










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.16 n.1 Pretoria Mar. 2024
http://dx.doi.org/10.7196/AJHPE.2024.v16i1.847
RESEARCH
Navigating the troubled waters of higher education – a phenomenological study on the needs and challenges of first-year clinical associate students in South Africa
C NelI; J E WolvaardtII; P H du ToitIII
IBPhysT, MPhysT; School of Health Systems and Public Health, Faculty of Health Sciences, University of Pretoria, South Africa
IIBCur, MPH, PGCHE, PhD; School of Health Systems and Public Health, Faculty of Health Sciences, University of Pretoria, South Africa
IIIBA, BEd, MEd, PhD; Department of Humanities Education, Division: Higher Education, Faculty of Humanities, University of Pretoria, South Africa
ABSTRACT
BACKGROUND. Clinical associates (ClinAs) are educated in decentralised learning platforms where they gain skills and a concrete understanding of the fundamental challenges of healthcare in remote and poverty-stricken districts of South Africa. Due to the decentralised nature of the programme, these students seldom have access to 'on-campus' academic and psychosocial support. A peer mentorship programme has proved useful in this regard in other settings.
OBJECTIVE. To explore the unique academic and psychosocial challenges and needs of first-year clinical associate (ClinA) students and describe the views of the research participants on the perceived enablers and constraints of a ClinA peer mentorship programme.
METHODS. A phenomenological research design was used. The population included ClinA students and academic members of staff. Five appreciative inquiry interviews and two focus group discussions were conducted.
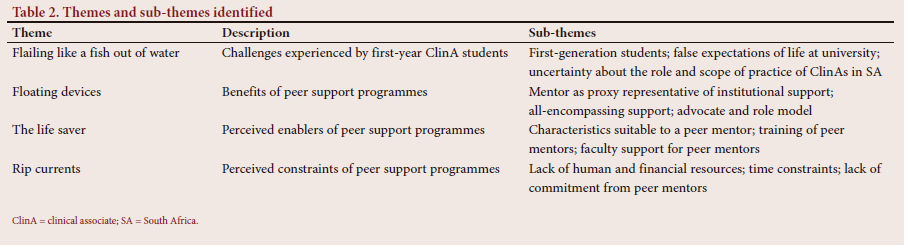
RESULTS. Four themes were identified: (i) flailing like a fish out of water (challenges experienced by ClinA students); (ii) floating devices (benefits of peer support programmes); (iii) the life saver (perceived enablers of peer support programmes); and (iv) rip currents (perceived constraints of peer support programmes).
CONCLUSION. Unique challenges identified were: (i) the teaching and learning strategy implemented by the facilitator of the programme; (ii) the decentralised learning platforms; and (iii) the absence of institutional support at clinical learning centres. All participants agreed that peer mentor support is beneficial and essential for ClinA students, but that the peer mentor programme needs to be bespoke to address the limited access to academic and psychosocial on-campus support and the profile of the students, who are of rural origin and first-generation students.
The Bachelor of Clinical Medical Practice (BCMP) programme was introduced to increase the number of skilled mid-level healthcare workers in underserved rural areas of South Africa (SA). The shortage of healthcare workers in SA negatively impacts on patient care and increases the workload on other healthcare workers. Students in the BCMP programme are known as clinical associate (ClinA) students, who proceed to work as clinical associates (ClinAs) under the supervision and mentorship of a medical doctor after their graduation. ClinAs are educated in healthcare facilities that are predominantly situated in rural areas. These decentralised learning platforms provide them with opportunities to gain skills and a concrete understanding of the fundamental challenges of healthcare in remote and poverty-stricken districts of SA.[1,2]
ClinAs work as part of the healthcare team in district hospitals and clinics in the public sector, as well as with medical doctors in the private sector. Their scope of practice includes assessing and managing medical emergencies, performing routine procedures and managing patients in different medical wards, including maternal health, paediatrics and mental health. They also assist in theatre and perform routine surgical procedures under supervision.[3,4]
The BCMP programme is a 3-year degree course offered at three universities in SA, i.e. Walter Sisulu University (WSU), the University of the Witwatersrand (Wits) and the University of Pretoria (UP). A national curriculum framework was developed to ensure standardisation but allows for local differences at each university. Students are either recruited by provincial departments of health with a special emphasis on identifying students from rural and disadvantaged areas or students can apply through open enrolment.[1] When the programme was rolled out initially, the majority of students received bursaries from the provincial departments of health, but these bursaries were reduced drastically over the years. Currently, the majority of ClinA students have to rely on the National Student Financial Aid Scheme (NSFAS)[5] or private funding. The BCMP programme is unique, as students learn almost exclusively in clinical environments away from campus.[6]
At UP, the BCMP programme is characterised by ClinA students remaining on campus during the first semester of their first year for subjects such as anatomy and physiology and other foundation modules. From the second semester of the first year until the end of their final year, ClinA students spend most of their time at their allocated clinical learning centre (CLC). A CLC is a selected provincial, tertiary or district hospital or clinic where students are placed to do their clinical work-integrated learning (WIL), supervised/facilitated by healthcare staff at the specific CLC. ClinA students spend ~60% of their 3-year programme at a CLC. The reason for this is a strong emphasis on problem-based learning and the need for early and prolonged clinical exposure to allow them to integrate theory in 'real life' clinical settings. Traditional support structure services offered by the university, e.g. student advisors, clinical psychologists and tutors, are not available at all the remote CLCs, making it difficult for students to access such services, if needed.
Doherty et al.[7] report that one of the positive lessons learnt from the introduction of the BCMP programme in SA was that the recruitment strategy (students from rural and disadvantaged areas) is important for retention. The authors suggest that specific support mechanisms, e.g. mentorship, should be developed for these students to ensure a smooth transition from school to university and to improve retention in higher education.[7] Studies show that students in higher education face numerous challenges including high levels of stress, with resultant negative effects on their physical health and psychological wellbeing.[8] These factors can lead to poor academic performance.[9] In addition, many ClinA students are first-generation students and are recruited from rural areas. Being a first-generation student at university means that the student is the first person in their immediate family to attend university and/or complete a degree in higher education.[10]
In higher education, peer mentors are usually senior students who are trained to be mentors for junior students, and their role depends on the objectives of the mentorship programme. In a systematic review performed on the outcomes of peer mentoring programmes for first-year students, the following benefits were identified and included for the mentees: social (integrating into the new environment), professional (learnt medical etiquette), academic (study tips and 'tricks of the trade') and emotional (motivation and stress reduction). Peer mentors reported the development of personal and professional attitudes as benefits.[11]
The objectives of mentorship programmes for first-year students at higher education institutions are to provide social, emotional and academic support to assist with the transition from school to higher education and to improve retention of students.[9,11,12] Several higher education institutions in SA have implemented, or are starting to implement, mentorship programmes for their first-year students as part of a general student support strategy. It is difficult to show whether these mentorship programmes have an influence on students' academic success, as there is limited research published in an SA context.[13] The major part of the SA literature on mentoring programmes explores a single aspect, such as mentoring in a problem-based learning curriculum;[14] mentors' reflections on the student support programme;[15] and mentees' feedback on student-mentor attributes.[16] Little is known about peer mentorship programmes for students - such as ClinA students - who learn and work on decentralised platforms.
Objectives
The objectives of this research were: (i) to determine and describe the unique challenges and needs (academic, socioeconomic and emotional) of first-year ClinA students; and (ii) to describe the views and experiences of these students and academic members of staff involved in peer support on the perceived enablers and constraints of a ClinA peer mentorship programme.
Methods
A phenomenological research design was used. The purpose of phenomenological studies is to understand and describe a specific phenomenon in-depth and uncover the 'essence of participants' lived experiences of the phenomenon'.[17] Phenomenology is based on a constructivist philosophy. With social constructivism[18] as a theoretical framework, we B the researchers B believe that people actively contribute to the construction of their own knowledge through interaction with others in authentic situations, learning from studying the literature and from our own practice.[19]
When using a phenomenological research approach, a fairly homogenous group of participants is required.[20] Participants should have experience with the same phenomenon;[17] therefore, the study population included all ClinA students, academic staff members involved with BCMP programmes, heads of department (HODs), BCMP programme managers and clinical facilitators at all three abovementioned universities.
Non-random, purposive sampling was used, as student participants were selected based on their roles (experience in being a mentor, mentee or tutor) and members of staff were selected based on their experiences as facilitators engaging with students.[21] Key stakeholders were selected in accordance with their involvement in overseeing, managing and/or policy development regarding student wellbeing (academic, psychosocial and/or physical).
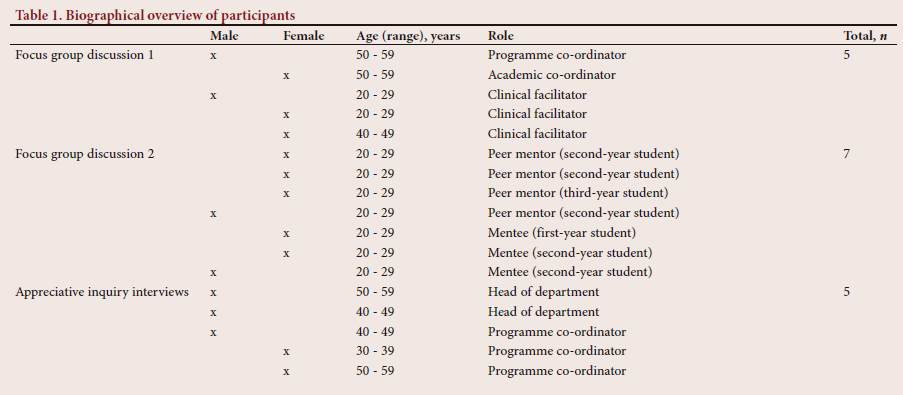
Two qualitative methods were used, i.e. appreciative inquiry interviews[22] and focus group discussions. A total of five online appreciative inquiry interviews were conducted via the Google Teams platform, with 3 programme co-ordinators and 2 HODs. Two virtual focus group discussions were held -also using Google Teams - one with staff members and one with students.
Five interviews were conducted with staff members from all three universities where the BCMP programme is offered (2 from UP; 1 from WSU and 2 from Wits). The focus group discussion for staff members of UP comprised 5 participants, including different role players - the academic co-ordinator, the programme manager and clinical facilitators. The focus group for the students comprised 7 participants, including representatives from all year groups, peer mentors and mentees.
The process of qualitative data analysis involves several steps, including data preparation, coding, categorisation, synthesis and interpretation.[23,24] In the first step, i.e. data preparation, researchers organise the data and remove any irrelevant or duplicate information. The appreciative inquiry interviews and focus group discussions were transcribed. The researcher read through the transcripts several times to get a sense of the data to become familiar with the content of the transcripts and to identify key topics B noting any interesting or noteworthy aspects. In the second step, i.e. data coding, the researcher assigned descriptive labels or codes to segments of data that represent the meaning or content of that segment. The coding was done on ATLAS.ti.8 (ATLAS.ti, Germany) and codes were created inductively (emerging from the data). The codes were then grouped into categories in the data categorisation step. In the fourth step, i.e. data synthesis, the categories were compared and contrasted to identify patterns and themes that emerged from the data. Finally, in the interpretation step, the researcher developed a narrative that described the findings of the study. These themes were based on patterns in the data that were identified through the categorisation and coding processes and are discussed in detail under the Results heading.
The study was approved by the Health Sciences Research Ethics Committee, University of Pretoria (ref. no. 657/2020). For the interviews and focus group discussions, participation was voluntary, and information was treated confidentially. Names of all interviewees and focus group participants were anonymised and allocated a participant code, i.e. academic staff members - AC; peer mentors - MR; and mentees - ME. All participants received information on the research project and completed an informed consent form before participation.
Results
A total of 17 people participated in the focus group discussions and interviews - a biographical overview can be seen in Table 1.
Four themes were identified: (i) flailing like a fish out of water (challenges experienced by BCMP students); (ii) floating devices (benefits of peer support programmes); (iii) the life safer (perceived enablers of peer support programmes); and (iv) rip currents (perceived constraints of peer support programmes).
Table 2 provides a summary of themes and categories. Each of these themes is discussed in detail below.
(i)Flailing like a fish out of water (challenges experienced by first-year ClinA students)
At least 50% of first-year ClinA students are first-generation students (HERI UP Readiness Survey 2021/2022) and arrive at university without an understanding of what higher education in general entails. One of the participating members of staff commented: 'If you're coming from a disadvantaged background, you are taking on [represent] the whole village.' [AC1]. Bursary holders are seen as 'breadwinners' [AC1] and are expected to send money home, although bursaries seldom exceed direct expenses. As a result, 'The majority of our students struggle, and they end up having to drop out. If you really were to dig deep, they're dropping out because of financial issues.' [AC2]
First-year ClinA students experience mismatched expectations of 'going to university' - they arrive on campus and then discover that they spend the majority of their time off campus. A participating member of staff reflected on her own first-year experience: for me, you know the idea I'm going to the university and I'm going to be studying at the university. And then you get there you are told no, after 6 months you have to go to a CLC.' [AC3] The first-year experience at university was considered more familiar: 'I really expected to have those contact sessions all the time and going to classes and I enjoyed that environment - being in the lecture halls, surrounded by classmates, because it's reminiscent of high school being back in a classroom with people.' [MR3]
The role and scope of practice of ClinAs in SA are unfortunately still not well known and many healthcare professionals have a misconception about the BCMP programme. These misconceptions lead to the students feeling 'like being side-lined or marginalised', [AC1] adding to their feelings of self-doubt and not fitting in. They are 'often being misunderstood, intentionally and unintentionally and often seen as second-rate citizens by the medical profession'. [AC5] ClinA students arrive, wet behind the ears, having to sink or swim through 'the big gap from a rural high school coming to university' [AC6] and find themselves in need of a floating device.
(ii) Floating devices (benefits of peer support programmes)
One source of support, in the absence of institutional support at the CLCs, was the peer mentors: 'Sometimes you really feel like you're thrown in the deep end and a mentor is that person to help you swim to land. I appreciate that.' [ME10]
According to participating academic members of staff, the peer support programme is all-encompassing; it not only entails academic support, but also assists first-year students to adapt to university life, helping them to find their feet and adapting to a new environment. In the words of a participating mentee: '. it becomes beneficial to the mentee, providing them with much support ... from clinical, academic and personal support.' [ME5]
A peer support programme is a 'powerful tool specifically for our students who are taken into a distant CLC' [AC3] - to have someone to guide them through the muddy waters of the curriculum, where they are expected to act as self-directed learners. A participating mentee confirmed that the '... peer relationship is very important because that is what got me through my first year . the fact that we are now in other provinces, we rely on each another (sic) more than we will ever rely on the facilitators'. [ME1]
Because ClinA students are exposed to clinical departments and 'real patients' early in their first semester, the peer mentor can be a valuable advocate and role model for this new profession. The importance of these roles was accentuated by one of the participating members of staff, who is also a clinical facilitator at a CLC: 'A peer mentor can sometimes be of a better benefit when looking at finding a voice for you. Because in most instances where you have a mentor, that mentor is most likely to advocate for the students and how things are supposed to be.' [AC3] As ClinAs still face challenges with recognition by healthcare institutions and colleagues, it can be a 'source of hope and inspiration' [AC3] for junior students to have someone who is part of the BCMP programme to mentor and guide them to achieve success.
Peer mentors are senior students who went through the same experiences: 'You are being advised by someone who has already walked your path.' [ME11] The mentees mentioned how the peer mentors assisted them in adapting to the 'new' academic environment and educational strategies -'the mentor helps you with a lot of things like general life at university to specific learning programme. It makes it easier for you to understand the program and how things are done and especially the [objective structured clinical examination] OSCE and head to toe for me.' [ME2] The peer mentors could encourage them, because they had insight into the challenges the mentees experienced - 'they make it feel that it's normal to have breakdowns'. [MR5] Participating mentees reported that learning from a peer made it easier to ask questions. Mentees might feel quite intimidated by the lecturers or facilitators, but asking a peer, who is friendly and approachable and shares the same experience, is less daunting: 'For me peer relationship is very important because that is what got me through my first year, because she had more knowledge and more experience than I did. And because I was very afraid of asking the educators, because sometimes you ask them, and they say it's a learning need and you need to back and learn about it - I wouldn't be free to ask them.' [ME1]
(iii) The life saver (perceived enablers of peer support programmes)
Participating staff members described successful ClinA students as 'having to have a lot of resilience - you have to be able to pick yourself up, you know, really quickly' [AC2]; they have internal motivation with a drive to know more, and they 'challenge each other without harming each other'. [AC5] One of the participating HODs commented: 'The way they manage life, the way they deal with uncertainty and the way they deal with people has amazed many.' [AC5]
Participants shared their views on what makes an ideal life saver (peer mentor): patience and understanding; being friendly; easily approachable; devoted to mentoring; kind; considerate; giving; and supportive. The reason why these characteristics are important was highlighted by one of the participating mentees: 'It was easy to reach out to my mentor when I needed something because she was very friendly, patient and approachable, which made communication between us very good.' [ME20]
For the peer mentor programme to be successful, participants mentioned the importance of training and support for the peer mentors. Members of staff commented: 'The mentors need to be taught, you know, that it's not only about "let me see if you understand percussion" but it's also about "what are your goals when you finish?"' [AC4]; train them on what a mentorship programme should look like; that they know what to do with their mentees.' [AC3] A participating programme co-ordinator mentioned the support needed: 'those that are supporting [peer mentors] also needs (sic) support and I think sometimes we forget that as a whole.' [AC2]
(iv) Rip currents (perceived constraints of peer support programmes)
Three main rip currents (sub-themes) were identified: lack of resources (human and financial); lack of time (especially for peer mentors); and lack of commitment from the peer mentors.
Participating HODs and academic staff listed several resource constraints: human resources (too few academic staff or facilitators); infrastructure (inadequate accommodation and lack of transport); and financial resources. The majority of the students are not funded and struggle to make ends meet: students really don't know where their next meal is coming from, or if they're going to have the money for a taxi to go to wherever it is they need to go.' [AC2] Furthermore, higher education institutions also experience financial challenges, especially after the COVID-19 pandemic and the associated additional costs to implement hybrid learning platforms.
A lack of time was a common constraint, especially mentioned by peer mentors. Because of the demanding study programme, mentors struggle to keep their heads above water: '... because we as BCMP students basically have a 9 to 5 job every day, so it's difficult to be a mentor after hours as well because you have to study, and you have to do a lot of other things as well.' [MR2] The number of students who volunteered to be peer mentors were also noted - if more students volunteer, each peer mentor will have a smaller number of mentees under their wing, and that will make it easier to spend time with them. Currently, some peer mentors have up to 5 mentees, making individual meetings almost impossible due to time constraints.
Student participants thought that it is important that the peer mentor is a volunteer who is dedicated to the programme: 'People that participate in the programme should be people that actually desire to mentor someone, not because it's done by others, but because you actually want to.' [MR6] When the peer mentor is devoted, approachable and supportive, the relationship can develop: 'Mentors have to try to treat their mentees as their siblings and always look out for them. When mentors put in effort then mentees get comfortable and start asking for help more often.' [ME6]
Discussion
This study explored the unique challenges and needs of ClinA students, as well as the perceived enablers and constraints of a peer mentorship programme.
Some of the challenges that the student participants described are not unique to the BCMP programme. Challenges faced included funding, accommodation and the gap between rural school and university, which were similar to challenges reported in the literature.[15,16, 25,26] Challenges unique to ClinA students not mentioned before in the literature were: (i) the teaching and learning strategy of the programme; (ii) the decentralised learning platforms; and (iii) the absence of institutional support at CLCs. Participants described the struggle to adjust to the educational strategy that is designed to incorporate authentic learning, self-directed learning, whole-brain learning and collaborative learning.[6] The peer mentors assisted with this adjustment by explaining what is expected of them in the BCMP programme: 'The mentors gave us tips on how to tackle questions and studying tips.' [ME2] Participants (staff and students) all agreed that peer mentor support is beneficial and essential for ClinA students. The mentees valued the lived experiences of the peer mentors, particularly as the decentralised nature of the programme makes it very difficult for students to access academic and psychosocial on-campus support. The ClinA peer mentor is currently a proxy representative of the institutional support programmes.
Perceived enablers included the characteristics of the peer mentors, training, as well as emotional and psychosocial support. Characteristics of peer mentors, i.e. being open, friendly, willing to help, committed, dedicated, approachable, knowledgeable, trusting, caring, warm, supporting and kind, are also reported elsewhere.[9,12,27,28] The importance of proper training for peer mentors emerged and is confirmed by Gershenfeld,[27] who conducted a review of undergraduate mentoring programmes. Sheri et al.[29] reports advantages of mentor training: boosts confidence in working with mentees and nurtures mentoring relationships; improves communication skills; and increases enthusiasm about mentoring. According to the participants of this study and supported by the literature, mentor training should include information on the objectives of the mentorship programme and the role of the peer mentor.[27,28]
One of the constraints mentioned by participants was the lack of resources (especially funding) and a lack of time (peer mentors struggle to find time to meet with the mentees regularly because of their own academic schedule). Other authors also mention a lack of time and resources as obstacles in running mentorship programmes.[15,29] The perceived lack of commitment from some peer mentors is not mentioned in the literature, but was raised in this study.
Conclusion
This study was a preliminary exploration of the needs and challenges of first-year ClinA students in SA. It is clear that a peer mentorship programme is a possible solution to address these students' unique needs. It is therefore recommended that a bespoke peer mentorship programme for first-year ClinA students and a short learning programme to train and prepare peer mentors for their specific roles are developed.
Acknowledgements. We would like to thank the Department of Family Medicine, Faculty of Health Sciences, University of Pretoria and the research participants for their contribution to the success of our work. We would also like to thank the research participants from the Division of Clinical Associates, Department of Family Medicine, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, and from the Division of Clinical Associates, Department of Family Medicine and Rural Health, Faculty of Health Sciences, Walter Sisulu University, Mthatha.
Author contributions. CN conceptualised and wrote the draft manuscript under the supervision of JEW and PHdT, who critically reviewed it and provided input to revise the document.
Funding. None.
Conflicts of interest. None.
References
1. Tshabalala Z, Smalley S, Louw M, et al. Clinical associates in South Africa: Optimising their contribution to the health system. South African Health Review. 2019. https://www.hst.org.za/publications/South%20African%20Health%20Reviews/ 17%20SAHR_2019_Clinical%20associates%20in%20South%20Africa.pdf (accessed 31 March 2022). [ Links ]
2. Mlambo M, Dreyer AR, Dube R, Mapukata NO, Couper I, Cooke R. Transformation of medical education through decentralised training platforms: A scoping review. Rural Remote Health 2018;18:4337. https://doi.org/10.22605/RRH4337 [ Links ]
3. University of Pretoria. Clinical Medical Practice (Internet). Pretoria: University of Pretoria. https://www.up.ac.za/clinical-medical-practise (accessed 31 March 2022). [ Links ]
4. University of the Witwatersrand. Clinical Medical Practice (Internet). Johannesburg: University of the Witwatersrand. https://www.wits.ac.za/course-finder/undergraduate/health/clinical-medical-practice/ (accessed 31 March 2022). [ Links ]
5. National Student Financial Aid Scheme. https://www.nsfas.org.za/content/mission.html (accessed 3 April 2022). [ Links ]
6. Hugo J, Slabbert J, Marcus T, et al. The clinical associate curriculum - the learning theory underpinning the BCMP programme at the University of Pretoria. Afr J Health Professions Educ 2012;4(2):128-131. https://doi.org/10.7196/AJHPE.188 [ Links ]
7. Doherty J, Conco D, Couper I, et al. Developing a new mid-level health worker: Lessons from South Africa's experience with clinical associates. Glob Health Action 2013;6. https://doi.org/10.3402/gha.v6i0.19282 [ Links ]
8. Shapiro S, Shapiro D, Schwartz G. A review of the literature on stress management in medical education, 1969 to 1998. Acad Med 2000;75(7):748-759. https://doi.org/10.1097/00001888-200007000-00023 [ Links ]
9. Mills C, Heyworth J, Rosenwax L, et al. Factors associated with the academic success of first year health science students. Adv Health Sci Educ 2009;14(2):205-217. https://doi.org/10.1007/s10459-008-9103-9 [ Links ]
10. Motsabi S, Diale B, van Zyl A. The role of social support in the persistence of first-year first-generation African students in a higher education institution in South Africa. S Afr J High Educ 2020;34(4):189-210. https://doi.org/10.20853/34-4-3486 [ Links ]
11. Akinla O, Haga P, Atiomo W. A systematic review of the literature describing the outcomes of near-peer mentoring programs for first year medical students. BMC Med Educ 2018;18(1):98. https://doi.org/10.1186/s12909-018-1195-1 [ Links ]
12. Collings R, Swanson V, Watkins R. The impact of peer mentoring on levels of student wellbeing, integration and retention: A controlled comparative evaluation of residential students in UK higher education. High Educ 2014;68(8):927-942. https://doi.org/10.1007/s10734-014-9752y [ Links ]
13. Kagee A, Naidoo T, Mahatey N. Theoretical underpinnings of a student mentoring programme at a historically black university in South Africa. Int J Adv Counsel 1996;19(3):249-258. https://doi.org/10.1007/BF00115680 [ Links ]
14. McLean M. Does the curriculum matter in peer mentoring? From mentee to mentor in problem-based learning: A unique case study. Mentor Tutor Partnership Learn 2004;12(2):173-186. https://doi.org/10.1080/136112604200023992 [ Links ]
15. Masehela L, Ndebele C, Sikhwari T, et al. Mentors' reflections of a pilot mentoring programme in a South African university. Anthropologist 2014;17(2):367-376. https://doi.org/10.1080/09720073.2014.11891446 [ Links ]
16. Mammen M. Using mentees' feedback to improve a mentoring program in a South African medical school. Anthropologist 2012;14(1):1-8. https://doi.org/10.1080/09720073.2012.11891213 [ Links ]
17. Yüksel P, Yıldırım S. Theoretical frameworks, methods, and procedures for conducting phenomenological studies in educational settings. Turkish Online J Qual Inquiry 2015;6(1). [ Links ]
18. Vygotsky LS. Thought and Language. Cambridge, MA: MIT Press, 1962. [ Links ]
19. Ackerman EK. Constructing knowledge and transforming the world. In: Tokoro M, Steels L, eds. A Learning Zone of One's Own: Sharing Representations and Flow in Collaborative Learning Environments. Amsterdam: IOS Press, 2004:15-37. [ Links ]
20. Cresswell JW Research Design: Qualitative, Quantitative, and Mixed Methods. Thousand Oaks, CA: SAGE, 2009. [ Links ]
21. Etikan I, Musa S, Alkassim R. Comparison of convenience sampling and purposive sampling. Am J Theoret Applied Stat 2016;5(1):1-4. https://doi.org/10.11648/j.ajtas.20160501.11 [ Links ]
22. Cooperrider DL, Srivasta S. Research in Organisational Change and Development. Connecticut: JAI Press, 1987. [ Links ]
23. Tesch R. Qualitative Research: Analysis Types and Software. London: Routledge, 2013. [ Links ]
24. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3(2):77-101. [ Links ]
25. Bojuwoye O. Stressful experiences of first year students of selected universities in South Africa. Counsel Psychol Quarterly 2002;15(3):277-290. https://doi:10.1080/09515070210143480 [ Links ]
26. Pillay A. University-based mentoring programmes for high-risk first year students: A critical literature review. MA thesis. Gqeberha: Nelson Mandela Metropolitan University, 2011. [ Links ]
27. Gershenfeld S. A review of undergraduate mentoring programs. Rev Educ Res 2014;84(3):365-391. https://doi.org/10.3102/0034654313520512 [ Links ]
28. Holt LJ, Lopez MJ. Characteristics and correlates of supportive peer mentoring: A mixed methods study. Mentor Tutori: Partnership Learn 2014;22(5):415-432. https://doi.org/10.1080/13611267.2014.983326 [ Links ]
29. Sheri K, Too J, Chuah S, et al. A scoping review of mentor training programs in medicine between 1990 and 2017. Med Educ Online 201934(1). https://doi.org/10.1080/10872981.2018.1555435 [ Links ]
 Correspondence:
Correspondence:
C Nel
corne.nel@up.ac.za
Declaration. The research for this study was done in partial fulfilment of the requirements for C Nel's PhD (Public Health) degree at the University of Pretoria.


{kind=link}
{kind=link}