










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Health Professions Education
versão On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.15 no.1 Pretoria Mar. 2023
http://dx.doi.org/10.7196/AJHPE.2023.v15i1.1629
RESEARCH
MB ChB fifth-year student response to e-learning in orthopaedic surgery during COVID-19
H A GamieldienI; N A KrugerII; R DeyIII
IMB ChB PG Dip HPE; Division of Orthopaedic Surgery, Department of Surgery, Faculty of Health Sciences, University of Cape Town, South Africa
IIBSc MB ChB, FRCS (Edin) PCS Orth (SA) PH Di pHPE; Acute Spinal Cord Injury Unit, Division of Orthopaedic Surgery, Department of Surgery, Faculty of Health Sciences, University of Cape Town, South Africa
IIIPhD, Division of Biomedical Engineering, Department of Human Biology, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. With the onset of the COVID-19 pandemic and the subsequent country-wide lockdown, South African (SA) universities were forced to quickly adapt to teaching that minimised or eliminated in-person contact. The pandemic period necessitated rapid changes to the way in which learning occurs and resulted in significant shifts in the academic environment. There is limited evidence in the literature to support e-learning in undergraduate orthopaedic training. This is the first study of its kind evaluating e-learning in orthopaedic surgery in a middle-to-low-income country.
OBJECTIVES. To identify the University of Cape Town fifth-year MB ChB cohort's attitudes towards the e-learning component of blended learning during the COVID-19 pandemic. It also aimed to investigate whether e-learning facilitates comparable levels of confidence and results among students and face-to-face methods.
METHODS. Multi-year cross-sectional survey analysis was completed by retrospectively analysing the students' end-of-block evaluations and end-of-block marks. Responses from the cohorts between 2016 and 2020 were compared.
RESULTS. Regarding course definition, workload, course organisation, intended preparation and course presentation, the 2020 cohort's responses were similar to those of previous years. The 2020 cohort agreed that the e-learning material was relevant; this response was higher than in previous years. They also agreed that the online practical sessions were useful and that the course stimulated more interest. Significantly, they also strongly agreed that the online course was easier to attend and participate in than in previous years. The 2020 cohort perceived the end-of-block assessment to be somewhat unreasonable; however, this cohort yielded similar grades compared with previous cohorts. Subjectively, the students' responses to e-learning were positive, as many of them welcomed the usefulness and stimulation of online media as a study tool. Students felt that more time should be made available to work through online material and that there was incongruity between the content taught and the content of the end-of-block assessments.
CONCLUSION. Subjectively, the students' responses to e-learning were positive, as many of them welcomed the usefulness and stimulation of online media. With comparable outcomes in terms of student confidence and final marks (compared with traditional teaching only), it further encouraged a move towards formulating a novel blended learning curriculum. With these positive findings, we were able to explore the possibilities of developing an e-learning course curriculum incorporating international blended learning practices, using locally sourced SA evidence-based literature to provide orthopaedic teaching relevant to our unique setting.
The study aimed at identifying the University of Cape Town (UCT) fifth-year MB ChB cohort's attitudes towards the e-learning component of blended learning during the COVID-19 pandemic. The findings of the cohort's end-of-block results are compared with the results in previous years.
This study investigates whether e-learning facilitates levels of confidence among students compared with face-to-face methods. Multi-year cross-sectional survey analysis was completed by retrospectively analysing the students' end-of-block evaluations and end-of-block marks. Responses from the cohorts of 2016 - 2020 were compared. Regarding course definition, workload, course organisation, intended preparation and course presentation, the 2020 cohort's responses were similar to those of previous years. The 2020 cohort agreed that the e-learning material was relevant, with a greater number in agreement than in previous years. They also agreed that the online practical sessions were useful. Compared with previous groups, the 2020 cohort agreed that the course stimulated more interest than prior courses. Significantly, they strongly agreed that the online course was easier to attend and participate in than in previous years. This cohort perceived the end-of-block assessment to be somewhat unreasonable; however, their grades were similar to those of previous cohorts. Subjectively, the students' responses to e-learning were positive, as many of them welcomed the usefulness and stimulation of online media as a study tool. Students felt that more time should be made available to work through online material and that there was incongruity between the content taught and the content of the end-of-block assessments. With comparable outcomes in student confidence and final marks, it further encouraged a move towards formulating a novel blended learning curriculum. Education is changing rapidly in South Africa (SA), and it has been forced to undergo a hurried shift so that students are able to progress. It is therefore vital that medical education evolves to accommodate these changes, while navigating the challenges of providing a blended learning curriculum that is accessible to all students.
With the onset of the COVID-19 pandemic and the subsequent country-wide lockdown, SA universities were forced to quickly adapt to teaching that minimised or eliminated in-person contact. The pandemic period necessitated rapid changes to the way in which learning occurs and has resulted in significant shifts in the academic environment. One of the most prominent and drastic changes has been an increased dependence on e-learning, which until now, has been auxiliary to the knowledge transfer process in health sciences education. Clinical skills are a crucial component required for the safe practice of medicine. However, in-person clinical education is essential to facilitate students' acquisition of skill proficiency and professional socialisation. It is argued that certain traditional classroom techniques, such as lectures, often fail to transfer crucial problem-solving techniques.[1] UCT's orthopaedic rotation consists of a shared 4-week rotation with general trauma. Prior to the COVID-19 pandemic, the block consisted of daily face-to-face lectures, which included demonstrations of physical examination skills. One of the changes brought about by the pandemic period in the UCT orthopaedic curriculum, was that consultants from respective specialties uploaded theoretical and clinical skills teaching videos to the UCT orthopaedics YouTube page.[2] The implementation and practice of these clinical skills were then demonstrated on patients in small groups in the outpatient clinic setting. Even though the process has presented numerous challenges - specifically in the SA context with regard to unequal internet and device access[3] - it has also provided concomitant insights into knowledge acquisition and the impact of the respective mediums that health science educators use to achieve desirable outcomes in assessments. However, the importance of this investigation - localised in an SA context - is demonstrated by the growing number of similar studies of the effects of blended and online teaching ushered in by the COVID-19 pandemic, such as the study by Ravat et al.,[4]which focused on outcomes of blended learning in physiotherapy students at the University of the Witwatersrand, Johannesburg, as well as a study conducted by Zimba et al.,[3] focusing on social work education. The aim of our study was to investigate the response of medical students in their fifth year to the e-learning component of the recently implemented blended learning approach, specifically in the orthopaedic block. This was achieved through a comparative analysis, using students' evaluations and assessment outcomes from previous years.
Current online media dominance means that blended learning is at the forefront of higher education teaching methods. As illustrated by López-Pérez et al.,[5]'a persistent concern in teaching is the aim to achieve a better outcome and to reduce the number of students dropping out ... achieving these goals might require a change in the teaching methods employed'. Blended learning, by allowing students more control and flexibility in their learning in relation to their personal circumstances, forms part of the natural progression in this constantly evolving process.[6] The goal of blended learning is to achieve a balanced curriculum, where a mix of e-learning and face-to-face teaching supports a logical progression of desired learning outcomes. Sangrá et al.[7]define e-learning as 'an approach to teaching and learning, representing all or part of the educational model applied, that is based on the use of electronic media and devices as tools for improving access to training, communication and interaction and that facilitates the adoption of new ways of understanding and developing learning'. Evaluating the quality of blended learning requires relating the aspects of such learning to the complete student experience, and establishing whether they agree that the e-learning and face-to-face aspects are complementary.[8-10]
The manner in which the fifth-year orthopaedic block is conducted at UCT, is a constantly evolving process subject to changes and adaptations intended to accommodate and facilitate optimal orthopaedic knowledge acquisition for an evolving and increasingly diverse student population. The insights provided by this study serve to further this critical and essential development, given that 'most of the continent's orthopaedic care is provided by non-specialists, which makes adequate training and transfer of knowledge and skills to general practitioners paramount, especially during medical school'.[8] Due to the relatively short period of time dedicated to orthopaedic training during the MB ChB programme - and a general under-emphasis on musculoskeletal training in medical education worldwide'[11,12] - it is vital that the orthopaedic block undergo constant revision and optimisation. This is to adequately prepare students for their roles as health practitioners, particularly those who may serve in areas of the country that are under-resourced or lack access to specialised orthopaedic care, which is largely centralised in main urban areas.[13] This article primarily aims to analyse fifth-year MB ChB students' perception of online learning during COVID-19 and compare it to face-to-face learning perspectives from the previous years. During the pandemic, learning predominantly took place online as a result of nationwide lockdowns to prevent the spread of the COVID-19 virus. All face-to-face lectures were converted to pre-recorded lectures available on YouTube, as well as demonstrations of relevant clinical skills that formed part of their core learning objectives.
Methods
Fifth-year students in UCT's MB ChB programme, who completed their orthopaedic rotation, were included in the study. The study size was determined by the number of students who completed the survey and end-of-block assessment. A total of 1 054 students' summative results and 924 end-of-block evaluations were analysed - the total number of students between 2016 and 2020; 89% of the students in our cohort completed the online evaluation. The data were collected from the student feedback online evaluations, and the results of their end-of-block summative assessments from 5 February 2016 to 15 December 2020.
The 2020 online evaluation was intended to measure and qualitatively assess the students' responses to the dynamic shift from traditional teaching methods to blended learning. Students were presented with an end-of-block online course evaluation consisting of 13 questions regarding their learning experience during the undergraduate orthopaedic training block. Prior to 2020, this evaluation included questions related to course material and delivery of the content, which would evaluate the general structure and benefit of the course to the student. The clinical groups completed the same or a similarly themed survey before COVID-19, which provided a source of data to compare the students' perceptions of the transition from traditional teaching methods to blended learning. The main differences between the evaluation in previous years and the evaluation in the 2020 pandemic year were the incorporation of questions regarding blended learning and e-learning. Examples of specific statements and questions relating to e-learning are, 'I listened to all the video-recorded lectures in the course', 'Do you think the lack of clinical training now will affect your ability to manage orthopaedic conditions after you have qualified?', 'Do you feel the practical skills videos were adequate to prepare you for hands-on procedures when you are qualified?', 'The practical skills demonstrated in the videos were useful and adequate to prepare me for orthopaedics at general practitioner level'. The responses to these questions were graded on a scale from 'strongly disagree' to 'strongly agree', with a positive response being the latter option. Students were also allowed to comment on each question to provide further insight into their unique experiences during the online learning phase. These comments were analysed to provide further information on the students' feelings toward the online learning experience.
All face-to-face lectures were recorded and uploaded to the department's orthopaedic YouTube page. No follow-up was required, as the data were collected and analysed retrospectively. The evaluations were completed at the end of every block on the UCT online VULA platform and the results were accessible to the administrators of the course. VULA is UCT's online resource portal for students and lecturers. A comparison between grades of multiple-choice questions (MCQs), objective structured clinical examination (OSCE) and total marks pre- and post-COVID was done. This allowed for an indication of the relationship between students' summative assessments and their perception of the new online learning platform, which also provided a quantitative correlation to aid in determining the efficacy or shortfalls of the programme. During the COVID-19 pandemic, the OSCE was conducted in the regular manner with 6 separate 7-minute stations; however, the MCQ assessments were completed from home on an online platform at a dedicated time.
A multiple cross-sectional analysis of the cohorts was done, and statistical analysis was performed. No a priori power analysis or sample size calculation was performed, as this was a retrospective study. The data were anonymised, with students using only their student numbers on the evaluations. The data are described in the form of central tendencies such as medians and ranges. Non-parametric tests were done for comparison (Mann-Whitney U-test), and the limit for all statistical significance was p<0.05. The primary outcome measurement was whether to assess if e-learning/blended learning facilitated comparable levels of confidence in relation to traditional face-to-face teaching methods, which was achieved at the end-of-block evaluation. Additionally, we were able to provide an objective measurement analysing end-of-block results during the new online learning curriculum and the previous traditional curriculum at UCT. The data set is a representation of UCT medical students and would need to be applied cautiously as a representation of other students in SA or abroad. The evaluation tool was not validated, but was the standard end-of-block evaluation used by the orthopaedic division at UCT since 2016.
The study was approved by the Human Research Ethics Committee of UCT (ref. no. 855/2020).
Results
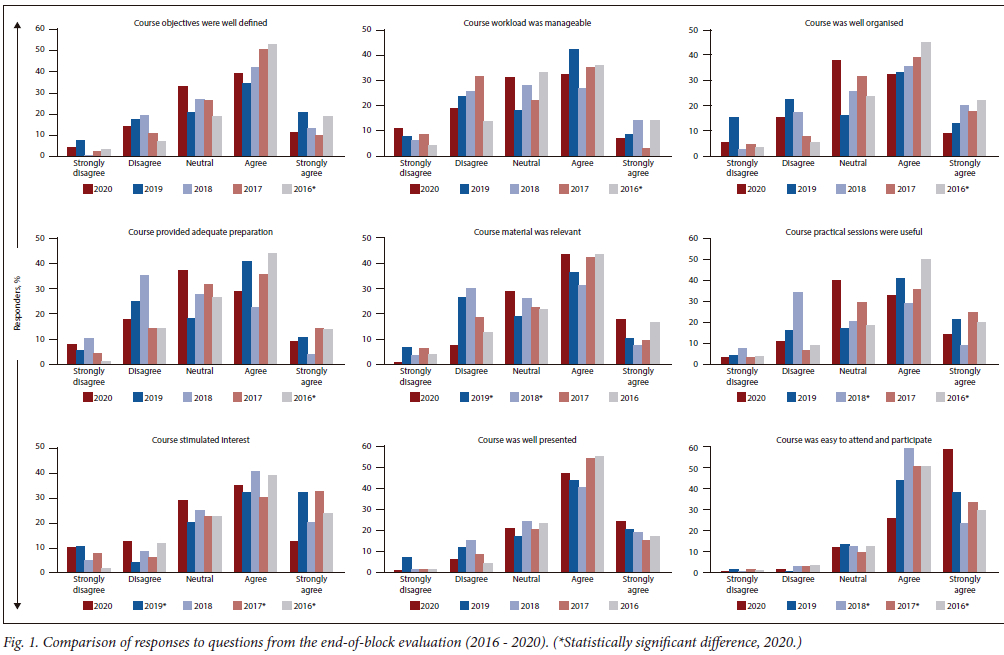
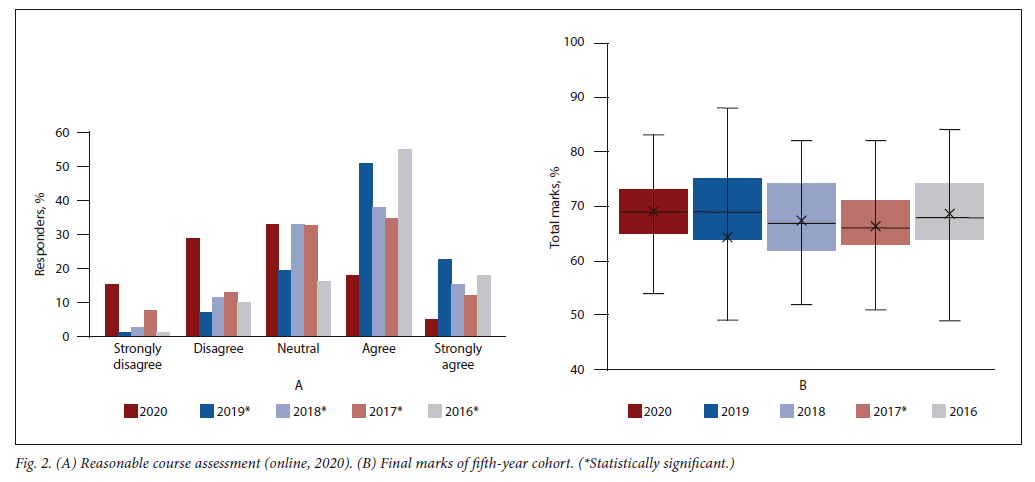
All the students from 2016 and 2020 replied to the online course evaluation questionnaires, while only 38%, 40% and 44% of the 2017, 2018 and 2019 cohorts, respectively, gave their feedback. In terms of course definition, workload, course organisation, intended preparation and course presentation, the 2020 cohort's response was similar to the responses of cohorts from recent years (Fig. 1). The 2020 cohort, compared with the 2019 and 2018 cohorts, agreed (p<0.05) that the material provided to them was more relevant. They also gave more agreeable responses (p<0.05) towards the usefulness of the practical sessions than the 2018 cohort. The 2020 cohort, compared with the 2019 and 2017 cohorts, agreed (p<0.05) that the course stimulated more interest. Interestingly, they also strongly agreed (p<0.05) that the online course was easier to attend and participate in compared with the 2018 and 2017 cohorts. The 2020 cohort strongly disagreed with the course assessment method employed for the online courses (Fig. 2). This response was significantly different from those of the other cohorts included in the study (p<0.05) (Fig. 1). Although the 2020 cohort was not agreeable with the mode of evaluation, their final marks were very similar to those of the rest of the cohorts and were only different (p<0.05) to those of the 2017 cohort (Fig. 2).
For the 2020 cohort, the classes were conducted online. Student responses from this cohort regarding the organisation and course material were very similar to those of previous years. The majority of the statistical differences observed was between the 2020 and 2016 cohorts for 8 of 10 questions. All of the statistical analyses described above are illustrated in Fig. 1.
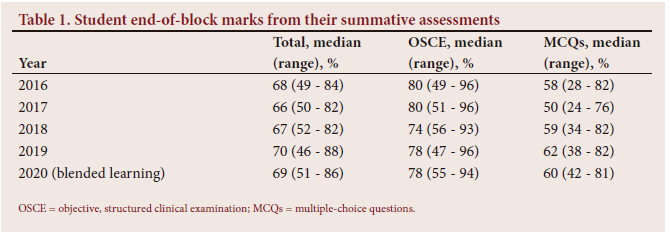
The median (range) marks obtained by the students over the years are presented in Table 1. The 2020 cohort's total marks were significantly different from those of the 2017 cohort. The 2020 cohort obtained significantly different OSCE and MCQ marks compared with the 2018, 2017 and 2016 cohorts. MCQs provide a more reliable modality of assessing an objective quantitative comparison between the pre- and post-COVID years. The MCQ assessment has greater reliability, as it is reproducible and consistent compared with the format of the oral-based OSCE summative assessment tool.[11] The OSCE and MCQ results of 2018 and 2019 show a similar correlation to the results of 2020. This demonstrates a comparable outcome of the results of assessing clinical skills and knowledge acquisition during the implementation of blended learning. Even though the MCQ assessment was completed online at home, there was no statistically significant difference in the outcome of the results. The responses to the open-ended questions regarding the blended learning curriculum are provided in Table 2. Students were given 2 questions: (i)The best features of the course were?; and (ii) The course could have been improved by? The overall impression of the best feature of the course was the overwhelmingly positive response to having the video-recorded lectures available online. This has shown to allow students to navigate through the content at their own pace, which further allows them to focus on content that they find either more relevant, or content that requires their attention to aid understanding. They also appreciated being able to use the textbook and watch the lectures regarding examination skills online simultaneously. When assessing their responses to how the course can be improved, the majority of the students requested more clinical exposure and practical teaching. The students found that there was a large disparity in the quality and content of teaching, depending on which clinician they were assigned to in the clinic. They suggested more formative assessments, clearer guidelines with regard to learning objectives and consideration for home circumstances with regard to using online platforms for teaching.
Discussion
Students appear to have responded adequately to the shift from traditional learning to blended learning. The convenience of online course material was generally welcomed and the usefulness of having the course content available electronically to be accessed at any time met with positive responses. It has been shown that a more conceptual change and novel techniques in information transmission strategies result in a more complete approach to teaching.[13-15] We have further demonstrated through comparing and observing the trend of the MCQ and OSCE marks that the relationship of the results between the two assessment methods has remained consistent. This indicates that not only do students display similar levels of knowledge acquisition, but the level of clinical skills acquisition is also similar, or possibly superior if one compares the results of 2018 with those during blended learning. However, some students were concerned that the lack of face-to-face teaching and clinical exposure may affect their skills as clinicians once they have qualified and practise independently in a primary care environment. The major disadvantage is the access to appropriate resources to facilitate online learning for all students. Access to stable and high bandwidth internet is not freely available off campus and not all students possess personal computers or laptops at home. UCT endeavoured to remedy these obstacles to learning by providing free laptops and mobile data to students during the time that the campus was placed into lockdown.
However, in utilising YouTube as a medium for uploading content, the department failed to consider that this would incur data charges as opposed to the UCT platform, Vula (which upon agreement between the university and some cellular networks, was free to use).[16]
The strength of this study is that, according to our knowledge, it is one of the first to scientifically assesses students' responses to e-learning in medical undergraduate orthopaedic teaching in SA. Despite being a retrospective study, the sample size was relatively large (> 1 000 students), with a response rate of 89% to the end-of-block evaluations. The major weakness is that a validated evaluation instrument was not used as the evaluation tool. Due to the retrospective nature of the data collection, this is a fixed variable that cannot be altered.
Despite a somewhat drastic shift in circumstances with the COVID-19 pandemic, which necessitated adequate adoption of blended learning (in other academic disciplines, online-only learning), existing infrastructure and familiarity with online platforms have facilitated vast improvements in the delivery of such learning with the use of new information and communication technology (ICT). Although, in many countries, educational institutions have previously employed some form of online learning, e.g. Spain, where since 2009, 92.5% of students have made use of institutional virtual teaching.[5] In the UK, studies have shown overwhelmingly positive student responses to blended learning and online course material, where the strengths of blended learning lie in factors such as increased access for students with disabilities, as well as flexible and more frequent access to content. This includes prerecorded lectures and presentations, allowing for student-controlled asynchronous online sessions.[14] Particularly, blended learning allows for the adaptation of a curriculum within context, with the recent COVID-19 pandemic being an example.[17-20] Blended learning is therefore a driver for transformative course redesign and permits the incorporation of team ideas and student feedback, which facilitates both immediate adaptation and long-term development. Transformative course design is seen as a core characteristic of blended learning.[21]
Despite these promising findings, it remains vital that specific and detailed study of the effects of blended learning occurs in diverse settings, particularly where resources are constrained, as in SA. Through this study and other research, blended learning has been shown to be particularly useful where student numbers are relatively high, as in MB ChB programmes in SA. Therefore, the application of blended learning curricula is effective in larger classes, where ICT is required to complement the face-to-face components of the course and compensates for the lack of targeted teaching that is more easily conducted in smaller cohorts. Statistics reveal that healthcare workers (HCWs) are distributed unevenly around the world. Low-need countries have high numbers of HCWs and those with higher needs have lower numbers of HCWs.'221 This crisis is far worse in sub-Saharan Africa and Asia. The World Health Organization has calculated a shortage of 7.2 million HCWs worldwide. In being integrated in developing countries, blended learning is beneficial to governments struggling to meet the demand of providing HCWs via traditional higher education means, given its lower delivery cost with increased scalability in undergraduate health sciences degrees. It also allows for improved access by students to course material and greater access to diverse experts who can contribute to teaching and novel curricula. However, when assessing the students' responses to the questions in the evaluations, it was evident that there remains a great desire and interest from the students for hands-on clinical, bedside learning to take place. Comments such as 'More contact learning, exposure to orthopaedic conditions and being able to practise techniques on patients' demonstrate that the current methods employed to facilitate the transferring of clinical skills via online media do not inspire sufficient confidence in students.
Doctors practising in an academic setting are required to take on many roles, such as that of clinician, educator, facilitator and examiner, to ensure that students are adequately prepared to provide a dignified clinical service. With the continuous development of education technology and the progressive evolution of student demographics, the role of the educator has evolved from the didactic, teacher-centred approach to a more complex constructivist approach focusing on self-directed and experiential learning. Technologically advanced, present-day students demand a higher-quality educational experience. Many forms of current teaching and assessment methods have merely been replicated from year to year, with little regard for evolving social conditions and changing levels of effectiveness. The COVID-19 pandemic has indeed brought about massive hardship and struggle throughout the world; however, it has necessitated the development of stronger teaching methods and highlighted the imperative of embracing technological advancements as opposed to either shying away from or remaining stoic about traditional methods of teaching - to the detriment of students. As highlighted by Cook and McDonald,[19] one should not view e-learning as inferior or superior to traditional instruction, but it should be seen as different and complementary. Each method can serve specific functions suited to its context. We have previously been guided by generalised frameworks provided by the university to structure courses; however, online learning necessitates the development of subject-specific content to ensure adequate training.[23] This change must be approached with the level of specificity required to account for the lack of in-person contact teaching in surgical interaction, clinical skills, such as reduction of fractures and application of casts, exposure to the examination of patients and core orthopaedic principles for the general practitioner.
Further research is required into the space of ICT accessibility in SA universities. The lack of access to infrastructure and resources required to fulfil all the requirements of an e-learning blended curriculum needs to be evaluated. Whether this method of teaching is sustainable for all students, in the context of university resources, should be investigated. Research must be grounded in and applicable to local experiences.
Conclusion
Subjectively, the studentsf responses to e-learning were positive, as many of them welcomed the usefulness and stimulation of online media as a study tool. With comparable outcomes in terms of student confidence and final marks (compared with traditional teaching only), it further encourages a move towards formulating a novel blended learning curriculum. Students strongly agreed that the online course was more relevant, well presented and easier to participate in and attend. Medical students are faced with large volumes of complex learning material which, when presented with traditional methods, often do not optimise positive learning engagement as recommended by cognitive researchers and theorists. Active learning engagement improves knowledge gain and recall.[24,25] With our implementation of active learning pedagogies, students found the online resources experience more stimulating, facilitating active learning engagement in the clinical environment. Subjectively, the students felt they were inadequately prepared for the end-of-block examinations, but objectively, the results from the summative assessments were comparable with those of previous years. Even though e-learning does not substitute procedural and experiential teaching, it fosters independent student learning, which encourages lifelong learning.[26,27] Importantly, we have demonstrated that the acquisition of theoretical knowledge can be gained and grasped from online learning, as well as from clinical skills. With these positive findings we are able to explore the possibilities of developing an e-learning course curriculum incorporating international blended learning practices, using locally sourced SA evidence-based literature to provide orthopaedic teaching relevant to our unique setting.
The study is aimed at identifying the fifth-year MB ChB learnersf perceptions and impressions of online learning, specifically regarding orthopaedic surgery, and then correlating these subjective findings with the cohortfs end-of-block results to provide an objective measure. Through identifying specific strengths and weaknesses of online learning through the studentsf feedback, we can potentially construct a refreshed teaching programme in line with modern online electronic methods. The students are technologically advanced and consume large quantities of online information, which provides an opportunity to create a more efficient and dynamic learning environment. Thus, higher-quality graduates are produced, who are able to cope with the demand of the growing burden on primary healthcare.
The purpose of this study was to gain insight into developing a novel approach to undergraduate orthopaedic training through a blend of online learning and traditional methods. Currently, there are no data to verify the validity and efficacy of online learning in undergraduate orthopaedic training. COVID.19, with all the difficulties it has brought, has demanded innovative ways of ensuring that academic processes continue. With the data available from pre-COVID.19 (such as traditional teaching methods that include face-to-face lectures and patient simulation tutorials), end-ofblock evaluations and end-of-block results, we were able to compare these responses and grades with a completely new set of results from the online orthopaedic undergraduate curriculum during COVID.19. The results will guide our transition into a well-structured blended learning environment.
Future students will benefit from this study through identification of areas where improvements in the course implementation can be made. It will allow us to provide a well-balanced blended learning course and valuable data to further pursue the construction of a robust, well-validated and reliable modern undergraduate orthopaedic training programme. It will provide data specifically relevant to our local setting and may potentially serve as the catalyst to standardise an approach to orthopaedic undergraduate teaching in SA.
Declaration. None.
Acknowledgements. We acknowledge Ayesha Mahatey for assisting with proofreading and editing.
Author contributions. HG contributed to data analysis and writing of the manuscript; NAK contributed to data collection and editing of the manuscript; and RD contributed to data analysis.
Funding. None.
Conflicts of interest. None.
References
1. Coyne E, Rands H, Frommolt V, Kain V, Plugge M, Mitchell M. Investigation of blended learning video resources to teach health students clinical skills: An integrative review. Nurse Educ Today 2018;63:101-107. https://doi.org/10.1016/j.nedt.2018.01.021 [ Links ]
2. UCTeach Ortho. YouTube, 2022. https://www.youtube.com/channel/UCR__mzghDSTLZ32sBJ18Xow (accessed 18 January 2023). [ Links ]
3. Zimba Z, Khosa P, Pillay R. Using blended learning in South African social work education to facilitate student engagement. Soc Work Educ 2021;40(2):263-278. https://doi.org/10.1080/02615479.2020.1746261 [ Links ]
4. Ravat S, Barnard-Ashton P, Keller MM. Blended teaching versus traditional teaching for undergraduate physiotherapy students at the University of the Witwatersrand. S Afr J Physiother 2021;77(1):8. https://doi.org/10.4102/sajp.v77i1.1544 [ Links ]
5. López-Pérez MV, Pérez-López MC, Rodríguez-Ariza L. Blended learning in higher education: Students' perceptions and their relation to outcomes. Comp Educ 2011;56(3):818-826. https://doi.org/10.1016/j.compedu.2010.10.023 [ Links ]
6. Fyllos A, Kanellopoulos A, Kitixis P, et al. University students' perception of online education: Is engagement enough? Acta Inform Med 2021;29(1):4. https://doi.org/10.5455/aim.2021.29.4-9 [ Links ]
7. Sangrà A, Vlachopoulos D, Cabrera N. Building an inclusive definition of e-learning: An approach to the conceptual framework. Int Rev Res Open Distrib Learn 2012;13(2):145-159. https://doi.org/10.19173/irrodl.v13i2.1161 [ Links ]
8. Ginns P, Ellis RA. Evaluating the quality of e-learning at the degree level in the student experience of blended learning. Br J Educ Tech 2009;40(4):652-663. https://doi.org/10.1111/j.1467-8535.2008.00861.x [ Links ]
9. Liu Q, Peng W, Zhang F, Hu R, Li Y, Yan W. The effectiveness of blended learning in health professions: Systematic review and meta-analysis. J Med Internet Res 2016;18(1):e4807. https://doi.org/10.2196/jmir.4807 [ Links ]
10. Mašić I, Novo A, Kudumović M, et al. Web based distance learning at Faculty of Medicine of Sarajevo University. Bosnian J Basic Med Sci 2006;6(2):71. https://doi.org/10.17305/bjbms.2006.3178 [ Links ]
11. Held MF, Laubscher M, Graham SM, et al. Topics, skills, and cases for an undergraduate musculoskeletal curriculum in southern Africa: A consensus from local and international experts. J Bone Joint Surg Am 2020;102(3):e10. https://doi.org/10.2106/JBJS.19.00664 [ Links ]
12. Dachs R, Roche S, Vrettos B, et al. Assessing musculoskeletal training in South Africa. S Afr Orthop J 2014;13(3):57-63. [ Links ]
13. Dell A, Gray S, Fraser R, Held M, Dunn R. Orthopaedic surgeon density in South Africa. World J Surg 2018;42(12):3849-3855. https://doi.org/10.1007/s00268-018-4709-4 [ Links ]
14. Wass V, van der Vleuten C, Shatzer J, Jones R. Assessment of clinical competence. Lancet 2001;357(9260):945-949. https://doi.org/10.1016/S0140-6736(00)04221-5 [ Links ]
15. Trigwell K, Prosser M, Ginns P. Phenomenographic pedagogy and a revised approaches to teaching inventory. High Educ Res Dev 2005;24(4):349-360. https://doi.org/10.1080/07294360500284730 [ Links ]
16. Patil N, Chan Ho Yan Y. SARS and its effect on medical education in Hong Kong. Med Educ 2003;37(12):1127-1128. https://doi.org/10.3946/kjme.2016.30 [ Links ]
17. Swaminathan N, Ravichandran L, Ramachandran S, Milanese S. Blended learning and health professional education: Protocol for a mixed-method systematic review. J Educ Health Promot 2020;9:46. https://doi.org/10.4103/jehp.jehp_489_19 [ Links ]
18. University of Cape Town. Zero-rated mobile data access to specific UCT online resources. http://www.icts.uct.ac.za/Zero-rated-access-some-UCT-websites (accessed 18 January 2023). [ Links ]
19. Sharpe R, Benfield G, Roberts G, Francis R. The undergraduate experience of blended e-learning: A review of UK literature and practice. High Educ Acad 2006:1-103. [ Links ]
20. Vallée A, Blacher J, Cariou A, Sorbets E. Blended learning compared to traditional learning in medical education: Systematic review and meta-analysis. J Med Internet Res 2020;22(8):e16504. https://doi.org/10.2196/16504 [ Links ]
21. De Jong N, Savin-Baden M, Cunningham AM, Verstegen DML. Blended learning in health education: Three case studies. Perspect Med Educ 2014;3(4):278-288. https://doi.org/10.1007/s40037-014-0108-1 [ Links ]
22. Ngan OMY, Tang TLH, Chan AKY, Chen DM, Tang MK. Blended learning in anatomy teaching for non-medical students: An innovative approach to the health professions education. Health Professions Educ 2018;4(2):149-158. https://doi.org/10.1016/j.hpe.2017.11.001 [ Links ]
23. Ortiz PA. Teaching in the time of COVID-19. Biochem Molec Biol Educ 2020;48(3):201. https://doi.org/10.1002/bmb.21348 [ Links ]
24. Garrison DR, Kanuka H. Blended learning: Uncovering its transformative potential in higher education. High Educ 2004;7(2):95-105. https://doi.org/10.1016/j.iheduc.2004.02.001 [ Links ]
25. George PP, Papachristou N, Belisario JM, et al. Online eLearning for undergraduates in health professions: A systematic review of the impact on knowledge, skills, attitudes and satisfaction. J Glob Health 2014;4(1). https://doi.org/10.7189/jogh.04.010406 [ Links ]
26. Cook DA, McDonald FS. E-learning: Is there anything special about the 'E'? Perspect Biol Med 2008;51(1):5-21. https://doi.org/10.1353/pbm.2008.0007 [ Links ]
27. Almarzooq Z, Lopes M, Kochar A. Virtual learning during the COVID-19 pandemic: A disruptive technology in graduate medical education. J Am Coll Cardiol 2020;75(20):2635-2638. https://doi.org/10.1016/j.jacc.2020.04.015 [ Links ]
 Correspondence:
Correspondence:
H Gamieldien
hammaad.gamieldien@gmail.com
Accepted 22 July 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}