










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouthern African Journal of HIV Medicine
versão On-line ISSN 2078-6751
versão impressa ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.22 no.1 Johannesburg 2021
http://dx.doi.org/10.4102/sajhivmed.v22i1.1222
SCIENTIFIC LETTER
Determination of lopinavir/ritonavir concentrations in four different oral solutions for the application of antiretroviral therapy in very young, HIV-1-infected children
Nils von HentigI; Carlo AngioniII; Christoph KönigsIII
IInternal Medicine II, HIVCENTER, Goethe University Hospital, Frankfurt, Germany
IIInstitute of Clinical Pharmacology, Goethe University Hospital, Frankfurt, Germany
IIIDepartment of Pediatrics and Adolescent Medicine, Goethe University Hospital, Frankfurt, Germany
Infants infected with HIV-1 are generally more affected by disease progression and mortality than older children.
Early initiation of antiretroviral therapy (ART) prevents progression to AIDS and death. However, therapy options for very young children are quite scarce, as many antiretrovirals are not approved for use in children younger than 3 years of age, and experience regarding the dosing, application, side effects and outcome is limited.1,2,3,4,5,6
An antiretroviral regimen containing lopinavir/ritonavir (LPV/r) in addition to two nucleoside reverse transcriptase inhibitors (NRTIs) is the main treatment option for HIV-1-infected infants in most African countries.7,8 The LPV/r combination is available as a meltrex tablet, in a fixed-dose combination added to NRTIs, or as a liquid formulation that is bodyweight-dose adjusted.2,5,6,9,10,11,12,13 The tablet formulation is not applicable for very young children because of their inability to swallow the tablet. Crushing of the LPV/r meltrex formulation is not recommended, and the liquid formulation remains the only alternative for very young patients. However, as the taste of the pure LPV/r liquid formulation is unpalatable, many parents seek alternative ways to give the medicine, including mixing the LPV/r oral solution with formula milk, for example, as part of the child's nutrition. However, flocculation of the oral solution results, and no bioavailability data are available.
Following the report of parents administering the solution in formula milk, which was well tolerated by the child, and having observed a good virological response, lopinavir plasma levels were determined at the University of Frankfurt, following routine monitoring of the child on ART. The parents provided informed consent before the procedure. The standard pharmacokinetic testing protocol for the examination of antiretroviral plasma concentrations in small children allows sampling at the following time points: at 0, 1 and 2 h after the dosing interval. Each sample is < 1 mL whole blood in children < 2 years of age. The sample is then processed and analysed by means of liquid chromatography-tandem mass spectrometry (LC-MS/MS). The child was treated with the licensed dose (230 mg/m2) twice daily and surprisingly reached a cmin of 3330 ng/mL and cmax of 5610 ng/mL.
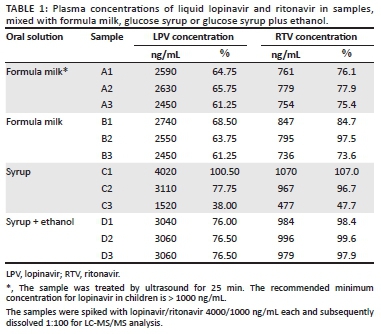
We therefore prepared several oral solutions by mixing the LPV/r liquid formulation together with glucose syrup, glucose syrup and ethanol, or formula milk, with and without ultrasound treatment, and tested these oral solutions for their taste and drug stability. Three samples each of (1) formula milk (10 mL Humana PRE containing 0.32 g fat, 0.76 g carbohydrate and 0.12 g protein), (2) ultrasound-treated formula milk (to improve solubility and inhibit flocculation), (3) glucose syrup, and (4) glucose syrup plus ethanol (chemistry-based decision to improve the solubility) were spiked with the same concentration of liquid LPV/r (4000/1000 ng/mL), and the concentrations of LPV/r were measured by means of validated LC-MS/MS.14 The accuracy of controls was 92% - 105% for lopinavir and 95% - 109% for ritonavir. The linearity of the calibration curve ranged from 100 ng/mL to 60 000 ng/mL.15 Three samples of each formulation were prepared in order to test the possible variability of sampling. The investigators controlled the taste by taking it orally and inhibiting flocculation by visual inspection; tasting was performed independently and then reported to each other.
The three samples of formula milk treated with ultrasound for 25 min and the three samples of untreated formula milk showed lopinavir concentrations ranging from 2450 ng/mL to 2590 ng/mL and from 2450 ng/mL to 2790 ng/mL, respectively. The samples dissolved in ethanol-glucose syrup and glucose syrup alone showed lopinavir concentrations of 3040 ng/mL - 3060 ng/mL and 1520 ng/mL - 4020 ng/mL, respectively (Table 1).
It was found that LPV/r flocculated in formula milk, regardless of whether the formula milk was ultrasound treated, and was intolerably bitter. In contrast, the taste of the LPV/r solution was completely masked when mixed together with glucose syrup. In general, the LPV/r liquid formulation proved to be stable for at least 15 min when dissolved in either formula milk or glucose syrup.
The samples from the LPV/r liquid formulation and glucose syrup mixture showed a marked variation in the lopinavir concentrations, but the variable results were not attributable to any instability of the drug in the resulting solution. This variation can be explained by sampling errors, because it was nearly impossible to accurately pipette small quantities of this highly viscous solution. This problem was confirmed through the addition of 1 mL ethanol to the syrup solution, which resulted in improved solubility as well as the most accurate concentration measurements obtained in this case.
In general, LPV/r can be dissolved in glucose syrup with a moderate loss of stability. The taste of the solution was greatly improved, so this method of application could very well help young children swallow the medication more easily. Dissolving the antiretroviral liquid formulation in formula milk resulted in flocculation of the solution, lower LPV/r concentrations and an incredibly bitter taste.
Because this report is based on a small sample size, a more comprehensive study should be carried out in order to confirm these findings and assist children living with HIV and their parents with the administration of the liquid LPV/r formulation.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this letter.
Authors' contributions
C.A. performed the lab analyses and the previous validation of lab methods regarding liquid chromatography-tandem mass spectrometry. C.K. conceptualised the study, supervised the evaluation and reviewed the publication. N.V.H. conceptualised the study, supervised the evaluation and performed the statistical analysis; he is the corresponding author of this letter.
Ethical considerations
As this study was conducted on material obtained from routine clinical blood assessments being analysed regularly in children with HIV according to treatment guidelines in Germany that were then processed ex vivo and in vitro, no ethical clearance was necessary according to the German medical laws, and no informed consent was applicable.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
Data are available from the corresponding author, N.V.H., upon reasonable request.
Disclaimer
The views and opinions expressed in this letter are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1. Siberry GK, Abzug MJ, Nachman S, et al. Guidelines for the prevention and treatment of opportunistic infections in HIV-exposed and HIV-infected children: Recommendations from the National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. Pediatr Infect Dis J 2013;32(Suppl 2):i-KK4. https://doi.org/10.1097/01.inf.0000437856.09540.11 [ Links ]
2. Amani-Bosse C, Dahourou DL, Malateste K, et al. Virological response and resistances over 12 months among HIV-infected children less than two years receiving first-line lopinavir/ritonavir-based antiretroviral therapy in Cote d'Ivoire and Burkina Faso: The MONOD ANRS 12206 cohort. J Int AIDS Soc 2017;20(1): 21362. https://doi.org/10.7448/IAS.20.01.21362 [ Links ]
3. Bastiaans DE, Forcat S, Lyall H, et al. Pharmacokinetics of pediatric lopinavir/ritonavir tablets in children when administered twice daily according to FDA weight bands. Pediatr Infect Dis J 2014;33(3):301-305. https://doi.org/10.1097/INF.0000000000000014 [ Links ]
4. Bouazza N, Foissac F, Fauchet F, et al. Lopinavir/ritonavir plus lamivudine and abacavir or zidovudine dose ratios for paediatric fixed-dose combinations. Antivir Ther 2015;20(2):225-233. https://doi.org/10.3851/IMP2876 [ Links ]
5. Rojas Sanchez P, Prieto L, Jimenez De Ory S, et al. Impact of lopinavir-ritonavir exposure in HIV-1 infected children and adolescents in Madrid, Spain during 2000-2014. PLoS One 2017;12(3):e0173168. https://doi.org/10.1371/journal.pone.0173168 [ Links ]
6. Yang J, Nikanjam M, Best BM, et al. Population pharmacokinetics of lopinavir/ritonavir: Changes across formulations and human development from infancy through adulthood. J Clin Pharmacol 2018;58(12):1604-1617. https://doi.org/10.1002/jcph.1293 [ Links ]
7. WHO. Treatment of children living with HIV. 2021 [cited 2021 Mar 25]. Available from: https://www.who.int/hiv/topics/paediatric/en/ [ Links ]
8. Health NDo. 2019 ART clinical guidelines for the management of HIV in adults, pregnancy, adolescents, children, infants and neonates. 2019 [cited 2021 Mar 25]. Available from: https://www.knowledgehub.org.za/elibrary/2019-art-clinical-guidelines-management-hiv-adults-pregnancy-adolescents-children-infants [ Links ]
9. Ananworanich J, Kosalaraksa P, Hill A, et al. Pharmacokinetics and 24-week efficacy/safety of dual boosted saquinavir/lopinavir/ritonavir in nucleoside-pretreated children. Pediatr Infect Dis J 2005;24(10):874-879. https://doi.org/10.1097/01.inf.0000180578.38584.da [ Links ]
10. Jullien V, Urien S, Hirt D, et al. Population analysis of weight, age, and sex-related differences in the pharmacokinetics of lopinavir in children from birth to 18 years. Antimicrob Agents Chemother 2006;50(11):3548-3555. https://doi.org/10.1128/AAC.00943-05 [ Links ]
11. Weber V, Radeloff D, Reimers B, et al. Neurocognitive development in HIV-positive children is correlated with plasma viral loads in early childhood. Medicine (Baltimore) 2017;96(23):e6867. https://doi.org/10.1097/MD.0000000000006867 [ Links ]
12. Resino S, Bellon J, Munoz-Fernandez M, Infection. SGoH. Antiretroviral activity and safety of lopinavir/ritonavir in protease inhibitor-experienced HIV-infected children with severe-moderate immunodeficiency. J Antimicrob Chemother 2006; 57(3):579-582. https://doi.org/10.1093/jac/dki469 [ Links ]
13. Rosso R, Di Biagio A, Dentone C, et al. Lopinavir/ritonavir exposure in treatment-naive HIV-infected children following twice or once daily administration. J Antimicrob Chemother 2006;57(6):1168-1171. https://doi.org/10.1093/jac/dkl136 [ Links ]
14. Von Hentig N, Babacan E, Staszewski S, Sturmer M, Doerr HW, Lotsch J. Predictive factors for response to a boosted dual HIV-protease inhibitor therapy with saquinavir and lopinavir in extensively pre-treated patients. Antivir Ther 2007;12(8):1237-1246. [ Links ]
15. Burger D, Teulen M, Eerland J, Harteveld A, Aarnoutse R, Touw D. The international interlaboratory quality control program for measurement of antiretroviral drugs in plasma: A global proficiency testing program. Ther Drug Monit 2011;33(2):239-243. https://doi.org/10.1097/FTD.0b013e31820fa528 [ Links ]
 Correspondence:
Correspondence:
Nils von Hentig
hentig@em.uni-frankfurt.de
Received: 04 Feb. 2021
Accepted: 30 Mar. 2021
Published: 11 May 2021

