










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of HIV Medicine
On-line version ISSN 2078-6751
Print version ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.23 n.1 Johannesburg 2022
http://dx.doi.org/10.4102/sajhivmed.v23i1.1377
ORIGINAL RESEARCH
The sexual and reproductive health needs of young people living with HIV in Gauteng, South Africa
Bandile E. Ndlazi; Thembekile Masango
Department of Health Studies, Faculty of Human Sciences, University of South Africa, Pretoria, South Africa
ABSTRACT
BACKGROUND: HIV has been the focus of health systems strengthening in South Africa for the past two decades. Despite progress, sexual and reproductive health (SRH) challenges such as contraception, condom usage and HIV disclosure of young people living with HIV (YPLHIV) remain inadequately addressed. Therefore, the purpose of the study was to describe the SRH needs of YPLHIV and make recommendations to address identified gaps
OBJECTIVES: To explore and describe the SRH needs and potential systemic gaps of YPLHIV with an aim to make recommendations for improvement and contribute to the development of an integrated approach to SRH care in HIV programming
METHOD: A quantitative cross-sectional research design with purposive sampling was utilised. YPLHIV were recruited from five healthcare facilities in Gauteng, South Africa, for face-to-face interviews
RESULTS: One hundred and six YPLHIV with a median age of 18 years were enrolled. A large proportion (57/106; 53.8%) of respondents reported being either single or double orphaned. Sex-related discussions with parents were reported by only 36/106 (34.0%). History of teenage pregnancy was reported in 39/70 (56.0%) of female respondents. A high prevalence of multiple sexual partnerships 41/97 (42.2%) was noted. Consensual partner HIV disclosure was low at 47/97 (48.4%) and the male gender was associated with low 10/35 (28.6%) disclosure of serostatus to sexual partners
CONCLUSION: Multiple SRH needs were identified. Interventions are needed to improve parental guidance on SRH issues, increase contraception knowledge and access, and provide better male-centred care
Keywords: sexual and reproductive health; HIV; young people; contraception; HIV disclosure.
Introduction
In 2021 it was estimated South Africa had 8.2 million people living with HIV.1,2 The HIV programme has made significant progress in South Africa, providing strong support for prevention, treatment, and care of those affected and infected. Almost 5.2 million people have been enrolled in the antiretroviral therapy (ART) programme and were receiving treatment in 2019.3 Availability of paediatric and adult ART has enabled the reduction of vertical transmission to less than 1% and the survival into adolescence and adulthood of many. A mathematical model study suggests approximately 400 000 children and adolescents are living with HIV in South Africa; this is attributed to high maternal HIV prevalence, but attenuated by the impact of ART through the prevention of mother-to-child HIV transmission programmes.4 The growth in numbers of children and adolescents living with HIV continues to create a gap in the parental understanding of their sexual and reproductive health (SRH) dynamics, which eventually has a negative effect on health-seeking behaviour and accessing of health services. As most young people living with HIV (YPLHIV) enter childbearing age, a clear understanding of their SRH needs, including dating, sex, contraception, condom usage, consensual partner serostatus disclosure and sexual practices is required, as is further exploration to devise effective interventions and develop focused guidelines.5
Social barriers, such as the perception and assumption that YPLHIV do not engage in sexual relationships due to their HIV status, serve to exacerbate limited access to relevant SRH information as it limits opportunities for sexual education and open discussions on sexual issues.6 YPLHIV desire to be accepted and live as their HIV negative peers, which may include engaging in risky sexual behaviours.6 Limited early access to sexual information and treatment further exposes YPLHIV to additional risks of HIV re-infection, opportunistic infections, and sexually transmitted infections (STIs).7 Deepened understanding of the SRH needs of YPLHIV will further inform the design of country-specific, culturally sensitive and multisectoral policies and programmes.7 Growing awareness of these challenges is gradually building more demand for healthcare services, especially those focusing on reproductive healthcare services for young people.8,9 As part of a holistic HIV treatment and care package, YPLHIV should receive culturally sensitive, accurate, and language- and age-appropriate health information on HIV management, STIs, contraception and safe sex. However, this seldom happens.10,11,12 Structural and social barriers are also still noted for adolescents to access SRH information, contraception, and other related services at an early age. Structural barriers refer to various cultural-driven norms that promote dominance of the older generation in making decisions directly affecting adolescents and young people, which further reduces young people's opportunities for access to SRH services and related decisions.13
Our study aimed to describe the SRH needs of YPLHIV in order to contribute to the development of an integrated approach to this group's SRH care in HIV programmes and guidelines.
Research method and design
Study design
A quantitative cross-sectional research design with the application of non-probability purposive sampling was utilised to study YPLHIV from five healthcare facilities in Gauteng, South Africa. Face-to-face interviews were conducted with respondents at the treating facility. The study applied a non-experimental design to explore questions pertaining to the SRH needs of YPLHIV and describe relationships among variables, rather than supporting inferences of causality.
Setting
The study was conducted in three metropolitan districts in Gauteng, namely City of Ekurhuleni, City of Johannesburg, and City of Tswane. Non-probability convenience sampling was applied when selecting five healthcare facilities for the study. The selection was made conveniently with the direction of the district programme managers with the consideration of facility size, number of clients and the number of other studies in the facility, avoiding overburdening. The selected healthcare facilities were a mix of two community health centres and three primary health care facilities; all providing general preventative and curative services of minor ailments and chronic diseases including HIV prevention, treatment, care, and support. All professional nurses providing services to YPLHIV were trained on nurse initiated and management of antiretroviral treatment (NIMART) and, when required, patients are referred to doctors for further diagnosis and management.
Study population and sampling strategy
Inclusion criteria were prospective respondents living with either vertically- or horizontally-acquired HIV and receiving HIV treatment, care and support from participating clinics, aged 18-24 years old, and willing to participate. Respondents' HIV treatment adherence was not a prerequisite for this study. Mode of HIV acquisition was not used to determine eligibility. The Tier.Net electronic record system was used to determine the sampling frame from which the sample was drawn - no clinical data were extracted.
The sampling procedure was conducted to limit error and determine the sample size to assure reliable results. A sample size was computed from the total population of 374 young people aged 18-24 years receiving HIV treatment and care services in the five facilities drawn from Tier.Net. A representative sample size of 106 with a 5% margin of acceptance error was concluded for this study.
Data collection
Data were collected between June 2018 and February 2019. The interviews were conducted by two trained research assistants using a standardised questionnaire adapted from John Cleland's Illustrative Questionnaire for Interview-Surveys with Young People (see Appendix 2) to capture respondents' responses to the assisted questionnaire with a maximum duration of 30 min. The list of prospective respondents drawn from Tier.Net was used to pull out the patients' records to obtain their contact details. The research assistants approached those who were scheduled for their appointments and telephonically contacted those who were not scheduled for appointments. All respondents were asked to sign written informed consent. For standardisation, questionnaires were not distributed to respondents. The research assistants asked the questions and completed the questionnaires. Questions were translated into the respondent's preferred language during the sessions. As respondents had already reached age 18, SRH historic questions were asked based on recall. All completed questionnaires were numbered according to the code assigned for the participating facility, with each respondent allocated an enrolment number for easy tracking of data errors and management of queries arising during data analysis. To maintain anonymity and confidentiality, only respondents' codes (for identification by the researcher) and demographics were captured on the consent forms. Respondents with signs of distress and history of abuse were reported to facility managers for appropriate referrals.
Data analysis
Raw data from completed questionnaires were coded, captured into an Excel© data sheet, and crosschecked for accuracy and missing values. Data were then transferred to statistical software (Statistical Package for Social Sciences [SPSS]© version 24) with the threshold for statistical significance set at P < 0.05 for all statistical analyses. Chi-square test was used to compare proportions. The statistical analysis plan included the generation of frequency distribution tables for all variables to enable exploration of data quality. Cross-tabulation was done to determine the relationship between the predictor variables and responses. Continuous variables were summarised using means with standard deviations or medians with interquartile ranges (IQR) as appropriate. Categorical variables were described as the total number and relative percentage of respondents per response category.
Participation was voluntary and open to all eligible prospective respondents without discrimination or coercion. The study objectives were the determining factor for inclusion and exclusion. Adolescents younger than 18 years were not included as the study was aimed at gathering data based on historical experiences. Prospective respondents' culture, race and gender were not used to limit participation eligibility. The researcher treated the collected data and respondents' personal information with strict confidentiality.
Ethical considerations
The researcher obtained ethical clearance and permission to conduct the study from a Northern Gauteng university ethical review board (reference number HSHDC/630/2017). On receipt of the research proposal approval, approval was obtained from National Health Research Database (NHRD; reference number GP_2017 RP12_180). Application was submitted to the districts' research committees for review and permission to access healthcare facilities, and approvals to proceed were granted on 15 February 2017.
Results
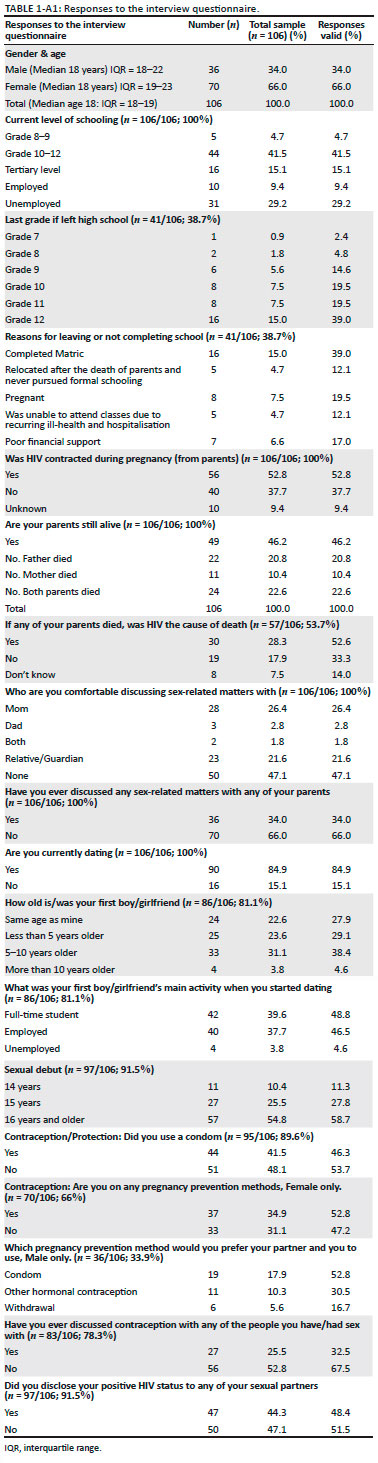
A total of 106 respondents were interviewed in this study. The sample was predominantly female, 70 (66%). Respondents' median age was 18 years (IQR: 17-19). All interviewed respondents were on ART - no information was collected on adherence and virologic outcomes. Detailed responses to the interview questionnaire are given in Appendix 1.
Data on HIV mode of transmission was self-reported. HIV acquisition was horizontal in 40 (37.7%), vertical in 56 (52.8%) and unknown in 10 (9.4%). Twenty-seven of the 56 respondents (48.2%) with vertically acquired HIV were informed of their positive HIV status when they were younger than 14 years. Education status was 44 (41.5%) respondents in Grade 10-12, 16 (15.1%) at tertiary level, and five (4.7%) in lower grades. Most of the study respondents self-reported being sexually active. Twenty-five (23.5%) respondents had left school before completing matric, eight due to pregnancy. Thirty-nine (55.7%) of the female respondents had a history of teenage pregnancy with eight reporting a miscarriage or stillbirth.
General sex discussion at home
Fifty-seven (53.8%) respondents reported either both (n = 24/106 [22.6%]) or one (n = 33 [31.2%]) of their parents were deceased. Thirty of these 57 (52.6%) had been informed their parents' cause of death was HIV. Sex-related discussions with parents were reported by only 36/106 (34%). Fifty-seven (53.8%) respondents had someone other than their parents with whom to discuss sex-related issues. Gender was associated with discussing sex-related matters with household members: more male respondents 30/36 (83.3%) reported having never discussed sex-related matters with others at home, compared to 40/70 (57.1%) of female respondents (P < 0.01).
First consensual relationship partner's profile and HIV disclosure to sexual partner
The first consensual relationship partner profile in the 86 respondents who reported these relationships was with someone 5-10 years older in 33 (38.4%) and was with someone more than 10 years older in four (4.6%). Five respondents (5.8%) knowingly had a relationship with a married person. The first consensual partners' occupational status was 42 (48.8%) employed, 40 (46.5%) full-time students, and four (4.6%) unemployed.
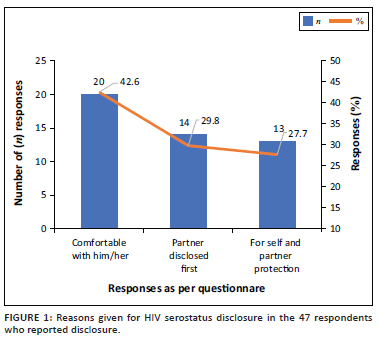
Slightly above half, 50/97 (51.5%), had not disclosed their HIV-positive status to their sexual partners. Gender was associated with HIV status disclosure to sexual partners: 22/32 (68.7%) of the male respondents had never disclosed their HIV status to any of their sexual partners compared to 28/65 (46.1%) of the female respondents (P < 0.01). Reasons for HIV status disclosure are shown in Figure 1. Respondents who reported non-disclosure cited fear of rejection by their partners as the main reason.
Sexual practices
Sexual debut was reported by 97 respondents: 11 (11.3%) at 14 years of age, 27 (27.8%) at 15 years of age, and 57 at 16 years of age or older. The median age of sexual debut was 18 years (IQR: 16-19). Nine respondents (8.4%) reported to have never had sex. The first sexual encounter was consensual in 84/97 (86.5%), and non-consensual in 10/97 (10.3%). There was a high prevalence, 41/103 (41.8%), of multiple concurrent sexual partnerships while in a stable relationship.
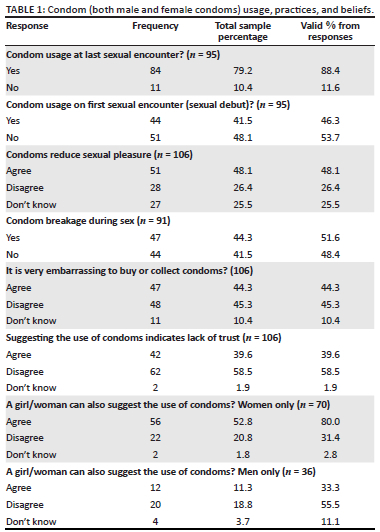
Thirty-seven of 70 (52.8%) female respondents reported using pregnancy prevention methods. Nineteen of the 36 (52.8%) male respondents reported condoms as their contraceptive method of choice and six (16.7%) used withdrawal as a means of pregnancy prevention. Condom usage, practices, and beliefs are shown in Table 1. Self-reported condom usage at last sexual encounter was 84/95 (88.4%) while only 44/95 (46.3%) reported condom usage on sexual debut. Despite the high rate of condom usage among study respondents, findings revealed negative attitudes towards condom usage as 51/106 (48.1%) of respondents believed that condoms reduce sexual pleasure and 47/106 (44.3%) felt it was embarrassing for them to buy or collect condoms. Most female respondents 56/70 (80.0%) agreed women could proactively suggest the use of condoms, while more than half 20/36 (55.5%) of male respondents disagreed.
Past STIs were reported by 44/106 (41.5%) with some admitting having had more than one recurrence. Most (42/44; 97.7%) respondents who reported STI incidence had sought medical attention, however only 23/44 (52.2%) notified their consensual partners.
Healthcare-seeking behaviour and communication with healthcare workers
Sixty-four of 106 (60.4%) respondents indicated they were comfortable with asking clinic staff sex-related questions. Fifty-one of 64 (80.0%) respondents indicated they used HIV treatment follow-up consultation sessions as an opportunity to raise SRH-related questions, 53 of whom (82.8%) felt that their engagement with healthcare workers was fruitful as questions were responded to satisfactorily and without judgement. Gender was associated with whether the respondents felt comfortable with asking clinic staff questions: more male respondents (21/35; 60.0%) were not comfortable with asking clinic staff questions than female respondents (20/70; 28.6%) (P < 0.01).
Discussion
The current study explored the SRH needs of YPLHIV. The study sample was predominantly female (66%) and included young people who have both vertically and horizontally acquired HIV infection. Teenage pregnancy was a common reason for females to drop out of school. These findings concur with Chakalisa et al., where 44% of female adolescents reported to have fallen pregnant during their adolescent years.14 High proportions of our respondents were single or double orphaned, which is important as orphaned children, more especially those growing up with vertically acquired HIV, become increasingly susceptible to a variety of hardships negatively impacting their quality of life.15 Integration of family planning and mental healthcare within HIV care could reduce unplanned pregnancies and other associated stressors among YPLIHV.16
The death of parents disrupts adolescents' and young peoples' quality of life and creates lifelong instabilities resulting in mental and behavioural challenges.10 Our findings that YPLHIV were more likely to have experienced the death of one or both parents is similar to those in a study from Cambodia where more than 50% of respondents reported at least one deceased parent.9 Ntuli et al. cited long-term effects of orphanhood, especially maternal death beyond age 18 years as these children suffer emotional distress from prolonged bereavement, which affects their ability to develop positive coping strategies.17 Their common coping strategy becomes silence and withdrawal which then further exacerbates their emotional distress.17
Absence of communication by parents and caregivers on sexual topics was found to be common in our respondents. Other studies have shown that parent-child sexuality discussions were described as selective, harsh and parent driven while children were just passive information receivers, and parents used threats to promote abstinence.18,19 Limited SRH support and guidance in the home has been linked to the perception and expectation that YPLHIV should not engage in sexual relationships.6 An Ethiopian study found only small proportions of young people reporting open communication with parents on topics pertaining to sex - only 28.0% were able to have related discussions with their mothers, and fewer, 18.5%, with their fathers.20
Sexual debut findings from the current study align with those of studies in Botswana and Zambia, where sexual debut was reported at 15 years of age.14 Generally, YPLHIV delay sexual debut due to their HIV status compared to the general population.21
The current study reported high condom usage at last sexual encounter, but very low condom usage at sexual debut. Contrary to these findings, low (38.0%) condom usage among sexually active YPLHIV was reported in a Ugandan study while 57.9% condom use at last sexual encounter was found in a study conducted among heterosexual sexually active young women in South Africa.22,23 The current study found inconsistent condom usage in most relationships, while convenience appeared to play an important role in condom usage with a relatively high proportion finding the purchase or collection of condoms embarrassing. Contrary to this finding, Wondemagegn et al. reported that only 5.0% referred to condom unavailability as a cause of inconsistent use.24 The current study's findings, depicted high female autonomy with regard to condom suggestion and negotiation. The finding might not be a true reflection of the real practice: Ntshiqa et al. noted that young women reported low (47.0%) condom use with high risky sexual behaviour.23 In the current study, male respondents were more likely to engage in multiple sexual partners, aligning with those of other studies.14,25
Young men in the current study displayed reluctance regarding communication with healthcare workers regarding their SRH challenges; this was also noted in a study assessing the SRH service utilisation by male adolescents in a Gauteng district, where healthcare workers were perceived as judgemental.26 These findings indicate the need for male-focused SRH interventions.
Reported contraception use in this study was slightly lower than the national contraceptive use of 60.0% among sexually active women.27 A study conducted among women living with HIV in Soweto, South Africa, in 2010 found 84.0% were on contraception which is in contrast to our study; however, a study in Lao People's Democratic Republic found only 34.0%.28,29 Different settings where data were collected could be the cause of data variations depending on other barriers. Withdrawal as a method to prevent pregnancy was reported by 16.7% of our male respondents which is twice as high as that reported by a study conducted in Lao People's Democratic Republic.29
The current study found low consensual partner serostatus disclosure among YPLHIV. Our findings are similar to those of other studies.21,22 Male gender was associated with low serostatus disclosure to sexual partners compared to female in our study, which is consistent with other studies.30,31 These findings highlight the need for promotion of consensual partner disclosure of HIV and finding new approaches for partner notification, HIV index testing, and linkage to care and treatment. Early disclosure improves both the SRH and HIV treatment adherence and viral load suppression of YPLHIV.32
Limitations of the study
Our study may be limited in generalisability to other districts and provinces because the sample was exclusively drawn from three metro districts, and because we only studied young people aged 18-24 years. We adopted a cross-sectional design and non-random sampling technique, which might pose a risk of bias. The mode of HIV acquisition relied on self-report.
Conclusion
Our findings indicate multiple missed SRH needs of YPLHIV. Interventions are needed to improve parental guidance on SRH issues, contraception knowledge and access, especially directed at teenage pregnancies, reduction of HIV-related stigma, and provision of better male-centred care. A high proportion of YPLHIV are orphaned, which has profound impacts on health.
Acknowledgements
The authors would like to express their sincere appreciation to the respondents, who took their time to make this study a success, and to the Tshwane, eKurhuleni and Johannesburg Metro Research Health Committees, for granting access and seeing value of the study of this nature.
Competing interests
The authors declare that there are no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
B.E.N. and T.M. conceived of the presented idea. T.M. supported B.E.N. in the investigation of the sexual and reproductive health dynamics of young people living with HIV and supervised the study processes and conclusion of this work. All authors discussed the results and contributed to the final manuscript.
Funding information
The authors disclosed receipt of the following financial support for the research, authorship, or publication of this article: This work was supported by the University of South Africa's M & D bursaries. SEAD Consulting provided support for data analysis.
Data availability
The data that support the findings of this study are openly available on request from the corresponding author, B.E.N.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1. Joint United Nations Programme on HIV/AIDS (UNAIDS). Global update AIDS update 2021. Seizing the moments: Confronting inequalities, lessons for pandemic response from 40 years of AIDS [homepage on the Internet]. 2021 [cited 2021 Sept 15]. Available from: https://www.unaids.org>20210714_global-aids-update [ Links ]
2. World Health Organization (WHO). Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Accountability for the global health sector strategies 2016-2021: Actions for impact [homepage on the Internet]. Geneva: World Health Organization; 2021 [cited 2021 Sept 15] Available from: http://www.who.int/publications/i/item/9789240027077 [ Links ]
3. Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS data 2020 [homepage on the Internet]. 2020 [cited 2021 Sept 29]. Available from: https://www.unaids.org/en/resources/documents/2020/unaids-data [ Links ]
4. Johnson LF, May MT, Dorrington RE, et al. Estimating the impact of antiretroviral treatment on adult mortality trends in South Africa: A mathematical modelling study. PLoS Med. 2017;14(12):e1002468. https://doi.org/10.1371/journal.pmed.1002468 [ Links ]
5. Okawa S, Mwanza-Kabaghe S, Mwiya M, et al. Sexual and reproductive health behaviour and unmet needs among a sample of adolescents living in Zambia: A cross-sectional study. Reprod Health. 2018;15:55. https://doi.org/10.1186/s12978-018-0493-8 [ Links ]
6. Shapiro K, Ray S. Sexual health for people living with HIV. Reprod Health Matters. 2007;15(29):67-92. https://doi.org/10.1016/S0968-8080(07)29034-2 [ Links ]
7. Melesse D, Mutua MK, Choudhury A, et al. 2020. Adolescent and sexual and reproductive health in sub-Saharan Africa: Who is left behind? Biomed J Glob Health. 2020;5(1):e002231. https://doi.org/10.1136/bmjgh-2019-002231 [ Links ]
8. Pretorius L, Gibbs A, Crankshaw T, Willan S. Interventions targeting sexual and reproductive health and rights outcomes of young people living with HIV: Comprehensive review of current interventions from sub-Saharan Africa. Glob Health Action. 2015;8(1):8-11. https://doi.org/10.3402/gha.v8.28454 [ Links ]
9. Toth G, Mburu G, Tout S, et al. Social support needs among adolescents living with HIV in transition from pediatric to adult care in Cambodia: Findings from a cross-sectional study. AIDS Res Ther. 2018;15:8. https://doi.org/10.1186/s12981-018-0195-x [ Links ]
10. Kaunda-Khangamwa BN, Kapwata P, Malisita K, et al. Adolescents living with HIV, complex needs and resilience in Blantyre, Malawi. AIDS Res Ther. 2020;17:35. https://doi.org/10.1186/s12981-020-00292-1 [ Links ]
11. Roxo U, Mobula LM, Walker D, Ficht A, Yeiser S. Prioritizing the sexual and reproductive health and rights of adolescent girls and young women within HIV treatment and care services in emergency settings: A girl centred agenda. BioMed Cent. 2019;16(1):57. https://doi.org/10.1186/s12978-019-0710-0 [ Links ]
12. Smith P, Marcus R, Bennie T, et al. What do South African adolescent want in sexual health services? Evidence from the South African studies on HIV in adolescents (SASHA) project. S Afr Med J. 2018;108(8):677-681. https://doi.org/10.7196/SAMJ.2018.v108i8.13013 [ Links ]
13. Wigle J, Paul S, Birn A, Gladstone B, Braitstein P. Youth participation in sexual and reproductive health: Policy, practice, and progress and Malawi. Inter J Pub Health 2020;65:379-389. https://doi.org/10.1007/s00038-020-01357-8 [ Links ]
14. Chakalisa U, Wirth K, Bennet K, et al. Self-reported risky sexual practices among adolescents and young adults in Botswana. S Afr J HIV Med. 2018;20(1):899. https://doi.org/10.4102/sajhivmed.v20i1.899 [ Links ]
15. Burkholder M. The impact of HIV/AIDS on orphans in a South African context [homepage on the Internet]. Taylor University; 2019. [cited 22 Feb 20]. Available from: https://core.ac.uk/download/pdf/229387449.pdf [ Links ]
16. Adeniyi VO, Ajayi AI, Moyaki MG, Goon DT, Avramovic G, Lambert J. High rate of unplanned pregnancy in the context of integrated family planning and HIV care services in South Africa. BMC Health Serv Res. 2018;18:140. https://doi.org/10/1186/s12913-018-2942-z [ Links ]
17. Ntuli B, Mokgatle M, Madiba S. The psychosocial wellbeing of orphans: The case of early school leavers in socially depressed environment in Mpumalanga Province, South Africa. PLoS One. 2020;15(2):e0229487. https://doi.org/10.1371/journal.pone.0229487 [ Links ]
18. Mabunda A, Madiba S. The context of parent-child communication about sexuality and HIV prevention: The perspective of high school learners in Gauteng province, South Africa. Pula: Botswana J Afr Stud [serial online]. 2017;31(1). Available from https://www.researchgate.net/publication/322402877 [ Links ]
19. Vilanculos E, Nduna M. 'The child remember your voice': Parent-child communication about sexuality in the South African context. Afr J AIDS Res. 2017;16(1):81-89. https://doi.org/10.2989/16085906.2017.1302486 [ Links ]
20. Alamrew Z, Bedimo M, Azage M. Risky sexual practices and associated factors for HIV/AIDS infection among private college students in Bahir Dar City, Northwest Ethiopia. International Scholarly Research Notices. Public Health. 2013;2013:763051. https://doi.org/10.1155/2013/763051 [ Links ]
21. Ndongmo TN, Ndongmo CB, Michelo C. Sexual and reproductive health knowledge and behaviour among adolescents living with HIV in Zambia: A case study. Pan Afr Med J. 2017;26:71. https://doi.org/10.11604/pamj.2017.26.71.11312 [ Links ]
22. Ankunda R, Atuyambe LM, Kiwanuka N. Sexual risk related behaviour among youth living with HIV in central Uganda: Implications for HIV prevention. Pan Afr Med J. 2016;24-49. https://doi.org/10.11604/pamj.2016.24.49.6633 [ Links ]
23. Ntshiqa T, Musekwa A, Mlotshwa M, et al. Predictors of male condom use among sexually active heterosexually active heterosexual young women in South Africa, 2012. BMC Public Health. 2018;18:1137. https://doi.org/10.1186/s12889-018-6039-8 [ Links ]
24. Wondemagegn F, Berkessa T. High level risky sexual behaviour among persons living with HIV in the urban setting of the highest HIV prevalent areas in Ethiopia: Implications for interventions. PLoS One. 2020;15(11):e0242701. https://doi.org/10.1371/journal.pone.0242701 [ Links ]
25. Poudel KC, Poudel-Tanduka K, Palmer PH, et al. Coinfection of sexually transmitted infections among HIV-positive individuals: Cross-sectional results of a community-based positive living with HIV (POLH) study in Nepal. J Inter Assoc Providers Health Care. 2017;16(4):338-346. https://doi.org/10.1177/2325957415614644 [ Links ]
26. Cooper V, Clatworthy Youssef E, et al. Which aspects of health care are most valued by people living with HIV in high-income countries? A systematic review. BioMed Cent Health Services Res. 2016;16:677. https://doi.org/10.1186/s12913-016-1914-4 [ Links ]
27. National Department of Health (NDoH), Statistics South Africa (Stats SA), South African Medical Research Council (SAMRC) & ICF. South Africa Demographic and Health Survey 2016 [homepage on the internet]. 2019. [cited 2022 Feb 28]. Available from: https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf [ Links ]
28. Kaida A, Laher F, Strathdee SA, et al. Contraceptive use and method preference among women in Soweto South Africa: The influence of expanding access to HIV care and treatment services. PLoS One. 2010;5(11):e13868. https://doi.org/10.1371/journal.pone.0013868 [ Links ]
29. Phongluxa K, Langeslag G, Jat TR, Kounnavong S, Khan MA, Essink DR. Factors influencing sexual and reproductive health among adolescents in Lao PDR. Global Health Action. 2020;13(2):1791426. https://doi.org/10.1080/16549716.2020.1791426 [ Links ]
30. Francis SC, Mthiyane NT, Baisley K, et al. Prevalence of sexually transmitted infections among young people in South Africa: A nested survey in a health and demographic surveillance site. PLoS Med. 2018;15(2):e1002512. https://doi.org/10.1371/journal.pmed.1002512 [ Links ]
31. Vranda MN, Subbakrishna DK, Ramakrishna J, Veena HG. Sexual and reproductive health concerns of adolescents living with perinatally infected HIV in India. Ind J Comm Med [serial online]. 2018;43(3):329-342. [2021 Sept 10]. Available from: https://www.ncbi.nlm.nih.gov/pmc.articles/PMC6166509 [ Links ]
32. Montalto JG, Sawe FK, Miruka A, et al. 2017. Diagnosis disclosure to adolescents living with HIV in rural Kenya improves antiretroviral therapy adherence and immunologic outcomes: a retrospective cohort study. PLoS One 12(10):e0183180. [cited 2022 Oct 20]. Available from https://doi.org/10.1371/journal.pone.0183180 [ Links ]
 Correspondence:
Correspondence:
Bandile Ndlazi
bandile.ndlazi@yahoo.com
Received: 04 Feb. 2022
Accepted: 29 Apr. 2022
Published: 06 Sept. 2022
Appendix 1
Appendix 2


