










Servicios Personalizados
Articulo
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.15 no.1 Pretoria mar. 2023
http://dx.doi.org/10.7196/AJHPE.2023.v15i1.1573
RESEARCH
A nominal group technique to review undergraduate medical students' training in emergency care
D T HagemeisterI; M J LabuschagneII
IMD, PhD (HPE), MPH, EMMB, BA; Department of Family Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIMB ChB, MMed (Ophth), PhD (HPE); Clinical Simulation and Skills Unit, School of Biomedical Sciences, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND. The management of clinical emergencies is an essential skill for medical practitioners; therefore, proper training in these skills is crucial. This is a review of emergency care training by recent graduates of a medical programme to provide feedback on the usefulness of their training experience for entry into clinical practice. Academic clinicians working in the clinical environment, who provide the training, and academic managers who manage the training programme, could provide valuable inputs into reviewing the emergency care training programme contextualised for the uniquely South African challenges.
OBJECTIVES. To obtain and prioritise experience-based and relevant suggestions for improving the current teaching and to invite comment on the suggestions from the relevant managers.
METHODS. Research was conducted in three phases using a nominal group technique to review an undergraduate medical programme. In the first phase, recent graduates from the existing programme identified its strengths and weaknesses. In the second phase, academic clinicians and technical experts provided suggestions for addressing these challenges. In the third phase, data obtained were discussed with academic managers responsible for the undergraduate medical programme.
RESULTS. Findings were grouped into thematic categories: skills and short courses, module structure and content, experiential learning opportunities, health professions educational practice and interprofessional education. Opportunities to gain experience in emergencies in different clinical fields and as a multi-professional team, both in simulation and real-life practice, were among the highlights of the findings.
CONCLUSION. Many of the suggested improvements, such as a dedicated emergency care module, and more simulated and small-group case-based teaching, are achievable with the given resources. Additionally, with recent changes due to the COVID-19 pandemic and lockdown, an environment for change that benefits online content delivery was created. The creation of longitudinal themes will be an enhancement of the current programme.
The handling of clinical emergencies is a fundamental skill expected of medical practitioners.[1] Medical schools in South Africa (SA) have different approaches to teaching emergency care to their students, as there is no national curriculum. Ensuring competence in emergency care is an essential component of preparing graduates successfully for serving as entry-level practitioners working towards independent practice in their third year after graduation (community service).[2]
Aim
This is a follow-up study of junior trainees conducted 2 years ago, with the aim of widening the perspective of the review of emergency skills training in the medical programme.[3] Whereas the earlier study focused only on the students' experience with the emergency care content of their third-year module, the current study extended the view on emergency skills acquisition to the entire undergraduate programme and the usefulness for early-career clinicians.
Objectives
The objectives were to obtain experience-based and relevant suggestions and priorities for improving the current teaching and to invite comment on the suggestions from the relevant managers.
Methods
This qualitative, sometimes called 'semi-quantitative', cross-sectional study comprised three phases based on the nominal group technique (NGT) for programme development, which was introduced in the 1970s by Delbecq and Van de Ven[4] and adopted and used in clinical[5] and health education contexts.[6]
In the first phase, a nominal group of medical interns was formed, who had graduated from our medical school and had since completed either one or both years of the mandatory internship. Convenience sampling was done of graduates employed as medical interns at the local internship training complex. All interns available and willing to participate at the time of the study were included. Appropriate representation of clinical experience from primary healthcare, district hospital and referral hospital sites was aimed for. A total sample of 30 - 40 graduates was included.
In the second phase, we invited academic clinicians and education experts involved in the undergraduate medical programme at our medical school to reflect on the strengths and weaknesses identified by the graduates and to formulate suggestions for the way forward, both within the current resource envelope and with a view to additional resources required. A good representation of clinical disciplines and professional functions (academic clinician/academic manager/educational specialist) was aimed for when recruiting a total of 10 - 15 participants.
For both phases, we followed the steps described in the literature,[5] with the group generating ideas in response to the topic, first in a round-robin session, and then discussing and clarifying the collected ideas (qualitative data). The generated and refined statements were then put to a vote in the group, with each participant prioritising the first- to fifth-most important statements. Points were allocated to each statement - 5 points for the first statement and 1 point for the fifth statement; the total points per statement resulted in a priority rank order (semi-quantitative processing).
In addition to capturing and sorting the hand-written NGT statements on a whiteboard, the first author audio-recorded and transcribed the discussions to analyse concepts and themes that might not be reflected in the written, summarised results of the NGTs.
In the third phase, the findings from the first two phases, together with the proposed categories and themes for improvement and a draft submission to the relevant committee overseeing the training activities, were presented to three academic managers in the undergraduate programme (programme director and the chairs of the education committees for the preclinical and clinical phases in the medical programme) for comment.
The two rounds of NGT discussions were held during November and December 2019. A discussion was held to verify the results with the resource controllers, i.e. the director of the undergraduate medical programme and the chairs of the preclinical and clinical phases of the medical training programme, who were invited to a discussion on the findings and a proposed way forward.
Ethical approval
Ethical approval was obtained from the Health Sciences Research Ethics Committee, University of the Free State (UFS) (ref. no. UFS-HSD2017/1547/2801) and institutional permission was obtained from the university. All participants gave informed consent.
Results
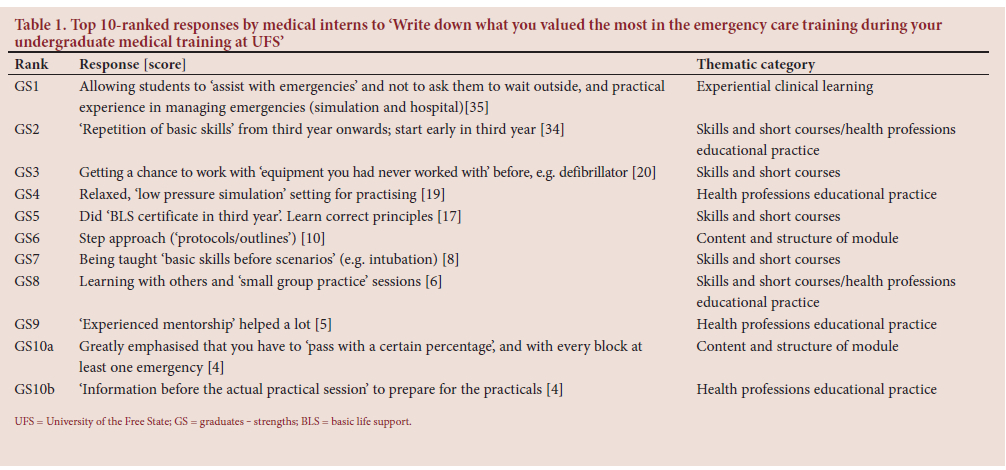
In the first phase of the study, 11 (5 women and 6 men) of the 25 current medical interns at the Bloemfontein complex who had graduated from the programme at UFS agreed to take part in the study. Six were completing the first year of their internship, and 5 were about to finish the second year. (One female first-year intern left before the second question.) The top 10-ranked results from this session are shown in Table 1 (Write down what you valued the most in the emergency care training during your undergraduate medical training at UFS) and Table 2 (Write down suggestions on how to improve the emergency care training during undergraduate medical training at UFS).
Seven participants constituted the panel for the second phase; they represented the departments of Obstetrics and Gynaecology (male specialist, training co-ordinator), Paediatrics (female medical officer, training co-ordinator), Family Medicine (male specialist, training co-ordinator and 1 male and 1 female specialist from the joint provincial and university staff) and the Simulation Unit (female medical officer and male educational technologist). (One female participant left before the second question.) The top 10-ranked results of this session are shown in Table 3 (Write down suggestions, given current resources and based on the comments of the students, what you think can be done to improve the emergency care content and delivery in the undergraduate medical programme at UFS) and Table 4 (Write down suggestions what additional resources and structures might be needed and how these would influence the delivery of the content).
In the third-phase discussion with the 3 academic managers of the undergraduate programme, the topics and themes suggested for improvement were considered in relation to their possible implementation and availability of resources.
The managers indicated that a separate emergency medicine module appears unrealistic in the short-to-medium term. Still, the need to create longitudinal 'themes', including palliative care, communication skills, ultrasound and community-based and interprofessional education, was confirmed. Outcomes for such themes would have to be mapped and appropriately linked throughout the programme. Stewardship of these themes plays a crucial role by individuals taking ownership of the matters. Teaching and learning co-ordinators in the clinical departments play a key role in ensuring the outcomes. However, they will have to be supported in collecting and consolidating current and continuously updated protocols from their disciplines. Of sheer necessity, online content delivery enjoyed a major boost in the 2020 academic year due to the COVID-19 pandemic, and achievements made in this regard need to be perpetuated and expanded.
Managers emphasised the availability of staff development opportunities and support resources and alluded to the individual lecturer's responsibilities to take up such offers. Specific suggestions such as interprofessional education, with the involvement of paramedic staff from the provincial emergency services, a focus on debriefing in the clinical context and the use of a learning portfolio were received positively. Existing structures and projects in this regard were mentioned.
Discussion
A range of themes emerged during the NGT discussions and can be summarised under four categories: (i) resuscitation skills and short courses; (ii) emergency module(s) structure and content; (iii) experiential clinical learning; and (iv) health professions educational practice and interprofessional education. We discuss each theme below as headings for improvement suppositions. Themes are referenced with their placement in Table 1 (rank GS (graduates - strengths)), Table 2 (rank GW (graduates - wishes)), Table 3 (rank EC (educators - current)) and Table 4 (rank EA (educators - additional)), with related literature from the literature review. [7] Annotated text represents the verbatim responses of the participants.
Resuscitation skills and short courses
Formal advanced resuscitation short courses were top of the list for the graduates' 'wish list' (GW1) and the educators' suggestions (EC1).[8] Such teaching events allow students to act as team leaders (GW4) and train in small groups (GS8; EC4; EC5).[9] This finding echoes the graduates' appreciation of the spiralling of resuscitation skills (GS2; GS3; GS7) and the provision of certified basic life-support training (GS5),[10] although more and earlier training would be desirable (GW4; GW7).[11] The introduction of additional formal courses, including early first-aid skills training (EC1; EC2)[12] and training in smaller groups (EC4), is highly dependent on the commitment of resources.
Emergency module(s) structure and content
Structure and content of the module(s) was placed second on the wish list (GW2) and involved a request for an 'emergency module'[13,14] with a 'well-written, all-in-one study resource' (GW2; GW5b). It was reflected in the educators' demand for integration in a 'unified approach between departments' (EC3; EC10b)[15] and for 'approved, current emergency protocols' for each discipline (EA3) to expand on existing protocol-based approaches (GS6). Similarly valued (GS10a) and requested to be expanded (GW5b; GW8) was the presentation of emergencies in the clinical rotations, with the graduates asking for a 'dedicated emergency week per rotation' (GW5a). The educator group responded by suggesting to 'have discipline-specific emergency cases in the curriculum of each department' (EC6),[16] as well as the recommendation to 'provide solutions for resource-constrained environments' (EC7c)[17] and to 'teach preparation for the emergency' (EC13c).
Experiential clinical learning
Hands-on practice under supervision is the age-old concept of apprenticeship. Despite the invention of simulation-based skills training, clinical practice skills as an art and science are mainly acquired in real-life encounters with patients.[18] The graduates, therefore, appreciated having been 'allowed to assist with emergencies' as students (GS1), but wished they could have had more exposure (GW5b).[19] Lecturers would enjoy having case discussions in smaller groups (EC5) and suggested that students get 'exposed to prehospital emergency care' (EC13b)[20,21] and are assign'ed] specific roles and responsibilities during on-calls, to avoid them being not-serious' (EC16a) - although these suggestions did not make it into the top 10-ranked results.
Health professions educational practice and interprofessional education
Educational skills are essential for facilitating learning. Graduates lauded the 'relaxed, low pressure simulation setting' (GS4), 'experienced mentorship' (GS9) and 'information before the actual practical session to prepare' (GS10b). As suggestions for improvement, they mentioned more testing/ assessment (GW8), enough time to practise (GW10), 'teaching by peers' (GW11b) and also tools such as 'mnemonics and rhymes' (GW11a). Logbooks were criticised as being 'not always the answer', with students 'feel[ing] they will be penalised' (GW9) and 'teaching by humiliation or embarrassment is not teaching' (GW13).[22] Educators' suggestions for improving the assessments included the introduction of a 'portfolio to capture experiential learning and reflection' (EC7b) and the inclusion of 'pass/fail-stations' in a dedicated emergency medicine objectively structured clinical examination (OSCE) (EC10c). 'In situ simulations in the clinical environment' could be a way to combine simulation-based learning with the real-life context (EC18b).[23]
Debriefing was mentioned, with lesser emphasis, by the graduates as 'helped a lot after real-life resus' (GS12) and in relation to a wish for 'more regular debriefing in the hospital setting' (GW14), indicating a staff development need on the clinical platform. This was echoed by the educators in the suggestion to 'structure in formal debriefing sessions (psychological and clinical) and teach students how to conduct it' (EC7a).[24]
Interprofessional education was another common theme running through the discussions. The graduates proposed to 'involve nursing students and [emergency medical services] EMS as well with simulations' (GW3),[25] resulting in the lecturers suggesting '[interprofessional education] IPE simulations based on emergency scenarios' (EC10a)[26] and the exposure of students to prehospital emergency care (EC13b), possibly facilitated by a 'formal agreement with EMS about mutual involvement in training' (EA9) and 'better faculty coordination' (EA13).[27]
Additional resources
In keeping with the question posed, the second part of the educators' NGT provided a prioritised list of additional resources required. The most important were human resources, with a demand for appointment of preceptors (affiliated lecturers) on the extended training platform, as well as clinical staff (EA1; EA2).[28,29] Providing 'current protocols' by departments and 'formal agreements with EMS' were mentioned. Additional money, acquisition of 'accredited courses' and a 'proper functioning emergency department at [...] Tertiary Hospital', were also seen as essential building blocks (EA4a-c).[30] Identification of and equipping (telemedicine)[31] with additional training sites (EA7),[32] the production of blended learning material (EA8)[33] and 'additional part-task trainers' (EA10a) complete the list. 'Evaluation of implemented developments' (EA10b)[34,35] and a 'focus on health education research' (EA12) would ensure quality.[36]
Comparison with a previous study[3]
Students and graduates share an appreciation of practical, hands-on skills training, and the demand for a consolidated, well-integrated emergency module that provides clear protocols in a concise module guide was reiterated. Strengthening of training by increasing the number of sites, facilitators, formative assessments, simulation and task trainers, and blended learning use of videos resonate with the findings of our previous study.[3]
Major differences between the student participants in the previous study and the graduates participating in the current study are the increased valuation of structured advanced resuscitation courses and the request for more exposure to and more independent (team leader) handling of real-life clinical emergencies, including structured debriefing, which can certainly be explained by the increased clinical experience of the participants and the broader focus of this study.
Interestingly, ultrasound skills were not mentioned in any of the discussions. This absence, in contrast to the presence of the topic as a basic skill in the recent literature[31,37,38] on emergency skills training, suggests a 'blind spot' or an 'unknown unknown' shared by graduates and educators.
Study limitations
As this study was conducted at an SA medical school and focused on the SA regulatory framework, the applicability of the findings in other contexts might be limited. The training of emergency care skills at other undergraduate medical programmes was not investigated, but the findings could be transferrable to other SA training institutions.
This study also does not cover postgraduate training in emergency medical care.
Recommendations for the way forward
Based on the findings, the following is proposed as a summary of the suggestions from the three phases:
• Creating a dedicated emergency care/medicine module with clearly defined and mapped outcomes. This module should be driven by dedicated staff, preferably with emergency medicine qualifications, and should be well integrated with the teaching and practice of emergency scenarios in the clinical disciplines.
• The abovementioned recommendation needs to be complemented by a thorough needs assessment regarding online material development, simulation equipment and skills, and the availability of a clinical training platform and skills (e.g. debriefing) of preceptors on this platform.
• Depending on the available 'resource envelope', small-group case-based teaching should be strengthened throughout the programme. It would ideally include skills short courses that range from basic first aid in the first year via cardiopulmonary resuscitation courses to advanced courses, such as advanced cardiac life support (ACLS) and advanced trauma life support (ATLS).
• In co-operation with other stakeholders in the academic institutions and on the service delivery platform, a comprehensive interprofessional education programme should use synergies and complementary skills of trainers and foster good interprofessional practice (e.g. handover, joint resuscitations).
Conclusion
Existing strengths of the programme were again highlighted, and many of the suggested improvements could be achieved with the existing resources available at the medical school. Simulation, blended learning and ongoing formative assessment would be essential building blocks for the successful implementation of an emergency care module. The creation of longitudinal 'themes', such as palliative care, communication skills, ultrasound and community-based and interprofessional education, could enhance the emergency care module even further.
Declaration. The research for this study was done in partial fulfilment of the requirements for DTH's PhD degree at the University of the Free State.
Acknowledgements. Our sincere gratitude to Sr Rynsie Hattingh for facilitating the first NGT, Mrs Nokuthula Tlalajoe for facilitating both NGT sessions, and Mrs Theanette Mulder for language editing of the manuscript.
Author contributions. DTH wrote the protocol under supervision of MJL; DTH organised the NGT sessions with the assistance of MJL and created the first draft of the manuscript; both authors edited the manuscript and approved the final version.
Funding. DTH received a bursary from the Health and Welfare Sector Education and Training Authority (HWSETA) towards the completion of a PhD.
Conflicts of interest. None.
References
1. Hobgood C, Anantharaman V, Bandiera G, et al. International Federation for Emergency Medicine model curriculum for medical student education in emergency medicine. Emerg Med Australas 2009;21(5):367-372. https://doi.org/10.1007/s12245-009-0142-7 [ Links ]
2. Abuhusain H, Chotirmall SH, Hamid N, O'Neill SJ. Prepared for internship? Ir Med J 2009;102(3):82-84. [ Links ]
3. Hagemeister DT. Nominal group technique review of the emergency care content of the clinical skills module in the undergraduate medical programme at the University of the Free State. Afr J Health Professions Educ 2021;13(4):240-245. https://doi.org/10.7196/AJHPE.2021.v13i4.1321 [ Links ]
4. Delbecq AL, van de Ven AH. A group process model for problem identification and program planning. J Appl Behav Sci 1971;7(4):466-492. https://doi.org/10.1177/002188637100700404 [ Links ]
5. Gallagher M, Hares T, Spencer J, Bradshaw C, Webb I. The nominal group technique: A research tool for general practice? Fam Pract 1993;10(1):76-81. https://doi.org/10.1093/fampra/10.L76 [ Links ]
6. Dobbie A, Rhodes M, Tysinger JW, Freeman J. Using a modified nominal group technique as a curriculum evaluation tool. Fam Med 2004;36(6):402-406. [ Links ]
7. Hagemeister DT. A framework for integrated emergency care education in South African undergraduate medical programmes. PhD thesis. Bloemfontein: University of the Free State, 2020. [ Links ]
8. Ruesseler M, Weinlich M, Müller MP, Byhahn C, Marzi I, Walcher F. Simulation training improves ability to manage medical emergencies. Emerg Med J 2010;27(10):734-738. https://doi.org/10.1136/emj.2009.074518 [ Links ]
9. Cho Y, Je S, Yoon YS, et al. The effect of peer-group size on the delivery of feedback in basic life support refresher training: A cluster randomised controlled trial. BMC Med Educ 2016;16(1):167. https://doi.org/10.1186/s12909-016-0682-5 [ Links ]
10. Afzal MF, Afzal MN, Sultan MA, Hanif A. Evaluation of performance of basic life support and clinical skills among interns in Mayo and allied hospitals of King Edward Medical University, Lahore. Pak J Med Res 2012;51(4):117. [ Links ]
11. Willmore RD, Veljanoski D, Ozdes F, et al. Do medical students studying in the United Kingdom have an adequate factual knowledge of basic life support? World J Emerg Med 2019;10(2):75-80. https://doi.org/10.5847/wjem.j.1920-8642.2019.02.002 [ Links ]
12. Khan A, Shaikh S, Shuaib F, et al Knowledge attitude and practices of undergraduate students regarding first aid measures. J Pak Med Assoc 2010;60(1):68-72. [ Links ]
13. Wald DA, Lin M, Manthey DE, Rogers RL, Zun LS, Christopher T. Emergency medicine in the medical school curriculum. Acad Emerg Med 2010;17:S26-S30. https://doi.org/10.1111/j.1553-2712.2010.00896.x [ Links ]
14. Cevik AA, Cakal ED, Abu-Zidan FM. Emergency medicine clerkship curriculum in a high-income developing country: Methods for development and application. Int J Emerg Med 2018;11(1):31. https://doi.org/10.1186/s12245-018-0190-y [ Links ]
15. Tews MC, Hamilton GC. Integrating emergency medicine principles and experience throughout the medical school curriculum: Why and how. Acad Emerg Med 2011;18(10):1072-1080. https://doi.org/10.1111/j.1553-2712.2011.01168.x [ Links ]
16. Bernard AW, Malone M, Kman NE, Caterino JM, Khandelwal S. Medical student professionalism narratives: A thematic analysis and interdisciplinary comparative investigation. BMC Emerg Med 2011;11(1):11. https://doi.org/10.1186/1471-227X-11-11 [ Links ]
17. Nelson BD, Saltzman A, Lee PT. Bridging the global health training gap: Design and evaluation of a new clinical global health course at Harvard Medical School. Med Teach 2012;34(1):45-51. https://doi.org/10.3109/0142159X.2011.577122 [ Links ]
18. Sheng AY, Sullivan R, Kleber K, et al Fantastic learning moments and where to find them. West J Emerg Med 2018;19(1):59-65. https://doi.org/10.5811/westjem.2017.10.35179 [ Links ]
19. Avegno J, Leuthauser A, Martinez J, et al. Medical student education in emergency medicine: Do students meet the national standards for clinical encounters of selected core conditions? J Emerg Med 2014;47(3):328-332. https://doi.org/10.1016/j.jemermed.2014.04.029 [ Links ]
20. Ahmad M, Goodsman D, Lightbody E. Introducing medical students to prehospital care. Clin Teach 2012;9(3):168-172. https://doi.org/10.1111/j.1743-498X.2012.00528.x [ Links ]
21. Brenner J, Bird J, Ginzburg SB, et al. Trusting early learners with critical professional activities through emergency medical technician certification. Med Teach 2018;40(6):561-568. https://doi.org/10.1080/0142159X.2018.1444745 [ Links ]
22. House JB, Griffith MC, Kappy MD, Holman E, Santen SA. Tracking student mistreatment data to improve the emergency medicine clerkship learning environment. West J Emerg Med 2018;19(1):18-22. https://doi.org/10.5811/westjem.2017.11.36718 [ Links ]
23. Watmough S, Box H, Bennett N, Stewart A, Farrell M. Unexpected medical undergraduate simulation training (UMUST): Can unexpected medical simulation scenarios help prepare medical students for the transition to foundation year doctor? BMC Med Educ 2016;16(1):110. https://doi.org/10.1186/s12909-016-0629-x [ Links ]
24. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: A best evidence practical guide. AMEE Guide No. 82. Med Teach 2013;35(10):e1511-e1530. https://doi.org/10.3109/0142159X.2013.818632 [ Links ]
25. Ericson A, Masiello I, Bolinder G. Interprofessional clinical training for undergraduate students in an emergency department setting. J Interprof Care 2012;26(4):319-325. https://doi.org/10.3109/13561820.2012.676109 [ Links ]
26. Sigalet E, Donnon T, Grant V. Undergraduate students' perceptions of and attitudes toward a simulation-based interprofessional curriculum: The KidSIM ATTITUDES questionnaire. Simul Healthc 2012;7(6):353-358. https://doi.org/10.1097/SIH.0b013e318264499e [ Links ]
27. Daniel MM, Ross P, Stalmeijer RE, de Grave W. Teacher perspectives of interdisciplinary coteaching relationships in a clinical skills course: A relational coordination theory analysis. Teach Learn Med 2018;30(2):141-151. https://doi.org/10.1080/10401334.2017.1384381 [ Links ]
28. Chong A, Weiland TJ, Mackinlay C, Jelinek GA. The capacity of Australian ED to absorb the projected increase in intern numbers. Emerg Med Australas 2010;22(2):100-107. https://doi.org/10.1111/j.1742-6723.2010.01268.x [ Links ]
29. Ward EC, Kwan J, Garlan K, Bassett E, Klein L. 'To teach or not to teach?' Factors that motivate and constrain Australian emergency medicine physicians to teach medical students. Emerg Med Australas 2013;25(4):353-358. https://doi.org/10.1111/1742-6723.12104 [ Links ]
30. Elnicki DM, Gallagher S, Willett L, et al Course offerings in the fourth year of medical school: How US medical schools are preparing students for internship. Acad Med 2015;90(10):1324-1330. https://doi.org/10.1097/ACM.0000000000000796 [ Links ]
31. Poland S, Frey JA, Khobrani A, et al. Telepresent focused assessment with sonography for trauma examination training versus traditional training for medical students: A simulation-based pilot study. J Ultrasound Med 2018;37(8):1985-1992. https://doi.org/10.1002/jum.14551 [ Links ]
32. Wei G, Arya R, Ritz ZT, He A, Ohman-Strickland PA, McCoy JV. How does emergency department crowding affect medical student test scores and clerkship evaluations? West J Emerg Med 2015;16(6):913-918. https://doiorg/10.5811/westjem.2015.10.27242 [ Links ]
33. Leszczynski P, Gotlib J, Kopanski Z, Wejnarski A, Swiezewski S, Galazkowski R Analysis of web-based learning methods in emergency medicine: Randomised controlled trial. Arch Med Sci 2018;14(3):687-694. https://doiorg/10.5114/aoms.2015.56422 [ Links ]
34. Morphet J, Hood K, Cant R, Baulch J, Gilbee A, Sandry K. Teaching teamwork: An evaluation of an interprofessional training ward placement for health care students. Adv Med Educ Pract 2014;5:197-204. https://doi.org/10.2147/AMEP.S61189 [ Links ]
35. Carr SE, Celenza A, Lake F. Designing and implementing a skills program using a clinically integrated, multi-professional approach: Using evalution to drive curriculum change. Med Educ Online 2009;14(14). https://doi.org/10.3885/meo.2009.F0000221 [ Links ]
36. Cook DA, Bordage G, Schmidt HG. Description, justification and clarification: A framework for classifying the purposes of research in medical education. Med Educ 2008;42(2):128-133. https://doi.org/10.1111/j.1365-2923.2007.02974.x [ Links ]
37. Krause C, Krause R, Krause R, Gomez N, Jafry Z, Dinh VA. Effectiveness of a 1-hour extended focused assessment with sonography in trauma session in the medical student surgery clerkship. J Surg Educ 2017;74(6):968-974. https://doi.org/10.1016/j.jsurg.2017.03.007 [ Links ]
38. Lian A, Rippey JCR, Carr PJ. Teaching medical students ultrasound-guided vascular access - which learning method is best? J Vasc Access 2017;18(3):255-258. https://doi.org/10.5301/jva.5000730 [ Links ]
 Correspondence:
Correspondence:
D T Hagemeister
hagemeisterdt@ufs.ac.za
Accepted 14 July 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}