










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of HIV Medicine
On-line version ISSN 2078-6751
Print version ISSN 1608-9693
South. Afr. j. HIV med. (Online) vol.16 n.1 Johannesburg 2015
http://dx.doi.org/10.4102/sajhivmed.v16i1.428
GUIDELINES
Southern African HIV Clinicians Society adult antiretroviral therapy guidelines: Update on when to initiate antiretroviral therapy
Graeme MeintjesI; John BlackII; Francesca ConradieIII; Sipho DlaminiIV; Gary MaartensV; Thandekile C. ManziniVI; Moeketsi MatheVII; Michelle MoorhouseVIII; Yunus MoosaIX; Jennifer NashX; Catherine OrrellXI; Francois VenterVIII; Douglas WilsonXII
IDepartment of Medicine and Institute of Infectious Disease and Molecular Medicine, University of Cape Town, South Africa
IIDepartment of Medicine, Livingstone Hospital, South Africa
IIIRight to Care and Clinical HIV Research Unit, University of the Witwatersrand, South Africa
IVDivision of Infectious Diseases & HIV Medicine, Department of Medicine, University of Cape Town, South Africa
VDivision of Clinical Pharmacology, University of Cape Town, South Africa
VIDepartment of Infectious Diseases, King Edward VIII Hospital, University of KwaZulu-Natal, South Africa
VIIPrivate practice, Vereeniging, South Africa
VIIIWits Reproductive Health and HIV Institute, Johannesburg, South Africa
IXDepartment of Infectious Diseases, University of KwaZulu-Natal, South Africa
XAmathole District Clinical Specialist Team, Eastern Cape, South Africa
XIDesmond Tutu HIV Foundation, University of Cape Town, South Africa
XIIDepartment of Internal Medicine, Edendale Hospital, University of KwaZulu-Natal, South Africa
ABSTRACT
The most recent version of the Southern African HIV Clinicians Society's adult antiretroviral therapy (ART) guidelines was published in December 2014. In the 27 August 2015 edition of the New England Journal of Medicine, two seminal randomised controlled trials that addressed the optimal timing of ART in HIV-infected patients with high CD4 counts were published: Strategic timing of antiretroviral therapy (START) and TEMPRANO ANRS 12136 (Early antiretroviral treatment and/or early isoniazid prophylaxis against tuberculosis in HIV-infected adults). The findings of these two trials were consistent: there was significant individual clinical benefit from starting ART immediately in patients with CD4 counts higher than 500 cells/μL rather than deferring until a certain lower CD4 threshold or clinical indication was met. The findings add to prior evidence showing that ART reduces the risk of onward HIV transmission. Therefore, early ART initiation has the public health benefits of potentially reducing both HIV incidence and morbidity. Given this new and important evidence, the Society took the decision to provide a specific update on the section of the adult ART guidelines relating to when ART should be initiated.
The 2014 guidelines
In the 2014 version of the Southern African HIV Clinicians Society's adult antiretroviral therapy guidelines, antiretroviral therapy (ART) was recommended for certain clinical indications (including WHO stage 3 and 4 disease, and other significant morbidities), for HIV-infected partners in serodiscordant relationships, and in all patients with a CD4 < 350 cells/μL. Further, these guidelines advised that if patients had two CD4 counts between 350 and 500 cells/μL, ART should be started if the patient was ready and motivated to start ART. However, in these guidelines it was advised that if a patient's CD4 count was > 500 cells/μL and the patient did not qualify on clinical grounds, then ART should be deferred. The rationale was that insufficient evidence existed to advise a 'test-and-treat' approach to HIV at that time, and it was stated that we awaited the results of the TEMPRANO and Strategic timing of antiretroviral therapy (START) trials.1
For patients diagnosed during acute HIV seroconversion, initiation of standard first-line ART was advised, provided that adherence requirements were met. For such patients, it was advised that ART should be continued for at least 3 years, but consideration should be given to continuing lifelong ART.
The strategic timing of antiretroviral therapy and TEMPRANO trials
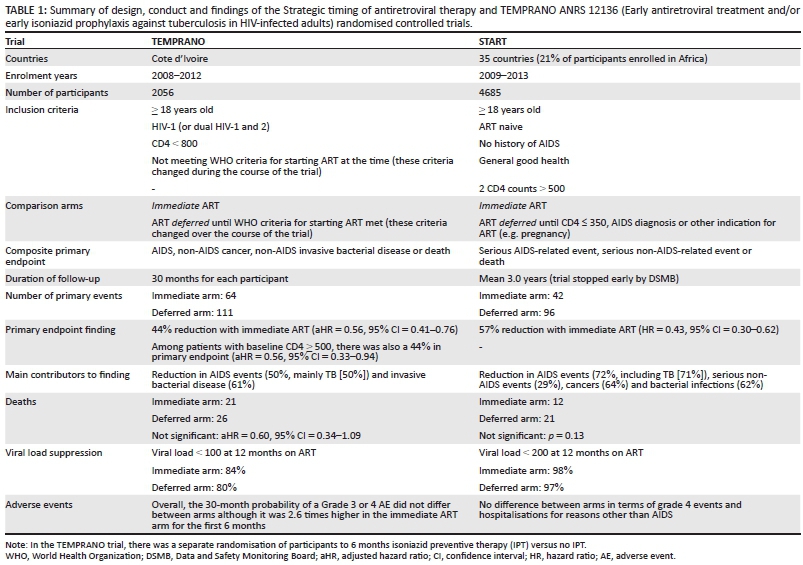
Both the START and TEMPRANO trials enrolled patients with high CD4 counts (in START all participants had a study entry CD4 count > 500 cells/μL; in TEMPRANO, 41% had an entry CD4 count > 500 cells/μL). A summary of the trials is presented in Table 1. Both trials involved randomisation to one of two strategies: immediate ART initiation, or to defer ART until the participant was eligible on the basis of CD4 count or clinical criteria. Patients were followed for about 3 years in each trial, and the primary endpoint was a composite endpoint that included AIDS events, serious non-AIDS events and death, with minor differences in specific aspects of the endpoint definition between the two trials.
Both trials demonstrated a statistically significant, approximate halving of events contributing to the primary endpoint when ART was started immediately. In TEMPRANO, this benefit was largely attributable to reductions in incident TB and invasive bacterial diseases (particularly pneumonia). In START, the benefit was related to a decrease in AIDS-related events (including TB) and serious non-AIDS events (including cancer). The relative reduction in the rate of primary endpoint events was greater in START (57% reduction compared with 44%). However, the absolute benefit of immediate ART was greater in the TEMPRANO trial (conducted in Cote d'Ivoire) than in the START trial (which was conducted in countries across the world), because the event rate in the control arms (mainly from TB and invasive bacterial infections) was higher in the TEMPRANO trial, reflecting the high co-infection risks that exist for individuals living with HIV infection in Africa, even with higher CD4 counts. No significant difference in mortality was observed between the study arms in either trial.2,3
There are two main concerns about ART initiation with CD4 counts > 500 cells/μL. Firstly, the risk of adverse events could outweigh clinical benefits. Secondly, adherence could be lower in asymptomatic patients. In both trials, immediate ART did not increase the risk of adverse events overall, nor did patients who started immediately have a higher risk of adherence problems, at least in the short term, as evidenced by the high proportion of patients achieving HIV viral suppression seen in the immediate arms in both trials (Table 1).
The HPTN052 trial4 previously demonstrated that ART prevented onward transmission of HIV within serodiscordant couples, which suggested that ART at HIV diagnosis for all may be an important strategy to help prevent the growth of the HIV epidemic at a public health level. However, such an approach would be difficult to justify if there were no individual benefit and potential individual harm. What these two trials have demonstrated is that there is indeed individual clinical benefit with no signal of harm during ~3 years of follow-up, providing significant additional support for the 'test-and-treat' strategy.
These were well-conducted randomised controlled trials with good participant retention and assured drug supply, and the vast majority of participants were on tenofovir/emtricitabine/efavirenz regimens in both trials. In less motivated patients, or in the context of inconsistent drug supply or different first-line ART regimens, these results should be treated with caution, as the modest benefits seen with early treatment may not be realised. In particular, if tenofovir (or abacavir) is unavailable and zidovudine or stavudine needs to be used in place, then the substantial side-effect profile of these drugs and effect on patients' quality of life may outweigh the benefit of early ART.
Isoniazid preventive therapy in patients on antiretroviral therapy
The TEMPRANO trial involved a separate randomisation of participants to 6 months of isoniazid preventive therapy (IPT) started one month after study entry, versus no IPT. The addition of IPT to ART provided added protection against active TB disease, even in these patients with relatively high CD4 counts. This finding was similar to those of a placebo-controlled trial conducted in Khayelitsha, South Africa, where 12 months of IPT prescribed to patients on ART reduced TB incidence by 37%.5 Our December 2014 guidelines1 recommended IPT for all patients on ART provided that there was no contra-indication to isoniazid, and active TB was not suspected based on symptom screen. Guidelines on duration of IPT based on tuberculin skin test results were provided. Given that southern Africa has the highest incidence rates of HIV-associated TB in the world, IPT as a TB-preventive strategy implemented within ART clinics should be prioritised.
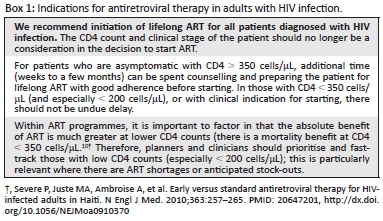
Updated recommendations of SA HIV Clinicians Society regarding antiretroviral therapy initiation
Our updated recommendations are shown in Box 1. It is important to note that these are the guidelines of the SA HIV Clinicians Society, and clinicians working within national public sector ART programmes should continue to follow the guidelines that pertain to their programme. Whilst National Departments of Health are very likely to consider a change in ART initiation policy in the near future based on these study findings, such a change will need to factor the financial cost, adequate planning of drug supply and health service capacity. Sustaining funding for ART programmes in resource-limited countries is a huge challenge currently.6
Specific patient groups
For patients who are diagnosed with HIV during acute seroconversion, we continue to advise that those patients be counselled and initiated on ART. This should preferably be expedited ART initiation as there is evidence that this may limit the size of the HIV reservoir.7 However, we no longer recommend that these patients should have ART interrupted after 3 years. Rather, once ART is started in this situation, this should be lifelong ART, and this should be discussed with the patient. Additional counselling once the patient is established on ART may be required for patients who start ART in this acute situation because there is limited time for extensive counselling pre-ART and there is often considerable psychological distress around this time.
A minority of patients (< 1%) have very effective immune control of HIV infection and are able to control HIV viraemia at undetectable levels in the absence of ART - termed 'elite controllers'. An argument could be made that such individuals do not require ART if their CD4 count is > 500 cells/μL. The START and TEMPRANO trials did not specifically address the question of whether early ART was beneficial in such patients, and it is highly unlikely that any sufficiently powered randomised controlled trial could ever be conducted focused on these individuals. In the absence of such data, we rely on indirect evidence. Firstly, elite controllers still have evidence of chronic immune activation and inflammation that may drive non-infectious morbidities.8 Secondly, elite controllers have been shown to have a higher rate of hospitalisation than patients who are virologically controlled by ART.9 For these reasons, we do advise starting ART in elite controllers too, with the same caveats regarding the patient being prepared. One important consideration in such patients is that careful attention should be paid to confirming the diagnosis of HIV before starting ART. They are typically patients who have a positive HIV ELISA test, undetectable HIV viral load, CD4 count in the normal range and are clinically well. The possibility of a false positive HIV ELISA test should be excluded either by performing a qualitative HIV DNA PCR assay or a Western blot assay. If the patient at some point previously had a detectable HIV viral load, this would also serve as confirmation. Such patients should be discussed with a laboratory virologist to assist with confirmation of HIV infection status.
In patients with active TB or opportunistic infections, the 2014 guidelines included guidance as to when to initiate ART in relation to treatment of the TB or opportunistic infection. This guidance remains unchanged.
We recommend ART initiation without delay in all HIV-infected women who are pregnant or breastfeeding, irrespective of CD4 cell count, to prevent mother-to-child transmission of HIV infection. We advise that such ART should be continued lifelong and not stopped after the pregnancy or weaning.
In children and adolescents, advice from the Society's Child and Adolescent Guidelines Committee is that the 'test-and-treat' approach is supported in principle for all ages. However, there is an absence of data for the 5-15-year-old age group. Adherence issues for adolescents in particular and the lack of a simplified first-line regimen make 'test-and-treat' for 5-15- year-olds complicated. Please refer to national Department of Health guidelines for further advice regarding children and adolescents.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article. G.M. is a consultant for Aid for AIDS and received speaker fees from Sanofi Aventis. F.C. have received support from Janssen Pharmaceutica, Abbvie, GSK, Merck, Aspen, Sanofi Aventis and Mylan to attend conference, and received honoraria for speaking and attendance at advisory board.
Authors' contributions
G.M. (University of Cape Town) is the first author, and undertook preparation of the first draft of the manuscript. The remaining authors were involved in the discussions that guided the development of the manuscript and also reviewed the first draft. All authors contributed to the review of the data informing the new recommendations, and to the development of the recommendations.
References
1. Meintjes G, Black J, Conradie F, et al. Adult antiretroviral therapy guidelines 2014. S Afr J HIV Med. 2014;15:121-143. http://dx.doi.org/10.7196/sajhivmed.1130 [ Links ]
2. INSIGHT START Study Group, Lundgren JD, Babiker AG, et al. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373:795-807. PMID: 26192873, http://dx.doi.org/10.1056/NEJMoa1506816 [ Links ]
3. TEMPRANO ANRS 12136 Study Group, Danel C, Moh R, et al. A trial of early antiretrovirals and isoniazid preventive therapy in Africa. N Engl J Med. 2015;373:808-822. PMID: 26193126, http://dx.doi.org/10.1056/NEJMoa1507198 [ Links ]
4. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365:493-505. PMID: 21767103, http://dx.doi.org/10.1056/NEJMoa1105243 [ Links ]
5. Rangaka MX, Wilkinson RJ, Boulle A, et al. Isoniazid plus antiretroviral therapy to prevent tuberculosis: A randomised double-blind, placebo-controlled trial. Lancet. 2014;384:682-690. PMID: 24835842, http://dx.doi.org/10.1016/S0140-6736(14)60162-8 [ Links ]
6. Abdool Karim SS. Overcoming impediments to global implementation of early antiretroviral therapy. N Engl J Med. 2015;373:875-876. PMID: 26193047, http://dx.doi.org/10.1056/NEJMe1508527 [ Links ]
7. O'Brien M, Markowitz M. Should we treat acute HIV infection? Curr HIV/AIDS Rep. 2012;9:101-110. PMID: 22415472, http://dx.doi.org/10.1007/s11904-012-0113-0 [ Links ]
8. Krishnan S, Wilson EM, Sheikh V, et al. Evidence for innate immune system activation in HIV type 1-infected elite controllers. J Infect Dis. 2014;209:931-939. PMID: 24185941, http://dx.doi.org/10.1093/infdis/jit581 [ Links ]
9. Crowell TA, Gebo KA, Blankson JN, et al. Hospitalisation rates and reasons among HIV elite controllers and persons with medically controlled HIV infection. J Infect Dis. 2015;211:1692-1702. PMID: 25512624, http://dx.doi.org/10.1093/infdis/jiu809 [ Links ]
10. Severe P, Juste MA, Ambroise A, et al. Early versus standard antiretroviral therapy for HIV-infected adults in Haiti. N Engl J Med. 2010;363:257-265. PMID: 20647201, http://dx.doi.org/10.1056/NEJMoa0910370 [ Links ]
 Correspondence:
Correspondence:
Graeme Meintjes
Private Bag X3, Rondebosch 7701
South Africa
Email: graemein@mweb.co.za
Note: This guideline was compiled by the Southern African HIV Clinicians Society.
Disclaimer: Specific recommendations provided here are intended only as a guide to clinical management, based on expert consensus and best current evidence. Treatment decisions for patients should be made by their responsible clinicians, with due consideration for individual circumstances. The most current version of this document should always be consulted.


{kind=link}