










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.14 no.4 Pretoria dic. 2022
http://dx.doi.org/10.7196/AJHPE.2022.v14i4.1544
RESEARCH
The use of peer physical examination in undergraduate health professions education: Exploring the perceptions of students and educators in a multicultural, multiracial institution
A AdefuyeI; M HattinghII; M LabuschagneIII; J BusariIV
IMB ChB, MSc, PhD (Med); Division of Health Sciences Education, Office of the Dean, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIBSocSc (Nursing), PGDip, MHPE; Clinical Simulation and Skills Unit, School of Medicine, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIMB ChB, MMed, PhD (HPE); Clinical Simulation and Skills Unit, School of Medicine, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IVMB ChB, MHPE, PhD (HPE) Educational Development and Research Department, Faculty of Health, Medicine and Life Sciences, Maastricht University, The Netherlands
ABSTRACT
BACKGROUND. Teaching clinical skills is core content of the medical and allied health curricula of the Faculty of Health Sciences (FoHS) at the University of the Free State (UFS) in South Africa. A major pedagogical tool used for this purpose across the faculty is peer physical examination (PPE).
OBJECTIVE. To investigate the lived experience and perceptions of students and educators on the use of PPE in undergraduate health professions education at a multicultural and multiracial institution. Suggestions on guidelines for a PPE policy for the FoHS at the UFS were also obtained from the participants.
METHODS. This research was designed as a qualitative study that used focus group interviews involving 26 participants (19 students and 7 educators) to obtain verbal statements that described their experience and perceptions of the use of PPE in undergraduate health professions education.
RESULTS. Participants reported that PPE was useful to create a safe learning environment and to prepare students for the clinical aspects of their training. Enhancing students' empathy, competency and clinical confidence were among the advantages attributed to using PPE; it also encouraged peerassisted learning. Some of the disadvantages ascribed to PPE were that it made it difficult to maintain classroom discipline, and that it could promote memorisation over understanding. Finally, participants suggested that a guideline for PPE policy should address matters of consent, confidentiality, participation and gender, cultural, religious and racial considerations.
CONCLUSIONS. The findings of this study reveal that PPE is an acceptable and useful learning strategy for the majority of students and educators. Issues relating to consent, confidentiality and cultural, religious and racial considerations are some of the potential problems associated with the use of PPE at the UFS. We believe that the suggestions given by the participants of this study will inform the establishment of a PPE policy for the FoHS of the UFS.
The role of practical skills in daily clinical practice cannot be overemphasised. Hence practical clinical competence and competence-oriented training are often essential aspects of most medical curricula.[1] To ensure patient safety, it is expected that certain practical skills, such as physical examination, should have been mastered during undergraduate medical training.[1] While textbooks can describe the theoretical aspects of physical examination skills and signs, creative teaching techniques are required to translate theoretical knowledge into a more tactile experience for students.[2] Experiential learning is regarded as a key component of teaching clinical skills to medical students.[3] However, it has become increasingly challenging for educators to structure learning events for their students with patients, owing to factors such as shorter inpatient stay and patients' unwillingness to be examined by several students.[3,4
Strategies such as the use of clinical skills laboratories, increasing clinical attachments in ambulatory care, simulated patients, role play and peer physical examination (PPE) have been employed by some health sciences faculties to counteract this effect.[4] PPE is a pragmatic method of learning, during which students act as models for each other for the purpose of learning skills relating to physical examination, acquiring basic skills and practising simple, non-invasive procedures.[4] The rationale for using PPE in undergraduate health professions education is that PPE is cheaper than using simulated patients, that it promotes certain pedagogical advantages, such as enhanced opportunities to study normal anatomy and physiology, and that it helps to teach students empathy.[4,5] However, some ethical and topical issues relating to informed consent and duty of care, as well as to cultural, racial, ethnic and religious diversity, have been highlighted as some of the potential problems of using PPE in an ethnically diverse student population.[4] Furthermore, little is known about using PPE in a multicultural and multiracial medical faculty in Africa.
In this study, we explored students' and educators' lived experience and perceptions of the use of PPE in undergraduate health professions education in a multicultural and multiracial medical faculty in South Africa (SA). In addition, we obtained participants' opinions on what should be included in the guidelines for a policy on the use of PPE. We anticipated that obtaining empirical data on stakeholders' lived experience and perceptions of the use of PPE would reveal information about the effectiveness of this pedagogical tool for student learning and identify problematic areas, and could inform policy formation on the use of PPE in the faculty in the future.
Methods
This research was designed as a qualitative study that made use of focus group interviews (FGIs). It was decided to use FGIs because they are particularly appropriate for research into poorly understood or ill-defined topics, and where the researcher is interested in the depth and richness of the information collected.[6]
Study population
The target population included all lecturers involved in teaching clinical skills through PPE as a pedagogy, in the different departments of the three schools (medicine, nursing and allied health) of the health sciences faculty at the University of the Free State (UFS). It also included students enrolled at the three schools who had had prior exposure to PPE. Purposive sampling was used to select participants (i.e. the researchers purposefully selected participants who had experience of the phenomenon being explored).[7] Participants were invited via email to participate in the FGIs, and the survey population consisted of individuals who, after reading and signing the informed consent forms, voluntarily agreed to participate in the study. The sample consisted of 26 participants (19 students and 7 educators) out of 45 potential candidates (32 students and 13 educators) approached. All participants received an invitation letter to participate in a FGI, which explained the aim of the study. The lecturers received their invitation via email, and follow-up telephone calls reminded them of the FGI. The students received their invitations from class representatives.
Data collection
For the purpose of this study, three separate FGIs (two for student participants and one for educators) were conducted using a predetermined interview guide. Arrangements for the date, time and venue of the FGIs were communicated to the participants via email and cellphone messages. The three FGIs were conducted between April 2016 and August 2016. FGI 1 was attended by 11 students and lasted 47 minutes, FGI 2 by 7 educators and lasted 53 minutes, and FGI 3 by 8 students and lasted 62 minutes. An independent facilitator acquainted with PPE and the interview guide directed the discussions, while one of the researchers acted as co-facilitator and took field notes. In addition, an independent observer was present to take field notes, including on the body language of participants, the atmosphere in which the FGIs took place, group dynamics and personal interpretations of the discussions.
At the beginning of each FGI, participants received a short introduction to the purpose of the study and were assured that there were no right or wrong answers, and that all contributions would be valued. All participants were requested to sign an informed consent document prior to data collection. All FGIs were conducted in the debriefing room of the Simulation and Skills Unit of the School of Medicine in the Francois Retief building, UFS. All activities during the FGIs were video- and audio-recorded after prior consent had been obtained from the participants. All voice and video recordings were downloaded to a computer that is password protected to ensure the safekeeping of the data.
The focus group interview guide
An interview guide developed for the purpose of this study comprised three open-ended questions:
(i) What are the experiences and perceptions of students regarding the use of PPE at the Faculty of Health Sciences (FoHS), UFS?
(ii) What are the experiences and perceptions of lecturers regarding the use of PPE at the FoHS, UFS?
(iii) What should be included in the guidelines for a policy on the use of PPE for the FoHS, UFS?
Question 1 was presented to participants in FGIs 1 and 3, while question 2 was presented to participants in FGI 2. Question 3 was presented to participants in all three FGIs (1, 2 and 3).
Exploratory interview
An exploratory interview was conducted prior to the official start of data collection, with two participants (one student and one educator) using the interview guide. Participants of the exploratory interview were selected from the list of individuals who had voluntarily agreed to participate in the study. The exploratory interview was done to establish the feasibility of the chosen data collection method, congruity of the interview guide and the estimated duration of the FGI. Adjustments were made to the interview guide based on the recommendations of these participants. The data generated from the exploratory interview were not included in the final data of the study.
Data analysis
One of the researchers transcribed the recorded FGIs. We used iterative inductive coding, and paid attention to patterns and emerging themes. All transcribed data were organised in students' and educators' audio-recorded documents, the complete transcript was read and re-read by the researchers to familiarise themselves with the content, units of meaning (codes) were generated from the transcribed data, generated units of codes were grouped into categories and major categories were grouped to form themes.[8,9]Themes were generated separately for each focus group and then compared to find similar themes. All the investigators confirmed the identified themes and sub-themes.
Ethical considerations
Ethics approval for the research project was obtained from the Health Sciences Research Ethics Committee at the UFS (ref. no. ECUFS 188/2015).
Results
Demographic profile of participants
Of the student participants in this study, female students accounted for 74% (n=14), while men made up only 26% (n=5). Of the educators, only 29% (n=2) were men, while women accounted for 71% (n=5). Seventy-four percent (n=14) of the student participants were white, 16% (n=3) were coloured and 11% (n=2) black. Attempts to recruit student participants representative of the Indian population were unsuccessful. Of the educators, 14% (n=1) were coloured and 86% (n=6) white.
At the time this study was conducted, the UFS was a parallel-medium university, i.e. lectures were presented separately in English and Afrikaans. More than half (58%; n=11) of the student participants studied in Afrikaans (i.e. were Afrikaans-speaking), while the remaining 8 students (42%) studied in English (i.e. were English-speaking). Similarly, 6 (86%) of the participating educators reported Afrikaans as their home language, while only 1 (14%) reported that their home language was English.
The majority (42%, n=8 and 47%, n=9) of the student participants were enrolled at the School of Medicine and School for Allied Health Professions, respectively, while only 11% (n=2) represented the School of Nursing. The majority (57%, n=4) of the educators taught in the School for Allied Health Professions, 29% (n=2) taught in the School of Medicine, and only 14% (n=1) taught in the School of Nursing.
Students' experience and perceptions of the use of PPE in undergraduate health professions education
To obtain data on student experience and perceptions of the use of PPE in undergraduate health professions education, participants were asked to respond to the question, 'What are your experiences and perceptions on the use of PPE at the FoHS, UFS?' Content analysis of students' responses yielded only one core theme, namely the value of PPE. Categories identified under this theme were the utility of PPE, advantages of PPE and disadvantages of PPE (Table 1). Building self-confidence and increasing competencies in clinical skills were among the major utilities and advantages of PPE that were highlighted by the participants, while lack of supervision was identified as a disadvantage.
Students' suggestions on what should be included in the guidelines for a policy on the use of PPE
Analysis of students' responses to the request to provide guidelines for a policy on the use of PPE for the faculty yielded three main themes, namely ethical considerations, student safety and student concerns (Table 2). Further analysis of these themes generated 13 subthemes (Table 2). The need to develop policies relating to certain aspects of giving consent, voluntary participation in PPE, respect and confidentiality, and ethical dilemmas emanated from the theme 'ethical consideration' (Table 2). Policies on students' safety during PPE sessions were discussed under the subthemes of supervision during PPE, disabled students and types of physical examinations that can be performed during PPE. Participants also expressed the opinion that the policy for PPE should address student concerns related to gender privileges, religious sensitivities, racial sensitivities, religious bias, exposure to variable techniques and the use of videos in PPE sessions.
Educators' experience and perceptions of the use of PPE in undergraduate health professions education
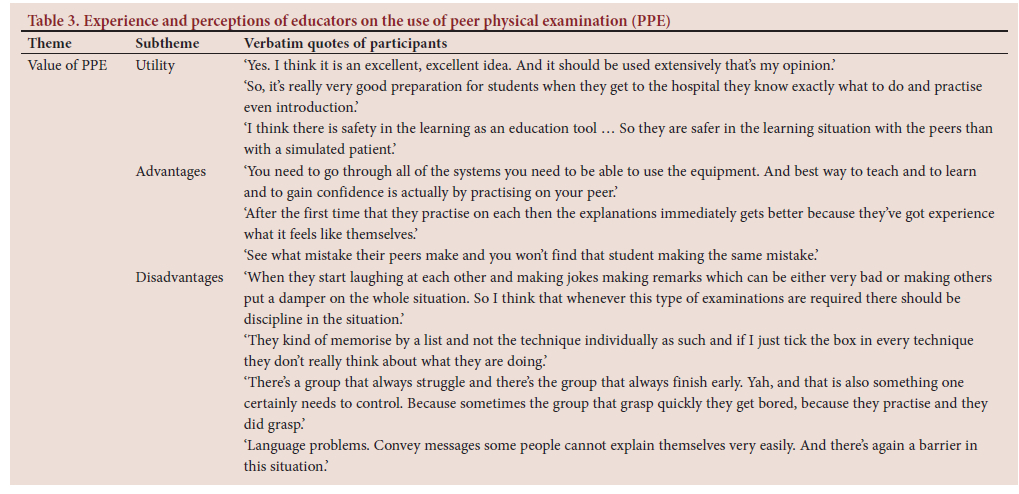
All the educators were united in their support of using PPE to enhance teaching and learning of clinical skills in undergraduate education. The educators were of the opinion that PPE was an excellent idea, that it is safe, and that it can help prepare students for the clinical environment (Table 3). The educators identified a lack of class discipline during PPE sessions and poor communication due to language barriers as some of the disadvantages of using PPE (Table 3).
Educators' suggestions on what should be included in the guidelines for a policy on PPE
Analysis of educators' suggestions regarding guidelines for a policy on PPE yielded three main themes: ethical considerations, student safety and miscellaneous. Regarding ethical considerations, the educators highlighted the need for a policy on detailed consent, indemnity (which was already in use in some departments), compulsory student participation, privacy and what to do in the case of certain ethical dilemmas (Table 4). Regarding student safety, educators reported that statements forbidding students to perform PPE without supervision, and specifications on the types of examination that were allowed, should be included in the policy guidelines (Table 4). Preferences related to gender, religion, culture and other beliefs were the categories discussed by the educators and allocated to the theme miscellaneous.
Discussion
PPE is used by medical faculties all over the world to mitigate the challenges posed by teaching with patients.[10] This study investigated students' and educators' lived experience and perceptions of the use of PPE in undergraduate health professions education at a multicultural and multiracial medical faculty in SA. In addition, participants' opinions on guidelines for policy on PPE were obtained.
The majority (74%) of student participants in this study were female. The high ratio of female to male student participants (74:26) could be because most undergraduate students in the nursing and allied health professions faculties at the UFS at the time of study were female - similar to a finding in New Zealand, that the fields of practice of dietetics/nutrition, occupational therapy and nursing were dominated by women.[11] Moreover, a 2019 World Health Organization report on gender equity in the health workforce reports that women make up 70% of workers in the health and social sector.[12] The racial distribution of the participants, with the majority of the students and educators being white (74% and 86%, respectively) and Afrikaans-speaking (58% and 86%) is similar to findings by Van Zyl et al.[13] These findings depict the background of a historically white Afrikaans university.[14]
In comments about their experience and perceptions of the use of PPE, all the participants were unanimous in their support of PPE as an innovative strategy to teach clinical skills. This finding confirms that of similar studies conducted in India and Australia that report students' support of and preference for PPE as a teaching and learning tool in health professions education.[15,16] Participants of this study also reported that PPE is useful because it creates a safe learning environment for students, and prepares them for the clinical aspect of their training (Tables 1 and 3) - this finding is confirmed by the literature.[17,18] This suggests that PPE helps students to achieve learning outcomes by fostering a safe learning environment. It has been reported that having empathy facilitates patients' treatment, and improves their physical and psychosocial outcomes.[19] The therapeutic importance of empathy emphasises why health professions graduates need to possess empathy for clinical practice. Hands-on experience (such as PPE) has been suggested as a practical way to promote the development and use of this skill by students.[19] In the present study, students reported that developing empathy was an advantage of PPE (Table 1).
Though it is not directly related to competency, clinical confidence is the self-perceived ability to deal with clinical scenarios,[20] and it is an essential outcome of most health professions curricula. Participants of this study reported that an increase in self-confidence related to clinical practice was an advantage of PPE (Tables 1 and 3). In addition, they reported that PPE encouraged peer-assisted learning (Tables 1 and 3). Peer-assisted learning is known to promote active learning by students,[21] and this suggests that PPE can also promote active learning. Finally, other advantages attributed by the participants to the use of PPE were that it increased students' level of competency, and developed students' tactile skills (Tables 1 and 3).
According to the student participants of this study, poor supervision and feeling exposed were some the disadvantages of using PPE (Table 1). The complaint about poor supervision by this study's participants is echoed by other studies,[22,23] namely that medical and nursing students reported that poor supervision adversely affected their learning during their undergraduate training. It is not unlikely that poor student supervision during PPE could affect students' learning adversely. Good instructional supervision has been found to correlate positively with students' academic achievement[24] Therefore, we recommend that health professions educators who use PPE should be trained on instructional supervision methods. Moreover, the students suggested that a guideline for student supervision during PPE should be included in a PPE policy (Table 2).
Classroom discipline and management has been described as the process of keeping a class under control, so that students pay attention during lessons, and that teachers and students, and students among themselves, respect each other.[25] Establishing and managing classroom discipline is a prerequisite for active teaching and learning.[25] Educators who participated in this study reported a lack of classroom discipline during PPE as a disadvantage (Table 3). This suggests that a lack of classroom discipline during PPE may precipitate passive learning, or no learning. Hence, it is proposed that educators who use PPE as a teaching tool must be trained on strategies to achieve and manage classroom discipline during PPE. In addition, educators said that PPE promotes memorisation over understanding; they believed that this was a disadvantage of PPE (Table 3). Memorisation is defined as a surface approach to learning that generates a fragmented knowledge base, and is characterised by the intention to memorise facts and information, and to recite facts in response to questions.[26] This suggests that using PPE can nurture a surface approach to learning, and the acquisition of fragmented knowledge.
Students admitted into the UFS, and also the FoHS, represent a variety of racial groups, and have a variety of home languages. Language barriers in the classroom are increasingly being recognised as a major hindrance to effective learning. While much of the discussion on the effect of language barriers on learning in the SA context focuses on the difficulties caused by teaching and learning in languages that are not one's mother tongue (i.e. home language),[27] little is known about how language affects peer-assisted learning. Educators who participated in this study reported that language barriers between students led to ineffective communication that hindered peer-assisted learning.
It has been reported that using PPE can produce unexpected, complex problems, which can only be managed effectively by establishing and enforcing a PPE policy.[4,10] In their suggestions for guidelines for a policy on PPE, participants of the present study said that informed consent should be detailed, mutual (obtained from both students who agree to perform PPE on each other) and must include withdrawal and indemnity clauses (Tables 2 and 4). This is in accordance with a report by Koehler et al.,[10] which found that issues of consent during PPE must be addressed in a policy that states that consent should be written and can be withdrawn at any time and without a reason. Other suggestions on best practice for PPE include that participation in PPE should be voluntary and non-coercive.[4] This view was shared by the students of the present study (Table 2), while the educators advocated for compulsory participation (Table 4). According to the educators, students were aware, before choosing a medical career, that taking part in PPE was an essential component of their training. Students who decide against participation in PPE should be reminded that participation in PPE engenders competency regarding physical examination prior to examining real patients.[10]
Confidential information can be revealed at any stage during PPE, and confidentiality breaches are a possibility. Students and educators must keep information obtained during PPE confidential, and addressing such breaches is crucial. Hence, confidentiality should be an integral component of a PPE policy.[10] Students who participated in this study suggested that matters relating to confidentiality should be clearly stated and emphasised in the proposed PPE policy (Table 2). Participants also suggested that the proposed policy should address ethical dilemmas, such as procedures and processes to follow when abnormal findings are made during PPEs.
In the past, most school-based problems were settled out of court, as they were often viewed as domestic.[28] However, increasing politicisation of education and citizens' greater awareness of their Constitutional, legal and fundamental human rights necessitate that educators and school administrators are aware of the legal implications of their work.[28] Violations of human rights by schools have been reported to have a multidimensional impact upon
students' academic performance and personality development.[29] Hence educators and school administrators have been enjoined to find ways to prevent violation of human rights in schools. Educators who participated in this study advocated that steps to prevent violations of human rights should be included in a proposed PPE policy (Table 4). In addition, educators asserted that they also referred to the medicolegal risks posed by performing PPE outside the confines of the classroom and without supervision. Consequently, they suggested that rules to prevent students from performing PPE outside the confines of the classroom should be included in the PPE policy (Table 4).
A study that assessed medical students' attitudes to and comfort with PPE reported that the majority of students were opposed to examinations of intimate body parts.'[30] Participants (students and educators) of the present study proposed that the types of physical examination that are permitted during PPEs should be set out in the PPE policy (Tables 2 and 4). Schools should clearly preclude examination of intimate parts of the body during PPE.'[4,10]
Despite rhetorical commitments to promote non-racialism and an all-inclusive society - the so-called rainbow nation - issues relating to ethnicity, cultural diversity and race remain ever-present in contemporary SA.[31,32] Consequently, participants commented on the need for guidelines to address matters of gender privilege/preferences, and religious, cultural and racial sensitivity/bias (Tables 2 and 4). In a multicultural and multiracial institution, cultural, religious and gender differences could serve as barriers to the use of PPE as a useful learning strategy[4] - as some participants of this study confirmed. Students claimed that PPE created undesirable outcomes such as gender favouritism (PPE favours women over men - male students are used as practice subjects most of the time); unfair religious/cultural biases (only students whose religion and culture permit it serve as practice subjects); and racial/gender segregation (students want to be examined only by a student of the same race or gender). Discussions on the cultural, racial and religious implications of PPE should be part of ongoing dialogue with faculty members and an ethnically diverse student population.[4] Other suggestions made by students in this study relate to the need for guidelines to address intervariability in physical examination techniques of educators, and using video-assisted teaching. Video demonstration could supplement traditional methods of teaching clinical skills, but is unlikely to be a sufficient substitute[33, 34]
Conclusion
PPE is reported to be broadly accepted as a useful learning strategy by the majority of students and educators.[4] Similarly, participants of this study acknowledged the utility and advantages of using PPE to teach clinical skills. However, despite its many advantages, participants identified certain disadvantages of using PPE, and indicated that issues relating to consent, confidentiality and cultural, religious and racial considerations were some of the potential problems associated with PPE. This confirms findings reported in the literature.[4] It is suggested that these problems can be effectively managed by creating and applying a PPE policy and procedure.[10] Hence, participants of this study suggested guidelines for a policy on PPE for the FoHS, UFS, and it is anticipated that suggestions given by the participants of this study will inform the establishment of a PPE policy. We propose that similar studies should be undertaken at other racially and culturally diverse institutions in SA, to get a holistic perspective on the views of students and educators on the use of PPE. An open-ended questionnaire would be valuable in reaching a large population of students and educators. A policy on the use of PPE is likely to enhance students' experience in clinical skills classrooms, and ensure the ethical use of PPE as a teaching technique.
Declaration. None.
Acknowledgements. The researchers wish to thank all the University of the Free State Faculty of Health Sciences students and staff who participated in this study.
Author contributions. AA collated and analysed the data and wrote the manuscript, MH conceptualised the study and collected data, ML supervised the execution of the study and reviewed the manuscript, and JB reviewed the manuscript and provided expert input.
Funding. None.
Conflicts of interest. None.
References
1. Hoefer SH, Sterz J, Bender B, et al. Conveying practical clinical skills with the help of teaching associates -a randomised trial with focus on the long-term learning retention. BMC Med Edu 2017;17(1):65. https://doi.org/10.1186/s12909-017-0892-5 [ Links ]
2. Gormley GJ, Murphy P. Teaching clinical skills in the theatre of medicine. Perspect Med Educ 2018;7(4):226-227. https://doi.org/10.1007/s40037-018-0445-6 [ Links ]
3. Hudson J, Ratnapalan S. Teaching clinical skills with patient resources. Can Fam Physician 2014;60(7):674-677. https://www.cfp.ca/content/cfp/60/7/674.full.pdf (accessed 26 February 2021). [ Links ]
4. Outram S, Nair BR. Peer physical examination: Time to revisit? Med J Aust 2008;189(5):274-276. https://www.mja.com.au/system/nles/issues/189_05_010908/out11362_fm.pdf (accessed 15 January 2021). [ Links ]
5. Hattingh MGM. The experiences and attitudes of students and lecturers regarding peer physical examination in the Faculty of Health Sciences at the University of the Free State. Mini-dissertation. Bloemfontein: University of the Free State, 2017. [ Links ]
6. Stalmeijer RE, McNaughton N, Van Mook WN. Using focus groups in medical education research. Med Teach 2014;36(11):923-939. https://doi.org/10.3109/0142159X.2014.917165 [ Links ]
7. Maree K. First Steps in Research. Bellville: Van Schaik, 2016. [ Links ]
8. Kekeya J. Analysing qualitative data using an iterative process. Contemp PNG Stud 2016;24:86-94. https://search.informit.org/doi/epdf/10.3316/informit.220284691031027 [ Links ]
9. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval 2006;27(2):237-246. https://doi.org/10.1177%2F1098214005283748 [ Links ]
10. Koehler N, Currey J, McMenamin C. what should be included in a peer physical examination policy and procedure? Med Sci Educ 2014;24(4):379-385. https://doi.org/10.1007/s40670-014-0068-4 [ Links ]
11. Grant VJ, Robinson E, Muir P. Sex ratios in healthcare occupations: Population-based study. BMJ 2004;328(7432):141-142. https://doi.org/10.1136/bmj.328.7432.141 [ Links ]
12. Boniol M, McIsaac M, Xu L, Wuliji T, Diallo K, Campbell J. Gender equity in the health workforce: Analysis of 104 countries. Geneva: World Health Organization, 2019. [ Links ]
13. Van Zyl G, Adefuye A, Bezuidenhout J. Factors affecting academic performance in anatomical sciences at a South African university: Students' perspectives. Afr Educ Rev 2019:1-22. https://doi.org/10.1080/18146627.2019.1596748 [ Links ]
14. Breier M, Wildschut A. Changing gender profile of medical schools in South Africa. S Afr Med J 2008;98(7):557-560. https://hdl.handle.net/10520/EJC69281 (accessed 10 December 2020). [ Links ]
15. Manjunath H, Venkatesh D, Taklikar R, Vijayanath V. Medical students' perception and preferences about peer physical examination (PPE). Asian J Health Sci 2014;2(1):42-44. https://doi.org/https://doi.org/10.15419/ajhs.v2i1.423 [ Links ]
16. Vaughan B, Grace S. Perception of peer physical examination in two Australian osteopathy programs. Chiropr Man Therap 2016;24(1):21. https://doi.org/10.1186/s12998-016-0102-2 [ Links ]
17. Braunack-Mayer AJ. Should medical students act as surrogate patients for each other? Med Educ 2001;35(7):681-686. https://doi.org/10.1046/j.1365-2923.2001.00970.x [ Links ]
18. Rees CE, Bradley P, Collett T, McLachlan JC. 'Over my dead body?': The influence of demographics on students' willingness to participate in peer physical examination. Med Teach 2005;27(7):599-605. https://doi.org/10.1080/01421590500237671 [ Links ]
19. Pohontsch N, Stark A, Ehrhardt M, Kötter T, Scherer M. Influences on students' empathy in medical education: An exploratory interview study with medical students in their third and last year. BMC Med Educ 2018;18(1):231. https://doi.org/10.1186/s12909-018-1335-7 [ Links ]
20. McNair R, Griffiths L, Reid K, Sloan H. Medical students developing confidence and patient centredness in diverse clinical settings: A longitudinal survey study. BMC Med Educ 2016;16(1):176. https://doi.org/10.1186/s12909-016-0689-y [ Links ]
21. Sukrajh V. The use of peer teaching to promote active learning amongst senior medical students Minidissertation. Stellenbosch: Stellenbosch University, 2018. [ Links ]
22. Dolmans D, Wolfhagen I, Heineman E, Scherpbier A. Factors adversely affecting student learning in the clinical learning environment: A student perspective. Educ Health 2008;21(3):32. https://media.proquest.com/media/hms/PFT/1/ZQ1KA?_s=FNzLAjkrL89d%2Ft9GmbNsjReoo4g%3D (accessed 16 June 2021). [ Links ]
23. Kamphinda S, Chilemba EB. Clinical supervision and support: Perspectives of undergraduate nursing students on their clinical learning environment in Malawi. Curationis 2019;42(1). http://www.scielo.org.za/scielo.php?pid=S2223-62792019000100009&script=sci_arttext&tlng=es (accessed 10 October 2020). [ Links ]
24. Usman YD. The impact of instructional supervision on academic performance of secondary school students in Nasarawa State, Nigeria. JEP 2015;6(10):160-167. https://files.eric.ed.gov/fulltext/EJ1081647.pdf (accessed 10 November 2021). [ Links ]
25. Konti F. Teachers and students perceptions towards teachers classroom management applications in primary schools. Procedia Soc Behav Sci 2011;15:4093-4097. https://doi.org/10.1016/j.sbspro.2011.04.503 [ Links ]
26. Pandey P, Zimitat C. Medical students' learning of anatomy: Memorisation, understanding and visualisation. Med Educ 2007;41(1):7-14. https://doi.org/10.1111/j.1365-2929.2006.02643.x [ Links ]
27. Banda F. The dilemma of the mother tongue: Prospects for bilingual education in South Africa. Lang Cult Curric 2000;13(1):51-66. https://doi.org/10.1080/07908310008666589 [ Links ]
28. Bassey SW, Arop F, Akpama E, Ayang E. School location and human rights violation in secondary school students' personnel administration in Cross River State, Nigeria. Int J Acad Res Progress Educ Dev 2012;1(2):199-210. https://www.aJol.info/index.php/lwati/article/view/79714 (accessed 5 February 2020). [ Links ]
29. Sofi MA. Violation of human rights in schools and its impacts on school going children at secondary level. Int J Adv Educ 2017;2(4):39-41. http://www.alleducationjournal.com/archives/2017/vol2/issue4 (accessed 15 April 2020). [ Links ]
30. Chang EH, Power DV. Are medical students comfortable with practicing physical examinations on each other? Acad Med 2000;75(4):384-389. https://journals.lww.com/academicmedicine/fulltext/2000/04000/are_medical_students_comfortable_with_practicing.20.aspx (accessed 16 October 2020). [ Links ]
31. Scheepers CLvW. Ethnicity, cultural diversity and poverty in South Africa: Archaeological perspectives from Iron Age Palestine. Old Testam Essays 2010;23(1):161-177. http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S1010-99192010000100009 (accessed 10 February 2020). [ Links ]
32. Seekings J. Race, discrimination and diversity in South Africa. Cape Town: Centre For Social Science Research, University of Cape Town, 2007. [ Links ]
33. Devi B, Khandelwal B, Das M. Comparison of the effectiveness ofvideo-assisted teaching program and traditional demonstration on nursing students learning skills of performing obstetrical palpation. Iran J Nurs Midwifery Res 2019;24(2):118. https://doi.org/10.4103%2Fijnmr.IJNMR_35_18 [ Links ]
34. George A, Blaauw D, Green-Thompson L, et al. Comparison of video demonstrations and bedside tutorials for teaching paediatric clinical skills to large groups of medical students in resource-constrained settings. Int J Educ Technol 2019;16(1):34.nhttps://doi.org/10.1186/s41239-019-0164-z [ Links ]
 Correspondence:
Correspondence:
A Adefuye
AdefuyeAO@ufs.ac.za
Accepted 17 February 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}