










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.14 no.4 Pretoria dic. 2022
http://dx.doi.org/10.7196/AJHPE.2022.v14i4.1218
RESEARCH
Perceptions of undergraduate allied health students of the clinical learning environment and clinical educators' attributes at the University of Ghana
J QuarteyI; K AcheampongII; S K KwakyeIII; J DankwahIV
IPhD Department of Physiotherapy, School of Biomedical and Allied Health Sciences, College of Health Sciences, University of Ghana, Accra, Ghana
IIBSc Komfo Anokye Teaching Hospital, Kumasi, Ghana
IIIBSc West Africa Football Academy, Sogakope, Ghana
IVBSc Sefwi Wiawso Government Hospital, Sefwi Wiawso, Ghana
ABSTRACT
BACKGROUND. Clinical education is a vital aspect of the education of health sciences students and consists of two components, i.e. the clinical learning environment and supervision.
OBJECTIVES. To determine the undergraduate allied health sciences students' perceptions regarding clinical educators' attributes and the clinical learning environment.
METHODS. This cross-sectional study included 169 undergraduate students, randomly recruited from various allied health professions programmes of the University of Ghana. The McGill clinical teacher evaluation tool and the clinical learning environment inventory were used to determine students' perceptions of clinical educators' attributes and the clinical learning environment, respectively. The Kruskal-Wallis test and independent t-tests were used to test for relationships between students' level and programme of study and their perceptions. The level of significance was set at 95%.
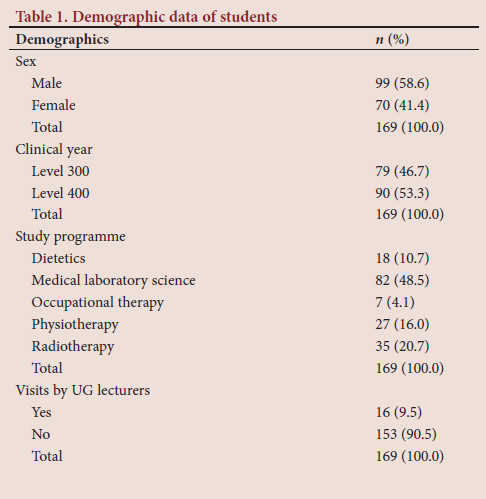
RESULTS. Of the 169 participants, there were 99 (58.6%) male students, 79 (46.7%) third-year students and 82 (48.5%) medical laboratory science students. Only 16 (9.5%) participants indicated visits by lecturers during clinical rotations. The third-year students had a statistically significant perception of their clinical learning environment (p=0.000), while the differences between perceptions of clinical learning environment among the various programmes were also statistically significant (p=0.028), but not for clinical educators' attributes (p=0.261).
CONCLUSION. Allied health sciences students have positive perceptions of their clinical learning environment and clinical educators' attributes. More frequent visits by lecturers to students during clinical rotations may ensure that student innovation is achieved in accordance with their classroom tuition.
Clinical learning comprises two parts, i.e. the clinical learning environment and supervision,[1] which is provided by clinical educators. The clinical learning environment is defined as the interactive network of forces influencing student learning outcome in the clinical setting.[2] However, a significant mismatch has been found between the preferred and actual learning environments of paramedical students.[3] Quality supervision[4] and the relationship between clinical educators and students[5] are also fundamental in successful clinical education. The clinical experience integrates academic study with competency development.[6] It is therefore important for clinical educators to train students in accordance with the growing challenges of combining evidence-based learning with the acquisition of clinical competencies.[7]
A conducive clinical learning environment contributes to a student's sense of safety, belongingness, perceived value and self-confidence.[8] A study by Williams et al.[3] revealed that allied health sciences students perceived students' satisfaction as the most important requirement for effective learning in the clinical learning environment. Meyers[9] reported that students viewed communication and personal interaction with their instructors as the most significant aspect of their learning. A survey among radiography students in Ghana showed that the majority of students perceived their clinical learning environment as satisfying and rich in learning experiences.[10] Physiotherapy students in Nigeria showed high ratings of clinical educators on important attributes, as measured by the McGill clinical teacher evaluation (CTE) tool.[11]
The education of allied health students of the University of Ghana is a 4-year intensive programme, followed by 1 year of clinical internship. Clinical training occurs in the third and fourth years. During the clinical years, students spend part of each semester and vacation in clinics, working under clinical supervisors, with regular visits by lecturers from the University of Ghana to streamline and guide teaching and learning. Some clinical year students commute between the main campus, which is ~15 km from the Korle-Bu Teaching Hospital where lectures are held, while some students live on Korle-Bu campus or in its environs in rented apartments due to inadequate accommodation. The journey to and from the main campus to attend lectures can be quite stressful and thus affect the learning process. The ongoing changes in healthcare needs, together with the increasing focus on evidence-based practice by health professionals, have transformed students' clinical experiences from 'learning by doing' to evidence-orientated learning.[12] Given its complex nature, understanding the experience from the perspective of the student may help to identify strategies to improve the learning process and facilitate engagement.[13] However, there is a paucity of information on the perceptions of students on the attributes of their clinical educators and the clinical learning environment. This study therefore aimed to determine undergraduate allied health professions students' rating of clinical educators' attributes and perceptions of the clinical learning environment.
Methods
This cross-sectional study was conducted at the Korle-Bu campus of the University of Ghana. Undergraduate clinical year (levels 300 and 400) allied health sciences students from the physiotherapy, occupational therapy, dietetics, medical laboratory sciences and radiography departments were recruited for the study. Clinical year students were recruited because they are engaged in clinical rotations, where they encounter real clinical situations while being supervised. First- and second-year students are usually mostly engaged in classroom activities involving courses that build theoretical knowledge in key areas of clinical practice. The University of Ghana has separate institutions for theoretical and clinical education, with bridging arrangements to facilitate clinical education. These bridging arrangement practices are visits by lecturers of the school to students on clinical rotation, as well as training seminars organised by the various allied health sciences departments for clinicians who are responsible for supervising students. Most of the clinicians have a master's degree or a higher degree, with a minimum of 4 years' clinical experience.
A sample size of 169 was calculated with the Taro Yamane formula: n=N/ [(1+N(e)2)],[14] where n = sample size required, N = number of people in the population (294) and e = allowable error (5%) at the 95% confidence level. A stratified sampling method was employed to determine the representation of each department in the sample, using the formula: (class size/population) χ sample size. Participants were then randomly recruited from each stratum, according to their proportions.
Data were obtained with a data capturing form (Appendix I: https://www.samedical.org/file/1887) for demographic details of participants, and two self-administered questionnaires, i.e. the McGill CTE tool (Appendix II: https://www.samedical.org/file/1887) and the clinical learning environment inventory (CLEI) (Appendix III: https://www.samedical.org/file/1887).
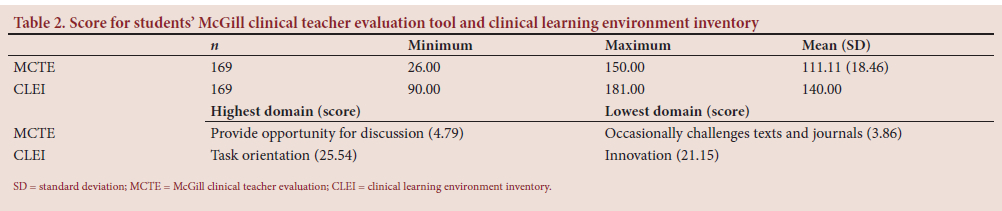
The McGill CTE tool, which takes about 10 minutes to complete, has been validated for assessing physician clinical tutors' effectiveness in previous studies.[15,16] It was the preferred tool for this study because all the items in the tool represent the behaviour expected of physiotherapy[11] and other allied health sciences clinical educators, and is scored on a 6-point Likert scale. It is a 25-item tool that lists attributes of effective clinical teachers, anchored on a 6-point Likert scale - from very strongly disagree (1), to very strongly agree (6). The higher the total agreement score on a particular attribute, the better the rating. A total mean agreement score >80 is considered a more positive rating of the attributes of clinical educators. A pilot study among Nigerian physiotherapy students yielded a reliability coefficient of 0.73 (0.05 alpha level of significance).[11]
The CLEI (Appendix III), adopted for this study, was developed in Australia for nursing students and has a reliability coefficient of 0.73. It is a 42-item tool, consisting of 6 subscales of clinical learning from students' perspectives. These scales are individualisation, innovation, involvement, personalisation, task orientation and satisfaction. Each question is scored on a 5-point Likert scale - from strongly disagree (1), to strongly agree (5). A mean score of >18 in a subscale indicates a positive perception of that subscale, and an overall mean rating of >110 indicates a positive perception of students regarding the clinical learning environment.
The nature and aim of the research were explained to participants via an information sheet, and they had to sign a consent form. Copies of the data-capturing form, McGill CTE tool and CLEI were distributed to students in their lecture halls and hostels. The questionnaires were retrieved from those who were able to complete them immediately and followed up at the lecture halls and hostels within 2 weeks for those who could not return them on the same day. Data were collected in the second semester of the 2017/2018 academic year over a 4-week period, from the middle of February to the middle of March 2018 after ethical clearance was obtained. Participants were assured of confidentiality by explaining the process of data collection to them. Questionnaires were number coded to ensure anonymity of participants. Completed questionnaires were filed under lock and key in the principal investigator's office cabinet. The data obtained were also entered onto Microsoft Office Excel 2013 (Microsoft Corp., USA) spreadsheets and stored on a password-protected computer accessible by the researchers only.
The data obtained were analysed using SPSS version 23.0 (IBM Corp., USA). Descriptive statistics such as means and percentages were used to summarise the data. The independent f-test was used to test for relationships between students' level of study and their perception of clinical educators' attributes, as well as the clinical learning environment. The Kruskal-Wallis test was used to test relationships between the programme of study and students' perceptions of their clinical educators' attributes and clinical learning environment. The level of significance was set at 95%.
Ethical approval
Ethical approval was obtained from the Ethics and Protocol Review Committee, School of Biomedical and Allied Health Sciences, University of Ghana (ref. no. SBAHS-PH/AKA/SA/2017-2018). Permission was obtained from the heads of the various departments included in the study.
Results
A total of 169 (93.9%) of 180 questionnaires distributed were completed and returned. The participants comprised 99 (58.6%) male students, 79 (46.7%) third-year students (level 300) and 82 (48.5%) medical laboratory science students (Table 1). Of the participants, ~10% indicated that lecturers visited them during their clinical rotations. The mean scores show a positive perception by students of their clinical educators' attributes and the clinical learning environment (Table 2).
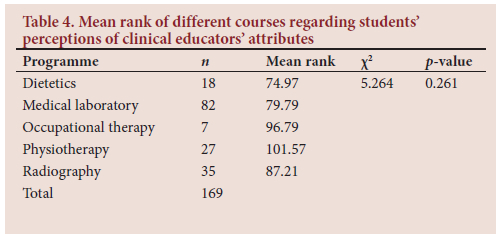
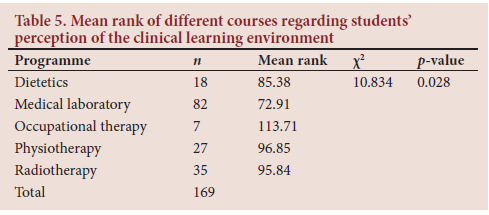
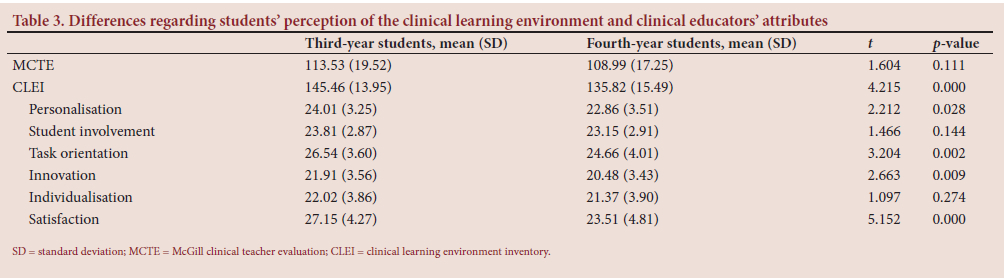
The third-year students' (level 300) perception of their clinical educators' attributes compared with that of fourth-year students (level 400) was not statistically significant (p=0.111); however, the third-year students had a statistically significant perception of their clinical learning environment (p=0.000) (Table 3). The differences between perceptions of clinical educators' attributes among the various programmes were not statistically significant (p=0.261) (Table 4), while those of the clinical learning environment were statistically significant (p=0.028) (Table 5).
Discussion
Two important bridging arrangements between the university and the hospitals, which provide clinical education, were assessed. Almost all the students indicated that they had never been visited during clinical placements. This revelation defeats the purpose of the arrangement, i.e. streamlining the tuition of students to ensure that clinicians instruct students in line with the latest evidence, as the students are taught in the classroom. Apart from occupational therapy participants, all of whom indicated that they had never been visited, participants from the other departments had varying responses, which may be due to the different locations of clinical placements, such as in- or outpatient departments. The workload of lecturers of the school is quite heavy and some hospitals are far from the university campus. These factors may have hampered the regularity of lecturers' visits or may have limited their visits to students in nearby hospitals.
The second bridging arrangement that was assessed was whether the various departments of the school organised formal training for clinical educators. The majority of participants was aware that clinical educators attended seminars and workshops on clinical education for students, which may have accounted for the overall high ranking of clinical educators' attributes. Similar findings, which ranked clinical educators high on the McGill CTE tool, were reported in Nigeria and Pakistan.[7,11]
The least ranked attribute in this study was 'my clinical teacher occasionally challenges points presented in text and journals', which alludes to a similar report by Ehsan et al.[7] in 2017. This report suggests that research-based evidence is not adequately used by the clinical educators who participated in this study and that students do not read recently published articles.
The highest rated attribute was 'my clinical teacher is usually readily available for discussion'. This indicates that students might have achieved benefit from such discussions, which probably translates into an association between what they see in the clinic and what they learn in the classroom or lecture hall. A study by Mulholland et al.'6] revealed that occupational therapy students appreciated an educator who challenged them appropriately and gave them constructive feedback during discussions, thus reaffirming the importance of discussions between clinical educators and their students.
The study also showed that the difference between the course pursued and the rating of clinical educators on the McGill CTE tool was not statistically significant, probably because the same clinicians who teach third- and fourth-year students also undertake clinical placement at their facilities.
The general positive perception of students' clinical learning environment implies that students consider it conducive to learning, which corroborates the finding by Kyei et al.[10] Bisholt et al.'[4] indicated that the task of the healthcare unit is to guarantee that the clinical placement offers adequate and appropriate learning opportunities to ensure maximum learning outcomes.
The highest rated domain was 'task orientation', probably because some of the hospitals where students are offered clinical placements have specialised units, and tasks are therefore clearly defined. The objectives for each placement are aligned with the tasks of the unit; therefore, there is improved facilitation of student learning. The lowest rated subscale was 'innovation', which indicates that most clinical learning environments are traditional in nature. This may be because clinicians prefer to adhere to established protocols or are not motivated to implement knowledge acquired from workshops and seminars regarding the most recent research and innovative approaches in their respective practices. The low level of innovation in the clinical learning environment raises questions, which may lead students to possibly query how to translate knowledge from classroom tuition to the clinic environment, which could also result in dissatisfaction during the clinical placement.
The results of this study indicate that the third-year students had a significantly better perception of their learning environment, with major differences in personalisation, innovation, task-orientation and satisfaction subscales. It is not clear why students of the same school have different perceptions of the learning environment, especially in the four different subscales, as clinical education takes place in similar environments for clinical year students in each department. It is imperative to note that intrinsic factors such as student motivation and interests may influence their perceptions, as nursing students reported that being in their senior years of study made them more critical because of their ability to better reflect on clinical practice.[1] They also have an improved understanding of the essential content of clinical practice,[16] which could be attributed to why allied health students in their fourth year perceived the clinical learning environment less positively than their colleagues in the third year.
There was a statistically significant difference in perceptions of the clinical learning environment among the students in the different programmes in the school. This may be due to the differences in clinical teaching adopted by each department and the differences in the nature of the job description of the respective professions. The student-clinical educator ratio could also be a contributory factor to the disparity observed, as occupational therapy students, whose perception was the most positive, are the smallest group, while medical laboratory science students, who reported the least positive perception, are the largest group in the school.
It also stands to reason that a positive perception of clinical educators' attributes and the clinical learning environment positively influences students' learning, because an ideal clinical education experience takes place in a learning atmosphere that allows for establishing a mutually beneficial student-supervisor relationship.[11] Furthermore, a conducive clinical learning environment contributes to a student's sense of safety, belonging, perceived value and self-confidence.[8]
Conclusion
Allied health sciences students have a positive perception of their clinical learning environment and their clinical educators' attributes. This study shows that the programme and level of study have a significant influence on students' perception of their clinical learning environment. However, the programme and level of study do not have a significant influence on students' perceptions of their clinical educators' attributes.
Further research could be carried out to determine the effect of factors such as sex of students and clinical educators, students' preferred learning styles and duration of rotation on the clinical learning environment. The perception of clinical educators regarding the attitudes of students could also be investigated. Frequent visits by lecturers to students during clinical placement could enhance innovation for students, while clinicians and students need to be encouraged to read recent journal articles.
Declaration. None.
Acknowledgements. We wish to express our profound gratitude to the School of Biomedical and Allied Health Sciences, College of Health Sciences, University of Ghana, for making it possible to perform this study. We are also grateful to all the undergraduate allied health sciences students who took part in the study for their immense contribution towards the study's success.
Author contributions. JQ and KA conceptualised the study and its design, and subsequently collected data. JQ, KA, SKK and JD contributed towards the data analysis, wrote the article and reviewed the manuscript for important intellectual content. JQ, KA, SKK and JD revised the draft and approved the final version of the manuscript for submission.
Funding. None.
Conflicts of interest. None.
References
1. Pitkänen S, Kääriäinen M, Oikarainen A, et al. Healthcare students' evaluation of the clinical learning environment and supervision - a cross-sectional study. Nurse Educ Today 2018;62:143-149. https://doi.org/10.1016/j.nedt.2018.01.005 [ Links ]
2. Papastavrou E, Lambrinou E, Tsangari H, Saarikoski M, Leino-Kilpi H. Student nurses' experience of learning in the clinical environment. Nurse Educ Pract 2010;10(3):176-182. https://doi.org/10.1016/j.nepr.2009.07.003 [ Links ]
3. Williams B, Brown T, Winship C. The mismatch between perceived and preferred expectations of undergraduate paramedic students. Internet J Allied Health Sci Pract 2012;10(4):12. https://doi.org/10.46743/1540-580X/2012.1422 [ Links ]
4. Bisholt B, Ohlsson U, Engström AK, Johansson AS, Gustafsson M. Nursing students' assessment of the learning environment in different clinical settings. Nurse Educ Pract 2014;14(3):304-310. https://doi.org/10.1016/j.nepr.2013.11.005 [ Links ]
5. Hall M, McFarlane LA, Mulholland S. Positive clinical placements: Perspectives of students and clinical educators in rehabilitation medicine. Int J Ther Rehab 2012;19(10):549-556. https://doi.org/10.12968/ijtr.2012.19.10.549 [ Links ]
6. Mulholland S, Derdall M, Roy B. The student's perspective on what makes an exceptional practice placement educator. Br J Occup Ther 2006;69(12):567-571. https://doi.org/10.1177/030802260606901206 [ Links ]
7. Ehsan S, Butt MS, Umar B. Perception of undergraduate physical therapy students regarding the clinical teaching attributes of their clinical instructors. Biomed Res 2017;28(3):1091-1094. [ Links ]
8. Maher J, Pelly F, Swanepoel E, Sutakowsky L, Hughes R. The contribution of clinical placement to nutrition and dietetics competency development: A student-centered approach. Nutr Diet 2015;72(2):156-162. https://doi.org/10.1111/1747-0080.12163 [ Links ]
9. Meyers SA. Do your students care whether you care about them? College Teach 2009;57(4):205-210. https://doi.org/10.1080/87567550903218620 [ Links ]
10. Kyei KA, Addo BM, Antwi WK, David N. Impact of clinical placement on radiography students in Ghana. Int J Med Res Health Sci 2014;3(4):819-824. https://doi.org/10.5958/2319-5886.2014.00007.1 [ Links ]
11. Oyeyemi A. Activities of the professoriate: A new perspective on scholarship. Afr J Physiother Rehab Sci 2009;1(1):37-40. https://doi.org/10.4314/ajprs.v1i1.51316 [ Links ]
12. Papastavrou E, Dimitriadou M, Tsangari H, Andreou C. Nursing students' satisfaction of the clinical learning environment: A research study. BMC Nurs 2016;15(1):44. https://doi.org/10.1186/s12912-016-0164-4 [ Links ]
13. Milanese S, Gordon S, Pellatt A. Undergraduate physiotherapy student perceptions of teaching and learning activities associated with clinical education. Physical Ther Rev 2013;18(6):439-444. https://doi.org/10.1179/1743288X12Y.0000000060 [ Links ]
14. Yamane T. Statistics, an Introductory Analysis. 2nd ed. New York: Harper and Row, 1967. [ Links ]
15. McLeod PJ. The student case presentation: An integral component of the undergraduate curriculum. Teach Learn Med 1991;3(2):113. https://doi.org/10.1080/10401339109539491 [ Links ]
16. Burford B, Morrow G, Rothwell C, Carter M, Illing J. Professionalism education should reflect reality: Findings from three health professions. Med Educ 2014;48(4):361-374. https://doi.org/10.1111/medu.12368 [ Links ]
 Correspondence:
Correspondence:
J Quartey
neeayree@googlemail.com
Accepted 10 March 2022.


{kind=link}
{kind=link}