










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouthern African Journal of HIV Medicine
versão On-line ISSN 2078-6751
versão impressa ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.20 no.1 Johannesburg 2019
http://dx.doi.org/10.4102/sajhivmed.v20i1.976
ORIGINAL RESEARCH
Acceptability of short text messages to support treatment adherence among adolescents living with HIV in a rural and urban clinic in KwaZulu-Natal
Mthokozisi A. Cele; Moherndran Archary
Department of Paediatrics and Child Health, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: The use of mobile communication technologies (mHealth) has improved adherence and viral suppression among HIV-infected adults. Adolescents have disproportionally lower levels of adherence and viral suppression compared with adults, potentially impacting the goal of 90% viral suppression by 2030.
OBJECTIVES: The aim of this study was to evaluate the acceptability of using short message service (SMS)-based mHealth interventions as a tool to improve adherence in HIV-infected adolescents in a rural and urban clinic in KwaZulu-Natal (KZN).
METHOD: A cross-sectional study with a sample size of 100 participants was conducted in a rural and urban clinic in KZN, from January 2018 to June 2019. Fifty participants were sequentially enrolled from each clinic. A questionnaire was self-administered with the assistance of the treating clinician depending on the adolescent's level of understanding. Informed consent was obtained from guardians and questionnaires were anonymised. Appropriate descriptive and comparative statistics were used.
RESULTS: The mean age of participants was 15 years, with 88% having access to a mobile device (MOD). There was no significant difference in MOD ownership between rural and urban participants. Majority of participants (65%) were willing to receive SMS-based adherence support with no difference between rural and urban area.
CONCLUSION: With high rates of MOD ownership and acceptability (willingness to use mHealth to improve health status), SMS-based mHealth interventions have the potential to improve adherence and viral suppression in adolescents living with HIV in both rural and urban KZN. Further studies with a larger sample size need to be conducted to further explore these findings.
Keywords: adolescents on antiretroviral therapy; HIV; text messaging system; adherence support; retention cell phone technology; mHealth.
Introduction
In 2015, an estimated 1.8 million adolescents worldwide were living with HIV,1 with over two-thirds living in sub-Saharan Africa (SSA).2 In 2018, an estimated 310 000 adolescents were living with HIV in South Africa.3 The earlier initiation of antiretroviral treatment (ART) in vertically HIV-infected children has resulted in more children surviving into adolescence potentially increasing these estimates in the future. With the aim of controlling the HIV epidemic, the World Health Organization (WHO) launched the 90-90-90 campaign, which aims for 90% of people living with HIV knowing their HIV status, 90% started on ART and 90% with a suppressed HIV viral load.4
One of the challenges in achieving the 90-90-90 targets is the poor adherence among adolescents in Africa.5 Poor adherence is associated with lower rates of viral suppression both in adult and adolescent populations.6,7,8 A recent systemic review estimated that viral suppression ranged from 27% to 89% in Africa.9 West and Central Africa had the lowest viral suppression rate (8%), while East Africa had the highest (56%).10 In South Africa, a study conducted in Gauteng and Mpumalanga found that adolescents were more likely to be unsuppressed by 12 months (Risk Ratio 2.30, 95% CI, 1.38-3.82) than adult patients.11
Adolescents also have lower rates of retention in care compared with adults.12 An evaluation of lost to follow-up in adolescents starting ART in four SSA countries was 20% at 3 months and 44% at 12 months.13 In a study conducted in a cohort of 241 adolescents in South Africa between 2007 and 2015, 89% were retained in care and 81% achieved viral suppression. Furthermore, adolescents attending designated adolescent clinics had higher retention rates (95%) compared with those attending paediatric clinics (85%). The needs of adolescents should be addressed differently from the general population,14 with individualised care associated with higher adolescent retention in care.15 Mobile communication technologies in medical care (mHealth) have the potential to address some of these issues.
mHealth refers to the use of mobile devices (MODs), such as mobile phones to support practice of medicine and public health.16 There are several variations to mHealth interventions, including short messaging service (SMS) reminders, gaming applications (apps) and interactive mobile apps. A mobile app study conducted in New England found improved motivation in taking antiretroviral therapy,17 while a MedMinder pill counter that generates automated SMS to adolescents found that there was a significant increase in CD4 counts.18
A randomised controlled trial of a personalised SMS reminder to promote adherence in adults in Kenya improved adherence from 28% to 64% after 3 months.19 In studies conducted in Uganda and Kenya found that 97% of the surveyed participants thought that SMS reminders would improve treatment adherence.19,20 A study conducted in Ethembeni clinic in Durban found that 98% of the adult participants remembered their medications and would recommend the service to a friend.21 Concerns expressed regarding mHealth included privacy and security with unintentional sharing of personal information being of most concern.22 Sharing of MODs is common in Africa and has implications on mHealth interventions. The majority (88%) of respondents from a study in Mozambique felt that unauthorised access to text messages could result in accidental disclosure of their HIV status because they share MODs.23 Sharing of MODs may also result in a delay in relaying of the message or message not being delivered to right person.20 Intermittent and limited funding for public health and sustainable mHealth interventions is a major problem especially in resource-limited countries with competing priorities.24
The majority of mHealth studies have been based on an SMS reminder that is sent as daily or weekly reminders. More research is needed to determine the optimal frequency of messages to support adherence. Improvements in mobile technology have allowed interactive text messages that have been shown to help with emotional support and build patient knowledge and allowed the adolescents to ask questions.7 However, SMS provides an easy, cheap and accessible technology for mHealth that is accessible even in remote areas with limited resources.25 An mHealth intervention (MomConnect) in pregnant women was launched in South Africa in 2014 and has been successfully implemented in the adult population. To our knowledge, there is limited data evaluating mHealth interventions in adolescent populations in KwaZulu-Natal (KZN), especially comparing rural and urban populations.
The aim of our study was to evaluate the acceptability of using SMS-based mHealth interventions as the tool for mHealth in adolescents living with HIV from KZN, comparing a rural and urban clinic, with the aim to support adherence and retention in care. Furthermore, we explored the preferred type of mHealth support (peer support or daily or weekly reminders).
Methodology
We conducted a cross-sectional observational survey in a rural and urban clinic in KZN from January 2018 to June 2019. The two study sites, a rural clinic (Umbumbulu clinic) and an urban clinic (King Edward VIII Hospital [KEH]) were selected based on the geographic location and patient profile. Umbumbulu clinic is in a deep rural area in a sub-district of KZN, 30 km south of Durban. The Umbumbulu clinic is a primary healthcare centre serving the marginalised community of Umbumbulu, with a high rate of unemployment, poor transport system and patients have to walk 3 km - 5 km to access the clinic. Umbumbulu clinic is a combined service serving children, adolescents and adults. The ARV clinic (Philani clinic) at KEH, Durban, serves an urban and peri-urban area, including patients from formal and informal housing in Umbilo, Cato Manor, Manor Gardens and Mayville. These communities include low- and middle-class families.
Population and sample
We sequentially enrolled 100 adolescents (12-19 years of age) living with HIV on ART from the adolescent clinics in the two sites. As an exploratory pilot study, the sample size of 100 was based on availability of limited resources and the patient numbers at each of the study sites. The sample size was powered to detect a difference in mHealth acceptability of 70% between the rural and urban sites with a power of 95% and alpha of 0.05. A further study with a larger sample size would need to be performed to determine smaller differences between the two groups. Fifty participants were enrolled from each clinic with an equal distribution of males and females. Informed consent to participate in the study was provided by the parent or guardian (telephonic consent was provided when the adolescent came alone), the adolescent provided signed assent and those above 18 years signed informed consent. S.N. at Umbumbulu Clinic and C.K. at KEH recruited participants while registering their details before the doctor consultation. No patient incentives were provided for participation in the study as patients were recruited during scheduled visits and the questionnaire was completed while waiting for their consultations. The investigator conducted a 2-h workshop 2 months prior to the commencement of the study at both clinics, to engage with S.N. and C.K. and standardise the survey collection. Participants were provided with a pen and questionnaire in the waiting area and answered the questionnaire while waiting for their consultation. After completion, the questionnaire was dropped in the box inside the consultation room.
An anonymous questionnaire was used as a tool to collect data from the participants. The questions were divided in 10 sections, mainly containing information about age, language frequently used, sex, gender, level of education, MOD ownership and perceptions about SMS mHealth interventions. The questionnaire was available in IsiZulu and English. The questionnaire had been piloted at KEH as part of the Passages project.
Statistical analysis
Results were reported as means for continuous variables and as frequencies and percentages for categorical variables. Chi-square tests for categorical data and Student t-tests for continuous data were used to compare the difference in covariates between the rural and urban clinic sites.
A chi-square test was also used to assess phone ownership and mobile health technology feasibility by level of education. If more than 25% of the cells had expected counts less than five, a Fisher's exact test was run in place of the chi-square test. This is necessary because having small expected counts violates an assumption of the chi-square test. Analysis was performed using SAS 9.4.
Ethical considerations
Approval for this study was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (BREC Number BE480-17), the KZN Department of Health (KZ_201801_031) and the two institutions.
Results
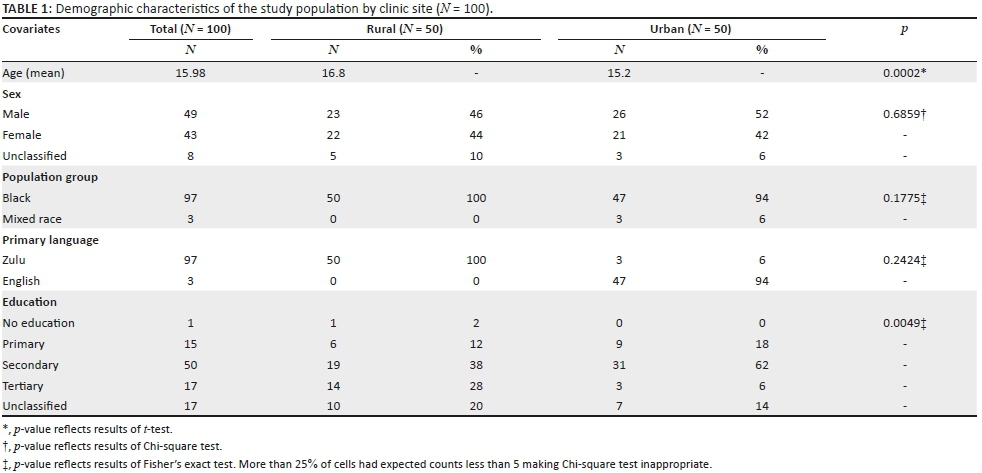
The key demographics of this survey from both rural and urban areas are depicted in Table 1. The mean age was 15 years (range 13-19 years). There was an almost equal distribution between males and females as per the study design. The majority of the population in this sample was black Africans and the preferred language of communication was IsiZulu. There were significant differences between the participants in the urban and rural clinics with regard to age and level of education.
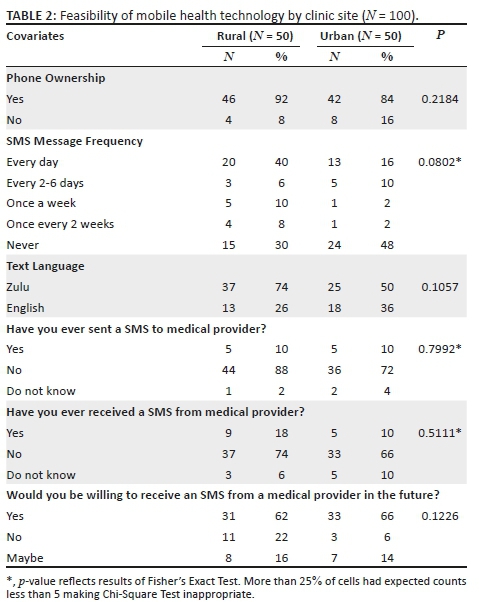
Access to an MOD was high as shown in Table 2, with 88% of adolescents surveyed having access to an MOD. There was no statistical difference in MOD ownership between rural and urban sites (92% vs. 84%, p = 0.2). The MOD ownership was almost the same between males and females (88% vs. 83% p = 0.19). There was a high frequency of SMS messages use in the rural site as compared to urban (40% vs. 26%, p = 0.08). Despite high MOD ownership, 48% of participants in the urban site had never sent an SMS text message. The majority of the study population at both sites had not sent or received any form of text message from a medical provider; however, adolescents at both the rural and urban sites were willing to use mobile technology to access healthcare (Table 2).
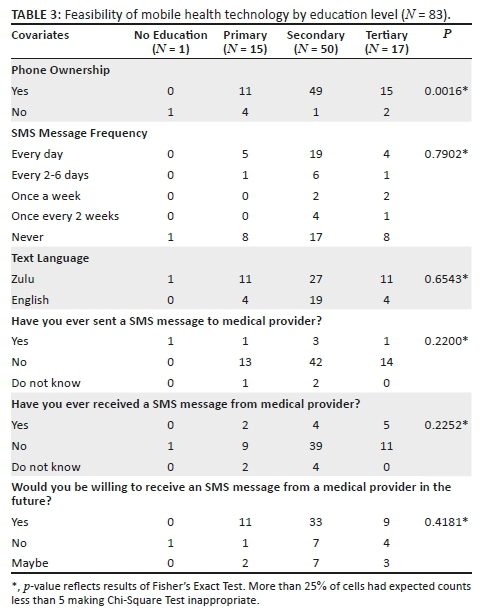
Feasibility of mHealth interventions was stratified by participant level of education (Table 3). Fifty per cent of the study population was attending secondary school with a statistically significant increase in MOD ownership with higher level of education (p = 0.0016). Only 38% of participants reported that they use SMS every day; however, 34 % reported that they never sent an SMS text message. Use of mHealth was feasible particularly in adolescents who attend secondary school with high levels of MOD ownership and 67% willing to receive SMS regarding their health.
Discussion
In this exploratory pilot study evaluating the acceptability of text messaging support for adolescents in an urban and rural clinic, we found no significant difference in MOD ownership and acceptability of mHealth between the two sites. Participants in both sites had high MOD ownership, with more than 90% of adolescents in this cohort owning a MOD. There are similar trends in MOD ownership that have been noted in other studies from Africa. A study of MOD ownership among the youth population in Malawi, Ghana and South Africa showed that 88% of youth owned an MOD.26 Despite the high levels of MOD ownership, there is a possibility that adolescents share their MODs with other family members, which increased the risks of accidental disclosures of confidential information regarding their health status.16 Investing in improving SMS-based mHealth interventions that do not divulge patient information and protecting individual privacy is urgently needed.16,27 While there have been different mHealth interventions studied in adult populations in developing and developed countries, these findings support the exploration of mHealth in adolescents residing in both rural and urban KZN.
Telecommunication technologies are emerging as an important means of extending healthcare to patients with limited direct access to a healthcare facility, with a Cochrane review showing that there is growing interest in the use of cell phone technology.28 In this study, 65% of adolescents were willing to participate in a mHealth intervention. There are different communication tools that have been used for delivering mHealth, ranging from simple, for example SMS, to more complicated, for example interactive apps. Participants from both clinics found that communicating with a healthcare provider using SMS text messages was an acceptable tool. One of the major potential benefits of mHealth is in improving adherence and retention to care. A study conducted in a rural area of Kenya found that an SMS-based mHealth intervention was associated with 90% improvement in adherence over 48 weeks.29 Additional benefits include decreased need for regular follow-up appointments resulting in a positive financial effect for patients as most clinics are far from the community.18 Several studies have found a correlation between high usage of mHealth and improvement of adherence.22,30,31 The high MOD ownership and willingness to access mHealth at both sites indicate that there is a space for mHealth interventions among these communities.
The higher usage of SMS text messaging in the participants from the rural clinic compared to the urban clinic likely highlights the influence of different access to telecommunication technologies between the settings. The ready availability of Internet-based messaging (e.g. WhatsApp) in urban centres may account for the lower use of SMS text messaging. This finding highlights the need for the use of simple technologies that can be accessed by both urban and rural communities when designing mHealth interventions. Implementation of telecommunication technologies requires adequate infrastructure, sustained budget for operational costs and this will need involvement of public and private sector support for it to be sustainable.32
The frequency of preferred messages differs by country, with patients in developing countries preferring to receive messages once a week,20,29,30 compared to daily text messaging that was preferred by patients in some developed countries.33 This preference may be related to socio-economic status with adolescents in developing countries being more likely to share MODs and less frequent messages would decrease the chances of accidental disclosure. Other suggestions by youth to improve confidentiality of mHealth include the use of MODs with access codes to increase security.22 In addition, daily SMS might be intrusive, produce habituation and response fatigue.34 There is suggestion that a two-way text messaging may be better than a simple text message reminder. More evidence is warranted regarding the optimal frequency of messaging.35 The majority of adolescents attending school may have restriction placed on the use of MOD both at school and at home during the school terms; this is important for the timing of SMS.
While the frequency of messaging is high among adolescents, only 12% of adolescents use cell phones for health-related information26; this is lower than previously thought. A study conducted in Malawi, Ghana and South Africa showed that 29% use cell phone technology for health-related issues.26 The possible reasons that can be extrapolated for the low usage include that people struggle to differentiate between good and bad information from the Internet about health and the prohibitively high cost of using data.26 Text messaging and phone calls maybe unaffordable in certain very low resource settings.24 These challenges will need to be addressed to achieve adherence and retention. Our study indicates that mHealth interventions hold promise, as 65% of adolescents are willing to use cell phone technology for health-related information.
Providing healthcare-related messages in a language that the recipient is comfortable with is very important. There are differences in languages used at home between participants in the urban and rural clinic, highlighting the need for the language to be customised to accommodate different ethnic and linguistic groups.
The average age of the participants in this survey is 15 years, with the majority in secondary school. However, if mHealth interventions are to be implemented, then content of messages might need to be different to accommodate different age groups. These messages need to be individualised and free of abbreviations like HIV/AIDS to decrease risk of accidental disclosure.35
A limitation of this study was the small sample size, which limited the power of the study to detect smaller differences between the two populations. However, this analysis was aimed at exploring mHealth in rural and urban areas in KZN and provides a rationale for further research in this area. Bias may arise as caregivers consented for enrolment into this survey, which may influence the responses, but assent was obtained and those adolescents who refused participation were not included. Further participants may have shared information while waiting outside the consultation room, which can lead to contamination of the data.
Strategies like mHealth are in line with the Fourth Industrial Revolution, as technology has become the focus. With dwindling international funding for provision of ART globally, this is a key opportunity to use innovative technologies (such as mHealth) to support a sustainable ART programme especially in vulnerable groups.36 However, as many African countries struggle with poverty, high unemployment rate and weak economic growth, it will be challenging to channel resources for implementation of such projects.24
Conclusion
This study has demonstrated that adolescents in this study population were willing to use simple SMS technology to communicate their health status with the health system both in urban and rural areas. This demonstrates the acceptability of potential of mHealth interventions that might have positive impact in supporting adherence and retention in care. Further studies are required to identify the most effective types of messaging, cost-effectiveness and sustainability especially in developing countries. This will require partnership with the private sector cellular phone networks while tailoring the intervention to the needs and information required by adolescents.
Acknowledgements
The authors would like to thank Sister Sibongiseni Ngubelanga from Umbumbulu Clinic and Dr Chirjeev Kindra from KEH Philani Clinic for their assistance in collecting the questionnaires and the adolescents for their participation in the study.
Competing interests
The authors have declared that no competing interests exist.
Authors' contributions
M.A.C. did the literature review, summarised and interpreted data collection, and wrote the summary. M.A. assisted with corrections and did overall supervision of the project.
Funding
This research received no specific grant from any funding agency in the public, commercial or not for profit sectors.
Data availability statement
Data can be shared upon permission from the authors.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1. UNICEF. For Every Child, End AIDS: Seventh Stocktaking Report, 2016. Seventh Stocktaking Report 2016. 2016. [cited n.d.]. Available from: https://www.unicef.org/publications/index_93427.html [ Links ]
2. Slogrove AL, Mahy M, Armstrong A, Davies MA. Living and dying to be counted: What we know about the epidemiology of the global adolescent HIV epidemic. J Int AIDS Soc. 2017;20(Suppl 3):4-15. https://doi.org/10.7448/IAS.20.4.21520 [ Links ]
3. UNAIDS, AIDSinfo. UNAIDS 2019 estimates. 2019. [cited n.d.]. Available from: https://aidsinfo.unaids.org/ [ Links ]
4. Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90 An ambitious treatment target to help end the AIDS epidemic, 2014. [cited n.d.]. Available from: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf [ Links ]
5. Firdu N, Enquselassie F, Jerene D. HIV-infected adolescents have low adherence to antiretroviral therapy: A cross-sectional study in Addis Ababa, Ethiopia. Pan Afr Med J. 2017;27(80):1-11. https://doi.org/10.11604/pamj.2017.27.80.8544 [ Links ]
6. Arrivé E, Dicko F, Amghar H, et al. HIV status disclosure and retention in care in HIV-infected adolescents on antiretroviral therapy (ART) in West Africa. PLoS One. 2012;7(3):1-8. https://doi.org/10.1371/journal.pone.0033690 [ Links ]
7. Koech E, Teasdale CA, Wang C, et al. Characteristics and outcomes of HIV-infected youth and young adolescents enrolled in HIV care in Kenya. AIDS. 2016;28(18):2729-2738. https://doi.org/10.1097/QAD.0000000000000473 [ Links ]
8. Adejumo OA, Malee KM, Ryscavage P, Hunter SJ, Taiwo BO. Contemporary issues on the epidemiology and antiretroviral adherence of HIV-infected adolescents in sub-Saharan Africa: A narrative review. J Int AIDS Soc. 2015;18(1):20049. https://doi.org/10.7448/IAS.18.1.20049 [ Links ]
9. Ridgeway K, Dulli LS, Murray KR, et al. Interventions to improve antiretroviral therapy adherence among adolescents in low- and middle-income countries: A systematic review of the literature. PLoS One. 2018;13(1):e0189770. https://doi.org/10.1371/journal.pone.0189770 [ Links ]
10. Mark D, Armstrong A, Andrade C, et al. HIV treatment and care services for adolescents: A situational analysis of 218 facilities in 23 sub-Saharan African countries. J Int AIDS Soc. 2017;20(3):25-33. https://doi.org/10.7448/IAS.20.4.21591 [ Links ]
11. Evans D, Menezes C, Mahomed K, et al. Treatment outcomes of HIV-Infected adolescents attending public-sector HIV clinics across Gauteng and Mpumalanga, South Africa. AIDS Res Hum Retroviruses. 2013;29(6):892-900. https://doi.org/10.1089/aid.2012.0215 [ Links ]
12. Harries AD, Zachariah R, Lawn SD, Rosen S. strategies to improve patient retention on antiretroviral therapy in sub-Saharan Africa. Trop Med Int Heal. 2010;15(SUPPL. 1):70-75. https://doi.org/10.1111/j.1365-3156.2010.02506.x [ Links ]
13. Porteus MH. Use of a Comprehensive HIV care cascade for evaluating HIV program erformance: Findings from 4 sub-Saharan African countries. J Acquir Immune Defic Syndr. 2016;1(1):23-30. https://doi.org/10.1007/s40778-014-0003-z [ Links ]
14. Zanoni BC, Sibaya T, Cairns C, Lammert S, Haberer E. Higher retention and viral suppression with adolescent-focused HIV clinic in South Africa. PLoS One. 2017;12(12):1-12. https://doi.org/10.1371/journal.pone.0190260 [ Links ]
15. Cluver L, Pantelic M, Toska E, Orkin M, Casale M, Bungane N. Stacking the odds for adolescent survival : Health service factors associated with full retention in care and adherence amongst adolescents living with HIV in South Africa. J Int AIDS Soc. 2018;21(9):1-8. https://doi.org/10.1002/jia2.25176 [ Links ]
16. Haberer JE, Kiwanuka J, Nansera D, Wilson IB, Bangsberg DR. Challenges in using mobile phones for collection of antiretroviral therapy adherence data in a resource-limited setting. AIDS Behav. 2010;14(6):1294-1301. https://doi.org/10.1007/s10461-010-9720-1 [ Links ]
17. Whiteley L, Brown L, Lally M, Heck N, Van den Berg JJ. A mobile gaming Intervention to increase adherence to antiretroviral treatment for youth living with HIV: Development guided by the information, motivation, and behavioral skills model. JMIR Mhealth Uhealth. 2018;6(4):e96. https://doi.org/10.2196/mhealth.8155 [ Links ]
18. Spratt ES, Papa CE, Mueller M, et al. Using technology to improve adherence to HIV medications in transitional age youth: Research reviewed, methods tried, lessons learned. J Gen Med. 2017;1(1):1002. [ Links ]
19. Lester RT, Ritvo P, Mills EJ, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): A randomised trial. Lancet. 2010;376(9755):1838-1845. https://doi.org/10.1016/S0140-6736(10)61997-6 [ Links ]
20. Rana Y, Haberer J, Huang H, et al. Short message service (SMS)-based intervention to improve treatment adherence among HIV-positive youth in Uganda: Focus group findings. PLoS One. 2015;10(4):1-14. https://doi.org/10.1371/journal.pone.0125187 [ Links ]
21. Georgette N, Siedner MJ, Zanoni B, et al. The acceptibility and percieved usefulnes of weekly sms. AIDS Behav. 2017;20(11):2629-2638. https://doi.org/10.1007/s10461-016-1287-z [ Links ]
22. Saberi P, Siedle-Khan R, Sheon N, Lightfoot M. The use of mobile health applications among youth and young adults living with HIV: Focus group findings. AIDS Patient Care STDS. 2016;30(6):254-260. https://doi.org/10.1089/apc.2016.0044 [ Links ]
23. Nhavoto JA, Grönlund Å, Klein GO. Mobile health treatment support intervention for HIV and tuberculosis in Mozambique: Perspectives of patients and healthcare workers. PLoS One. 2017;12(4):1-13. https://doi.org/10.1371/journal.pone.0176051 [ Links ]
24. Kliner M, Knight A, Mamvura C, Wright J, Walley J. Using no-cost mobile phone reminders to improve attendance for HIV test results: A pilot study in rural Swaziland. Infect Dis Poverty. 2013;2(1):2-8. https://doi.org/10.1186/2049-9957-2-12 [ Links ]
25. Saberi P, Johnson MO. Technology-based self-care methods of improving antiretroviral adherence: A systematic review. PLoS One. 2011;6(11):e27533. https://doi.org/10.1371/journal.pone.0027533 [ Links ]
26. Hampshire K, Porter G, Owusu SA, et al. Informal m-health: How are young people using mobile phones to bridge healthcare gaps in Sub-Saharan Africa? Soc Sci Med. 2015;142:90-99. https://doi.org/10.1016/j.socscimed.2015.07.033 [ Links ]
27. Crankshaw T, Corless IB, Giddy J, Nicholas PK, Eichbaum Q, Butler LM. Exploring the patterns of use and the feasibility of using cellular phones for clinic appointment reminders and adherence messages in an antiretroviral treatment clinic, Durban, South Africa. AIDS Patient Care STDS. 2010;24(11):729-734. https://doi.org/10.1089/apc.2010.0146 [ Links ]
28. Horvath T, Azman H, Kennedy GE, Rutherford GW. Mobile phone text messaging for promoting adherence to antiretroviral therapy in patients with HIV infection. Cochrane Database Syst Rev. 2012;(3):CD009756. https://doi.org/10.1002/14651858.CD009756 [ Links ]
29. Pop-Eleches C, Thirumurthy H, Habyarimana JP, et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: A randomized controlled trial of text message reminders. AIDS. 2013;25(6):825-834. https://doi.org/10.1097/QAD.0b013e32834380c1 [ Links ]
30. Maduka O, Tobin-West CI. Adherence counseling and reminder text messages improve uptake of antiretroviral therapy in a tertiary hospital in Nigeria. Niger J Clin Pract. 2013;16(3):302-308. https://doi.org/10.4103/1119-3077.113451 [ Links ]
31. Kanters S, Park JJH, Chan K, et al. Interventions to improve adherence to antiretroviral therapy: A systematic review and network meta-analysis. Lancet HIV. 2017;4(1):e31-e40. https://doi.org/10.1016/S2352-3018(16)30206-5 [ Links ]
32. Avery M, Mills SJ, Stephan E. Real-time monitoring through the use of technology to enhance performances throughout HIV cascades. Curr Opin HIV AIDS. 2017;12(5):488-493. https://doi.org/10.1097/COH.0000000000000397 [ Links ]
33. Garofalo R, Kuhns LM, Hotton A, Johnson A, Muldoon A, Rice D. A randomized controlled trial of personalized text message reminders to promote medication adherence among HIV-positive adolescents and young adults. AIDS Behav. 2017;20(5):1049-1059. https://doi.org/10.1007/s10461-015-1192-x [ Links ]
34. Finitsis DJ, Pellowski JA, Johnson BT. Text message intervention designs to promote adherence to antiretroviral therapy (ART): A meta-analysis of randomized controlled trials. PLoS One. 2014;9(2):e88166. https://doi.org/10.1371/journal.pone.0088166 [ Links ]
35. Amankwaa I, Boateng D, Quansah DY, Akuoko CP, Evans C. Effectiveness of short message services and voice call interventions for antiretroviral therapy adherence and other outcomes: A systematic review and meta-analysis. PLoS One. 2018;13(9):1-20. https://doi.org/10.1371/journal.pone.0204091 [ Links ]
36. Mcgillen JB, Sharp A, Honermann B, Millett G, Collins C, Hallett TB. Consequences of a changing US strategy in the global HIV investment landscape. AIDS. 2017;31(18):F19-F23. https://doi.org/10.1097/QAD.0000000000001669 [ Links ]
 Correspondence:
Correspondence:
Mthokozisi Cele
mthokozisicele@rocketmail.com
Received: 31 Mar. 2019
Accepted: 16 July 2019
Published: 03 Oct. 2019


{kind=link}