










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouthern African Journal of HIV Medicine
versão On-line ISSN 2078-6751
versão impressa ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.21 no.1 Johannesburg 2020
http://dx.doi.org/10.4102/sajhivmed.v21i1.1116
ORIGINAL RESEARCH
Human immunodeficiency virus, diabetes mellitus and thyroid abnormalities: Should we be screening?
Somasundram PillayI, II; Davashni PillayIII; Deepak SinghIV; Romashan PillayV
IDepartment of Internal Medicine, King Edward VIII Hospital, Durban, South Africa
IIDepartment of Internal Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIStar College Girls Durban, Durban, South Africa
IVDepartment of Physics, Durban University of Technology, Durban, South Africa
VClifton College Durban, Durban, South Africa
ABSTRACT
BACKGROUND: Diabetes mellitus (DM) and human immunodeficiency virus (HIV) are associated with thyroid abnormalities. Scarce literature exists on the prevalence of thyroid abnormalities in people living with HIV (PLWH) and DM (PLWHD). Guidelines vary regarding thyroid-stimulating hormone (TSH) screening in PLWH and/or DM
OBJECTIVES: This study describes thyroid abnormalities in PLWHD and HIV-uninfected people living with DM (PLWD).
METHOD: This was a cross-sectional analysis of demographic, clinical and biochemical data including TSH results of first-visit patients to the Edendale Hospital diabetes clinic between January 2016 and December 2017
RESULTS: A total of 915 patients were enrolled: 165 PLWHD and 750 PLWD. Overall prevalence of thyroid disorders in PLWD was 8.53% (64/750). The occurrence of 'total' thyroid disorders and of 'subclinical-hypothyroidism' (SCH) was higher in PLWHD than PLWD (23.03% vs. 8.53% and 20.61% vs. 4%, p < 0.001; respectively). People living with HIV and diabetes with thyroid disorders had lower CD4 counts than PLWHD without thyroid disorders (376.08 ± 333.30 vs. 509 ± 341.7 cells/mm3; p = 0.004). Subclinical-hypothyroidism was more common in patients on antiretroviral therapy [ART] (27/136 [19.85%] vs. 4/27 [14.81%], p < 0.001). A significant number of PLWHD acquired HIV before the onset of DM (107/165 [64.85%] vs. 58/165 [35.15%], p < 0.001). Patients on ART were more likely to develop DM, OR 2.66 (95% CI 1.11-6.38.
CONCLUSION: Our study showed an increased prevalence of thyroid disorders (especially SCH) in PLWD and a higher prevalence in PLWHD. Young, overweight, female PLWHD were at risk of SCH. People living with HIV and DM on ART demonstrated an increased prevalence of thyroid dysfunction and poor lipaemic control. The introduction of combined communicable-non-communicable disease clinics might provide an integrated patient screening option.
Keywords: patients with diabetes mellitus; HIV infection; thyroid disorders; antiretroviral therapy; patient screening options.
Introduction
The emerging burden of diabetes mellitus (DM) and chronic human immunodeficiency virus (HIV) infection will inflict strain on the limited resources of the low- and middle-income countries of Africa. Both conditions have been independently associated with thyroid dysfunction.1,2,3,4 Furthermore, thyroid disorders may destabilise the control of both HIV and DM.1,5 Thyroid hormones participate in carbohydrate metabolism, insulin secretion and pancreatic function.6 Similarly, hypothyroidism is associated with the decreased secretion of insulin from the pancreas.7
Shujing et al. showed that thyroid dysfunction, particularly hypothyroidism, is common (33.1%) in people living with HIV (PLWH). This study found that CD4 levels were lower in those with hypothyroidism and that overall biochemical thyroid dysfunction was more frequent in those on antiretroviral therapy (ART) versus those patients who were ART-naïve (39.4% vs. 24.3%, p < 0.05, respectively).2 Other researchers have also noted an increase of thyroid dysfunction in PLWH. In these studies, few, namely 1% - 2% of PLWH, exhibit overt thyroid disease. However, up to 35% have thyroid-related biochemical abnormalities.3,4,8,9 The data have not always been consistent. Jain et al. observed an inverse correlation between CD4 and thyroid-stimulating hormone (TSH) levels and found that progression of HIV was accompanied by a primary hypothyroid state.5 In contrast, Lambert noted that both overt and biochemical thyroid dysfunction in PLWH was rare.10 Harslof et al. found no difference between treated PLWH and HIV-uninfected persons with regard to the prevalence of hypo- or hyperthyroidism.11 Madge et al. has stated that neither HIV nor ART increases the risk of overt or subclinical hypothyroidism (SCH) in PLWH.12
People living with HIV who are on ART are now living longer and have become susceptible to chronic conditions such as DM. In some instances, HIV-infected patients have developed insulin resistance resulting from the inflammatory changes that accompany long-term HIV infection and the metabolic toxicities of the early antiretrovirals used at the time.13,14
The prevalence of thyroid abnormalities in a United Kingdom population (the Whickham Survey)15 was reported to be approximately 6.6%. These data are not specific to PLWD and precede the HIV pandemic by several years. The Colorado (USA) thyroid disease prevalence study of 1995 (n = 25 862) found that 9.5% of attendees at a state fair had an elevated TSH test result whilst 2.2% had decreased levels.16 The overall prevalence of thyroid abnormalities in PLWD is between 12% and 16%.1,17,18,19 Although a Nigerian and an Indian study found higher prevalence rates, namely 46.5% and 30%, respectively, these PLWD subjects may have been non-randomly recruited. Subclinical hypothyroidism was the most frequent diagnosis.20,21
Screening guidelines for thyroid disorders in PLWD remain varied globally.1,21,22,23,24 Thyroid-stimulating hormone is the most sensitive screening test and establishes the diagnosis of hypo- and hyperthyroidism.19,25,26 In the context of HIV, Parsa et al. recommend that TSH be the initial screening tool for the diagnosis of thyroid disorders in PLWH.27 Global and South African data on the prevalence of thyroid abnormalities in PLWHD are scarce. International guidelines vary with regard to TSH screening in PLWH and/or PLWHD.
The primary aim of this study was to provide an initial description of some of the thyroid/TSH abnormalities found in South African PLWHD and in those South African PLWD who are HIV uninfected. A secondary aim was to identify the extent, if any, of differences in thyroid/TSH abnormalities between PLWHD and HIV-uninfected PLWD.
Methods
The visits of all patients attending the Edendale Hospital diabetic clinic are recorded on specially designed data sheets. These were introduced in September 2012 and are completed in triplicate and have been approved by the University of KwaZulu-Natal Biomedical Research and Ethics Committee (BCA 194/95). This ensures that all patients are consulted in a standardised and comprehensive manner. Demographic, clinical and biochemical variables for the patients are captured on these data sheets.
In order to identify concomitant thyroid disorders, TSH tests are performed routinely at all initial clinic visits and the result transferred onto the data sheets. Screening thyroxine (T4) levels were not performed at this clinic because of cost implications. The TSH test, measured in mIU/L, was performed by the National Health Laboratory Services (NHLS) using the Siemens® Avdia Centaur XP analyser. The NHLS's normal TSH range was 0.35 mIU/L to 5.5 mIU/L. A history of pre-existing thyroid disorders was noted in the medical history and documented as either pre-existing hyper- or hypothyroidism. For this study, patients without a history of a thyroid disorder but with a TSH level < 0.35 mIU/L were classified as having subclinical hyperthyroidism, whilst those patients with a TSH > 5.5 mIU/L and no history of a thyroid disorder were captured as having SCH. Patients with elevated TSH were further subdivided into two groups (5.5-10 mIU/L vs. > 10 mIU/L). This was done as both categories have specific therapeutic implications. Total thyroid disorders were categorised as all patients with either a history of hyper- or hypothyroidism plus all those who were found to have subclinical hypo- or hyperthyroidism. The Bio-Rad D-10 machine (Bio-Rad, USA) was used for the HbA1c analysis. The device and the operator (the NHLS) are National Glycohaemoglobin Standardisation Program (NGSP) accredited. Estimated glomerular filtration rates (eGFR) were calculated by the NHLS using the Modified Diet in Renal Disease (MDRD) formula. The CD4 results are reported in cells/µL or cells/mm3.
This is a retrospective cross-sectional study of demographic, clinical and biochemical data, including TSH results, extracted and analysed from the datasheets of all first-visit patients attending the diabetic clinic from 1 January 2016 till 31 December 2017.
Categorical and continuous variables were noted as median and interquartile ranges (25% - 75% IQR). Numbers (n) and percentages (%) are provided for categorical variables. Since data was non-parametric, all data were log-transformed. The results shown are back-transformed values. A p-value < 0.05 was used as an indicator of significance. Data were analysed by Statistical Package for Social Science (SPSS) version 25 for windows (SPSS Inc., Chicago, IL, USA) and Medcalc (version 19.3.1, Ostend, Belgium).
Patient and public involvement
Informed consent was not sought as the study is retrospective and all patient-identifying information was anonymised in the study database. Neither patients nor the general public were involved in the design, the operation, the reporting or the dissemination of this research.
Ethical consideration
Ethics approval for this study was received from the University of KwaZulu-Natal Biomedical Research and Ethics Committee (BE 137/19).
Results
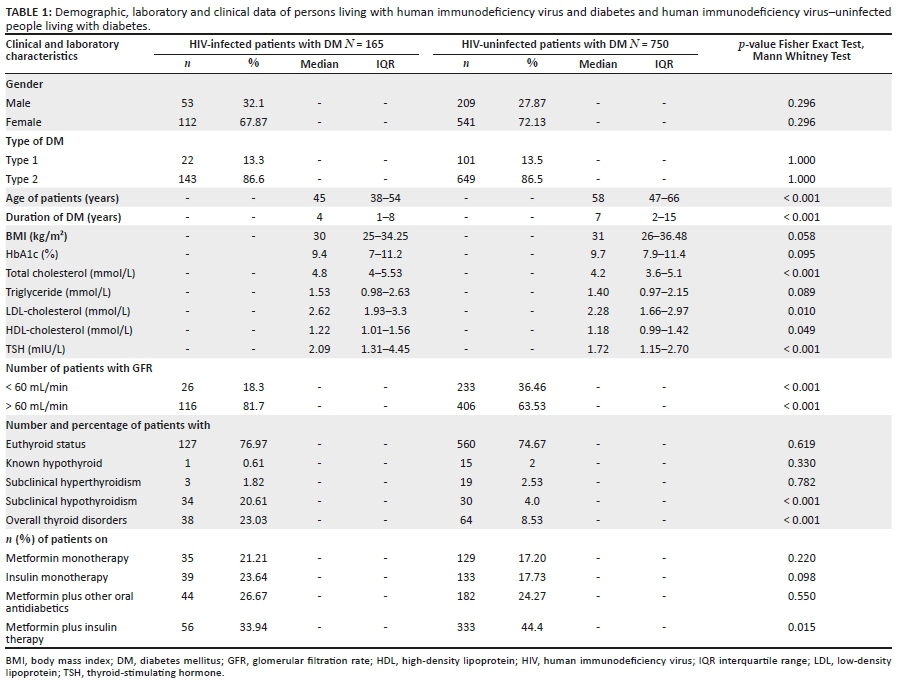
A total of nine hundred and fifteen (n = 915) PLWD were enrolled in the study; n = 165 (18.0%) were PLWHD and n = 750 (81.9%) were HIV-uninfected PLWD (Table 1). The study revealed that a significant number of PLWHD had acquired HIV before the onset of DM (n = 107/165, 64.85% [before] vs. n = 58/165, 35.15% [after]; p < 0.001). After adjusting for age, patients on ART were more likely to develop DM (OR = 2.66 [95% CI 1.11-6.38], p = 0.028). The prevalence of ART usage in patients who acquired HIV infection before and after onset of DM was 67.65% (92/136) vs. 32.35% (44/136), respectively. Elevated body mass index (BMI) was associated with increased likelihood of developing DM (OR = 1.136 [95% CI 1.098-1.175], p < 0.001). The glycaemic control of both the PLWHD and the HIV-uninfected PLWD was generally suboptimal - median ± IQR HbA1c 9.4% (7-11.2) vs. 9.7% (7.9-11.4), respectively. Nonetheless, a higher percentage of PLWHD achieved optimal glycaemic control, namely HbA1c ≤ 7%, compared to the PLWD (26.43% vs. 15.38%, respectively; p < 0.001).
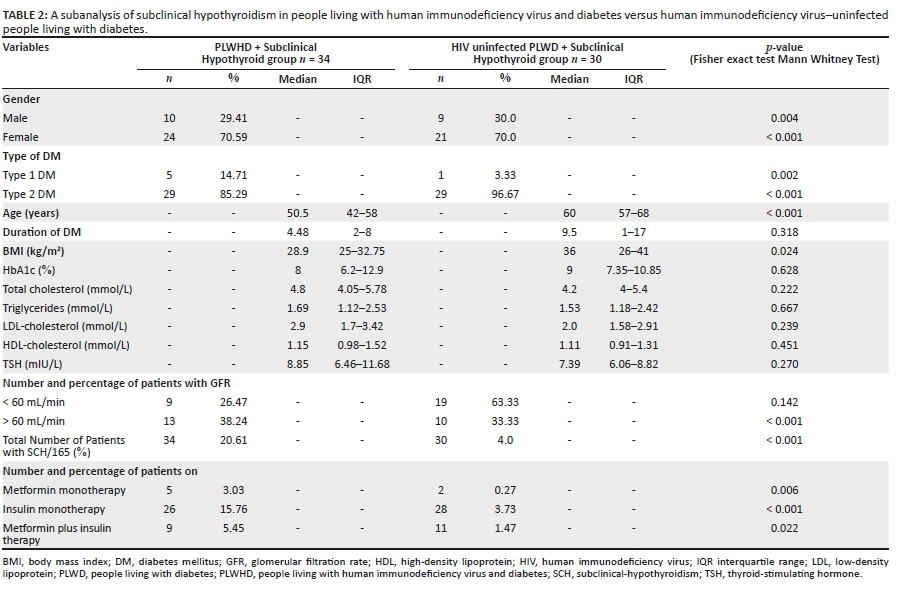
The prevalence of (total) thyroid disorders was significantly higher in the PLWHD than the HIV-uninfected PLWD, n = 38/165 (23.03%) vs. n = 64/750 (8.53%), respectively, p < 0.001. The principal thyroid disorder was SCH. This was disproportionately represented in the PLWHD (Table 2). A significant percentage of the PLWHD with SCH were female, p < 0.001, had Type 2 DM and yet were on insulin monotherapy. The median age of the SCH cohort was older than that of the originator group. The median ± IQR of HIV infection and ART usage in the PLWHD with SCH was 5 (2-9) and 5 (1-9) years, respectively. This group had a median CD4 count of 423 (92.76-888.41) cells/mm3. The median CD4 count and inter-quartile range of the entire cohort of PLWHD (n = 165) was 446 (155-703) cells/mm3. The median CD4 level of PLWHD with thyroid disorders was, however, significantly lower than those PLWHD without thyroid disorders: CD4 = 376.08 ± 333.30 vs. 509 ± 341.75, respectively; p = 0.004.
People living with HIV and DM versus the HIV-uninfected PLWD were younger, had a shorter duration of DM, a lower but non-significant BMI, p = 0.058, and a larger number of individuals with normal renal function namely, GFR > 60 mL/min. The PLWHD group also had significantly higher total LDL and HDL cholesterols (p < 0.001, p = 0.01, p = 0.049, respectively). No such associations characterised patients with subclinical hyperthyroidism (Table 1). The median IQR of the duration of HIV infection and of ART usage by PLWHD was 6 (2-9.25) and 5 (2-9) years, respectively.
Despite the concomitant thyroid disorder, a group of 68 (7.43%) patients continued to receive metformin monotherapy. Less than a percent (7/915, 0.77%) of patients with SCH were on metformin.
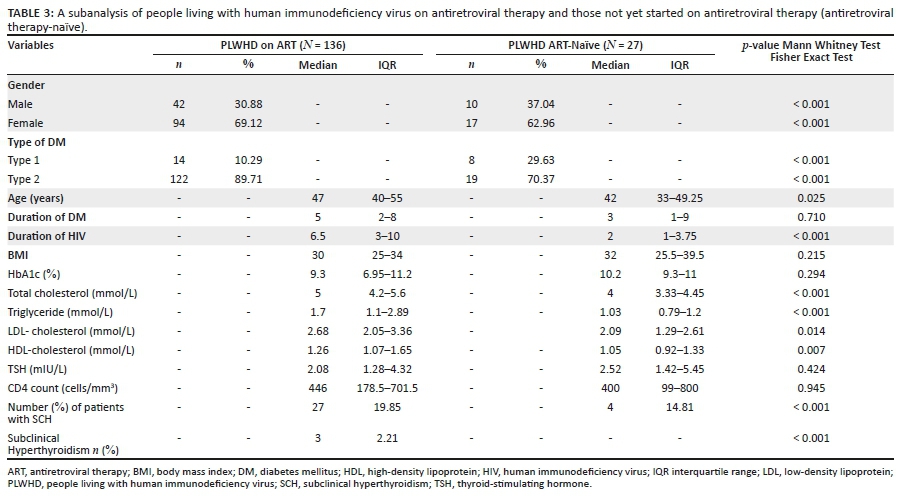
Table 3 demonstrates that patients on ART were significantly younger, female and had type 2 DM, and had a higher total, HDL and LDL cholesterol and triglyceride levels; SCH was substantially more common in patients on ART. Patients who were on ART had HIV infection for a longer duration than those who were not. The majority of patients on ART were on a first-line NNRTI-based regimen compared to second-line boosted protease inhibitor-based regimen (11/136, 8.90% vs. 125/136, 91.91%, respectively).
Whilst we found an inverse correlation between CD4 counts and TSH levels within the entire PLWHD cohort, this was not significant (r = ‒0.084. Pearson's correlation). This inverse correlation was present in patients on ART and those that were ART-naïve (r = 0.083 vs. 0.091, respectively).
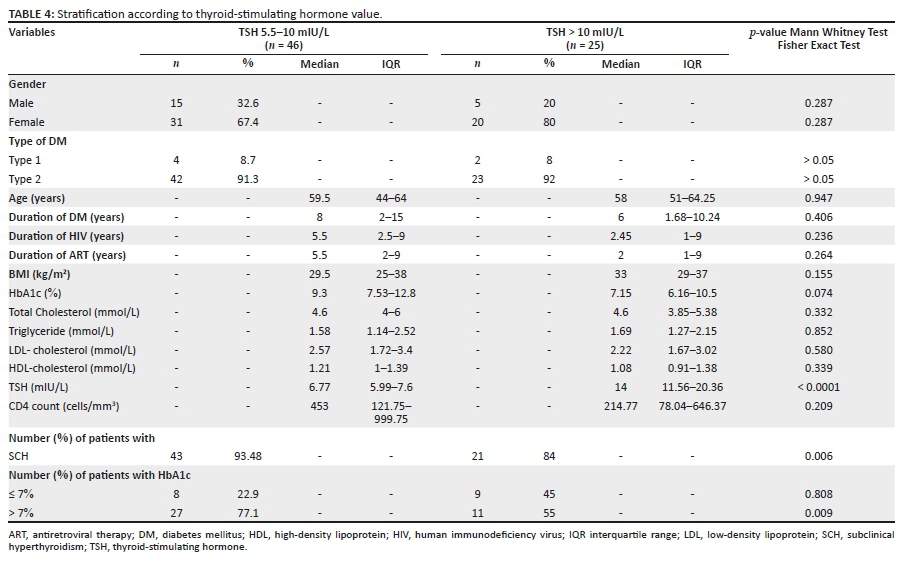
Subdivision of the cohorts into those with a moderately high TSH (5.5-10 mIU/L) and those with an extremely high TSH (> 10 mIU/L) revealed that the two groups were evenly matched for most demographic, clinical and biochemical variables. A significantly greater number of patients in the TSH (5.5-10) cohort had suboptimal glycaemic control (p = 0.009). A substantial number of patients with SCH had TSH values in the range of 5.5-10 mIU/L (p = 0.006). The shorter duration of both HIV and DM in those with very high TSH levels suggests a group who are at risk of a more precipitous course of SCH. Women outnumber men in this 'more severe' group, and this particularly so in obese women (Table 4).
Discussion
Diabetes mellitus and HIV infection pose a long-term global healthcare and fiscal problem for Africa. Both are independently associated with thyroid abnormalities. Data on the global prevalence of thyroid disorders in PLWHD are limited, with African data even more scarce.
Our study showed that within the cohort of HIV-uninfected PLWD, thyroid disorders were more common in female type 2 PLWD. These results correlated with those of Udiong et al. in Nigeria,20 but not so with Perros et al., whose data indicated that thyroid abnormalities were more common in type 1 DM.1 The subject base of our diabetic clinic reflects a preponderance of adult type 2 PLWD. Most young type 1 PLWD are cared for at the local tertiary hospital. The PLWHD had better glycaemic control, were younger, had DM for a shorter duration, had lower BMI and preserved renal function but had higher lipaemic levels than their HIV-uninfected PLWD counterparts, whilst the group of patients who were ART-naïve had a shorter duration of HIV infection and a decreased prevalence of SCH. The PLWHD may offer an opportunity to get ahead on DM and possibly thyroid management if integrated into ART control.
Twenty-three per cent (23.03%) of the PLWHD in this study had thyroid disorders, most notably, SCH in 20.61%. These results were similar to what Shujing et al.,2 Madeddu et al.,4 Brockmeyer et al.28 and Silva et al.9 showed in their studies. People living with human immunodeficiency virus and diabetes were mostly female, older, had type 2 DM, had increased BMI and were mainly on insulin monotherapy when compared to PLWHD. Weight gain in PLWHD may be a marker of thyroid dysfunction and needs to emphasised in patient evaluation.
Discussion on the implications of SCH and its management is ongoing. The risk of SCH is increased in PLWD, PLWHD and those on ART.3,4,8,29,30 Han et al. concluded in their meta-analysis that PLWD with SCH had increased diabetes-related complications in the form of nephropathy, retinopathy, peripheral arterial disease and peripheral neuropathy.31 The most important consequence of SCH remains progression to overt hypothyroidism (ranging from 3% to 18% annually).32,33,34,35,36 The Rotterdam study demonstrated an association between patients with SCH, aortic calcification and myocardial infarction and identified SCH as an independent risk factor for myocardial infarction.37 Other observational studies have also found associations between SCH and coronary artery disease.38,39,40 This association was, however, not found in the Wickham study.41 Haentjens et al. in their analysis of seven cohort studies found that there was an increased risk of all-cause mortality in patients with SCH, more so in patients with co-morbid conditions.42 We show that SCH is associated with hyperlipidaemia. Undiagnosed SCH may affect metabolic control and worsen cardiovascular risk in PLWD.43,44 Baseline TSH screening would help identify those patients who are at higher cardiovascular risk that need closer monitoring.
We demonstrated that over one-third (25/71, 35.21%) of our patients with SCH had TSH levels of > 10 mIU/L, and this was predominantly in obese female patients with a short duration of DM and HIV infection. Most authors agree that patients with a TSH > 10 mIU/L should be initiated onto levothyroxine therapy (LT).45,46,47 However, 64.78% (46/71) of our study SCH patients had TSH levels of between 5.5 and 10 mIU/L, which poses a therapeutic conundrum to the attending physician. Levothyroxine therapy in this group of patients is still very much debated in literature. Both Surks et al. and Kong et al. found no benefit in initiation of LT in this TSH range,48,49 whilst McDermott et al., Kadiyala et al. and Fatourechi advocated that patients with SCH with co-morbid cardiovascular conditions be treated with LT.45,46,50 It must be borne in mind that these studies were conducted in HIV-uninfected patients.
Thyroid dysfunction in the form of SCH was found to be significantly more common in patients on ART therapy in our study (22.06%). Although less common, it must be noted that thyroid disorders were also prevalent in patients who were ART-naïve (14.81%). This finding has also been demonstrated by Jain et al. in their study conducted in India.5 Our study also found that the CD4 counts were significantly lower in patients with combined HIV infection and thyroid disorders. The link between being on ART, having lower CD4 counts and thyroid dysfunction was also found in the study conducted by Shujing et al.2 and serves to highlight the importance of screening for thyroid disorders in both HIV clinics and in combined communicable-non-communicable disease (HIV-DM) clinics. In our study, patients on ART had higher levels of total cholesterol, triglycerides and LDL cholesterol and had HIV for a longer duration than their ART-naïve counterparts, illustrating the complex interactions between ART and increased cardiovascular risk.
Interestingly, we found that a significant number of HIV-infected patients developed DM after the onset of HIV infection. The aetiology of DM in the setting of HIV can be attributed to either the inflammatory milieu associated with the HIV infection itself, the ART or increased patient longevity.14 This finding underscores the importance of screening for DM in HIV clinics.
Studies have found that the occurrence of DM in the presence of HIV infection is usually due to insulin resistance rather than insulin deficiency and therefore is more likely to be type 2 in nature.13 Metformin use for the treatment of DM in the presence of HIV has been associated with increased risk of developing diarrhoea and may cause lactic acidosis in patients with renal failure. The advantages of metformin use in PLWHD remains that it is an insulin sensitiser, is cost-effective and can assist with weight loss.51 Insulin remains the treatment of choice in PLWHD and is endorsed by the American Association of Clinical Endocrinologists. The benefits of using insulin is that it does not cause gastrointestinal side effects and has no interactions with ART; however, insulin usage does pose increased risks of hypoglycaemia and requires safe disposal of needles.52 Metformin use in patients is discouraged in PLWD and thyroid dysfunction as in-vitro studies using metformin have demonstrated that metformin has inhibitory effects on cell proliferation.53 The majority (81.82%) of our PLWHD were still on metformin therapy (either monotherapy or in combination with other oral antidiabetic therapies or with insulin). However, within the group of HIV-uninfected PLWD and thyroid dysfunction, this message of the decreased use of metformin seemed to have been heeded, as the majority of these patients were on insulin therapy as compared to metformin (6.93% vs. 4.26%, respectively). This trend of using insulin instead of metformin monotherapy was also observed in the majority of patients with HIV infection and thyroid disorders (17.58% vs. 10.31%, respectively).
The cohort comprising the PLWHD but with no thyroid disorders were generally female, had type 2 diabetes, were younger, had a shorter duration of DM and a lower BMI with a significant percentage having glomerular filtration rates of > 60 mL/min. Pillay et al. have shown previously that PLWHD were at increased risk for nephropathy.54 Our findings of higher GFR and a greater percentage of patients achieving target HbA1c can be explained by the fact that this cohort were younger, not obese and only had DM for a short duration. Another important study finding was that this cohort had significantly higher total cholesterol and triglycerides when compared to their HIV-uninfected counterparts. Both DM and HIV are predisposing factors for cardiovascular morbidity and mortality.43,44,55 Our findings of elevated total cholesterol and triglyceride in this cohort will serve to further increase their cardiovascular risk.
Although not statistically significant, glycaemic control was poorer in the PLWHD compared to the PLWD with regards to those:
•with overall total thyroid disorders
•with SCH
•on ART
Future prospective studies are needed to determine the extent of this glycaemic difference between these groups of patients which may aid in providing another therapeutic avenue in improving overall diabetes control.
Strengths and limitations of study
•Results of this study will help strengthen the case for evaluation of thyroid disorders in PLWD but more especially in PLWHD.
•The limitations of this study include that we only used a single TSH level for diagnosis of thyroid dysfunction. Assay-related analytic errors and transient thyroid dysfunction secondary to drugs like lithium and amiodarone were not assessed.
•People living with HIV are at heightened risk of developing the euthyroid sick syndrome. During periods of recovery from acute illness, the TSH might be increased in this condition and may result in an overdiagnosis of SCH.
•Another limitation included that no T4 or T3 testing was performed in patients with low or high TSH. As this was a retrospective first visit study, we were able only to collect TSH data that were gathered during screening on first visit.
•A further limitation remains that no viral load and effectiveness of ART data was available to assess if patients were taking their medication and whether ART influenced the outcome.
Conclusion
Data on thyroid disorders in PLWHD are scarce. Our study has shown an increased prevalence of thyroid disorders (most notably SCH) in HIV-uninfected PLWD and an even higher prevalence in PLWHD.
Young overweight women who are HIV infected and have DM seem to be particularly at risk of SCH. This is a 'key' population group that should be evaluated in all HIV clinics for thyroid disorders.
People living with human immunodeficiency virus and diabetes on ART were shown to have an increased prevalence of thyroid dysfunction with poorer lipaemic control. This particular group of patients on ART need to be regularly screened for the aforementioned cardiovascular complications. The introduction of combined communicable-non-communicable disease clinics might provide an integrated option for these patients.
Acknowledgements
Competing interests
The authors have declared that no competing interest exists.
Authors' contributions
S.P. made substantial contributions to conception and design of the work, writing of the paper and final approval and agreed to be accountable for all aspects of the research. D.P. and R.P. made substantial contributions to conception of the work, critically reviewed and edited the draft paper and final approval and agreed to be accountable for all aspects of the research. D.S. made substantial contribution to the generation of statistics and critically reviewed the article and agreed to be accountable for all aspects of the research.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.Perros P, McCrimmon RJ, Shaw G, Frier BM. Frequency of thyroid dysfunction in diabetic patients: Value of annual screening. Diabet Med. 1995;12(7):622-627. https://doi.org/10.1111/j.1464-5491.1995.tb00553.x [ Links ]
2.Shujing J, Chanqzhong J, Hoxtermann S, et al. Prevalence and influencing factors of thyroid dysfunction in HIV-infected patients. BioMed Res Int. 2016;2016:3874257. https://doi.org/10.1155/2016/3874257 [ Links ]
3.Beltran S, Lescure FX, Deasilloud R, et al. Increased prevalence of hypothyroidism among human immunodeficiency virus-infected patients: A need for screening. Clin Infect Dis. 2003;37(4):579-583. https://doi.org/10.1086/376626 [ Links ]
4.Madeddu G, Spanu A, Chessa F, et al. Thyroid function in human immunodeficiency virus patients treated with highly active antiretroviral therapy. Clin Endocrinol. 2006;64(4):375-383. https://doi.org/10.1111/j.1365-2265.2006.02472.x [ Links ]
5.Jain G, Devpura G, Gupta BS. Abnormalities in the thyroid function tests as surrogate marker of advancing HIV infection in infected adults. JAPI. 2009;57(7):508-510. [ Links ]
6.Hage M, Zantout MS, Azar ST. Thyroid disorders and diabetes mellitus. Sage J Thyroid Res. 2011;2011:439463. https://doi.org/10.4061/2011/439463 [ Links ]
7.Stanicka S, Vondra K, Pelikanova T, Vlcek P, Hill M, Zamrazil V. Insulin sensitivity and counter-regulatory hormones in hypothyroidism and during thyroid hormone replacement therapy. Clin Chem Lab Med. 2005;43(7):715-720. https://doi.org/10.1515/CCLM.2005.121 [ Links ]
8.Calza L, Manfredi R, Chiodo F, et al. Subclinical hypothyroidism in HIV-infected patients receiving highly active antiretroviral therapy. J Acquir Immun Defic Syndr. 2002;31(3):361-363. https://doi.org/10.1097/00126334-200211010-00014 [ Links ]
9.Silva GA, Andrade MC, Sugui A, et al. Association between antiretrovirals and thyroid diseases: A cross-sectional study. Arch Endocrinol Metab. 2015;59(2):116-122. https://doi.org/10.1590/2359-3997000000023 [ Links ]
10.Lambert M. Thyroid dysfunction in HIV infection. Baillieres Clin Endocrinol Metabol. 1994;8(4):825-835. https://doi.org/10.1016/S0950-351X(05)80303-9 [ Links ]
11.Harslof M, Knudsen A, Benfield T, et al. No evidence of increased risk of thyroid dysfunction in well-treated people living with HIV. AIDS. 2018;32(15):2195-2199. https://doi.org/10.1097/QAD.0000000000001954 [ Links ]
12.Madge S, Smith CJ, Lampe FC, et al. No association between HIV disease and its treatment and thyroid function. HIV Med. 2007;8(1):22-27. https://doi.org/10.1111/j.1468-1293.2007.00422.x [ Links ]
13.Kalra S, Kalra B, Agrawal N, Unnikrishnan AG. Understanding diabetes in patients with HIV/AIDS. Diabetol Metab Syndr. 2011;3(1):2. https://doi.org/10.1186/1758-5996-3-2 [ Links ]
14.De Wit S, Sabin CA, Weber R, et al. Incidence and risk factors for new-onset diabetes in HIV-infected patients. The data collection on adverse events of anti-HIV drugs (D: A:D) study. Diabetes Care. 2008;31(6):1224-1229. https://doi.org/10.2337/dc07-2013 [ Links ]
15.Tunbridge WMG, Evered DC, Hall R. The spectrum of thyroid disease in a community: The Whickham survey. Clin Endocrinol. 1977;7(6):481-493. https://doi.org/10.1111/j.1365-2265.1977.tb01340.x [ Links ]
16.Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The Colorado thyroid disease prevalence study. Arch Intern Med. 2000;160(4):526-534. https://doi.org/10.1001/archinte.160.4.526 [ Links ]
17.Papazafiropoulou A. Prevalence of thyroid dysfunction among Greek type 2 diabetic patients attending an outpatient clinic. J Clin Med Res. 2010;2(2):75-78. https://doi.org/10.4021/jocmr2010.03.281w [ Links ]
18.Akbar DH, Ahmed MM, Al-Mughales J. Thyroid dysfunction and thyroid autoimmunity in Saudi type 2 diabetics. Acta Diabetol. 2006;43(1):14-18. https://doi.org/10.1007/s00592-006-0204-8 [ Links ]
19.Wang C. The relationship between type 2 diabetes mellitus and related thyroid diseases. J Diabetes Res. 2013;2013;390534. https://doi.org/10.1155/2013/390534 [ Links ]
20.Udiong CEJ, Udoh AE, Etukudoh ME. Evaluation of thyroid function in diabetes mellitus in Calabar, Nigeria. Indian J Clin Biochem. 2007;22(7):74-78. https://doi.org/10.1007/BF02913318 [ Links ]
21.Singh G, Gupta V, Sharma AK, Gupta N. Evaluation of thyroid dysfunction among type 2 diabetic Punjabi population. Adv Biores. 2011;2(2):3-9. [ Links ]
22.Ladenson PW, Singer PA, Ain KB, et al. American thyroid association guidelines for detection of thyroid dysfunction. Arch Int Med. 2000;160(11):1573-1575. https://doi.org/10.1001/archinte.160.11.1573 [ Links ]
23.Baskin HJ, Cobin RH, Duick DS, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. Endocr Pract. 2002;8(6):457-469. https://doi.org/10.4158/1934-2403-8.6.457 [ Links ]
24.UK guidelines for the use of thyroid function tests [homepage on the Internet]. 2006 [cited 2006 Jul n.d.]. Available from: http://british-thyroid-association.org/info-for-patients/Docs/TFT_guideline_final_version_July_2006.pdf [ Links ]
25.Stockigt JR. Case finding and screening strategies for thyroid dysfunction. Clin Chim Acta. 2002;315(1-2):111-124. https://doi.org/10.1016/s0009-8981(01)00715-x [ Links ]
26.Warren RE, Perros P, Nyirenda MJ, Frier BM. Serum thyrotropin is a better predictor of future thyroid dysfunction than thyroid autoantibody status in biochemically euthyroid patients with diabetes: Implications for screening. Thyroid. 2004;14(10):853-857. https://doi.org/10.1089/thy.2004.14.853 [ Links ]
27.Parsa AA, Bhangoo A. HIV and thyroid dysfunction. Rev Endocr Metab Disord. 2013;14(1):127-131. https://doi.org/10.1007/s11154-013-9248-6 [ Links ]
28.Brockmeyer N, Kreuter A, Bader A, Seemann U, Reimann G. Prevalence of endocrine dysfunction in HIV infected men. Horm Res. 2000;54(5-6):294-295. https://doi.org/10.1159/000053274 [ Links ]
29.Diez JJ, Iglesias P. Subclinical hyperthyroidism in patients with type 2 diabetes. Endocrine. 2012;42(1):157-163. https://doi.org/10.1007/s12020-012-9621-3 [ Links ]
30.Helfand M. Screening for subclinical thyroid dysfunction in nonpregnant adults: A summary of the evidence for the US Preventive Services Task Force. Ann Intern Med. 2004;140(2):128-141. https://doi.org/10.7326/0003-4819-140-2-200401200-00015 [ Links ]
31.Han C, He X, Xinghai X, et al. Subclinical hypothyroidism and type 2 diabetes: A systematic review and meta-analysis. PLoS One. 2015;10(8):e0135233. https://doi.org/10.1371/journal.pone.0135233 [ Links ]
32.Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the community: A twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf). 1995;43(1):55-68. https://doi.org/10.1111/j.1365-2265.1995.tb01894.x [ Links ]
33.Kabadi UM. Subclinical hypothyroidism. Natural course of the syndrome during a prolonged follow-up study. Arch Intern Med. 1993;153(8):957-961. https://doi.org/10.1001/archinte.1993.00410080025004 [ Links ]
34.Tunbridge WMG, Brewis M, French JM, et al. Natural history of autoimmune thyroiditis. Br Med J. 1981;282(6260):258-262. https://doi.org/10.1136/bmj.282.6260.258 [ Links ]
35.Wang C, Crapo LM. The epidemiology of thyroid disease and implications for screening. Endocrinol Metab Clin North Am. 1997;26(1):189-218. https://doi.org/10.1016/s0889-8529(05)70240-1 [ Links ]
36.Huber G, Mitrache C, Guglielmetti M, Huber P, Staub JJ. Predictors of overt hypothyroidism and natural course: A long-term follow-up study in impending thyroid failure. 71st Annual Meeting of the American Thyroid Association, Portland, OR; 1998; Abstract 109, September 1998. [ Links ]
37.Hak AE, Pols HAP, Visser TJ, Drexhage HA, Hofman A, Witteman JCM. Subclinical hypothyroidism is an independent risk factor for atherosclerosis and myocardial infarction in elderly women: The Rotterdam Study. Ann Intern Med. 2000;132(4):270-278. https://doi.org/10.7326/0003-4819-132-4-200002150-00004 [ Links ]
38.Rodondi N, Aujesky D, Vittinghoff E, Cornuz J, Bauer DC. Subclinical hypothyroidism and the risk of coronary heart disease: A meta-analysis. Am J Med. 2006;119(7):541-551. https://doi.org/10.7326/0003-4819-132-4-200002150-00004 [ Links ]
39.Ochs N, Auer R, Bauer D, et al. Meta-analysis: Subclinical thyroid dysfunction and the risk for coronary heart disease and mortality. Ann Intern Med. 2008;148(11):832-845. https://doi.org/10.7326/0003-4819-148-11-200806030-0022 [ Links ]
40.Singh S, Duggal J, Molnar J, Maldonado F, Barsano CP, Arora R. Impact of subclinical thyroid disorders on coronary heart disease, cardiovascular and all-cause mortality: A meta-analysis. Int J Cardiol. 2008;125(1):41-48. https://doi.org/10.1016/j.ijcard.2007.02.027 [ Links ]
41.Vanderpump MP, Tunbridge WM, French JM, et al. The development of ischemic heart disease in relation to autoimmune thyroid disease in a 20-year follow-up study of an English community. Thyroid. 1996;6(3):155-160. https://doi.org/10.1089/thy.1996.6.155 [ Links ]
42.Haentjens P, Van Meerhaeghe A, Poppe K, Velkeniers B. Subclinical thyroid dysfunction and mortality: An estimate of relative and absolute excess all-cause mortality based on time-to-event data from cohort studies. Eur J Endocrinol. 2008;159(3):329-341. https://doi.org/10.1530/EJE-08-0110 [ Links ]
43.Mohn A, Di Michele S, Di Luzio R, Tumini S, Chiarelli F. The effect of subclinical hypothyroidism on metabolic control in children and adolescents with Type 1 diabetes mellitus. Diabet Med. 2002;19(1):70-73. https://doi.org/10.1046/j.1464-5491.2002.00635.x [ Links ]
44.Franzese A, Buono P, Mascolo M, Leo AL, Valerio G. Thyroid autoimmunity starting during the course of type 1 diabetes denotes a subgroup of children with more severe diabetes. Diabetes Care. 2000;23(8):1201-1202. https://doi.org/10.2337/diacare.23.8.1201 [ Links ]
45.Fatourechi V. Subclinical hypothyroidism: An update for primary care physicians. Mayo Clin Proc. 2009;84(1):65-71. https://doi.org/10.4065/84.1.65 [ Links ]
46.McDermott MT, Ridgway EC. Subclinical hypothyroidism is mild thyroid failure and should be treated. J Clin Endocrinol Metab. 2001;86(10):4585-4590. https://doi.org/10.1210/jcem.86.10.7959 [ Links ]
47.Chu JW, Crapo LM. The treatment of subclinical hypothyroidism is seldom necessary. J Clin Endocrinol Metab. 2001;86(10):4591-4599. https://doi.org/10.1210/jcem.86.10.7961 [ Links ]
48.Surks MI, Ortiz E, Daniels GH, et al. Subclinical thyroid disease: Scientific review and guidelines for diagnosis and management. JAMA. 2004;291(2):228-238. https://doi.org/10.1001/jama.291.2.228 [ Links ]
49.Kong WM, Sheikh MH, Lumb PJ, et al. A 6-month randomised trial of thyroxine treatment in women with mild subclinical hypothyroidism [published correction appears in Am J Med. 2002;113(3):264] Am J Med. 2002;112(5):348-354. https://doi.org/10.1016/s0002-9343(02)01022-7 [ Links ]
50.Kadiyala R, Peter R, Okosieme OE. Thyroid dysfunction in patients with diabetes: Clinical implications and screening strategies. Int J Clin Pract. 2010,64(8):1130-1139. https://doi.org/10.1111/j.1742-1241.2010.02376.x [ Links ]
51.Kohli R, Shevitz A, Gorbach S, Wanke C. A randomised placebo-controlled trial of metformin for the treatment of HIV lipodystrophy. HIV Med. 2007;8(7):420-426. https://doi.org/10.1111/j.1468-1293.2007.00488.x [ Links ]
52.Rao PV. Persons with type 2 diabetes and co-morbid active tuberculosis should be managed with insulin. Int J Diabetes Dev Ctries. 1999;19(1):79-88. [ Links ]
53.Klubo-Gwiezdzinska J, Jensen K, Costello J, et al. Metformin inhibits growth and decreases resistance to anoikis in medullary thyroid cancer cells. Endocr Relat Cancer. 2012;19(3):447-456. https://doi.org/10.1530/ERC-12-0046 [ Links ]
54.Pillay S, Aldous C, Mahomed F. A deadly combination - HIV and diabetes: Where are we now? SAMJ. 2016;106(4):378-383. https://doi.org/10.7196/SAMJ.2016.v106i4.9950 [ Links ]
55.Hsue PY, Walters DD. Time to recognise HIV infection as a major cardiovascular risk factor. Circulation. 2018;138(11):1113-1115. https://doi.org/10.1161/circulationAHA.118.036211 [ Links ]
 Correspondence:
Correspondence:
Somasundram Pillay
drspillay@iafrica.com
Received: 18 June 2020
Accepted: 04 Sept. 2020
Published: 09 Nov. 2020
Project Number: BE 137/19


{kind=link}
{kind=link}
{kind=link}
{kind=link}