










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.15 no.4 Pretoria dic. 2023
http://dx.doi.org/10.7196/AJHPE.2023.v15i4.570
RESEARCH
Exploring how longitudinal integrated clerkships at Stellenbosch University influence the career journeys of medical graduates
F CoetzeeI; S van SchalkwykII; I CouperIII
IMB ChB, MMed (FamMed), MPhil (HPE) ; Ukwanda Centre for Rural Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIPhD; Centre for Health Professions Education, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIIBA, MB BCh, MFamMed, FCFP (SA);Ukwanda Centre for Rural Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
ABSTRACT
BACKGROUND. Longitudinal integrated clerkships (LICs) are increasingly being implemented across the globe for their educational benefits and the recruitment of rural medical practitioners. As new LICs are established, it is important to explore the extent to which these benefits manifest, and the influence of LICs on the career journeys of graduates. Stellenbosch University's LIC has been running for 11 years, and to date the career outcomes of graduates have not been described.
OBJECTIVES. To explore factors that influence the career journeys of graduates from Stellenbosch University's LIC.
METHODS. An interpretivist, qualitative study was performed. Semi-structured interviews that were recorded and transcribed were conducted (8 graduates, >5 years after graduation). Inductive thematic analysis was done. Participants were asked to depict their career journeys. These pictures and an interview guide were used as prompts during the interviews.
RESULTS. Three themes were generated from the data: (i) feeling prepared for the career journey; (ii) acquiring a new motivation and career goals; and (iii) unexpected influences on career journeys. The availability of posts and transformative influences are important factors in the career journeys of LIC graduates. These graduates were enabled by their undergraduate training to explore non-traditional career options and preferred working in rural environments. Although individual priorities caused many participants to work in urban settings, they indicated a desire to return to rural environments.
CONCLUSIONS. The LIC training at Stellenbosch University acts as a significant influence on the early career journeys of such graduates, which are possibly achieved in two ways. Firstly, LIC supports the development of professional identities among its graduates. Secondly, LIC supports transformative learning within a safe learning environment that leads to changes in perspectives regarding the graduates' responsibility towards patients and communities.
Institutions educating health professionals have been challenged to produce graduates who are socially responsible, adequately trained to function in interprofessional teams and responsive to the needs of rural and marginalised cornmunities.[1] Longitudinal integrated clerkships (LICs) are one of the interventions implemented to produce such graduates.[2] An LIC is a model of training where the student is immersed in a clinical environment for an extended period, and where learning takes place in an integrated way, while students are actively participating in the care of patients.[3] Medical students in rural primary care LICs are involved with the care of undifferentiated patients in generalist environments, where they treat patients presenting with various problems daily, as opposed to clinical rotations, where the students work in a department of a tertiary or secondary training hospital and for a period of time only learn about one specific clinical domain, such as internal medicine. Career journeys of junior doctors are influenced by a multitude of factors, and the career decision-making processes among doctors have been described as a complex and poorly understood phenomenon.[4,5] It is unclear to what extent the choices of career location (urban or rural) of doctors are influenced by their initial preferences, their training and their personal circumstances.[6,7] Furthermore, individuals have their own set of motivations, which are influenced by their background, personalities and work experiences[6,7]
The development of robust clinical reasoning and a holistic approach to care are also supported by learning environments that incorporate learning in a patient-centred apprenticeship, such as an LIC.[8] LICs further create opportunities for students to develop procedural, communication and teamwork skills that are important in healthcare contexts where junior doctors have significant clinical responsibilities.[9] LICs are primarily used as an effective strategy for the recruitment and retention of doctors in rural and remote areas.[10]
The popularity of LICs has grown in recent years. Fifty-five LICs were identified across four continents in 2013.[3] By July 2021, 95 LICs were listed on the website of the Consortium of Longitudinal Clerkships.[11] Uptake of LICs in South African (SA) medical schools has been modest. Of the 10 medical schools in SA, only 3 have an LIC of >6 months.
LICs have been adopted by a number of medical training institutions across the world, owing to the educational benefits they are reported to offer. [12] The benefits include facilitating transformative learning experiences[3,4 and enabling continuity with preceptors, patients and communities while students work in clinical environments for >6 months.[10]
Transformative learning experiences are events that challenge the paradigms of a learner and potentially lead to an alteration or reconstruction of perspectives.[13] Mezirow's initial description of transformative learning was outside the context of medical education, but it is now widely used as a pedagogy within the field.[14] LICs offer valuable and often challenging learning experiences to undergraduate medical students while they are immersed in clinical contexts and communities, with ample opportunities to reflect on these experiences.[10] Mezirow's phases of perspective transformation involve several steps, including perspective changes due to specific experiences. His work therefore provides a useful lens for viewing transformative learning within clinical contexts and when the development of professional identities is considered.[15,16]
A number of factors, some relating to the individuals, some to the working contexts and some to the healthcare system and society, have an influence on the career decisions and career journeys of docto rs.[4,5]
From the literature it is evident that the following factors often play a pivotal role when doctors choose to work/not to work in rural environments: (i) whether the graduate is of rural origin;[17] (ii) undergraduate clinical exposure to rural environments;!2,101 (iii) postgraduate training opportunities in rural areas; and (iv) the rural/urban origin of the doctor's partner.[181 The abovementioned factors are also applicable to SA doctors.[4,19]
The studies that involved SA doctors[4,191 included graduates from traditional rotation-based programmes; currently, little is known about where LIC graduates eventually practise and for what reasons.
The development and running of an LIC require a significant investment in time and resources.[12] It is therefore not surprising that many institutions with rural LICs have not only studied the career outcomes of their graduates, but also the reasons for such choices.[20,21] However, work of this nature has not been conducted in the SA context. Stellenbosch University's LIC, described as the longitudinal integrated model (LIM), has produced graduates since 2011, but the career outcomes of these graduates have not been investigated. This study was therefore designed to answer the question: What are the factors that influence the career journeys of Stellenbosch University LIC graduates?
Methods
This study was a qualitative exploration of the factors that influence the career choices of LIC graduates, conducted within an interpretivist paradigm that allowed for the exploration of social issues, experiences and situational factors[22] regarding the participants' careers. Eight LIC graduates from a cohort of 26 who qualified from Stellenbosch University between 2011 and 2016 were recruited through purposive sampling. The specific time frame was chosen so that graduates would have completed their community service 2 years before the interview. It was estimated that at this stage graduates potentially have a clearer view of their career plans. To incorporate a diversity of perspectives that reflect some of the important factors described in the literature, attempts were made to ensure that the participants were varied in terms of years after graduation, gender and work location (rural or urban).
Participants were telephonically recruited by the primary investigator (FC), followed by an email invitation. All graduates who were approached agreed to participate and gave written informed consent. Data were collected by conducting in-depth semi-structured interviews, using an interview guide. Prior to the interviews, participants were asked to draw a picture to illustrate their career journey since graduation. These drawings were used as prompts during the interviews. Six participants provided a drawing; those who did not, were asked at the start of the interview to describe how they would visually depict their careers. These descriptions were used as prompts for the interviews. FC conducted all the interviews via video calls using Zoom (Zoom Video Communications Inc., USA), which lasted 45 - 60 minutes. All interviews were conducted in English and were recorded. The audio files were transcribed verbatim by a contracted transcriber. Inductive thematic analysis of the data was performed by following the steps set out by Braun and Clarke:[23] (i) becoming familiar with the data; (ii) generating initial codes; (iii) searching for themes; (iv) reviewing themes; (v) defining and naming themes; and (vi) producing the report. FC took the lead in the process of analysis while the entire author team discussed the finalisation of codes and the identification of themes. After iterative reviewing of the data, codes were assigned to ideas and pertinent events related to the research question. This procedure was followed by in-depth analysis to ensure a rich description and interpretation of the data. Themes were generated from the explicit messages within the data, with the aim of revealing patterns for further interpretation and to theorise on their implications in relation to previous literature.[23] OneNote (Microsoft Corp., USA) software was used to capture the text and code the transcribed interviews, and allowed for analysis of the data similarly conducted with other data-analysis software. Codes were assigned to text within transcripts using the 'tag' function in OneNote. This allowed for searches and grouping of codes in the transcripts, which enabled easy recognition of patterns and generation of themes.
Efforts were made to ensure quality of the research process. An interview guide was developed, which was peer reviewed by IC and SvS. IC is a family physician and professor in the Ukwanda Centre for Rural Health at Stellenbosch University, and has experience in rural health; SvS has a background in health professions education and is director of the Centre for Health Professions Education at Stellenbosch University. FC is a family physician who works in a rural context and has been intimately involved with the training of LIC students and is therefore known by most of them. FC had an insider view as a researcher, with possible benefits of encouraging participation and having a better understanding of the subject matter than outsiders to the programme.[24] However, it is possible that participants might have been more likely to offer positive comments about their undergraduate training because of FC's involvement in the programme. At the start of interviews, the participants were encouraged to express their views freely and were assured that their responses would not only be anonymised, but that identifiers would also be removed from their responses.
Ethical approval
The study was approved by the Health Research Ethics Committee of Stellenbosch University (ref. no. S21/03/040). As the study consisted of a small number of participants, the reporting of the results sought to maintain anonymity by limiting the demographic information that is reported and by removing the names of facilities and persons involved.
Results
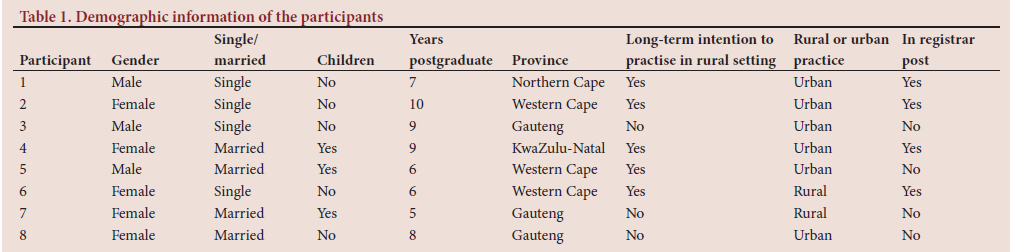
The demographics of the 8 participants are displayed in Table 1.
The male-to-female ratio is similar to that of the students who elected to participate in the LIC at Stellenbosch University.
The following three themes were developed from the data:
• feeling prepared for the career journey
• acquiring a new motivation and career goals
• unexpected influences on career journeys.
Participants' quoted responses are presented as follows:
• interviewee number (INT X)
• years working since graduation (PGY XX).
Theme 1: Feeling prepared for the career journey
Participants felt that their LIC training experiences in a district hospital prepared them for the experiences they encountered during the internship and following years:
'I think [LIC site] prepared me well for that [the career journey]. Again, maybe this is to a degree my personality, and the fact that I'm not scared to kind of step up and try something new, and when I was at Tygerberg [tertiary training hospital], yes, we did get to do things. But often, you know, you are so far back in the queue to do something.' [INT 2, PGY 10] 'I think it did, inasmuch as it showed me what the end goal was. People who have hit internship straight out of Tygerberg, they struggled clinically, and they struggled with the decision making. Whereas you are exposed to a primary level thing and getting to make those decisions as an undergrad and realising the gravity of what it is that we are doing.' [INT 5, PGY 6]
A key influence articulated by participants related to a sense of being ready for the responsibility that came with practising as a doctor because of their LIC experience. During their LIC training, participants had to take responsibility for the patients under their care, more so than their colleagues who remained at the tertiary hospital. Participants said that being responsible for patients increased their confidence and allowed them to venture into careers such as rural surgeons and rural psychiatrists, which they had not considered previously. Participants also felt that they were empowered to have an impact on the healthcare system by having more responsibility while working in clinical teams:
But our time in [LIC site] gave us an idea of what it's like to actually be doctors, and what the reality of it is ... Another thing I've noticed is once you've been there [a rural training site], you notice how simplified your time in a tertiary facility actually is. In terms of being in [LIC site] or being a primary level person, the buck stops with you. You've got to be the decision maker, and it's very easy to just pass on the responsibility in a tertiary facility, and it can hinder your development as a professional.' [INT 5, PGY 6]
'But having been in a small hospital where you are part of a team and you are working and you're responsible for patients, you learn that responsibility quite early on. I think throughout my career, that's the one thing that has stayed constant, that whatever patient you are seeing, you are responsible for that patient. When you understand that responsibility, you want to make a real change, and you want to make a real contribution.' [INT 6, PGY 6]
Being trained in rural settings during the undergraduate LIC training, permitted participants to become familiar with rural practice, rural communities and the way in which clinical teams functioned in these environments. Being familiar with rural environments lessened the uncertainty of having to enter an unknown domain when starting to work as a doctor and gave participants the confidence to apply for posts in rural environments:
'... the nice thing about the LIM [LIC] is we knew our patients, they knew us. We met them in the shops, and we felt, even as students we felt part of the community, and I don't think that's possible in a tertiary facility.' [INT 5, PGY 6]
'I think it's [LIC training] helped in the sense that maybe I wouldn't have considered taking that rural post, that sort of kickstarted my career, that MO [medical officer] post in psychiatry, had I not experienced living in a small town before. I think I sort of - I wouldn't say knew what to expect, but I sort of was already accustomed to some of the things I was experiencing in Ladysmith. So, it was not really new, some of it.' [INT 4, PGY 9]
A participant who lives in a city reported that she sought the rural hospital experience and consequently decided to work in an underserved environment instead of a tertiary hospital:
'. Many people ask me, but then why don't you go to Steve Biko or Kalafong or a private GP, and then I just feel like Mamelodi is closer to a small town than being in a tertiary academic setting. So ya, I'm still trying to get that experience by living in a city, if that makes sense.' [INT 7, PGY 5]
Theme 2: Acquiring a new motivation and career goals
Participants described how their LIC training had influenced their thinking about the type of doctor they wanted to be and the priorities they wanted to pursue. This enabled them to consider employment options outside of tertiary training hospitals, which are typically in urban areas. Working with generalist clinicians in primary care environments during their LIC training, had participants change their perspectives regarding their own priorities and the pursuit of monetary gain:
'I remember in [LIC site], the clinical time was spent in the emergency unit. We got exposed to a lot of primary level things, and I think that made the time in the emergency unit, it played the biggest impact . The people and the doctors working in Hermanus, they were just happy. They weren't specialising, they were just GPs, but they were happy, and they were living full lives . I learnt that the goals that I have for the future might not only just be monetary. There are other things as well. There's time, loved ones, and other things that are more valuable, I think, than a salary' [INT 5, PGY 6]
'I think that [the LIC training] was one of the best experiences I have been through ... as the time went by, that's when I started to really get into my calling of really just doing medicine.' [INT 3, PGY 9]
Some participants' role models demonstrated that it is possible to have a significant impact on patient outcomes in low-resourced environments in which the LIC training took place. Having then seen the impact that an individual can have within the system, the participants became motivated to do the same:
Dr ABC, he used to be the consultant in [LIC site] when I was there as a LIM [LIC] student. Hearing about his story, about how he had transformed the Hospital, but also, being there and working with him, and seeing how he worked. How he was able as a clinician to do so much ... I think maybe let me just say that just watching others ahead of me, work in situations where they were not necessarily deemed to be favourable, or the most ideal situation, but the impact that they had in their communities, I think for me, that became the drive.' [INT 6, PGY 6]
Being trained in communities where access to care and specialist services are limited, made participants aware of these challenges. For many participants, the LIC training stimulated a desire to improve healthcare outcomes - not only for patients, but also for communities. This encouraged them to pursue careers that would improve patient outcomes for communities:
'But going to [LIC site] for your final year of medical school, you know, I think it just makes you realise that you can do so much more in a small town, than what you think you can. There is so much more available today to reach out to, to other places, than what we think is possible.' [INT 2, PGY 10]
'Because when you measure your output by what you are able to do for the people that you're serving, for me, now that became important ... But working in a population where you can meet people at their need, and you can create whatever resource that you have, you can make it multiply.' [INT 6, PGY 6]
The influence of the LIC was seen to be carried through into participants' postgraduate years; they developed a greater sense of duty towards communities and chose to remain in the public service to serve more patients:
'... even though I love the current situation [working in the private sector in a city] I still see that I need to go back to my people [in a rural environment], and ja, and just serve them.' [INT 3, PGY 9] 'But I think, ja, I'm happy with the government sector, and I think I'm needed there. The amount of patients that are there, it's just a lot, and maybe I've been of more use there than I would be in the private sector.' [INT 4, PGY 9]
Theme 3: Unexpected influences on career journeys
Despite the positive influences described above, participants also reported on unexpected factors that re-routed their career journeys from their original intentions. These factors were often systemic and related to the availability of employment, and were therefore presumably shared with graduates from traditional rotation-based programmes.
In the years after graduation, participants discovered which clinical domains they preferred. For some this resulted in an internal conflict, as it led them to enrolling in a specialist training programme and consequently took them away from rural environments, whereas others' career interests encouraged them to continue their work in rural areas:
'... and then when I started noticing that I am enjoying this primary health facility setup in a [urban] mining working community, I thought let me just join this as a permanent contract, and that's what I did, and I've been enjoying it ever since .' [INT 3, PGY 9]
'... [Initially] I thought that I wanted to end up in a tertiary setting, because I enjoyed more high-risk obstetrics, I enjoyed critical care. But I was so conflicted, because I wanted to work in a rural setting, serve in a rural population, and serving women who are generally or traditionally
under-served.' [INT 6, PGY 6]
Participants' career journeys were also influenced by the limited number of available posts after their compulsory community service and by having to wait for a post to become available. This was a common experience shared by participants, affecting all but one participant:
'I did COM-Serve at Mamelodi last year, and only three of us have jobs, the rest [including rotation-based graduates] are still unemployed and frantically looking for jobs. So ya, I think job security is a huge factor that people don't tell people about when you're undergraduate.' [INT 7, PGY 8]
Discussion
This research explored the influences on the career journeys of graduates from a rural LIC. Several factors have an influence on the career decisions and career journeys of doctors - some relating to the individuals, some to the working contexts and some to the healthcare system and society.[4,5]
Regarding individual factors, most medical students exiting medical school feel unprepared for clinical practice, due to a lack of confidence regarding clinical and practical skills,[25,26] whereas LIC graduates often feel better prepared than their peers who were trained in rotation-based programmes.[27,28] This was indeed the case for most participants interviewed in this study. The increased confidence relates to having more opportunities to learn practical skills,[10] but also to the development of a strong professional identity.[12,29]
Our findings suggest that graduates of the LIC are supported in the development of their professional identities, as the training offers ample opportunities to be responsible for patient care, thus nurturing an increased confidence and willingness to take on greater challenges. Professional identity formation is the active process of developing professional values, moral principles, actions, aspirations and ongoing self-reflection regarding the identity of the individual.[30] Wald[30] discusses the key drivers of professional identity formation, which include experiential and reflection processes, the integral role of relationships and role models, and discussion in an authentic community of learners. Participants in this study specifically mentioned their experiences and role models as influences on their thinking regarding their own capabilities and possible careers. As part of professional identity formation, individuals link their motivations and competencies to chosen career roles.[30]
Brown et al.[12] report that LICs foster the development of caring and competency domains in medical practitioners, and that the professional identities that rural LIC graduates develop, encourage them to practise in primary healthcare and underserved environments. This is indeed a desirable outcome for LICs, as it aligns well with the ultimate goal of many LICs - to recruit and retain doctors in rural and underserved environments.[2,31] Konkin and Suddards[32] argue that LICs afford students experiences and time to develop relationships with patients for whose care they are responsible, which encourages them to develop an ethic of care.
Greenhill and Poncelet[33] propose that LICs support transformative learning by creating spaces where students can reflect on health issues together with the social context of their patients, and a social system where students can critically reflect on pertinent issues. Within this social system, students can also question, challenge and rejuvenate their personal values and shape their professional identities.[33] Brown et al.[34] report that LICs shape students' social consciences. Furthermore, LICs cause students to see themselves as responsible and caring patient advocates; LICs also endow some students with a sense of social responsibility to return to underserved settings in future.[34] These ideas regarding the transformative nature of LICs were supported by the findings of this study.
Transformative learning, as described by Mezirow,[13] comprises several steps; 'transformation' occurs when the person experiencing a 'disorientating dilemma' has moved beyond the experience and reached a place where a problematic frame of reference is replaced by new or revised frames of reference that will better equip the person for future actions.[13,14] LICs in rural environments provide students an earlier transition from being student to healthcare practitioner by enabling incorporation into healthcare teams and by challenging their attitudes and beliefs regarding rural populations.[33] Participants in this study experienced disorientating dilemmas regarding their 'drive' and career goals, causing some of them to change their 'problematic perspective' and to plan a different course for their careers. Specifically, some participants reported becoming aware of the disparities that exist in the healthcare system and that a pursuit of monetary gain or academic interests might be in conflict with addressing these disparities. Another disorientating dilemma that some participants faced related to their work environment. Working within a smaller district hospital during their LIC took away the strangeness of the environment, and they discovered that they preferred it to working in urban environments. These experiences were coupled with developing greater confidence while working and a sense of social responsibility towards communities.
The working contexts of undergraduate students in LICs allow students to experience disorientating dilemmas while being supervised, thus providing a safe space for encountering challenging situations.[32] Therefore, graduates are better equipped to deal with future disorientating dilemmas as they gain confidence while acquiring their professional identities.[30]
Regarding factors that pertain to the healthcare system and employment opportunities, participants in this study reported struggling to find a post in their preferred clinical domain. Some of them 'scrambled' to get employment and others had to move to urban environments when enrolling for specialist training. These challenges often interfered with their plans regarding rural career journeys. The realities of a limited variety of employment options in rural areas, job insecurity and limited professional development opportunities for rural clinicians are not unique to SA.[6] These factors potentially limit the workforce impact of rural LICs.
The findings of this study might not be applicable in contexts where internship or specialist training is structured differently and where healthcare systems differ significantly from those in SA. Another limitation is the timing of this study, as it was done relatively early in the career journeys of the participants; therefore, it is unclear if those who are working in rural environments will continue to do so. Similarly, we do not know if participants currently specialising and who have indicated that they would pursue rural practice, will return to work in rural environments.
Conclusion
LICs support the development of caring and empathic professional identities in students in the years after graduation. Graduates from the rural LIC of Stellenbosch University indicated that they experienced transformative learning by facing disorientating dilemmas within safe learning environments that led to changes in their perspectives regarding their responsibility towards patients and communities. The support that rural LICs offer students to develop their professional identities and adjust their perspectives regarding their roles as healthcare professionals may explain why these LICs encourage students to pursue rural careers. It is important for LIC co-ordinators to select LIC student supervisors carefully, as they will be role models for LIC students and may encourage or discourage rural practice. It might also be useful to include discussions related to role-modelling and communities of practice in faculty development for LIC student supervisors. The influence of the LIC on graduates' career journeys is limited by factors pertaining to the healthcare system and rural postgraduate training opportunities for doctors. More research on how to support professional identity formation and transformative learning in LICs is needed.
Declaration. The research for this study was done in partial fulfilment of the requirements for FC's MPhil (HPE) degree at Stellenbosch University.
Acknowledgements. The enthusiastic participation of the LIM graduates made this research possible and a pleasure; we are very grateful to all those involved.
Author contributions. FC, IC and SvS were involved in the initial conceptualisation of the research project. FC conducted the data collection, data analysis and preparation of the first draft of the manuscript. FC, IC and SvS worked on the subsequent drafts and final version of the manuscript.
Funding. Ukwanda Centre for Rural Health Strategic Research Fund.
Conflicts of interest. None.
References
1. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. Lancet 2010;376(9756):1923-1958. https://doi.org/10.1016/S0140-6736(10)61854-5 [ Links ]
2. Holst J. Increasing rural recruitment and retention through rural exposure during undergraduate training: An integrative review. Int J Environ Res Public Health 2020;17(17):1-19. https://doi.org/10.3390/ijerph17176423 [ Links ]
3. Worley P, Couper I, Strasser R, et al. A typology of longitudinal integrated clerkships. Med Educ 2016;50(9):922-932. https://doi.org/10.1111/medu.13084 [ Links ]
4. Reid SJ, Couper ID, Volmink J. Educational factors that influence the urban-rural distribution of health professionals in South Africa: A case-control study. S Afr Med J 2011;101(1):29-33. https://doi.org/10.7196/SAMJ.4342 [ Links ]
5. Spooner S, Pearson E, Gibson J, Checkland K. How do workplaces, working practices and colleagues affect UK doctors' career decisions? A qualitative study of junior doctors' career decision making in the UK. BMJ Open 2017;7(10):1-9. https://doi.org/10.1136/bmjopen-2017-018462 [ Links ]
6. Cosgrave C, Malatzky C, Gillespie J. Social determinants of rural health workforce retention: A scoping review. Int J Environ Res Public Health 2019;16(3):314. https://doi.org/10.3390/ijerph16030314 [ Links ]
7. Yang Y, Li J, Wu X, et al. Factors influencing subspecialty choice among medical students: A systematic review and meta-analysis. BMJ Open 2019;9(3):e022097. https://doi.org/10.1136/bmjopen-2018-022097 [ Links ]
8. Gupta S, Howden S. Medical students' experiences of a longitudinal integrated clerkship: A threshold concepts analysis. Educ Prim Care 2021;32(6):336-343. https://doi.org/10.1080/14739879.2021.1939796 [ Links ]
9. Poncelet A, Hirsh D, eds. Longitudinal Integrated Clerkships: Principles, Outcomes, Practical Tools, and Future Directions. New York: Gegensatz Press, 2016. [ Links ]
10. Hudson JN, Poncelet AN, Weston KM, Bushnell JA, Farmer E. Longitudinal integrated clerkships. Med Teach 2017;39(1):7-13. https://doi.org/10.1080/0142159X.2017.1245855 [ Links ]
11. Consortium of Longitudinal Integrated Clerkships. LIC programs. 2021. https://clicmeded.com/lic-programs/ (accessed 27 August 2022). [ Links ]
12. Brown MEL, Anderson K, Finn GM. A narrative literature review considering the development and implementation of longitudinal integrated clerkships, including a practical guide for application. J Med Educ Curric Dev 2019;6:1-12. https://doi.org/10.1177/2382120519849409 [ Links ]
13. Mezirow J. Transformative Dimensions of Adult Learning. San Francisco: Jossey-Bass, 1991. [ Links ]
14. Van Schalkwyk SC, Hafler J, Brewer TF, et al. Transformative learning as pedagogy for the health professions: A scoping review. Med Educ 2019;53(6):547-558. https://doi.org/10.1111/medu.13804 [ Links ]
15. Brown MEL, Whybrow P, Kirwan G, Finn GM. Professional identity formation within longitudinal integrated clerkships: A scoping review. Med Educ 2021;55(8):912-924. https://doi.org/10.1111/medu.14461 [ Links ]
16. Kerins J, Smith SE, Phillips EC, Clarke B, Hamilton AL, Tallentire VR. Exploring transformative learning when developing medical students' nontechnical skills. Med Educ 2020;54(3):264-274. https://doi.org/10.1111/medu.14062 [ Links ]
17. Walker JH, DeWitt DE, Pallant JF, Cunningham CE. Rural origin plus a rural clinical school placement is a significant predictor of medical students' intentions to practice rurally: A multi-university study. Rural Remote Health 2012;12(1):1-9. https://doi.org/10.22605/RRH1908 [ Links ]
18. Stagg P, Greenhill J, Worley PS. A new model to understand the career choice and practice location decisions of medical graduates. Rural Remote Health 2009;9(4):1-10. https://doi.org/10.22605/RRH1245 [ Links ]
19. Burch VC, McKinley D, van Wyk J, et al Career intentions of medical students trained in six sub-Saharan African countries. Educ Health: Change Learn Pract 2011;24(3):1-16. https://doi.org/10.4103/1357-6283.101416 [ Links ]
20. Myhre DL, Bajaj S. Practice locations of longitudinal integrated clerkship graduates: A matched-cohort study Can J Rural Med 2016;21(1):13. [ Links ]
21. Playford DE, Ng WQ, Burkitt T. Creation of a mobile rural workforce following undergraduate longitudinal rural immersion. Med Teach 2016;38(5):498-503. https://doi.org/10.3109/0142159X.2015.1060304 [ Links ]
22. Denzin NK, Lincoln YS. The discipline and practice of qualitative research. In: Denzin NK, Lincoln YS, eds. Strategies of Qualitative Inquiry. 3rd ed. Thousand Oaks: SAGE, 2008:1-43. [ Links ]
23. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3(2):77-101. https://doi.org/10.1191/1478088706qp063oa [ Links ]
24. Saidin K, Yaacob A. Insider researchers: Challenges and opportunities. Proceed ICECRS 2017;1(1):849-854.https://doi.org/10.21070/picecrs.v1i1.563 [ Links ]
25. Illing JC, Morrow GM, Rothwell née Kergon CR, et al. Perceptions of UK medical graduates' preparedness for practice: A multi-centre qualitative study reflecting the importance of learning on the job. BMC Med Educ 2013;13(1):1-12. https://doi.org/10.21070/picecrs.v1i1.563 [ Links ]
26. Frambach JM, Manuel BAF, Fumo AMT, van der Vleuten CPM, Driessen EW. Students' and junior doctors' preparedness for the reality of practice in sub-Saharan Africa. Med Teach 2015;37(1):64-73. https://doi.org/10.3109/0142159X.2014.920490 [ Links ]
27. Teherani A, Irby DM, Loeser H. Outcomes of different clerkship models: Longitudinal integrated, hybrid, and block. Acad Med 2013;88(1):35-43. https://doi.org/10.1097/ACM.0b013e318276ca9b [ Links ]
28. Latessa RA, Swendiman RA, Parlier AB, Galvin SL, Hirsh DA. Graduates' perceptions of learning affordances in longitudinal integrated clerkships. Acad Med 2017;92(9):1313-1319. https://doi.org/10.1097/ACM.0000000000001621 [ Links ]
29. Cruess SR, Cruess RL, Steinert Y. Supporting the development of a professional identity: General principles. Med Teach 2019;41(6):641-649. https://doi.org/10.1080/0142159X.2018.1536260 [ Links ]
30. Wald HS. Professional identity (trans)formation in medical education: Reflection, relationship, resilience. Acad Med 2015;90(6):701-706. https://doi.org/10.1097/ACM.0000000000000731 [ Links ]
31. Playford DE, Nicholson A, Riley GJ, Puddey IB. Longitudinal rural clerkships: Increased likelihood of more remote rural medical practice following graduation. Career choice, professional education and development. BMC Med Educ 2015;15(1):1-9. https://doi.org/10.1186/s12909-015-0332-3 [ Links ]
32. Konkin J, Suddards C. Creating stories to live by: Caring and professional identity formation in a longitudinal integrated clerkship. Adv Health Sci Educ 2012;17(4):585-596. https://doi.org/10.1007/s10459-011-9335-y [ Links ]
33. Greenhill J, Poncelet AN. Transformative learning through longitudinal integrated clerkships. Med Educ 2013;47(4):336-339. https://doi.org/10.1111/medu.12139 [ Links ]
34. Brown MEL, Ard C, Adams J, O'Regan A, Finn GM. Medical student identity construction within longitudinal integrated clerkships: An international, longitudinal qualitative study. Acad Med 2022;97(9):1-30. https://doi.org/10.1097/ACM.0000000000004732 [ Links ]
 Correspondence:
Correspondence:
F Coetzee
franna@sun.ac.za
Accepted 3 July 2023


{kind=link}