










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.14 no.3 Pretoria sep. 2022
http://dx.doi.org/10.7196/AJHPE.2022.v14i3.1426
RESEARCH
Interactive learning objects as a solution to challenges in basic medical science teaching
L KeillerI; A AlblasII; J R FoiretIII; A V KeillerIV
IBSc, MPhil, PhD; Learning Technology Systems, Academic Information Technology, Stellenbosch University, South Africa
IIBSc Hons, MSc, PhD; Department of Clinical Anatomy, Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa
IIIBSc Hons; Centre for Health Professions Education, Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa
IVPGDip Centre for Learning Technologies, Stellenbosch University, South Africa
ABSTRACT
BACKGROUND. As a core component of any health professions curriculum, basic medical science modules facilitate learning of biology, anatomy, histology and physiology content. To redress the challenges of class size and poor tertiary education readiness, interactive learning objects could facilitate learning and enhance engagement between lecturers and students.
OBJECTIVE. To determine whether the use of learning objects in a basic medical science first-year module is an effective tool for enhancing the student learning experience.
METHODS. A case study research design with mixed methods of data collection was used. Participants provided informed consent for this study. Learning objects were incorporated into a basic medical sciences first-year module in the Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa. A correlation analysis between usage statistics and assessment results was used to determine the academic effectiveness of this intervention. A thematic network analysis identified the barriers and enablers of the intervention.
RESULTS. Student attempts at learning objects correlated with a higher assessment outcome for two of the three tutorials. Technical difficulties, timing and assessment format were barriers to learning with the use of learning objects. Enablers to learning included student enjoyment, facilitating understanding of core concepts, adaptation to new ways of learning and formative assessment. The module team received valuable feedback on the constructed learning environment through the qualitative data collected from students within this study.
CONCLUSION. Interactive learning objects are useful and effective tools for facilitating learning in the context of large, diverse first-year health professions education classes.
Health professions curricula are rapidly changing in response to recommended teaching approaches[1,2] and changes in biomedical knowledge.[3] One of the ways in which lecturers have responded to the need that these changes have created is to adopt a creative blended learning approach to teaching[4,5] in their curricula. Blended learning can be defined as 'optimising achievement of learning objectives by applying the 'right learning technologies' to match the 'right personal learning style' to transfer the 'right skills to the 'right person at the 'right time'.[6] This definition implies that there is no 'one-size-fits-all' approach, and requires lecturers to facilitate learning through various forms of feedback, interaction with the learning environment and reflection.[7]
Learning environments vary within the health professions, though one area of commonality across disciplines is that of basic medical sciences. As a core component of any health professions curriculum, basic medical science modules facilitate learning of biology, anatomy, histology and physiology content. In the Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa, the biomedical sciences department is responsible for teaching these components for all health professions education (HPE) disciplines as a foundational subject. First-year intake has increased in the last decade, and is expected to escalate exponentially going forward. There has, however, been no reciprocal increase in teaching staff, which precipitates the need for alternative, theoretically sound approaches to engaging with students without sacrificing academic quality. Adding to the challenges posed by the high student-to-staff ratio is the inequality in secondary education within the SA context,[8] which potentially hampers the transition of students from secondary to tertiary education. Despite the resource and environmental challenges, we attempted to identify mechanisms that would ensure facilitation of learning of the foundation phase biomedical sciences.
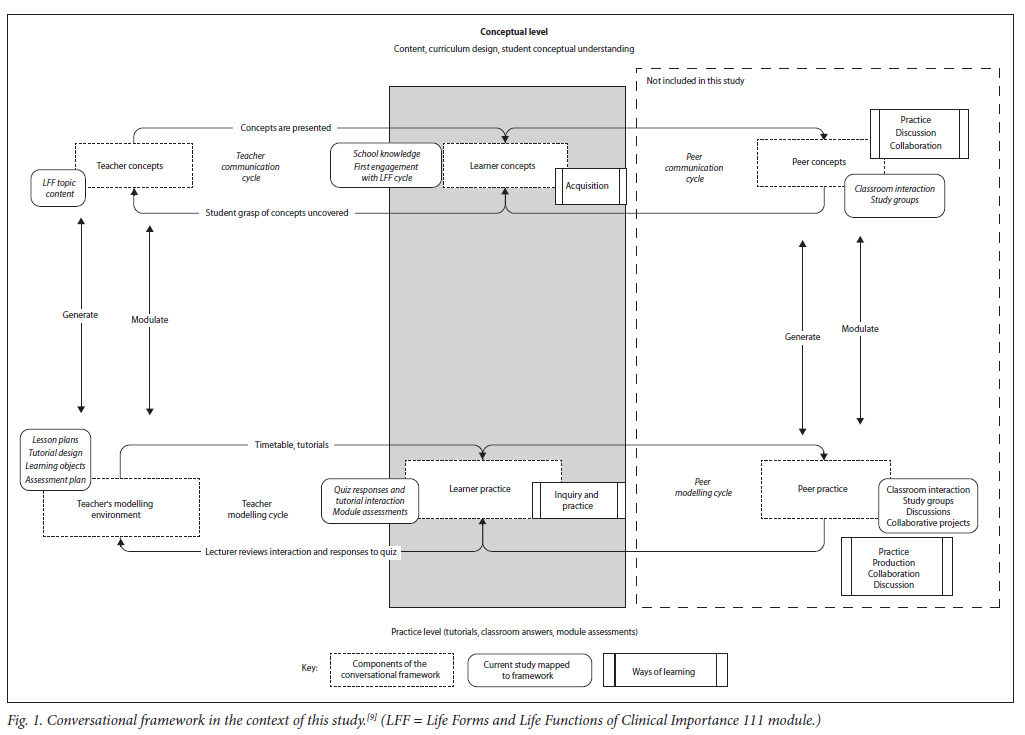
The conversational framework[9] highlights the notion that learning requires 'iterative, communicative, adaptive, reflective and goal-oriented action with feedback' to take place (Fig. 1).[9,10] In applying this framework to teaching design,[7] lecturers need to be aware of the ways in which students learn: acquisition, inquiry, practice, production, collaboration and discussion. Within this study, the applicable ways of learning are acquisition, inquiry and practice. Acquisition refers to a passive form of learning, engaging with didactic lectures, reading materials and other lecturer-selected resources. Inquiry guides a student through reflection, and requires the design of learning activities that facilitate intrinsic feedback. Finally, activities that include extrinsic feedback on conceptual understanding are useful for facilitating practice as a way of learning. Using learning objects could be a practical and sustainable mechanism for creating a learning environment that incorporates this iterative, communicative feedback. Interactive learning objects in the form of reusable shareable content object reference models (SCORMs) provide a potential mechanism for facilitating these ways of learning in a blended learning curriculum.[11] These types of learning activities are ideal for creating adaptive learning environments.[12] The conversational framework, and particularly these applicable ways of learning, were used to support the design and review of the use of SCORM-based learning activities to address the challenges of large classes and student understanding in basic medical sciences.
The Life Forms and Life Functions of Clinical Importance 111 (LFF) module team have tried to redress the challenges of class size and poor tertiary education readiness by revising knowledge presumed to be in place from secondary education at the onset of the module. In introducing interactive learning objects as tutorials for the first three biology topics (cytology, organismic kingdoms of medical importance and embryology) in the LFF module via the institutional Moodle-based learning management system (LMS), the aim was to support students' learning and comprehension by breaking up information into smaller conceptual components.[2,13] The research question guiding this study was: is the use of learning objects in a basic medical sciences first-year module an effective tool for enhancing the student learning experience, and, on a practical level, what are the barriers and enablers to the development and use of learning objects in the LFF module for academic staff and students?
Methods
As a result of the increasing student-to-staff ratio, and student feedback on the module in the 2 years preceding this study, this pilot study was designed using a descriptive case study methodology. The case study method supported the research team in developing a holistic view of the pilot intervention conducted here.[14] Institutional and ethics approval (ref. no. N16/05/069) was obtained for this study from Stellenbosch University. Participants included the module team, first-year students from the year preceding the study, and the first-year class within the study year. The conversational framework[7] served as the theoretical lens to understand the process of learning. A phased approach aligned to the conversational framework guided our quantitative and qualitative data collection.
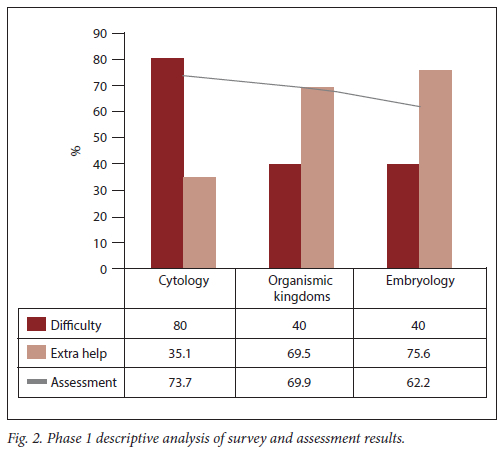
The conversational framework proposes that lecturers utilise the feedback provided by students on their learning experience to adapt (modulate) the content and design of their courses.[7] In phase 1, a paper-based survey was administered to the first-year cohort (n=369) from the year preceding the study. Using a Likert scale, students rated the difficulty of topics (1 = most difficult, 5 = least difficult) and need for additional support during the LFF module. The results of this survey were descriptively analysed. A review of summative assessment results for the preceding year's cohort was used to establish the need for the intervention and select the topics for the interactive tutorials.
Phase 2 of the study included converting the existing conceptual PowerPoint (Microsoft, USA) slides used in class into interactive tutorials using a software package (iSpring Suite; Microsoft, USA) published to the LMS as a SCORM activity. Tutorials included quizzes that would divert a student back to the content for revision based on incorrect answers, while students who answered correctly would progress to the next concept. Two members of the research team (JF, AVK) developed and designed the tutorials. This process aligns with the teacher concepts, modulating and generating the LFF content. A timesheet was used to record hours spent on creating all tutorials, providing data on implications for academic staff resources in adopting this approach.
The data collection and activities outlined above speak to the principles that underlie the conversational framework.[7] The design for learning should motivate learners to generate their own articulations/conceptual understanding and actions in a way that facilitates their modulation or understanding of concepts and practice. Adapting (modulating) his/her teaching and learning activities based on feedback (student generating), the teacher is able to set goals, which the student responds to in a constructivist approach, thus modulating their own practice (Fig. 1).
In phase 3, we introduced the learning objects in the biology component of the LFF module during the first semester. A blended approach to teaching included weekly compulsory learning objects for students to complete in parallel with the concepts taught in the classroom. The lecturer facilitated an information session during the first lecture with the students. This information session explained how these compulsory learning objects interact and align with the face-to-face lessons. Students received a grade for the learning objects on their first attempt, which contributed to continuous assessment within the module. Repeat attempts used as revision were not graded.
The lecturer downloaded and reviewed detailed interaction reports for each learning object. These were used to identify which concepts students struggled with, based on the assessment grades and time spent on working through that particular lesson. Where needed, the lecturer would include a short revision of that concept in the next class.
Data for phase 4 included a comparison of the marks of the two cohorts, the previous year (n=369) and current year (n=366), as well as a qualitative closed- and open-ended questions survey for students of the current cohort who consented to the questionnaire (n=52). We used a correlation analysis between usage statistics and assessment results to investigate the academic effectiveness of this intervention. Two researchers (LK, AA) independently applied a thematic network analysis approach,[15] with a combination of inductive (conversational framework) and deductive coding, to analyse the qualitative feedback from students. In the first round of analysis, each researcher created a codebook linked to the teacher concepts and student concepts, and any additional basic themes that arose from the data. The researchers compared basic themes to generate the organising themes. Final global themes emerged through discussion between all authors.
Results
Results are presented with reference to each phase, as described above.
Phase 1
A total of 35.5% (n=131) of the previous year cohort consented to participate in the survey relating to their perceptions of difficulty and need for additional resources in the LFF module. Cytology was perceived as the least difficult, while organismic kingdoms and embryology were perceived as being difficult concepts within LFF. Students identified embryology as the concept that most required extra online lessons (75.6%; n=99), followed by organismic kingdoms (69.5%; n=91) and cytology (35.1%; n=46) (Fig. 2).
Phase 2
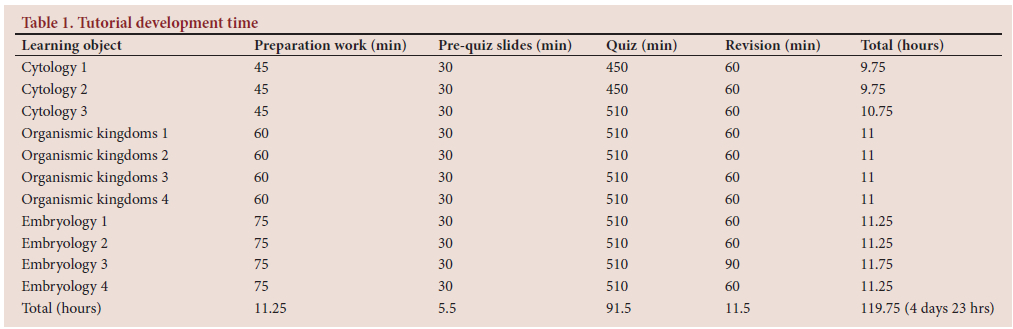
Designing and developing the interactive tutorials took ~5 days (4 days and 23 hours). This included content slides, assessment questions and branching of activities (Table 1).
Phase 3
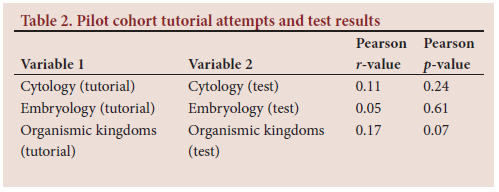
Tutorial interaction reports and module assessment data were submitted for statistical analysis after the learning objects were introduced to the current year cohort of first-year students. In the current year cohort, 33.1% (n=121 pilot cohort) consented to the researchers utilising their tutorial interaction reports, assessment results and questionnaire responses for Phase 4. The tutorials were completed by 119 students in the pilot cohort (completion rate = 98.4%). Results from the correlation analysis demonstrated that for the pilot cohort, there was a significantly stronger relationship between the number of tutorial attempts and assessment results for organismic kingdoms (r=0.17, Pearson p-value = 0.07) and cytology (r=0.11, Pearson p-value = 0.24) than for embryology (r=0.05, Pearson p-value = 0.61) (Table 2).
Phase 4
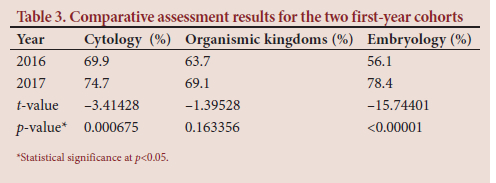
The results for the final phase were twofold: (i) the assessment marks for the first test written by the 2016 and 2017 class were compared; and (ii) a qualitative closed- and open-ended questions survey was completed for the pilot cohort in the current year. The marks for the 2 years for the different topics are compared in Table 3.
Students in the pilot cohort who had completed the tutorials were invited to respond to a questionnaire via the LMS. The questionnaire included both closed- and open-ended questions. A response rate of 43.7% (n=52) was achieved for this survey. Most respondents (57.7%) reported that they accessed tutorials on campus using their own computers, and did so following the lecturer prompts for completion (86.5%). Independent analysis of the responses was compared to identify key themes.
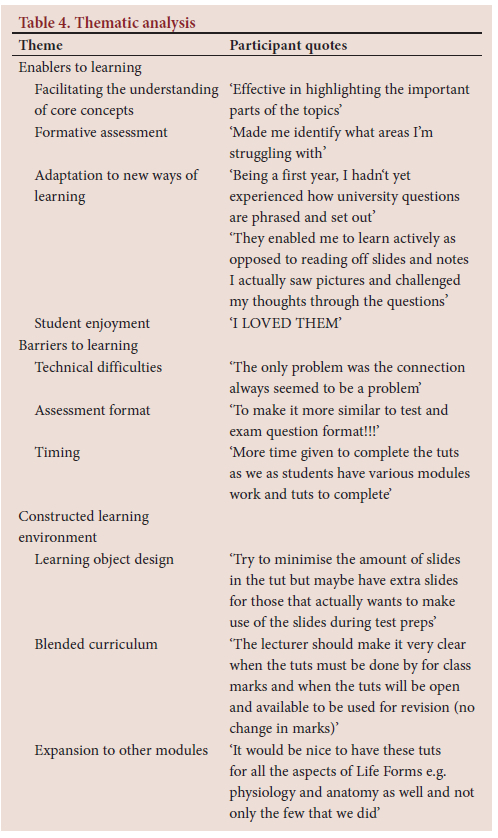
Three global themes were identified that corresponded with the research questions: constructed environment design; barriers to learning; and enablers to learning. These themes were further subdivided into organising themes. The constructed environment design included organising themes of learning object design, blended curriculum and expansion to other modules. Barriers to learning were clustered into organising themes that included technical difficulties, assessment format and timing. The most prevalent global theme was 'enablers to learning', which included facilitating the understanding of core concepts, formative assessment potential, adaptation to new ways of learning and student enjoyment as organising themes. Illuminating quotes are included in Table 4 to demonstrate the application of this analysis.
Discussion
In this pilot study, we provide an overview of how a basic medical sciences department is addressing the challenges of large classes and disparity in academic readiness of first-year health professions students. This was achieved through the use of interactive learning objects embedded in a blended curriculum approach. We approached these challenges by trying to understand and explore learning as a conversation between the lecturer, the constructed learning environment and the student.[11] The design of the study, as a roadmap to future curriculum renewal using adaptive learning tools in our context, solidifies the concept of student-centred blended learning in the biomedical sciences field.[13] Phases 1 and 2 investigated the interaction that occurs between lecturer conceptions, student conceptions and the constructed environment. The responses from the cohort of the previous year and the assessment results gave the module team a solid foundation and guideline for designing the interactive learning objects that responded to student experiences and voice,[16] as opposed to selecting a strategy and content based only on the 'teachers concept'. While the concept of using this type of material in teaching has been shown to be useful,'8-the concerns regarding the time it takes to develop content are valid, and widespread among educators.[17] In our study, we addressed the limited time resource by employing the assistance of a postgraduate student and instructional designer within the faculty to create the tutorials. This ensured that the content was appropriate and of high quality on both an academic and technical level.[1]
The person responsible for developing learning objects, and the scope of the content, has been debated in the literature.[18] In this study, the value in having a subject-expert as the designer/creator of the tutorials is something that we cannot overemphasise. Should an instructional or graphics design expert have been given the content independently, technical or content issues identified by students may have been more prevalent and required more time and financial resources to address. As class sizes increase and the drive to incorporate technology into our curricula becomes the norm, issues around the cost of educating our students and questions regarding the economies of scale around blended learning are common in our environment. One of the potential solutions to these issues is the use of learning objects,[2,19] owing to their cost-effectiveness, reusable nature and the support of a scaffolding approach to education.[19] This supports our contention that the reusable nature of the learning objects created for the LFF module justifies the time and financial resources used, as the content and assessments are useful beyond one module, as a revision tool for modules where these concepts apply to pathology, clinical practice or physiological processes. The statistically significant differences in the marks compared between the year before, implementing the learning objects, and the year after implementation show that the use of learning objects can have a positive influence in assessment results of students.
By using the conversational framework as the theoretical base for how we understand learning to occur, we argue here that assessment results should not be the focus of the intervention. Rather, we propose that a blended curriculum that includes interactive learning objects should be reproducible in similar contexts. To this end, we have attempted to present both the influence on academic achievement and the lessons learned from implementation in relation to learning objects as a valuable method of facilitating learning.
In analysing the relationship between tutorial attempts and assessment results, embryology content yielded the weakest correlation. The explanation for this finding is the higher complexity and more difficult nature of the subject in relation to cytology and organismic kingdoms. As a module team, efforts to address this correlation since this pilot study have included additional resources for revision and tutorials focused on the embryology content. It is also notable that the other topics are similar to the content covered in the final year of secondary education, which implies that students are more likely to perform better on assessments where these familiar concepts are covered. That said, it is still our experience that the formative assessment potential in using learning objects is likely to have a positive impact on summative assessment outcomes.
In the context of the conversational framework (Fig. 1), it is the teacher communication cycle that is affected by these learning objects. The lecturer has developed the curriculum and teaching material using the foundational concepts required for the degree programme. These are presented in class to students from diverse schooling backgrounds and levels of understanding. Once students have completed the tutorials, the lecturer can gauge their grasp of the concepts and address these with additional revision in the classroom before progressing to the next concept. The student is then able to respond again within this 'conversation' by completing additional tutorials in the form of learning objects, or completing the module assessment. This modulation of the constructed environment responds to the needs of individual students without requiring drastic changes to the timetable or curriculum itself. With larger classes, one of the fears of this team was that it would lead to limited opportunities for assessing conceptual understanding and responding to these timeously. The qualitative feedback received from the students during and after the module was completed provided additional information and insight to the lecturer regarding the design of the content, and motivation for continuation and expansion of the intervention.
Conclusion
The challenges of class size, student readiness for higher education and the importance of a strong foundational basic medical science learning experience are important considerations for educators in our context. Creating interactive learning objects and constructing an iterative and engaging learning environment provide a helpful contribution to meeting those challenges. In our study, we have proposed that the cumulative nature of developing resources that are meaningfully embedded in the curriculum is beneficial. For staff, the benefits include having available resources for revision and formative assessment, which improves their ability to respond to students' needs for revisiting concepts that are difficult but crucial to understanding. Our students could benefit through the ability to learn at their own pace, expand their knowledge on particular concepts and revisit biomedical science concepts as they become applicable to other subjects and practices within the curriculum. We recommend that interactive learning objects should be used as a mechanism for feedback to the lecturer on how the curriculum can facilitate learning more effectively, which could, in turn, facilitate multiple ways of learning in our rapidly changing and diverse environment.
Declaration. None.
Acknowledgements. The authors would like to thank the students who participated in this research.
Author contributions. Study concept and design: LK, AA, AK. Acquisition of data: JF, AK, AA, LK. Analysis and interpretation of data: AA, LK. Drafting of manuscript: LK, AA. Critical revision of manuscript for important intellectual content: LK, AA, JF, LK. Administrative, technical, or material support: LK, AA.
Funding. The authors gratefully acknowledge the Fund for Innovation and Research in Learning and Teaching (FINLO) for the funding provided to conduct this research.
Conflicts of interest. None.
References
1. Khogali SE, Davies D, Donnan P, et al. Integration of e-learning resources into a medical school curriculum. Med Teach 2011;33(4):311-318. https://doi.org/10.3109/0142159x.2011.540270 [ Links ]
2. Harden RM, Gessner IH, Gunn M, Issenberg SB, Pringle SD, Stewart A. Creating an e-learning module from learning objects using a commentary or 'personal learning assistant. Med Teach 2011;33(4):286-290. https://doi.org.10.3109/0142159X.2011.557104 [ Links ]
3. Prober CG, Khan S. Medical education reimagined: A call to action. Acad Med 2013;88(10):1407-1410. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00001888-201310000-00009 (accessed 20 July 2018). [ Links ]
4. Garrison DR, Vaughan ND. Institutional change and leadership associated with blended learning innovation: Two case studies. Internet Higher Educ 2012;18:24-28. https://doi.org/10.1016/j.iheduc.2012.09.001 [ Links ]
5. Lewis CE, Chen DC, Relan A. Implementation of a flipped classroom approach to promote active learning in the third-year surgery clerkship. Am J Surg 2018;215(2):298-303. https://doi.org/10.1016/j.amjsurg.2017.08.050 [ Links ]
6. Singh BH, Reed C. A white paper: Achieving success with blended learning. Centra Software, 2001. [ Links ]
7. Laurillard D. Teaching as a Design Science: Building Pedagogical Patterns for Learning and Technology. London: Routledge Farmer, 2012. [ Links ]
8. Badat S, Sayed Y. Post-1994 South African education. Ann Am Acad Polit Soc Sci 2014;652(1):127-148. https://doi.org/10.1177/0002716213511188 [ Links ]
9. Laurillard D. Rethinking University Education: A Conversational Framework for the Effective Use of Learning Technologies. 2nd edition. London: Routledge Farmer, 2002. [ Links ]
10. Laurillard D. The teacher as action researcher: Using technology to capture pedagogic form. Stud Higher Educ 2008;33(2):139-154. https://doi.org/10.1080/03075070801915908 [ Links ]
11. Wong G, Greenhalgh T, Pawson R. Internet-based medical education: A realist review of what works, for whom and in what circumstances. BMC Med Educ 2010;10:12. https://bmcmededuc.biomedcentral.com/articles/10.1186/1472-6920-10-12 (accessed 27 July 2022). [ Links ]
12. Ngan OMY, Tang TLH, Chan AKY, Chen DM, Tang MK. Blended learning in anatomy teaching for non-medical students: An innovative approach to the health professions education. Health Profess Educ 2018;4(2):149-158. https://doi.org/10.1016/j.hpe.2017.11.001 [ Links ]
13. Ruiz JG, Mintzer MJ, Issenberg SB. Learning objects in medical education. Med Teach 2006;28(7):599-605. https://doi.org/10.1080/01421590601039893 [ Links ]
14. Noor K. Case study: A strategic research methodology. Am J Applied Sci 2008;5(11):1602-1604. https://doi.org/10.3844/ajassp.2008.1602.1604 [ Links ]
15. Attride-Stirling J. Thematic networks: An analytic tool for qualitative research. Qualit Res 2001;1(3):385-405. https://doi.org/10.1177%2F146879410100100307 [ Links ]
16. Keiller L, Inglis-Jassiem G. A lesson in listening: Is the student voice heard in the rush to incorporate technology into health professions education? Afr J Health Profess Educ 2015;7(1):47-50. [ Links ]
17. Sandars J. It appeared to be a good idea at the time but ... a few steps closer to understanding how technology can enhance teaching and learning in medical education. Med Teach 2011;33(May):265-267. https://doi.org/10.3109/0142159X.2011.550972 [ Links ]
18. Krauss F, Ally M. A study of the design and evaluation of a learning object and implications for content development. Interdisciplin J Knowledge Learn Objects 2005;1:1-22. [ Links ]
19. Weller M. Learning objects and the e-learning cost dilemma. Open Learn J Open Distance e-Learn 2004;19(3):293-302. [ Links ]
 Correspondence:
Correspondence:
L Keiller
lkeiller@sun.ac.za
Accepted 18 August 2021


{kind=link}
{kind=link}