










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAfrican Journal of Health Professions Education
versión On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.14 no.3 Pretoria sep. 2022
http://dx.doi.org/10.7196/AJHPE.2022.v14i3.1584
RESEARCH
Nursing students' perceptions of support and active learning regarding simulation-based education in Lesotho: A quantitative study
P S MoabiI, II; N G MtshaliII
IPhD ; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIPhD; Scott College of Nursing, Morija, Lesotho
ABSTRACT
BACKGROUND. Simulation has taken centre stage in health sciences education in the context of the increasing adoption of a competency-based curriculum. Simulation replicates facets of the real world in an interactive manner that allows students to learn clinical skills and develop clinical reasoning skills in a safe learning environment. Facilitators have a responsibility to provide adequate instructional and psychological support to the students, while facilitating active and self-directed learning in the simulation environment.
OBJECTIVE. To explore and describe students' perceptions of support and active learning regarding simulation-based education (SBE) in Lesotho.
METHODS. A quantitative descriptive exploratory study was conducted using a validated questionnaire. A total of 275 nursing students participated in the study. A stratified systematic random sampling method was used and data were analysed using SPSS version 27.
RESULTS. The majority of participants (87.9%) had a positive perception of support that was offered prior, during and after simulation, which they appreciated. Active learning was also perceived positively, as most of the participants indicated that they actively participated in, and not merely observed, simulation. The results showed significant associations between an opportunity given to students to discuss simulation objectives with the teacher and various institutions (p<0.05 (p=0.01)). Institutions with trained simulation facilitators provided students the opportunity to discuss simulation objectives with their teacher.
CONCLUSION. The study showed that student support and active learning are essential when conducting SBE. Supporting students and actively involving them in the learning process lead to effective learning.
Simulation refers to a learning approach that is designed to promote development of decision-making skills and critical thinking in students learning in a controlled environment. Simulation allows replication of the real clinical environment, where students practise relevant knowledge and skills multiple times without putting the life of patients at risk.[1,2] Simulation, as one of the educational approaches, is grounded on various learning theories that include constructivism and adult and experiential leaning.[3,4] According to Rothgeb,[3] an adult learner who is placed in a simulation laboratory has a mature self-concept, has accumulated life experiences and has a readiness to learn, which are tied to internal motivating factors that need to be supported during learning. Taylor and Hamdy[5] explain that educators can support learners by actively involving them in learning, assisting them in identifying their learning needs and encouraging reflection. In constructivism - one of the learning theories underpinning simulation - Mukhalalati and Taylors-explain that the simulation facilitator can support learners by facilitating and negotiating meaning with them. In experiential learning, adults learn hands on.[3,4] The role of the facilitator in such learning is to create scenarios that allow learners to conduct a skill several times until they are competent regarding that skill, and give students the possibility to reflect on their performance, which must be done in a supportive environment and in a non-judgemental manner.[5]
Simulation support comprises instructional support, where the facilitator uses various teaching strategies to enhance student engagement to facilitate effective learning.[7] These strategies include provision of information and feedback to students and conducting proper debriefing.[8] As part of instructional support, students need to be provided with cues and comments as they progress during simulation activity, which will assist them to improve their learning. The cues need to be provided in a timely manner.[8,9-Psychosocial support also needs to be provided to nursing students. A study by Landeen et al.[10] shows that students need psychosocial support during simulation, as they experience anxiety. According to Au et al.[11] and Baptista et al.,[12] anxiety may be the result of a lack of realism, where the simulated case is not very real. Anxiety may also be caused by students being watched by colleagues and by the possibility of being criticised. Students need to be supported during simulation, and need to be actively involved. According to Fayombo,[13] active learning is defined as a learner-centred approach that actively involves students in their learning, and where students are allowed to explore their own meaning, attitudes and values. Teamwork is one of the active learning strategies that promotes leadership development.[6]- Active learning in simulation can be enhanced by peer debriefing,[8,9,14] which allows students to be actively involved in their learning, as peers provide feedback to each other.
Simulation-based education (SBE) was first instituted in Lesotho in 2012.[15,16] This methodology was introduced, because almost all of the nursing training institutions had inadequately equipped demonstration rooms, coupled with poor supervision of students during clinical
placement. With the support of developmental partners, each institution was provided with equipped skills laboratories and staff to assist in the laboratories.[10,11- A few nurse educators were trained on how to facilitate learning in simulation laboratories and others are still behind with training.[16] A study by Munangatire and Naidoo[16] showed that nurse educators in Lesotho lack training on facilitation of SBE. Untrained simulation facilitators may not provide adequate support to students and may not actively involve them during simulation. Therefore, this study aimed to explore and describe students' perceptions of support and active learning regarding SBE in Lesotho.
Methods
Research approach and design
This study adopted a quantitative descriptive exploratory design to assess, explore and describe nursing students' perceptions of support and active learning regarding SBE, with a large sample size. The design was appropriate, as it explains the phenomena from the perspective of the person being studied.[17]
Research setting
Four private nursing education institutions (NEIs) in Lesotho served as research settings. These NEIs were selected because of their competency-based curricula. They offer a 3-year nursing diploma and a 1-year midwifery diploma and use SBE as one of their clinical teaching methods.
Population and sample
The population comprised second-year, third-year and midwifery students from the 4 private NEIs. First-year students were excluded because the institutions did not have a first-year intake owing to COVID-19 restrictions.
NEI-1 had a population of 201 students, NEI-2, 76, NEI-3, 98 and NEI- 4, 118; the final sample size comprised those who returned the questionnaire (N=275). The researchers used stratified systematic random sampling, with each level of student forming a stratum. Sample proportions were identified per institution, and from the proportions the researchers identified the sample size using the Qualtrics (Qualtrics, USA) sample calculator. A list of all the students was used as a sampling frame from which to select the recommended sample, and a table of random numbers was used to select every third student.[18]
Data collection
Data were gathered by means of a structured questionnaire, which consisted of items from two tools, i.e. the National League for Nursing[19] instrument that assesses simulation design, and a survey tool[20] that evaluates the psychometric properties of the modified simulation effectiveness. This article focuses on two sections of the questionnaire: student support and active learning. The responses were rated on a 6-point Likert scale, which had the following options (one option per question): strongly disagree with the statement (1); disagree with the statement (2); undecided (3); agree with the statement (4); strongly agree with the statement (5); not applicable (6).
Validity and reliability
Content validity of the tool was ensured by presenting it to experts in SBE, by research to critique it and by matching items to the research objectives, incorporating submissions made by the experts. External validity was ensured by including a representative sample of the population; the reliability coefficient of the tool was 0.88.
Data analysis
SPSS version 27 (IBM Corp., USA) was used to analyse data. Sections on students' support and active learning were analysed and presented using descriptive statistics. This was done in the form of percentages, frequencies, standard deviations (SDs) and means. To assess the relationship between demographic characteristics and items on the tool, Pearson's χ2 test was used and p<0.05 was considered statistically significant. Frequency distribution was used to assess distribution of participants' responses.
Ethical approval
Ethical approval was obtained from the Humanities and Social Sciences Research Ethics Committee, University of KwaZulu-Natal (ref. no. HSSREC/00001411/2020) and the Ministry of Health, Lesotho (ref. no. 88-2020). Participants were informed that confidentiality and anonymity would be maintained - identified by codes. Consent forms were issued to and signed by the participants.
Results
The results section is presented as follows: (i) demographic information of the participants; (ii) students' perceptions of instructional and psychological support during simulation; and (iii) students' perceptions of active learning.
Demographic characteristics of participants
The majority of participants (78.9%; n=217) were female, while 21.1% (n=58) were male. Most (41.5%; n=114) were in their third year of study, 29.8% (n=82) studied midwifery and 28.7% (n=79) were in their second year. The majority (36%; n=99) of students who participated were from NEI-4, 27.6% (n=76) were from NEI-3, and 23.3% (n=64) were from NEI-2, while 13.1% (n=36) were from NEI-1.
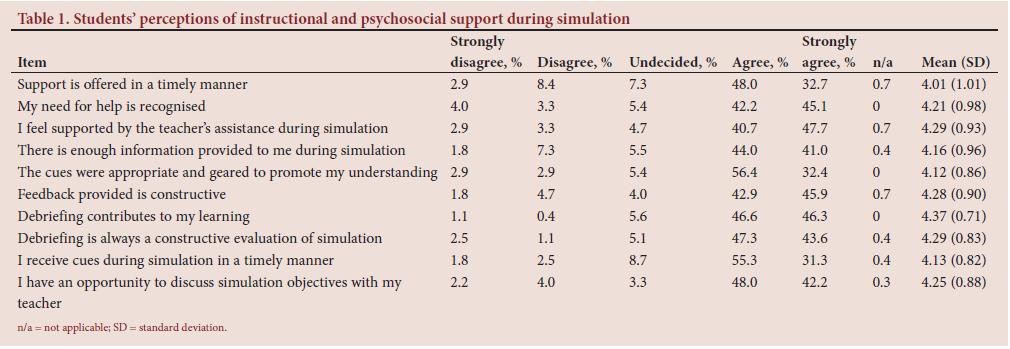
Instructional and psychological support during simulation
Regarding the support provided to the students before, during and after simulation, 32.7% (n=90) strongly agreed, 48% (n=132) agreed, 7.3% (n=20) were undecided, 2.9% (n=8) disagreed and 8.4% (n=23) strongly disagreed that support was offered in a timely manner. The mean score of the item was 4.01 (SD 1.01). With regard to recognising students' need for help, 45.1% (n=124) strongly agreed, 42.2% (n=116) agreed, 5.4% (n=15) were undecided, 3.3% (n=9) disagreed and 4% (n=11) strongly disagreed. The mean score of the item was 4.21 (0.98).
Regarding teachers' support, 47.7% (n=131) strongly agreed, 40.7% (n=112) agreed, 4.7% (n=13) were undecided, 2.9% (n=8) disagreed and 3.3% (n=9) strongly disagreed that they felt supported by teachers' during simulation. The mean score of the item was 4.29 (0.93).
There was a statistically significant association between recognising students' need for help and the year of study (p<0.05 (p=0.04)). The majority of participants (41.1%; n=113) strongly agreed, 44% (n=121) agreed, 7.3% (n=20) disagreed and 1.8% (n=5) strongly disagreed that enough information was provided to them during simulation. Few participants (5.5%; n=15) were undecided, while 0.4% (n=1) indicated that the question was not applicable to them. The mean score of the item was 4.16 (0.96).
Table 1 shows how students perceived instructional and psychosocial support during simulation.
Students' perceptions of active learning during simulation
A large number of respondents (52%; n=143) strongly agreed and 39.3% (n=108) agreed that they had an opportunity during simulation to discuss the ideas and concepts with the teacher and other students. Participants who account for 1.8% (n=5) disagreed and 3.3% (n=9) strongly disagreed, while 3.3% (n=9) were undecided regarding this opportunity. The mean score of the item was 4.36 (0.90). With regard to active participation in the debriefing session after simulation, 29.1% (n=80) of students strongly agreed, 60.4% (n=166) agreed, 2.2% (n=6) disagreed and 2.9% (n=8) strongly disagreed as regards active participation. The undecided rating was scored at 5.1% (n=14) and the mean score of the item was 4.12 (0.83).
The majority of students (33.8%; n=93) strongly agreed and 56.7% (n=156) agreed that they had the opportunity to put more thought into their comments during the debriefing session. About 5.1% (n=14), 2.9% (n=8) and 1.5% (n=4) of respondents were undecided, disagreed and strongly disagreed, respectively. The mean score of the item was 4.19 (0.78).
Regarding time in simulation, 50.9% (n=140) strongly agreed and 43.6% (n=120) agreed that using simulation activities made their time more productive, while 1.5% (n=4) disagreed and 2.2% (n=6) strongly disagreed. Only 1.8% (n=5) were undecided about the item. The mean score was 4.40 (0.79).
Pearson's χ2 showed that there was a significant association between an opportunity given to students to discuss simulation objectives with the teacher and the institutions (p<0.05 (p=0.01)). Table 2 shows how students perceived active learning during simulation. Institutions with trained simulation facilitators provided students the opportunity to discuss simulation objectives with their teacher.
Summary
Most participants showed that they were supported prior, during and after simulation, which possibly had an impact on their performance. Most students perceived active learning in simulation positively.
Discussion
The discussion section is presented as follows: (i) students' perceptions of instructional and psychological support during simulation; and (ii) students' perceptions of active learning.
Students' perceptions of instructional and psychological support during simulation
Most of the participants agreed that when they needed help during simulation, the facilitator provided such help (Table 1). When the facilitator provided help, most students felt that they were supported during simulation. According to Martins et al.,[8] instructional support can be provided to students by orientating them regarding the simulation space, simulator potential and available resources. It is important to discuss simulation objectives with the teacher. Most participants indicated that they had an opportunity to discuss such objectives with their teacher (Table 1). Discussing objectives of simulation with the teacher allows students to know the expectations for the day. Simulation objectives need to be discussed during the planning phase of the simulation experience.[8,9,21] According to Martins et al.,[8] these objectives, must be clear and feasible. In low-fidelity simulation, the objectives must focus on knowledge and psychomotor skills, while in medium-fidelity simulation, they must focus on more complex knowledge and techniques. In high-fidelity simulation, the objectives, according to Martins et al.[8] and Guinez-Molinos et al.,[9] must focus on non-technical skills such as communication, decision-making, teamwork and clinical judgement.
Debriefing is one of the instructional supports that needs to be provided; if the facilitator provides negative comments to students, there will be limited opportunities for them to learn. After simulation, the facilitator must conduct debriefing. In a non-judgemental approach, the facilitator must discuss positive aspects observed during simulation, as well as areas that need improvement.[8,9] A qualitative study by Moabi and Mtshali,[21] in Lesotho, found that some students are concerned about comments made by simulation facilitators, as some comments are negative and tend to belittle the students. Furthermore, students need to be provided with cues and comments as they progress during simulation activity,[12,13] which will assist them to learn more.[22] The cues were provided in a timely manner (Table 1).
According to Sebold et al.,[23] some nursing students experienced anxiety during simulation-based teaching and needed support, which possibly reduced students' anxiety. The anxiety was mostly caused by lack of realism as to the mannequins. Students debate that mannequins do not show emotions, or feel or move, which frustrates them.[2,15] Baptista et al}12-explained that for some students, anxiety is caused by being watched by colleagues; the students are also fearful of being criticised.
Students' perceptions of active learning
A large number of participants indicated that they had an opportunity during simulation to discuss the ideas and concepts of the course with the teacher and other students (Table 2). Discussing ideas and concepts with fellow students promotes teamwork, which is crucial in nursing. Simulation promotes teamwork, when students learn to respect each other's opinions.[23,24] Scenarios can be created that lead to students working in a team. During that time, the assessor evaluates teamwork, and gives feedback after the session. During teamwork, leadership development is promoted,[8,14] because during a team simulation experience, a leader will emerge who will guide the group on the next step.[14,22]
The majority of participants indicated that simulation activities made their time more productive (Table 2). They then learnt about patient care, decision-making and critical thinking. According to Landeen et al.[10] and Liaw et al.,[18] students found that simulation enhances their clinical capabilities, including decision-making skills that have been elicited by scenarios used during simulation. Simulation allows students to rehearse the role of nurses,[1] made possible by clinical scenarios that make their time more productive.[22]
Conclusion
The results of this study reflect positive perceptions of the support to students in SBE, which are ascribed to high motivation among nurse educators who facilitate SBE in Lesotho.[16] The study findings highlight that nurse educators in Lesotho lack SBE training, especially in the use of high-fidelity mannequins, even though they have a qualification in nursing education. As the study was conducted in a resource-constrained setting, the findings showed that even if there are limited resources in simulation laboratories, students are provided with enough instructional support to enable their learning. Furthermore, even if an institution lacks financial resources, students can be actively involved in such laboratories. Study results may benefit NEIs to continuously improve facilitation of SBE.
Study limitations
The researchers acknowledge that this study was purely exploratory-descriptive, and in-depth perceptions of students need to be explored qualitatively.
Declaration. None.
Acknowledgements. The authors thank the private nursing education institutions for granting permission to conduct the study. The Ministry of Health, Lesotho, and the Humanities and Social Sciences Research Ethics Committee, University of KwaZulu-Natal, are acknowledged for giving approval to conduct the research. We also thank the students who participated in the study.
Author contributions. PSM contributed towards conceptualisation of the research, collected and analysed the data and wrote the manuscript. NGM supervised the research and contributed towards analysis of the findings and writing of the manuscript. Additional study data are available on request from the corresponding author.
Funding. None.
Conflicts of interest. None.
References
1. Krishnan D, Keloth D, Ubedulla D. Pros and cons of simulation in medical education: A review. Int J Med Health Res 2017;6(3):84-87. [ Links ]
2. Unver V, Basak T, Tastan S, et al. Analysis ofthe effects of high-fidelity simulation on nursing students' perceptions of their preparedness for disasters. Int Emerg Nurs 2018;38:3-9. https://doi.org/10.1016/j.ienj.2018.03.002 [ Links ]
3. Rothgeb M. Creating a nursing simulation laboratory: A literature review. J Nurs Educ 2008;47(11):489-494. [ Links ]
4. Belanger P. Theories in adult learning and education. 2011. https://www.jstor.org/stable/j.ctvbkjx77.8 (accessed 5 September 2021). [ Links ]
5. Taylor D, Hamdy H. Adult learning theories: Implications for learning and teaching in medical education. AMEE Guide No. 83. Med Teach 2013;35(11):e1561-e1572. https://doi.org/10.3109/0142159x.2013.828153 [ Links ]
6. Mukhalalati B, Taylor A. Adult learning theories in context: A quick guide for healthcare professional educators. J Med Educ Curric Dev 2019;6:1-10. https://doi.org/10.1177/2382120519840 [ Links ]
7. Ertesvag S. Exploring improvement in teachers' instructional support: Classifying and analysing patterns of change in a national initiative on classroom management. Int J Leadership Educ 2021;24(4):533-557. https://doi.org/10.1080/13603124.2019.1613567 [ Links ]
8. Martins JCA, Baptista RCN, Coutihno VRD, Fernandes MID, Fernandes AM. Simulation in Nursing and Midwifery Education. Copenhagen: WHO, 2018:2-9. [ Links ]
9. Guinez-Molinos S, Martínez-Molina A, Gomar-Sancho C, et al. A collaborative clinical simulation model for the development of competencies by medical students Med Teach 2017;39(2):195-202. https://doi.org/10.1080/0142159X.2016.1248913 [ Links ]
10. Landeen J, Pierazzo J, Akhtar-Danesh N, Baxter P, van Eijk S, Evers C. Exploring student and faculty perceptions of clinical simulation: A Q-sort study. J Nurs Educ 2015;54(9):485-491. https://doi.org/10.1111/j.1365-2648.2012.06048.x [ Links ]
11. Au M, Lo M, Cheong W, Wang S, Van I. Nursing students' perception of high-fidelity simulation activity instead of clinical placement: A qualitative study. Nurse Educ Today 2016;39:16-21. https://doi.org/10.1016/j.nedt.2016.01.015 [ Links ]
12. Baptista R, Pereira F, Martins J, et al. Perceptions of nursing students on high fidelity practices; a phenomenological study. J Nurs Educ Pract 2016;6(8):10-21. https://doi.org/10.5430/jnep.v6n8p10 [ Links ]
13. Fayombo GA. Active learning strategies and student learning outcomes among some university students in Barbados. J Educ Soc Res 2012;2(9). https://doi.org/10.5901/jesr.2012.v2n9p79 [ Links ]
14. Park ME, McMillan MA, Conway JF, et al. Practice-based simulation model: A curriculum innovation to enhance the critical thinking skills of nursing students. Austr J Adv Nurs 2013;30(3):41-51. [ Links ]
15. Nursing Education Partnership Initiative. Lesotho NEPI Assessment Report. Maseru: NEPI, 2012:33-55. [ Links ]
16. Munangatire T, Naidoo N. Exploration of high-fidelity simulation: Nurse educators' perceptions and experiences at a school of nursing in a resource-limited setting. Afr J Health Professions Educ 2017;9(1):44-47. https://doi.org.10.7196/AJHPE.2017.v9i1.739 [ Links ]
17. Brink P, Brink P, Wood M. Introduction in Advanced Design in Nursing Research. Thousand Oaks: Sage, 2012:3-18. [ Links ]
18. Liaw S, Palham S, Chan S, Wong L, Lim F. Using simulation learning through academic-practice partnership to promote transition to clinical practice: A qualitative evaluation. J Adv Nurs 2014;71(5):1044-1054. https://doi.org/1044-1054.10.1111/jan.12585 [ Links ]
19. National League of Nursing. Descriptions of available instruments. 2021. http://www.nln.org/professional-development-programs/research/tools-and-instruments/descriptions-of-available-instruments (accessed 15 March 2021). [ Links ]
20. Leighton K. Updating the simulation effectiveness tool: Item modifications and re-evaluation of psychometric properties. Nurs Educ Perspect 2015;36(5):317-323. [ Links ]
21. Moabi P, Mtshali N. Nursing education institutions' readiness to fully implement simulation-based education in Lesotho. Africa J Nurs Midwifery 2021 33(1). https://doi.org/10.25159/2520-5293/8686 [ Links ]
22. Larue C, Pepin J, Allard É. Simulation in preparation or substitution for clinical placement: A systematic review of the literature. J Nurs Educ Pract 2021;5(9):132-140. https://doi.org/10.5430/jnep.v5n9p132 [ Links ]
23. Sebold LF, Boell JEW, Girondi JBR, dos Santos JLG. Clinical simulation: Development of relational competence and practical skills in nursing fundamentals. J Nurs 2017;11(10):4184-4190. https://doi.org/10.5205/reuol10712-95194-3-SM.1110sup201723 [ Links ]
24. Jeffries P, Rodgers B, Adamson K. NLN Jeffries simulation theory: Brief narrative description. Nurs Educ Perspect 2015;36(5):292-293. https://doi.org/10.5480/1536-5026-36.5.292 [ Links ]
 Correspondence:
Correspondence:
P S Moabi
pulemoabi@gmail.com
Accepted 24 January 2022


{kind=link}
{kind=link}