










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.16 no.1 Pretoria mar. 2024
http://dx.doi.org/10.7196/AJHPE.2024.v16i1.327
RESEARCH
Education about planetary health and sustainable healthcare: A national Delphi panel assessment of its integration into health professions education in South Africa
J H IrlamI; S ReidII; H-A RotherIII
IMSc (Climate Change and Development) MPhil (Epidemiology); Primary Health Care Directorate, Department of Family, Community and Emergency Care, Faculty of Health Sciences, University of Cape Town, South Africa
IIMB ChB, PhD; Primary Health Care Directorate, Department of Family, Community and Emergency Care, Faculty of Health Sciences, University of Cape Town, South Africa
IIIPhD (Environmental Sociology); Division of Environmental Health, School of Public Health, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Education about planetary health (PH) and sustainable healthcare (SH), or education for sustainable healthcare (ESH), enables health professionals to help protect public health and healthcare from climate change and environmental degradation. The Association for Medical Education in Europe Consensus (AMEE Consensus) Statement on Planetary Health and Education for Sustainable Healthcare has proposed a set of ESH learning objectives, activities and assessments for adaptation to different health professions education (HPE) contexts. The national audit phase of a mixed methods study in South Africa (SA) found that awareness of ESH and its curriculum development is emerging. The African Medical Education Directives for Specialists (AfriMEDS) is a competency framework for undergraduate medical students in SA that defines key competencies and enabling competencies related to seven roles of a health professional.
OBJECTIVES. To recruit a national Delphi panel of health professions educators to assess the applicability of the AMEE Consensus learning objectives, activities and assessments to HPE in SA; to elicit panellists' perceptions of the main barriers and opportunities for ESH in faculties; and to compare learning objectives recommended by AMEE and the panel for key competencies and enabling competencies within the AfriMEDS framework.
METHODS. Nine educators from three different disciplines and six national faculties of health sciences participated in two rounds of a Delphi process and in follow-up discussions. In round 1, they rated the AMEE Consensus learning objectives, activities and assessments, and proposed additional ones. In round 2, they rated the score-ranked AMEE lists, as well as relevant additions from round 1. All panellists participated in further discussions regarding applicability, and highlighted the potential barriers and opportunities for integrating ESH into their faculties. The lead author then matched the panel's learning objectives with enabling competencies related to all seven health professional roles described by AfriMEDS.
RESULTS. All panellists recognised the importance of ESH in SA and the need for eco-ethical leadership by health professionals. All 13 AMEE Consensus learning objectives, as well as three additional objectives from the panel, were matched most frequently with AfriMEDS-enabling competencies related to the roles of leader and manager (n=9), communicator (n=8) and healthcare practitioner (n=7). Panellists highly ranked learning activities and assessments that are authentic, multiprofessional and require systems thinking. They perceived the lack of capable educators and curriculum overload to be the main barriers to integration of ESH, as well as the need for strong leaders, disciplinary champions and trained educators.
CONCLUSIONS. Situating the selected learning objectives within the AfriMEDS competency framework provides a good basis for developing aligned learning activities and assessments of ESH. Strong leadership, capable educators and multidisciplinary collaboration are important enablers of integrating ESH into HPE in SA.
Planetary health (PH) is 'a solutions-oriented, transdisciplinary field and social movement focused on analyzing and addressing the impacts of human disruptions to Earth's natural systems on human health and all life on Earth'.[1] This definition encompasses the many ways, including climate change, pollution, biodiversity shifts, land use changes and resource scarcity, in which the environment can affect health, such as changing the epidemiology of vector-borne diseases, mental illness and heat and air pollution-related mortality.[2]
Education regarding PH and sustainable healthcare (SH), or education for sustainable healthcare (ESH), has emerged internationally to develop the competencies of health professionals to help protect public health from planetary climate change and environmental degradation and to help build health systems that are more sustainable and resilient to climate disruption.[3-5] The Declaration on Planetary Health of the Association of Faculties of Medicine of Canada (AFMC) recognises that faculties and academic health institutions have a social and environmental accountability mandate and therefore calls on them 'to take immediate action to both halt the negative impact of their activities on the planet's natural systems, and to institute adaptive and regenerative measures, including through advocacy'.[6]
The concept of eco-ethical leadership in health professions education (HPE) has emerged as an integrated values-based approach that prioritises social justice, collaboration and advocacy towards environmental, organisational and community sustainability and regeneration.[7] Systems thinking is a key feature of eco-ethical leadership that requires cognitive complexity to understand the world from a dynamic systems perspective.[8] Eco-ethical leadership is urgently needed and highly relevant for health professionals and educators to respond to the growing climate crisis and its impact on health and healthcare systems.[5]
The Association for Medical Education in Europe Consensus (AMEE Consensus) Statement on Planetary Health and Education for Sustainable Healthcare, 2021, proposed learning objectives, activities and assessments of ESH for adaptation to different educational contexts, although representation from low- and middle-income countries was limited.[9] Experience from many countries has shown that the integration of PH and SH content is generally inhibited by curriculum overload, poor alignment and assessment, and lack of capacity among educators to teach and assess these topics.[10]
In late 2021, the first phase of a three-phase mixed methods study of ESH in South Africa (SA), including a national audit of health professions curricula, was undertaken via the Education for Sustainable Healthcare Special Interest Group (ESH SIG) of the Southern African Association of Health Educationalists (SAAHE). It found that ESH awareness and curriculum development are emerging, although with a limited variety of learning activities and forms of assessment. The authors recommended further work in national curriculum development of ESH, enabled by strong institutional leadership and staff and student involvement.[11] The ESH SIG subsequently hosted a regional webinar on planetary health education in African primary healthcare curricula and issued a joint call for the integration of PH and SH into health professions curricula in Africa.[12]
The lead author (JHI) led a team of medical students at the University of Cape Town (UCT) in 2022 to complete a baseline planetary health report card (PHRC) assessment of the integration of PH and SH into the curricula and campus operations and services of the Faculty of Health Sciences (FHS), UCT, as part of a global student-led initiative.[13] The PHRC global summary report calls for curricular content on PH and SH to be formalised by developing testable learning objectives related to clinical knowledge and skills, and for such content to be integrated longitudinally as a cross-curricular theme.[2] The graduate profiles for most of the FHS, UCT, health professional programmes have been adapted from a competency framework for undergraduate students in medical programmes in SA.[14,15] This framework is known as the African Medical Education Directives for Specialists (AfriMEDS) and was adapted from the Canadian Medical Education Directives for Specialists (CanMEDS) Physician Competency Framework[16] by the predecessor to the Health Professions Council of South Africa (HPCSA), in collaboration with training institutions and faculty deans. CanMEDS was developed to enhance social accountability in medicine and has been widely used in the accreditation of medical education programmes.[14] The core competencies in the AfriMEDS framework include 26 key competencies, which are further divided into 122 enabling competencies. The enabling competencies are related to seven roles of a health professional, i.e. healthcare practitioner, communicator, collaborator, leader and manager, health advocate, scholar, and professional.[15]
The Delphi technique is a well-used method in HPE to achieve group consensus on developing curriculum components, assessment items, educational resources and defining competencies.[17] The aim of this second phase of the mixed methods study was to identify ESH learning objectives and related curriculum content applicable to HPE curricula in SA. The objectives were to undertake an expert Delphi panel assessment of the applicability of the AMEE Consensus learning objectives, activities and assessments to HPE in SA; elicit the panellists' perceptions of the main barriers and opportunities for integrating ESH into health sciences faculties; and compare learning objectives recommended by AMEE and the panel with key competencies and enabling competencies within the AfriMEDS framework.
Methods
Ten SA HP educators were invited to join two rounds of a Delphi panel through the ESH SIG in April 2022. Nine accepted, and one did not accept owing to personal time constraints. Eligible participants were identified by the national audit phase;[11] they had some expertise in ESH curriculum development and had indicated interest in promoting ESH in SA. Representation was sought from different disciplines and faculties to enhance the national applicability of the findings. Participants were recruited by email and their informed consent was obtained.
In round 1, panellists rated lists of learning objectives, activities and forms of assessment of PH and SH from the AMEE Consensus that they deemed applicable to HPE in SA. The panellists were invited to make additions to the lists. In round 2, they rated the score-ranked AMEE Consensus lists, as well as their additions from round 1. A 5-point scale was used for rating the learning objectives (1 = definitely exclude; 2 = exclude; 3 = neutral/not sure; 4 = include with reservations; 5 = definitely include) and a 3-point scale for the learning activities and assessments (1 = no; 2 = maybe; 3 = yes). The AMEE Consensus lists were ranked on their cumulative scores after both rounds, whereas round 1 additions were ranked on their round 2 scores only. Using a 3-point scale in round 1 only (1 = not at all; 2 = maybe; 3 = definitely), panellists also rated common barriers to integrating PH and SH into curricula, which were derived from the literature.[10] The ranked results were tabulated in Excel (Microsoft Corp., USA) by JHI and shared with the panellists via email before and via screen-sharing during online Teams (Microsoft Corp., USA) meetings in May 2022. The agenda of the meetings was to review and discuss round 1 and 2 results, and to explore panellists' perceptions of the main barriers and opportunities for integrating ESH into their respective faculties and national curricula.
The AMEE Consensus learning objectives, as well as all additions from the panel, were coded, categorised and tabulated in Excel by JHI, according to the three learning domains from the AMEE Consensus, i.e. knowledge (K); knowledge and skills (KS); and knowledge, values, attitudes and agency (KVA). They were further coded and categorised by six sub-domains created by JHI from his assessment of the purpose of each objective: understanding the environmental determinants of health (K1); understanding the environmental sustainability of healthcare (K2); enhancing the environmental sustainability of healthcare (KS1); critiquing environmental sustainability policy (KS2); advocating for planetary health and sustainable development (KS3); and eco-ethical leadership in healthcare (KVA1). A final column in the Excel table displayed one of the seven health professional roles in the AfriMEDS framework that appeared to JHI to be most closely related to each learning objective.
JHI then removed learning objectives added by the panel that looked as though they were essentially similar to those of the AMEE Consensus, compared the remaining learning objectives with all of the key competencies and enabling competencies for each health professional role within the AfriMEDS framework, and performed a best match, using Excel to tabulate the results. A narrative feedback report with accompanying tables (included in and supplementary to this article), as well as a narrated PowerPoint (Microsoft Corp., USA) presentation of the key findings and conclusions, was shared with all 9 panellists for review and comment within a month of the follow-up discussions.
Ethical approval
Ethical approval was obtained in August 2021 from the Human Research Ethics Committee, FHS, UCT (ref. no. HREC 358/2021).
Results
All 9 panellists participated in both Delphi rounds and in one of three follow-up meetings, as it proved impossible to schedule one meeting with all in attendance. They represented three different professions, i.e. family medicine (n=4), environmental health (n=3) and nursing (n=2); and six different faculties of health sciences: Stellenbosch University (SU; n=3), University of KwaZulu-Natal (UKZN; n=2), and one panellist each from Durban University of Technology (DUT), University of Cape Town (UCT), University of the Western Cape (UWC) and University of the Witwatersrand (Wits) (Supplementary Table 1. List of Delphi panellists: https://www.samedical.org/file/2122). Comment on the feedback report was received from only one of the panellists, who did not challenge the validity of the analysis.
Importance of ESH
All panellists highly rated the importance of educating health professional students about PH and SH. Their reasons included the dependence of human health and wellbeing on a healthy planet; that climate change poses the greatest risk to health and healthcare globally; and that many SA undergraduates lack knowledge and interest regarding planetary health and environmental sustainability. They recognised that health professionals, as trusted members of society, can exercise considerable agency in patient care and policy development based on a sound understanding of the concepts and principles of PH and SH.
One panellist observed that more awareness is needed of how consumption patterns and healthcare practices degrade the health of the planet and humankind: 'I think that all humans require greater awareness of the risks of how our consumption patterns threaten the survival of our planet. Health professional students are no exception. There are also certain "professional" practices that negatively impact human health. Our apartheid-era health facilities require massive overhaul together with other health infrastructure to become more environmentally friendly. In their professional roles, students will need to grapple with this and ultimately provide leadership' (W01).
Learning objectives
Thirty-three learning objectives (13 from the AMEE Consensus and 20 additions by the Delphi panel) were coded and categorised by the three AMEE learning domains (K/KS/KVA), six sub-domains (K1/K2/KS1/KS2/KS3/ KVA1) and the related AfriMEDS health professional roles (Supplementary Table 2. Learning objectives by learning domains, sub-domains and related AfriMEDS health professional roles: https://www.samedical.org/file/2123). Seventeen learning objectives added by the panel that JHI considered similar to the AMEE Consensus objectives were removed. The following three were retained on the grounds of their applicability to the SA context: K2.3 (understand how the health system contributes to the problem of planetary degradation); KS2.2 (critique current environmental protections in the SA constitution and other legislation in terms of how they affect other health rights of your patients, families and communities); and KVA1.2 (understand what is expected of health professionals in their personal and professional behaviour). Hence, 16 objectives, 13 from the AMEE Consensus and three added by the panel, were compared and matched with key competencies and enabling competencies for each health professional role within the AfriMEDS framework.
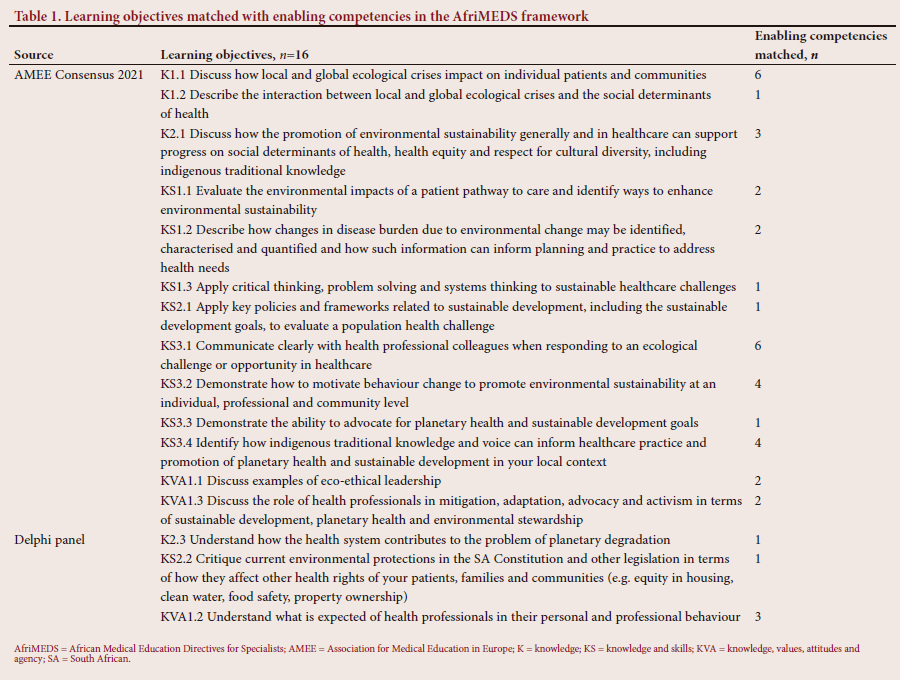
The results of this comparative exercise ranged from one match for enabling competencies for objectives K1.2, K2.3, KS1.3, KS2.1, KS2.2 and KS3.3 to six matches for objectives K1.1 and KS3.1 (Table 1). The AMEE Consensus learning objective KVA1.1 (discuss examples of eco-ethical leadership) was matched with two enabling competencies in AfriMEDS, while the additional objective from the panel (KVA1.2 (understand what is expected of health professionals in their personal and professional behaviour)) was matched with three enabling competencies. Overall, the learning objectives were matched most often with enabling competencies related to the AfriMEDS health professional roles of leader and manager (n=9), communicator (n=8) and healthcare practitioner (n=7), and least often with competencies related to the roles of scholar (n=3) and professional (n=3) (Supplementary Table 3. Core graduate competencies and roles related to ESH learning objectives: https://www.samedical.org/file/2124).
In follow-up discussions, one panellist proposed that educators should agree on core principles to guide future education and training before setting ESH-related learning objectives because of the diversity of HPE in SA. The panellist believed that such principles would help to motivate the relevance of PH and SH in overloaded curricula, especially for those who have not 'bought in' to its importance. Another panellist thought that some of the objectives were quite conceptual and hence difficult to assess, and that the key teaching topics to assess are the following: environmental impacts on health; building more resilient facilities and health services; and reducing the environmental harm caused by the health sector. A third panellist emphasised that 'learning objectives are the key to unpacking the content, learning opportunities, and assessment within a given programme' (S01).
Learning activities
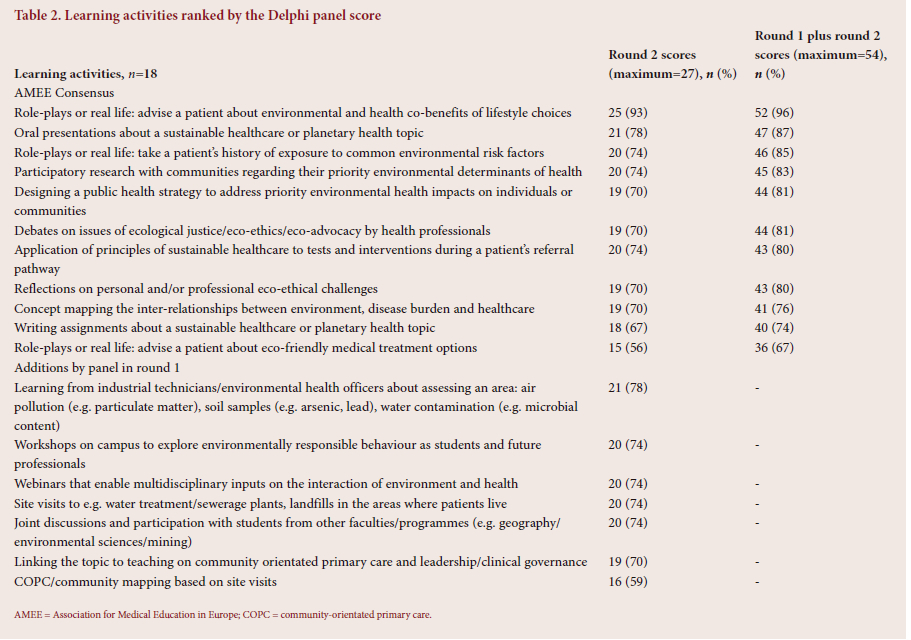
Eleven learning activities from the AMEE Consensus were scored in both Delphi rounds, and seven round 1 additions by the panel were scored in round 2 only (Table 2). The top-ranked AMEE Consensus learning activity was role-plays or real-life advice to a patient about environmental and health co-benefits of lifestyle choices (52 out of a maximum score of 54; 96%). Reflections on personal and/or professional eco-ethical challenges were ranked with a score of 80%. Of the round 1 addition made by the panel, learning from industrial technicians/environmental health officers about assessing an area was ranked highest (21 out of a maximum score of 27; 78%). This ranking was closely followed by suggestions for campus workshops on environmentally responsible behaviour, webinars on the interaction of the environment and health, site visits, and interactions with students from other faculties or programmes (score of 20 (74%) for all).
Assessments
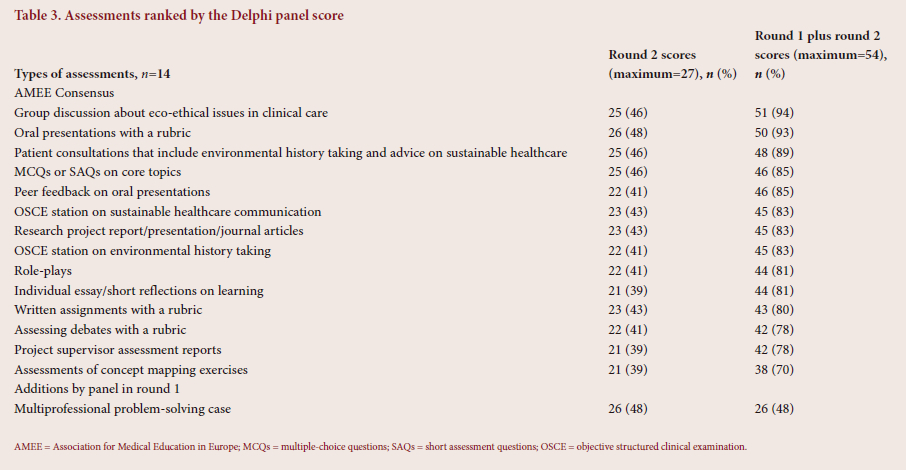
Fourteen types of assessment from the AMEE Consensus were scored by panellists in both rounds and one addition only by the panel (multiprofessional problem-solving case) was scored in round 2 (Table 3). The top-ranked assessments were group discussions regarding eco-ethical issues in clinical care (51 out of a maximum score of 54; 94%); oral presentations with a rubric (n=50; 93%); and patient consultations that include environmental history taking and advice on sustainable healthcare (n=48; 89%).
Barriers to curriculum integration
Eight barriers to integrating PH and SH into curricula were scored in round 1 only. The top-ranked barriers were: lack of educators who are knowledgeable about sustainable healthcare (26 out of a maximum score of 27; 96%); lack of understanding about the relevance of sustainability teaching to healthcare (n=25; 93%); too many competing educational interests (n=24; 89%); lack of faculty leadership on sustainability (n=23; 85%); and lack of time/space in the teaching curricula (n=23; 85%) (Supplementary Table 4. Barriers to curriculum integration of ESH: https://www.samedical.org/file/2125).
A panellist and specialist in environmental health practice reported few problems in integrating environmental health into their faculty programmes, but acknowledged challenges in 'scaffolding' it longitudinally: 'The curriculum mapping exercise is critical, but it has to go hand in hand with face-to-face discussion about how to integrate it' (D01). Another panellist proposed layering ESH learning objectives over the course of the spiral undergraduate curriculum and into postgraduate studies. A lecturer in PH described a 'conflict of interest' with colleagues who teach environmental health, who saw no need for climate change and PH to be taught as separate modules. A panellist from the nursing sciences reported that environmental and climate change issues had been included in their teaching on advocacy and health services management in recent years, despite the absence of these issues from the core nursing curriculum. She reported that the AMEE Consensus had been a helpful guide and described their challenges in attempting interactive teaching of large classes of students. Another nursing professional reported that monitoring in their faculty had shown that their curriculum had not been implemented correctly at times, which was exacerbated by a high turnover of staff and by 'threads' of SH often being insufficiently explicit and inconsistently championed. The lack of educator interest and expertise in teaching and assessing PH and SH was a prevalent theme of the discussions. Higher-degree pathways in ESH in SA faculties were therefore proposed to develop a cohort of capable educators in the field.
Several panellists noted that many students have prior awareness and knowledge of climate change from their schooling, yet deficient understanding of the connections between climate and health, and how individual lifestyle choices impact the environment. One panellist observed that 'It's almost as if there's kind of this immunity, I think, with climate change and these other issues, gender-based violence or addiction or a whole range of issues. It's almost as if you learn about this in a detached way, as if it doesn't impact you and your family. And you know that's what professionalism means, is that you sort of begin to distance yourself in a way from your own roots and your own trauma and your own pain and your own reality' (W01). This panellist therefore proposed educating students about using their positionality as future health professionals effectively to leverage political will for meaningful change within their campuses, health institutions and communities, and to hold their leaders accountable.
Discussion
Eco-ethical leadership
Eco-ethical leadership is given high priority in the results section of this study. This is apparent in the frequent matching of related learning objectives with enabling competencies in the AfriMEDS framework, and the high scoring by the panel for eco-ethical learning activities and assessments suited to the SA context. The panel's recognition of the potential agency of health professionals as trusted members of society, is consistent with growing international consensus in the face of increasing climate and environmental risks to health.[9] The need for eco-ethical leadership has been recognised by the AMEE Consensus,[9] while others have explored the implications for health professional leaders at the health systems and organisational levels[7] and the ethics of sustainability for responsible professionals.[18] The PHRC global report, e.g. the AMEE Consensus, strongly recommends that curricula should acknowledge indigenous knowledge and value systems as an essential part of the response to the planetary crisis.[2,9] Hence, eco-ethical leaders should 'demonstrate socio-cultural and ecological values that embody inclusivity and social and ecological justice'.[7] The national audit of ESH in SA found minimal coverage of this topic,[11] and the PHRC at FHS, UCT, found few examples of such leadership.[2]
Learning objectives, activities and assessments
The AMEE Consensus calls for the constructive alignment of ESH learning outcomes, objectives, activities and assessments, and for their adaptation to local settings, using a range of approaches that are relevant and authentic and incorporate interprofessional learning, where possible.[9] The PHRC global summary report recommends the development of testable learning objectives with students, as well as educating and incentivising faculty members to integrate PH and SH themes and topics into existing teaching and learning activities across curricula.[2]
Comparing and matching the ESH learning objectives to key competencies and enabling competencies of AfriMEDS have demonstrated their potential applicability within a widely adopted competency framework in HPE curricula in SA. The exercise helped to identify which learning objectives from the panel were sufficiently locally relevant to add to the AMEE Consensus objectives. It was found that the ESH learning objectives appear to be most relevant to the AfriMEDS health professional roles of leadership and management and communication. The complex and interconnected causal pathways associated with the planetary determinants of health and sustainability in healthcare systems, and hence their potential solutions, emphasise that future curricula should address the AMEE learning objective KS1.3 (apply critical thinking, problem solving and systems thinking to sustainable healthcare challenges). The need for systems thinking has also been identified as a central characteristic of eco-ethical leadership,[7] and is implicit in the recommendation of the PHRC summary report to situate teaching in a global interconnected context of human health.[2] Curricula should therefore also include related learning activities and assessments, such as skills in identifying the inter-relationships between environment, disease and healthcare. The panel's high scoring of concept-mapping activities and assessments supports this assertion.
The panel's support for authentic learning activities and assessments that are consistent with the AMEE Consensus[9] was apparent in their high scoring of role-played or real-patient history taking of environmental exposures, as well as advice regarding the environmental and health co-benefits of lifestyle choices, such as home food gardening and active commuting as pedestrians or cyclists.[19] The panel also added interprofessional and multiprofessional activities such as community health assessments and site visits that extend authentic learning beyond the clinical encounter to communities. Cross-disciplinary webinars, campus workshops, and multiprofessional problem solving were also suggested, which align with global efforts to integrate PH and SH topics into clinical disciplines to demonstrate their relevance to diagnostic history taking, health promotion and therapeutic interventions.[19-21] This is especially important for developing student and graduate agency, as students have reported often feeling unprepared to answer patients' questions about climate change and environmental sustainability.[13,22]
Three learning objectives from the panel (K2.3, KS2.2 and KVA1.2) were added to those of the AMEE Consensus owing to their contextual relevance in SA. Although these additonal objectives were not specifically reflected in the ranked learning activites and assessments, they could guide topics for student assignments, debates, workshops and site visits. The PHRC provides many helpful global examples of faculties that have introduced environmental justice opportunities into their curricula, re°search, student leadership and community engagement.[2] One panellist noted that health professional leadership is needed in transforming SA health facilities and infrastructure to become more environmentally friendly. The work of the Global Green and Healthy Hospitals (GGHH) network in SA is relevant, as it follows a global action agenda for mitigating the considerable 'carbon footprint' of the health system, which includes local champions, skills development and helpful case studies.[23,24] Hence, there are growing opportunities for authentic, relevant and interprofessional learning activities and assessments that require collaborative eco-ethical leadership.
Barriers and opportunities for ESH
Most panellists strongly agreed with almost all of the barriers that were summarised from the literature. In common with faculties worldwide, HPE curricula are perceived to be overloaded, yet they are often characterised by disciplinary 'silos'; thus, opportunities for cross-disciplinary integration are missed.[10,21] Strong leaders, capable educators and champions for integrated approaches were seen as necessary by many panellists, especially to challenge 'hidden' curricula, or the unofficial norms, values and beliefs that are transferred by an institution's culture.[25,26] Such a culture may devalue content not deemed relevant to what is considered to be 'core clinical' competencies of a health professional, yet such values and opinions can be altered.[10,27]
The suggestions made by the panel to overcome these barriers are generally consistent with recommendations from the PHRC and others for cross-curricular/multi- and interdisciplinary integration of ESH across the years, which require educational leaders to consult with key stakeholders in disciplines other than their own.[13,18] The Declaration on Planetary Health[6] and the PHRC initiative[13] are excellent opportunities for institutional reflection and global collaboration for achieving greater social and environmental accountability. For academic health institutions that strive to lead planetary health research, policy and advocacy for real-world solutions, key stakeholders could include those in engineering, agriculture, architecture, urban planning, communications and the behavioural sciences.[6]
Study limitations
Although the Delphi panel was small, it was reasonably representative of the limited community of ESH practice in SA, founded by the prior national audit. Panellists were from three health professions at six faculties, whereas nine types of health professions from 15 faculties submitted audit responses, and most professions in both phases were medical or environmental health practitioners.[11] Despite the inability to schedule only one follow-up meeting with all panellists, the smaller groups facilitated greater participation in the limited time available. Furthermore, the lead author alone selected learning objectives from the panel to add to those of the AMEE Consensus, and also compared them with the AfriMEDS framework of health professional roles and enabling competencies. Although a feedback report with the detailed tables, as well as a narrated PowerPoint (Microsoft Corp., USA) presentation of the key results, was shared with the panel soon after the follow-up meetings, no panellists interrogated the outcomes of this process. Further engagement with the study results, preferably face-to-face to facilitate deeper discussion, is therefore warranted to improve their validity and applicability to other settings.
Conclusions
The Delphi process was a useful and efficient means of assessing national expert perceptions of the applicability of the learning objectives, activities and assessments suggested by the AMEE Consensus, an international milestone for ESH development, and of the main barriers and opportunities for ESH in SA. The situation of ESH learning objectives with enabling competencies within the national AfriMEDS framework has provided a good basis for further refinement as a prerequisite for aligned learning activities and assessments. Key barriers to ESH in health sciences faculties that are consistent with global experience are the lack of capable educators and overloaded curricula. The study recommends integrating ESH as a cross-curricular theme in interprofessional curricula, empowering leaders and champions of ESH within faculties and health professional programmes, and training a national cohort of capable educators. Further work is required in developing national ESH accreditation standards and indicators of progress that are generally consistent with global standards. These recommendations may also apply to other settings where ESH development is still in its infancy, or which have adopted the AfriMEDS competency framework.
Declaration. None.
Acknowledgements. Members of the Delphi panel (Supplementary Table 1. List of Delphi panellists: https://www.samedical.org/file/2122).
Author contributions. All authors complied with the International Committee of Medical Journal Editors' rules of authorship. JHI conceptualised and designed the study, collected and analysed the data, and prepared all drafts of the article. H-AR and SR commented on the study protocol, provided conceptual inputs, and reviewed and edited the article.
Funding. None.
Conflicts of interest. None.
References
1. Planetary Health Alliance. Planetary health. https://www.planetaryhealthalliance.org/planetary-health (accessed 23 June 2023). [ Links ]
2. Planetary Health Leadership Team. Planetary health report card 2022 - 2023. Summary report: An international health student initiative. https://phreportcard.org/wp-content/uploads/2023/04/PHRC-2023-Med-Summary-Report-FINAL.pdf (accessed 23 June 2023). [ Links ]
3. Walpole SC, Mortimer F, Inman A, et al. Exploring emerging learning needs: A UK-wide consultation on environmental sustainability learning objectives for medical education. Int J Med Educ 2015;6:191-200. https://doi.org/10.5116/ijme.5643.62cd [ Links ]
4. Macpherson CC, Wynia M. Should health professionals speak up to reduce the health risks of climate change; AMA J Ethics 2017;19(12):1202-1210. https://doi.org/10.1001/journalofethics.2017.19.12.msoc1-1712 [ Links ]
5. Berrang-Ford L, Sietsma AJ, Callaghan M, et al. Systematic mapping of global research on climate and health: A machine learning review. Lancet Planet Health 2021;5(8):e514-e525. [ Links ]
6. Association of Faculties of Medicine of Canada (AFMC) Declaration on Planetary Health Development Committee. Declaration on planetary health. https://www.afmc.ca/initiatives/planetaryhealthdeclaration/ (accessed 22 June 2023). [ Links ]
7. McKimm J, McLean M. Rethinking health professions' education leadership: Developing 'eco-ethical' leaders for a more sustainable world and future. Med Teach 2020;42(8):855-860. https://doi.org/10.1080/0142159x.2020.1748877 [ Links ]
8. Guarana CL, Hernandez M. Building sense out of situational complexity: The role of ambivalence in creating functional leadership processes. Organ Psychol Rev 2015;5(1):50-73. [ Links ]
9. Shaw E, Walpole S, McLean M, et al. AMEE Consensus statement: Planetary health and education for sustainable healthcare. Med Teach 2021;43(3):272-286. https://doi.org/10.1080/0142159X.2020.1860207 [ Links ]
10. Tun S, Wellbery C, Teherani A. Faculty development and partnership with students to integrate sustainable healthcare into health professions education. Med Teach 2020;42(10):1112-1118. https://doi.org/10.1080/0142159x.2020.1796950 [ Links ]
11. Irlam J, Dreyer A, Filies G, et al. Education about planetary health and sustainable healthcare: A national audit of health professions education curricula in South Africa. Afr J Health Professions Educ 2023;15(4):e326. https://doi.org/10.7196/AJHPE.2023.v15i4.326 [ Links ]
12. Irlam JH, Scheerens C, Mash B. Planetary health and environmental sustainability in African health professions education. Afr J Prim Health Care Fam Med 2023;15(1). https://doi.org/10.4102/phcfm.v15i1.3925 [ Links ]
13. Hampshire K, Islam N, Kisse B, et al. The planetary health report card: A student-led initiative to inspire planetary health in medical schools. Lancet Planet Health 2022;6(5):e449-e454. https://doi.org/10.1016/S2542-5196(22)00045-6 [ Links ]
14. Naidu C, Reid S, Burch V. Development of a CanMEDS-based instrument for evaluating medical students' perceptions of the key competencies of a socially accountable healthcare practitioner. Perspect Med Educ 2020;9(2):98-106. https://doi.org/10.1007/s40037-020-00564-6 [ Links ]
15. Health Professions Council of South Africa. Core competencies for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa. 2014. https://www.hpcsa-blogs.co.za/wp-content/uploads/2017/04/MDB-Core-Competencies-ENGLISH-FINAL-2014.pdf (accessed 19 October 2023). [ Links ]
16. Frank JR, Danoff D. The CanMEDS initiative: Implementing an outcomes-based framework of physician competencies. Med Teach 2007;29(7):642-647. https://doi.org/10.1080/01421590701746983 [ Links ]
17. Humphrey-Murto S, Varpio L, Gonsalves C, et al. Using consensus group methods such as Delphi and nominal group in medical education research. Med Teach 2017;39(1):14-19. https://doi.org/10.1080/0142159X.2017.1245856 [ Links ]
18. Walpole S, Vyas A, Maxwell J, et al. Building an environmentally accountable medical curriculum through international collaboration. Med Teach 2017;39(10):1040-1050. https://doi.org/10.1080/0142159X.2017.1342031 [ Links ]
19. Tun S, Martin T. Education for sustainable healthcare - a curriculum for the UK. 2022. https://www.medschools.ac.uk/media/2949/education-for-sustainable-healthcare_a-curriculum-for-the-uk_20220506.pdf (accessed 19 October 2023). [ Links ]
20. Chase H, Hampshire K, Tun S. Improving the medical curriculum on planetary health and sustainable healthcare. BMJ 2022;376:0209. https://doi.org/10.1136/bmj.0209 [ Links ]
21. Tun S. Fulfilling a new obligation: Teaching and learning of sustainable healthcare in the medical education curriculum. Med Teach 2019;41(10):1168-1177. https://doi.org/10.1080/0142159X.2019.1623870 [ Links ]
22. Irlam J, Razzak Z, Parker Q, et al. Student knowledge and perceptions of climate change and environmental sustainability at the Faculty of Health Sciences, University of Cape Town, South Africa. Afr J Health Professions Educ 2023;15(1):2-6. https://doi.org/10.7196/AJHPE.2023.v15i1.1659 [ Links ]
23. Karliner J, Guenther R. Global green and healthy hospitals agenda: A comprehensive environmental health agenda for hospitals and health systems around the world. Health Care Without Harm 2011. [ Links ]
24. GroundWork. The Global Green and Healthy Hospitals (GGHH) network in Africa. https://groundwork.org.za/global-green-healthy-hospitals/ (accessed 22 June 2023). [ Links ]
25. Alsubaie MA. Hidden curriculum as one of current issue of curriculum. J Educ Prac 2015;6(33):125-128. [ Links ]
26. UNESCO International Bureau of Education. Hidden curriculum. https://www.ibe.unesco.org//en/glossary-curriculum-terminology/h/hidden-curriculum (accessed 22 June 2023). [ Links ]
27. Prasad V, Thistlethwaite W, Dale W. Effect of clinical vignettes on senior medical students' opinions of climate change. South Med J 2011;104(6):401-404. https://doi.org/10.1097/SMJ.0b013e31821a841d [ Links ]
 Correspondence:
Correspondence:
J H Irlam
james.irlam@uct.ac.za
Accepted 25 August 2023.


{kind=link}
{kind=link}
{kind=link}