










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of HIV Medicine
On-line version ISSN 2078-6751
Print version ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.23 n.1 Johannesburg 2022
http://dx.doi.org/10.4102/sajhivmed.v23i1.1369
CASE REPORT
Alere Determine-tuberculosis lipoarabinomannan positivity in disseminated non-tuberculous mycobacteria: An illustrative case series
Riana GreylingI; Graeme MeintjesII, III; Bianca SossenII
IMatthew Goniwe Clinic, Cape Town City Health Department, Cape Town, South Africa
IIDepartment of Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
IIIWellcome Center for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa
ABSTRACT
INTRODUCTION: In outpatients, the World Health Organization recommends that the urine Alere Determine-tuberculosis lipoarabinomannan (AlereLAM) should be used to support the diagnosis of tuberculosis (TB) in people living with HIV (PLHIV) with CD4 counts ≤ 100 cells/µL or with signs of being 'seriously ill'. There is a risk of a false-positive AlereLAM in disseminated non-tuberculous mycobacterial (NTM) infections and it may be difficult to differentiate a single infection (either Mycobacterium tuberculosis or NTM) from dual infection
PATIENT PRESENTATION: We report three patients, enrolled in an operational study assessing AlereLAM use in an outpatient setting, who had advanced HIV (all CD4 < 20 cells/µL) and strongly positive (grade 4+) AlereLAM results in whom Mycobacterium avium or kansasii were later cultured from blood or urine and sputum.
MANAGEMENT AND OUTCOME: Based on positive AlereLAM results, all three were initiated on TB treatment. One died before NTM infection was detected. Two were managed for dual infection (TB and NTM) but died within two years.
CONCLUSION: Tuberculosis remains a leading cause of death and a disproportionate number of these deaths occur in PLHIV. Tuberculous treatment should be initiated based on a positive AlereLAM result, and this should be followed by additional testing to confirm the diagnosis of TB and to obtain drug susceptibility results. In those not responding to TB treatment where the only positive result was an AlereLAM, an alternative or additional diagnosis of NTM infection should be considered, particularly in patients with a very low CD4 count.
Keywords: tuberculosis; Lipoarabinomannan; ambulatory; outpatient; point-of-care; urine; HIV; diagnostic.
Introduction
The World Health Organization (WHO) recommends the use of the Alere Determine-tuberculosis lipoarabinomannan assay, or AlereLAM, in outpatient settings for people living with HIV (PLHIV) with CD4 counts ≤ 100 cells/µL or signs of being 'seriously ill'.1 Evidence in support of this includes improved survival when AlereLAM is implemented in hospitalised, ill PLHIV, alongside its low cost, rapid turnaround time and instrument-free design.1,2,3 The diagnostic sensitivity and specificity of AlereLAM in outpatient settings are estimated at 31% and 95%.4
Lipoarabinomannan is present in the cell wall of all mycobacterium species. Different LAM assays have been designed to detect different LAM domains, some more specific to Mycobacterium tuberculosis (M. tb) than others.5 There is a risk of false-positive AlereLAM results in the setting of disseminated non-tuberculous mycobacterial (NTM) infections and it may be difficult to differentiate a single infection (either M. tb or NTM) from a dual infection.
With the ongoing scale-up of AlereLAM use in the South African public health sector, awareness of the possibility of a false-positive AlereLAM due to NTM infection is important. This is particularly critical as the patient groups affected by disseminated M. tb and NTM infections (i.e. low CD4 counts) overlap.6 To highlight this, we report three patients who were enrolled in a study of AlereLAM utility at outpatient clinics in Khayelitsha, Cape Town.7
Case reports
Patient 1
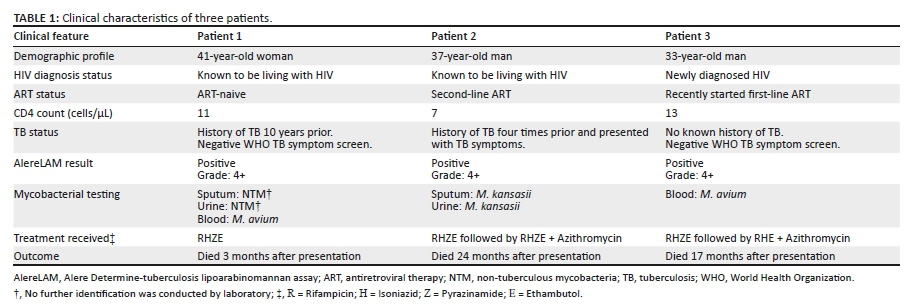
An antiretroviral therapy (ART)-naive woman was asymptomatic for tuberculosis (TB) at presentation and started on first-line ART (see Table 1 for more information). She rapidly deteriorated and presented again after 10 days with night sweats, a cough, and abdominal pain. She met the criteria for AlereLAM testing on this date, which revealed a strongly positive (4+) result. The patient was placed onto TB treatment and sputum was sent for Xpert MTB/RIF Ultra and mycobacterial culture, along with urine for mycobacterial culture.
After one month of TB treatment, the patient's condition worsened. She presented with vomiting and abdominal distension and was referred for inpatient care. By this time the sputum and urine cultures had detected NTM without further identification and a mycobacterial blood culture was then drawn. The patient died during hospital admission. After her death, the laboratory reported that the blood culture identified Mycobacterium avium. No Xpert MTB/RIF or cultures identified M. tb.
Patient 2
A man who was on second-line ART and had a history of TB four times prior presented with weight loss, fatigue and diffuse, hypopigmented skin lesions suggestive of a superficial fungal infection (see Table 1 for more information). The patient was classified as meeting the WHO 'seriously ill' criteria and an AlereLAM revealed a strongly positive (4+) result; he was therefore started on TB treatment. A sputum and urine sample were collected, and both of these later cultured Mycobacterium kansasii. Once the two samples had isolated M. kansasii, a dual infection of M. tb and M. kansasii was diagnosed and azithromycin was added to the patient's regimen. Unfortunately, the patient disengaged from treatment after one year and died as an inpatient two years after initial presentation. Blood culture on that admission was positive for Mycobacterium kansasii. No Xpert MTB/RIF or cultures identified M. tb.
Patient 3
A man with recently diagnosed HIV and cryptococcal meningitis had been started on ART one month prior to this (see Table 1 for more information). He presented with WHO 'seriously ill' criteria and an AlereLAM was performed, revealing a strongly positive (4+) result. He was started on TB treatment on the same day. A month later, he deteriorated clinically and required hospital admission. A blood culture during this admission cultured Mycobacterium avium. With this result, azithromycin was added to his TB treatment and pyrazinamide was stopped. The patient died as an inpatient 17 months after initial presentation. No Xpert MTB/RIF or cultures identified M. tb, although he was diagnosed with TB meningitis based on CT brain features during the protracted illness course.
Discussion
A disproportionate number of tuberculosis deaths occur in PLHIV.8 Tuberculosis treatment should be initiated based on a positive AlereLAM result,1 so that ill patients who are at high risk of dying will benefit from the test and a positive result.
These case reports illustrate that a positive AlereLAM result must be interpreted in the clinical context and further diagnostic testing should be conducted. The objectives of further investigations are mycobacterial species identification and drug susceptibility testing. If a patient with advanced immunosuppression is initiated on TB treatment based on an AlereLAM alone and further sampling is not possible, it is important to monitor the patient's response to tuberculosis treatment closely. In the case of a non-response to treatment or deterioration on treatment, NTM infection or dual infection (with M. tb and NTM) should be considered, particularly in patients with very low CD4 counts, together with other differential diagnoses. Finally, these case reports illustrate that disseminated NTM infections can result in strongly positive AlereLAM results. Whether this finding can be used as an indicator of disseminated NTM infection needs to be assessed further in larger studies.
Acknowledgements
The authors would like to acknowledge and thank all of the patients for taking part in this study, as well as all of the clinical staff at the clinic and hospital involved.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
G.M. conceived of the study. R.G. carried out the study protocol including enrolling the patients into this study, collecting data and performing the point-of-care tests during clinical consultations. R.G. and B.S. wrote the first version of the manuscript with input and review from G.M.
Ethical considerations
These case reports were drawn from a study that was approved by the Faculty of Health Sciences Human Research Ethics Committee of the University of Cape Town (reference 102/2018).
Funding information
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: G.M. was supported by the Wellcome Trust (098316, 214321/Z/18/Z, and 203135/Z/16/Z), and the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation (NRF) of South Africa (Grant No. 64787). The funders had no role in the study design, data collection, data analysis, data interpretation, or writing of this report. The opinions, findings, and conclusions expressed in this manuscript reflect those of the authors alone. This research was funded, in part, by the Wellcome Trust.
Data availability
The data that support the findings of this study are available from the corresponding author, B.S., upon reasonable request.
Disclaimer
The views expressed in the submitted article are our own and not a position of the institutions represented or funders.
References
1.World Health Organization. Lateral flow urine lipoarabinomannan assay (LF-LAM) for the diagnosis of active tuberculosis in people living with HIV: Policy update (2019) [homepage on the Internet]. 2019 [cited 2020 Jul 25]. Available from: https://apps.who.int/iris/bitstream/handle/10665/329479/9789241550604-eng.pdf?sequence=1&isAllowed=y&ua=1 [ Links ]
2.Peter JG, Zijenah LS, Chanda D, et al. Effect on mortality of point-of-care, urine-based lipoarabinomannan testing to guide tuberculosis treatment initiation in HIV-positive hospital inpatients: A pragmatic, parallel-group, multicountry, open-label, randomised controlled trial. Lancet. 2016;387(10024):1187-1197. https://doi.org/10.1016/S0140-6736(15)01092-2 [ Links ]
3.Gupta-Wright A, Corbett EL, Van Oosterhout JJ, et al. Rapid urine-based screening for tuberculosis in HIV-positive patients admitted to hospital in Africa (STAMP): A pragmatic, multicentre, parallel-group, double-blind, randomised controlled trial. Lancet. 2018;392(10144):292-301. https://doi.org/10.1016/S0140-6736(18)31267-4 [ Links ]
4.Bjerrum S, Schiller I, Dendukuri N, et al. Lateral flow urine lipoarabinomannan assay for detecting active tuberculosis in people living with HIV. Cochrane Database Syst Rev. 2019;10(10):CD011420. https://doi.org/10.1002/14651858.CD011420.pub3 [ Links ]
5.Bulterys MA, Wagner B, Redard-Jacot M, et al. Point-of-care urine LAM tests for tuberculosis diagnosis: A status update. J Clin Med. 2019;9(1):111. https://doi.org/10.3390/jcm9010111 [ Links ]
6.Gupta-Wright A, Kerkhoff AD, Meintjes G, Corbett EL. Urinary lipoarabinomannan detection and disseminated nontuberculous mycobacterial disease. Clin Infect Dis. 2018;66(1):158. https://doi.org/10.1093/cid/cix735 [ Links ]
7.Sossen B, Ryan A, Bielawski J, Greyling R, Matthews G, Hurribunce-James S, et al. Urine lipoarabinomannan for rapid tuberculosis diagnosis in HIV-infected adult outpatients in Khayelitsha. South Afr J HIV Med. 2021;22(1). https://doi.org/10.4102/sajhivmed.v22i1.1226 [ Links ]
8.World Health Organization. Global tuberculosis report 2021. Geneva: WHO; 2021. [ Links ]
 Correspondence:
Correspondence:
Bianca Sossen
blsossen@gmail.com
Received: 03 Jan. 2022
Accepted: 03 Feb. 2022
Published: 04 Apr. 2022


{kind=link}