up human papillomavirus vaccination on cervical cancer incidence in Kenya: A mathematical modeling evaluation of HPV vaccination strategies in the context of moderate HIV prevalence. Lancet. 2022; 45:101306. https://doi.org/10.2139/ssrn.3935689 [ Links ]
18.Weldegebreal F, Worku T. Precancerous cervical lesion among HIV-positive women in sub-Saharan Africa: A systematic review and meta-analysis. Cancer Control. 2019;26(1):1-11. https://doi.org/10.1177/1073274819845872. PMID: 31043067, PMCID: PMC6572896. [ Links ]
19.Menon S, Luchters S, Rossi R, et al. Human papilloma virus correlates of high grade cervical dysplasia in HIV-infected women in Mombasa, Kenya: A cross-sectional analysis. Virol J. 2018;15(1):54. https://doi.org/10.1186/s12985-018-0961-3 [ Links ]
20.Barnabas RV, Brown ER, Onono MA, et al. Efficacy of single-dose human papillomavirus vaccination among young African women. NEJM Evid. 2022;1(5):EVIDoa2100056. https://doi.org/10.1056/EVIDoa2100056 [ Links ]
21.Machalek D, Rees H, Chikandiwa A, et al. Impact of one and two human papillomavirus (HPV) vaccine doses on community-level HPV prevalence in South African adolescent girls: Study protocol and rationale for a pragmatic before-after design On behalf of the HOPE Study team. BMJ Open. 2022;12(2):59968. https://doi.org/10.1136/bmjopen-2021-059968 [ Links ]
22.WHO. The cancer we can eliminate - WHO/Europe urges Member States to consign cervical cancer to history [homepage on the Internet]. 2022 [cited 2022 Oct 31]. Available from: https://www.who.int/europe/news/item/12-09-2022-the-cancer-we-can-eliminate---who-europe-urges-member-states-to-consign-cervical-cancer-to-history [ Links ]
23.Wong JPH, Vahabi M, Miholjcic J, et al. Knowledge of HPV/cervical cancer and acceptability of HPV self-sampling among women living with HIV: A scoping review. Curr Oncol. 2018;25(1):e73. https://doi.org/10.3747/co.25.3855 [ Links ]
24.Hampson IN. Effects of the prophylactic HPV vaccines on HPV type prevalence and cervical pathology. Viruses. 2022;14(4):757. https://doi.org/10.3390/v14040757 [ Links ]
25.WHO. Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: Recommendations for a public health approach. Geneva: World Health Organization; 2021, 594 p. [ Links ]
26.Koliopoulos G, Vn N, Santesso N et al. Cytology versus HPV testing for cervical cancer screening in the general population (Review) summary of findings for the main comparison. Cochrane Database Syst Rev. 2018;(8):CD008587. https://doi.org/10.1002/14651858.CD008587.pub2 [ Links ]
27.Asare M, Abah E, Obiri-Yeboah D, Lowenstein L, Lanning B. HPV self-sampling for cervical cancer screening among women living with HIV in low- and middle-income countries: What do we know and what can be done? Healthcare (Switzerland). 2022;10(7):1270. https://doi.org/10.3390/healthcare10071270 [ Links ]
28.Cubie HA, Morton D, Kawonga E, et al. HPV prevalence in women attending cervical screening in rural Malawi using the cartridge-based Xpert® HPV assay. J Clin Virol. 2017;87:1-4. https://doi.org/10.1016/j.jcv.2016.11.014 [ Links ]
29.Badial RM, DIas MC, Stuqui B, et al. Detection and genotyping of human papillomavirus (HPV) in HIV-infected women and its relationship with HPV/HIV co-infection. Medicine (United States). 2018;97(14):e9545. https://doi.org/10.1097/MD.0000000000009545 [ Links ]
30.Okoye JO, Ofodile CA, Adeleke OK, Obioma O. Prevalence of high-risk HPV genotypes in sub-Saharan Africa according to HIV status: A 20-year systematic review. Epidemiol Health. 2021;43:e2021039. https://doi.org/10.4178/epih.e2021039 [ Links ]
31.Castellsagué X, Ault KA, Bosch FX, et al. Human papillomavirus detection in cervical neoplasia attributed to 12 high-risk human papillomavirus genotypes by region. Papillomavirus Res. 2016;2:61-69. https://doi.org/10.1016/j.pvr.2016.03.002 [ Links ]
32.Menon SS, Rossi R, Harebottle R, Mabeya H, Vanden Broeck D. Distribution of human papillomaviruses and bacterial vaginosis in HIV positive women with abnormal cytology in Mombasa, Kenya. Infect Agent Cancer. 2016;11(1):1-9. https://doi.org/10.1186/s13027-016-0061-1 [ Links ]
33.De Vuyst H, Mugo NR, Chung MH, et al. Prevalence and determinants of human papillomavirus infection and cervical lesions in HIV-positive women in Kenya. Br J Cancer. 2012;107(9):1624-1630. https://doi.org/10.1038/bjc.2012.441 [ Links ]
34.Guthrie BL, Rositch AF, Cooper JA, et al. Human papillomavirus and abnormal cervical lesions among HIV-infected women in HIV-discordant couples from Kenya. Sex Transm Infect. 2019;96(6):457-463. https://doi.org/10.1136/sextrans-2019-054052 [ Links ]
35.Sweet K, Bosire C, Sanusi B, et al. Prevalence, incidence, and distribution of human papillomavirus types in female sex workers in Kenya. Int J STD AIDS. 2020;31(2):109-118. https://doi.org/10.1177/0956462419884454 [ Links ]
36.Kombe Kombe AJ, Li B, Zahid A, et al. Epidemiology and burden of human papillomavirus and related diseases, molecular pathogenesis, and vaccine evaluation. Front Public Health. 2021;8:1003. https://doi.org/10.3389/fpubh.2020.552028 [ Links ]
37.Goodman E, Reuschenbach M, Kaminski A, Ronnebaum S. Human papillomavirus vaccine impact and effectiveness in six high-risk populations: A systematic literature review. Vaccines. 2022;10(9):1543. https://doi.org/10.3390/vaccines10091543 [ Links ]
38.Barnabas RV, Brown ER, Onono MA, Bukusi EA, Njoroge B, Winer RL, et al. Efficacy of single-dose human papillomavirus vaccination among young African women. NEJM Evidence. 2022;1(5). https://doi.org/10.1056/evidoa2100056 [ Links ]
39.Camara HB, Anyanwu M, Wright E, Kimmitt PT. Human papilloma virus genotype distribution and risk factor analysis amongst reproductive-age women in urban Gambia. J Med Microbiol. 2018;67(11):1645-1654. https://doi.org/10.1099/jmm.0.000848 [ Links ]
40.Ministry of Health Kenya. National Cancer Screening Guidelines [homepage on the Internet]. 2018 [cited n.d.]; p. 2-122. Available from: https://arua-ncd.org/wp-content/uploads/2022/10/National-Cancer-Screening-Guidelines-2018.pdf [ Links ]
41.Cubie HA, Campbell C. Cervical cancer screening - The challenges of complete pathways of care in low-income countries: Focus on Malawi. Women's Health. 2020;16. https://doi.org/10.1177/1745506520914804 [ Links ]
42.Krings A, Boateng G, Dunyo P, Amuah JE, Adams RA, Adunyame L, et al. Dynamics of genotype-specific HPV clearance and reinfection in rural Ghana may compromise HPV screening approaches. Papillomavirus Res. 2019 Jun 1;7:45-51. [ Links ]
43.Haque A, Kouriba B, Aïssatou N, Pant A. Eliminating cervical cancer in Mali and Senegal, two sub-Saharan countries: Insights and optimizing solutions. Vaccines. 2020;8(2):1-11. https://doi.org/10.3390/vaccines8020181 [ Links ]
44.Karanja-Chege CM. HPV vaccination in Kenya: The challenges faced and strategies to increase uptake. Front Public Health. 2022;10:802947. https://doi.org/10.3389/fpubh.2022.802947 [ Links ]
45.Friedman AL, Oruko KO, Habel MA, et al. Preparing for human papillomavirus vaccine introduction in Kenya: Implications from focus-group and interview discussions with caregivers and opinion leaders in Western Kenya. BMC Public Health. 2014;14:1-10. https://doi.org/10.1186/1471-2458-14-855 [ Links ]
46.Barnabas R V., Brown ER, Onono M, et al. Single-dose HPV vaccination efficacy among adolescent girls and young women in Kenya (the KEN SHE Study): Study protocol for a randomized controlled trial. Trials. 2021;22(1):1-19. https://doi.org/10.1186/s13063-021-05608-8 [ Links ]
47.Vermandere H. Introduction of HPV vaccination in Kenya. Afrika Focus. 2016;29(2):117-121. https://doi.org/10.1163/2031356X-02902010 [ Links ]
48.Memiah P, Mbuthia W, Kiiru G, et al. Prevalence and risk factors associated with precancerous cervical cancer lesions among HIV-infected women in resource-limited settings. AIDS Res Treat. 2012;2012:953743. https://doi.org/10.1155/2012/953743 [ Links ]
49.Organization WH. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. Behav Inform Technol [serial online]. 2017 [cited 2022 Feb 14];2:127-161. Available from: http://apps.who.int/bookorders [ Links ]
50.Bratcher LF, Sahasrabuddhe VV. The impact of antiretroviral therapy on HPV and cervical intraepithelial neoplasia: Current evidence and directions for future research. Infect Agent Cancer. 2010;5(1):1-13. https://doi.org/10.1186/1750-9378-5-8 [ Links ]
51.Brown DR, Weaver B. Human papillomavirus in older women: new infection or reactivation? J Infect Dis. 2013 Jan 15;207(2):211-2. https://doi.org/10.1093/infdis/jis662 [ Links ]
52.Okunade KS, Nwogu CM, Oluwole AA, Anorlu RI. Prevalence and risk factors for genital high-risk human papillomavirus infection among women attending the outpatient clinics of a university teaching hospital in Lagos, Nigeria. Pan Afr Med J. 2017;28:1-7. [ Links ]
53.Wencel-Wawrzeńczyk A, Lewitowicz P, Lewandowska A, Saługa A. Sexual behavior and the awareness level of common risk factors for the development of cervical, anogenital and oropharyngeal cancer among women subjected to HR HPV DNA-testing. Int J Environ Res Public Health [Internet]. 2022 Aug 1 [cited 2022 Nov 13];19(15):9580. Available from: /pmc/articles/PMC9367930/ [ Links ]
54.Soh J, Rositch AF, Koutsky L, Guthrie BL, Choi RY, Bosire RK, et al. Individual and partner risk factors associated with abnormal cervical cytology among women in HIV-discordant relationships. Int J STD AIDS. 2014;25(5):315-24. [ Links ]
55.Skinner SR, Wheeler CM, Romanowski B, et al. Progression of HPV infection to detectable cervical lesions or clearance in adult women: Analysis of the control arm of the VIVIANE study. 2016;2438:2428-38. https://doi.org/10.1002/ijc.29971 [ Links ]
56.Hecht SS, Chen C, Cook LS, et al. Correspondence re: C. Chen et al., CYP2D6 genotype and the incidence of anal and vulvar cancer. Cancer Epidemiol Biomark Prev 8: 317-321, 1999. Cancer Epidemiol Biomark Prev [serial online]. 1999 [cited 2022 Nov 21];8(9):839-840. Available from: https://aacrjournals.org/cebp/article/8/9/839/277738/Correspondence-re-C-Chen-et-al-CYP2D6-Genotype-and [ Links ]
57.Kjellberg L, Hallmans G, Åhren AM, et al. Smoking, diet, pregnancy and oral contraceptive use as risk factors for cervical intra-epithelial neoplasia in relation to human papillomavirus infection. Br J Cancer. 2000;82(7):1332-1338. https://doi.org/10.1054/bjoc.1999.1100 [ Links ]
58.Huang J, Deng Y, Boakye D, et al. Global distribution, risk factors, and recent trends for cervical cancer: A worldwide country-level analysis. Gynecol Oncol. 2022;164(1):85-92. https://doi.org/10.1016/j.ygyno.2021.11.005 [ Links ]
59.Oh HY, Kim MK, Seo S, et al. Alcohol consumption and persistent infection of high-risk human papillomavirus. Epidemiol Infect. 2015;143(7):1442-1450. https://doi.org/10.1017/S0950268814002258 [ Links ]
60.Weiderpass E, Ye W, Tamimi R, et al. Alcoholism and risk for cancer of the cervix uteri, vagina, and vulva. Cancer Epidemiol Biomark Prev [serial online]. 2001 [cited 2022 Nov 21];10(8):899-901. Available from: http://aacrjournals.org/cebp/article-pdf/10/8/899/1938579/ce0801000899.pdf [ Links ]
 Correspondence:
Correspondence:
James Kangethe
james.mburu@uonbi.ac.ke
Received: 27 May 2023
Accepted: 05 July 2023
Published: 27 Oct. 2023
What this study adds: These results add to the growing evidence that more efforts are needed to improve routine screening for high-risk human papillomavirus (HR-HPV) infections and cervical cancer among WLHIV as well as optimised HPV vaccination among eligible girls.


{kind=link}
{kind=link}
{kind=link}