










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.14 n.2 Pretoria Jun. 2022
http://dx.doi.org/10.7196/ajhpe.2022.v14i1.1506
RESEARCH
Module evaluation for emergency remote teaching: An oral hygiene case study during the COVID-19 pandemic
M CupidoI; N GordonII; N BehardienIII
IBChD; Department of Maxillofacial and Oral Surgery, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
IIDipl OH, MPH, Dipl Adult Education; Department of Oral Hygiene, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
IIIMSc (Dent); Department of Maxillofacial and Oral Surgery, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
ABSTRACT
BACKGROUND: The COVID-19 pandemic resulted in emergency remote teaching, with limited student contact time. For programmes with strong clinical and community-based requirements, such as the Bachelor of Oral Health, one had to be innovative to meet module outcomes
OBJECTIVES: To (i) evaluate the curriculum and pedagogy of two diverse modules in the second year; and (ii) explore contextual factors affecting teaching and learning
METHODS: This evaluation study used a mixed-methods design. The sample comprised lecturers (n=3), clinical teachers (n=2), students (n=29) and documents for analysis. The modified concept-indicator method and the emergency remote teaching environment frameworks guided the data collection process. Tools included questionnaires, a focus group discussion and document analysis. Quantitative data were presented as frequencies and qualitative data were themed
RESULTS: Student participation for the OHP213 module was 76% (n=19) and 68% for the LOS200 module (n=19). All the lecturers (n=3) participated. Overall, the content and teaching and learning specialists were satisfied with the modules, but made suggestions for improvement. Student experiences highlighted diversity in their learning styles and challenges, while lecturers articulated challenges and emphasised affordances during this period
CONCLUSIONS: The curricula were generally found to be aligned in terms of outcomes, content and assessment. Emergency remote teaching presented affordances from the perspective of students and lecturers, which could be explored further. If online teaching were to be a feature of university education, the affordances highlighted by students and staff may argue for a revised hybrid approach to delivering an oral health programme. However, such a system would require thorough research, with the necessary support built into the university as an ecosystem
The COVID-19 pandemic resulted in the disruption of academic programmes globally, thereby compelling contact universities to adopt a reactionary mode of programme delivery.[1,2] South African (SA) universities were affected similarly with regard to the academic agenda. Transitions from contact teaching to an online platform during the entire lockdown period, and transitions to an adjusted clinical/practical programme upon return to contact teaching, were instantaneous. During this period, rapidly developed instructional methodologies replaced the well-planned and well-designed academic programmes used before the crisis,[3] affecting academics and students in higher education in different ways.[4] Lecturers required theoretical and technological skills to present online teaching and assessment, and students, as adult learners, needed to become more independent.[4,5] SA, where there is a huge disparity of resources between the rich and the poor, has been quoted as the most unequal country in the world.[6] Data from 2002 to 2014 showed that nationwide, more than one-quarter of formal, low-cost dwellings were overcrowded.[7] Although food secure in terms of its ability to produce food for the population, 2012 figures indicated that 54% of SA households were food insecure, i.e. 28% were at risk of hunger and 26% experienced hunger.[8] Food security was previously expressed as a growing concern among university students in SA.[9] The consequences of the lockdown contributed to reduced access to the affordances of universities, put students at higher risk of food insecurity, led to challenges with communication technology[4] and reduced access to study space. Academics of the Faculty of Dentistry at the University of the Western Cape (UWC) had to resort to a temporary emergency teaching environment as seen in other parts of the world. [10]
The Bachelor of Oral Health (BOH) degree at UWC is offered as a full-time contact programme, with learning and teaching taking place in the classroom, preclinical laboratories, dental clinics and various community-based facilities. The focus of the oral hygiene profession is oral health promotion, prevention of oral diseases and delivery of preventive and therapeutic clinical care.[11] Core competencies include oral health promotion and a range of clinical procedures, encompassing scaling, polishing, restoration and provision of local anaesthesia (LA). In 2020, the academic year commenced with the traditional programme for the first term, ending in March. Subsequently, the various levels of lockdown resulted in an adjusted academic programme for the remainder of the year, which included online (synchronous and asynchronous) learning and teaching for the duration of the year. Modules with a clinical component required students to return to the clinical platform during the last term. With quality assurance being an integral part of all curricula offered at higher education institutions (HEIs), two diverse modules of the BOH degree that were presented during the COVID-19 pandemic were evaluated.
To ensure credibility and validity of academic programmes, diverse stakeholders and different sources should inform the evaluation process.[12] Modified versions of two evaluation tools, the modified concept-indicator method (CIM) and the emergency remote teaching environment (ERTE), were used to guide this process. Although findings are not generalisable to the BOH programme, an evaluation of sufficiently diverse modules in the same academic year may provide insight into the benefits and challenges regarding the teaching and learning pedagogy. The results may validate these modules in their current form, highlight areas for change and explore affordances presented by emergency remote teaching. The aim of this research was therefore to evaluate two modules presented in the second year of the BOH programme within the context of the COVID-19 pandemic. The objectives were: (i) to evaluate the module content; and (ii) to explore the learning and teaching experiences of involved stakeholders.
Methods
This research was an evaluation study using a mixed-methods design. Two methodological frameworks were used to guide data collection.[10,13] The overarching tool was the CIM framework,[13] with the ERTE educational framework[10] nested within. The core evaluation concepts emanated from the aim of this project, with aligned indicators from the objectives. Relevant key indicators, criteria, methods, tools and data sources were identified (Table 1). The selection of the two modules was based on the diversity presented by a clinical (LOS200) and public health (OHP213) focus. During the pandemic, the home environment was a proxy for the community, while the clinical platform was used to perform LA. Although both modules were year modules, formal teaching for OHP213 was completed at the end of semester 1, with a final assessment concluded at the end of the academic year.
Data collection and analysis
Participants comprised oral hygiene students in their second year of study (OHP213: n=29; LOS200: n=32), clinical chairside teachers (n=2) and lecturers (n=3) of the two modules. Data were generated from: (i) student evaluation of modules; (ii) documents, including assessments such as tests and assignments, learning activities and clinical procedures; (iii) reports of an internal teaching and learning specialist (Faculty of Dentistry) and external subject specialists (academics from two dental schools in SA); and (iv) lecturer/clinical teacher feedback. A modified version of the faculty module evaluation questionnaire, guided by the literature on the effects of the COVID-19 pandemic, was used for students. This questionnaire, using Google Forms, was self-administered and anonymous and included open-ended and closed-ended questions. The questionnaire comprised 4 sections, which included demographic information and student perceptions and opinions of teaching, learning and assessments within the context of the COVID-19 pandemic. Students could respond to a range of statements on a 5-point scale, ranging from strongly agree, agree, neutral, disagree to strongly disagree, to elicit their perception of teaching and learning (Table 2). In addition, they could identify their access to resources and factors impacting on their learning from a predefined list (Figs 1 - 3). Open-ended questions included their challenges, suggestions and reflections. Records of teaching, learning and assessment, as well as faculty protocols, were used as data on student performance. The teaching and learning specialist was requested to review these and provide a report on the alignment of modules in terms of outcomes, content, assessment and teaching practice, while the content specialists reported on theoretical and practical content and teaching application relevant to each module. A modified version of the ERTE framework[10] was used to generate data on lecturers' perceptions and experiences of their modules. Two iterations were done. The three lecturers individually recorded a self-reflection on 'affordances and challenges' presented and experienced during this period, which was then shared. These recordings informed the topics for the focus group discussion and a second iteration facilitated by a colleague acquainted with teaching and learning pedagogy, and allowed for deeper exploration of the themes. Quantitative data were described and presented as frequency tables.
Ethical approval
Ethical approval was obtained from the Biomedical Research Ethics Committee of UWC (ref. no. BM16/5/9).
Results
The results of the evaluation from the four data sources of core concepts 1 and 2 are presented.
Student response to key indicators of the CIM framework
Nineteen students completed the evaluation for both modules (76% for OHP213 and 68% for LOS200).
Core concept 1: Curriculum pedagogy
Students' views on course design, learning and teaching interaction, learning material and resources, competence in practical aspects of modules and assessments are presented below.
The results indicate that fewer students understood the learning outcomes of OHP213 than of LOS200. Furthermore, this difference was mirrored in the preparation of lessons for these modules (Table 2). Views of course design were further expressed as follows:
'Lecturers can reduce content and stick to what's really important to know'
'Overall, it was a well-planned module and the lecturer was always there to assist.'
Students' experiences of learning and teaching are reported in Table 2. The following quotations illustrate varying views:
'Weekly assessments and quizzes helped me a lot with my studies and helped me retain information.'
'Group assignments are not the best way in which group work can be tested.'
The view of lecturers being approachable and learning being interactive was consistent between the two modules. There was a strong view that assessments were fair in terms of the outcomes and that feedback supported learning.
Students identified the practical application (school visits during term 1 and administration of LA done in term 4) as supporting their understanding of the modules the most. For LOS200, the preclinical block (100%), administration of LA (94.7%), being paired with a dental student (94.7%), lecturer-student feedback (78.9%) and clinical teachers being approachable and providing the necessary support (89.5%) were deemed most effective for learning. Guided reflections were elicited as 'critical incidents,' as used by Tsang.[14]
The quotations from their reflections highlighted the main themes, supporting their learning as the behaviour of the clinical teacher, student experiences with patients and consolidating theory with clinical experience: Reflection of student experience of their learning was highlighted:
'Despite the pandemic and loss of clinical time, students were able to learn very quickly as the lecturers were hands on and very approachable if something needed more clarification.'
'One of my class mates had a needle prick injury [experience]. I was a little nervous [feeling] cause it can happen so quick ... learn to always use your mirror [learning] to retract ... always prepare my patient to cooperate [do differently].'
In the OHP213 module, most students reported that the school visits supported understanding of the module and encouraged an interest in community health (89.9%). A student reflection, after the first school visit with grade 1 learners, illustrates the value of community-based learning experiences:
'We had a discussion ... "What could happen if we do not brush our teeth?" They all replied, "You will have rotten teeth!" ... pointed to a girl who had visible dental caries. She went silent and one could see her discomfort [experience]. I felt shocked about how cruel such young children can be to one another, sad and embarrassed that we as healthcare professionals placed that little girl in that position [feeling]. In a similar situation, I would ask children to write down in their own words what they think can happen instead of letting them shout it out [do differently], which may result in some learners feeling invalidated [learning].'
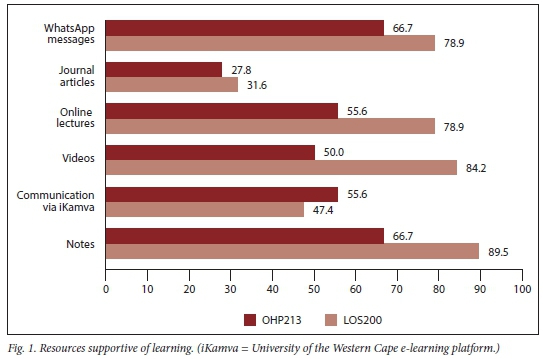
There was a marked difference between the two groups in the resources they found supportive of their learning (Fig. 1). In LOS200, activities best supporting understanding were: online practical demonstrations (84.2%), synchronous online lectures (78.9%), role-play (47.4%) and group work (47.4%). In contrast, in OHP213, the activities were: developing a portfolio (61.1%), voice-over PowerPoint (Microsoft Corp., USA) lectures in which the lecturer was visible (55.6%), reflecting on learning (55.5%) and researching professional websites (47.4%). Lecture notes were reportedly the most useful resource for both groups.
Responses of agree and strongly agree were combined and are reported as agreed. Responses of disagree and strongly disagree were combined and reported as disagreed. In one of the statements, most of the time was an option instead of neutral.
Core concept 2: Student contextual factors affecting teaching and learning
Contextual factors that impacted positively and negatively on student learning are presented below.
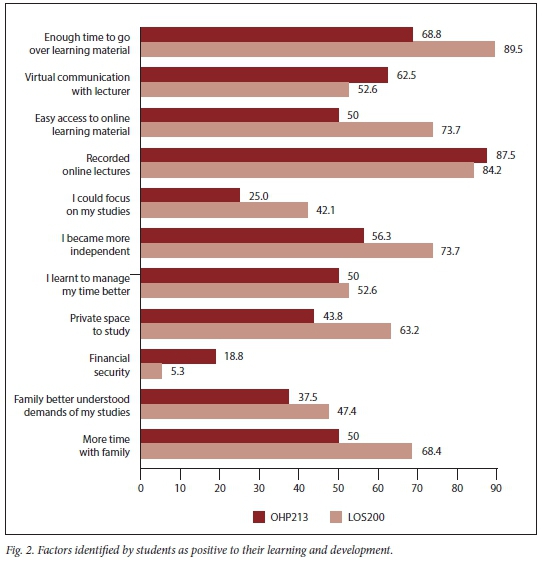
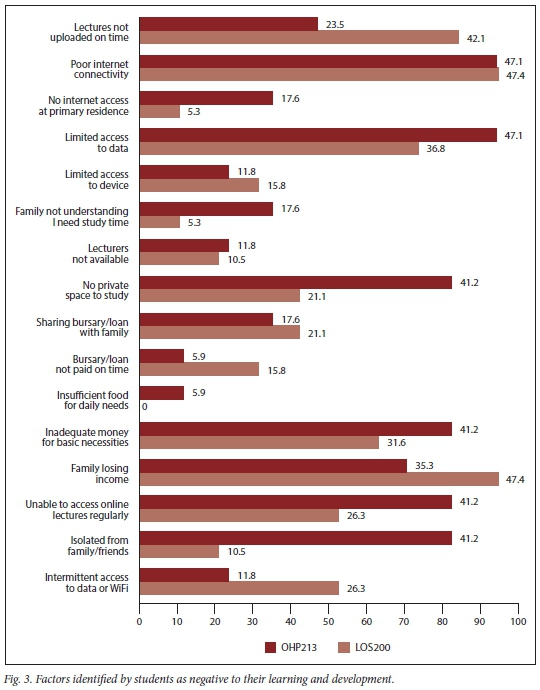
The views of student experiences of their learning environment and the impact on their learning are shown in Figs 2 and 3.
There were marked differences in the factors impacting positively on learning in the two modules (Fig. 2). These were less so in recorded online lectures and time management. There were marked differences in factors impacting negatively on student learning, except poor connectivity, which was common to both. Although food was not indicated as impacting negatively, inadequate money for basic necessities was a concern for approximately a third of students. The loss of family income was expressed as a concern for more than a third of students (Fig. 3).
In the open-ended questions, students were asked to identify the most significant change in their lives during lockdown. These were themed as: (i) personal such as time management, being more productive and organised, compromising on how the day was organised, being more disciplined, self-motivated and adapting to new ways; (ii) the home such as changes such as juggling household duties, not having to travel and being indoors most of the time; and (iii) learning such as adapting to a new norm of studying online, not going to university, not being able to interact with lecturers and peers, being dependent on technology, online assessments and insufficient practical experience:
'This really increased my stress levels because while I was still regularly studying to get good grades, they [parents] felt that me being home, meant that I had more time to focus on housework.'
Document analysis aligned to the CIM framework
Core concept 1: Curriculum pedagogy
In the OHP213 module, 25 of the 29 registered students (86.2%) completed and passed the module. In the LOS200 module, 28 of the 32 registered students (87.5%) completed and passed the module. Students in both modules discontinued participation at different periods of the lockdown and did not respond to faculty follow-up processes. This amounts to an attrition rate of 13.8% for OHP213 and 12.5% for LOS200.
Lecturers' views were that assessments were aligned to the faculty assessment and moderation protocol. The range of assessments (e.g. tests, case studies) accommodated the differing needs of students.
Expert response to key indicators of the CIM framework
Core concept 1: Curriculum pedagogy
The teaching and learning specialist suggested presenting module outcomes as 'applied integrated competencies' rather than 'knowledge, skills and values'. This would allow a more detailed description of learning to be attained and guide the associated teaching, learning and assessment practices. It was advised that when deciding on the type of assessment and the breakdown thereof, in view of adjustments due to lockdown-associated challenges, lecturers should be guided by the question, 'Do the assessment outcomes produce competence at a level expected of the students?' Furthermore, assessments should be flexible enough to encompass the differing needs of students.
The content specialist for LOS200 reported that the module was appropriately covered and relevant. It was suggested that content taught at a preclinical and clinical level be introduced through didactic lectures to scaffold clinical application, that selected topics be presented in greater detail, and where such topics are taught in other modules, these be consolidated in LOS200. The evidence of varied teaching methods, such as online lectures embedding theoretical knowledge and application in the clinical setting, and a good balance of learning activities aligned with the learning outcomes, was highlighted. A review on the weighting of the clinical component of the module was suggested; however, the reduction of this weighting during the pandemic was deemed acceptable.
The content specialist for the OHP213 module indicated that the attributes expected at second-year level were evident and clearly achieved from the outline of the learning units; relevant theories of oral health promotion were covered and appropriate; and the module content, supported by relevant theory, empowered learners to work in inter-disciplinary health promotion. It was further suggested that lecture presentations (PowerPoint (Microsoft Corp., USA)) were well organised and informative but that there should be a more visual presentation to accommodate diverse learners with differing learning styles.
Lecturer response to key indicators of the CIM framework
Core concept 1: Curriculum pedagogy
The views of lecturers were that assessments were aligned to the faculty assessment and moderation protocol. The range of assessments such as online tests, case studies, independent learning tasks and clinical procedures accommodated the differing needs of students. Lecturers expressed concern regarding the reliability and validity of online assessment outcomes, considering that these were conducted in an environment in which there was limited control over the process.
Lecturers indicated that the broad outcomes of modules were met within the current context and that there was alignment between outcomes, teaching and assessment despite the challenges of changing from contact teaching to a hybrid format. In both modules, theoretical and practical components could not be scaffolded as in the 'traditional' offering owing to effects of the lockdown. Practical aspects were in part presented online for both modules, but for OHP213, the home environment was used as an authentic learning activity for the practical component of the module.
In the OHP213 module, an opportunity was created to streamline content to outcomes, but adjustments to module design in terms of learning opportunities and assessment practices may have compromised the learning for some students. The school project (OHP213) was viewed as a 'real-world perspective' for students, enabling context-specific application of theory to practice, encouraging an appreciation of social determinants of oral health and understanding the difference between empathy and sympathy, as also evident in a student reflection (as reported above).
Clinical chairside teachers (LOS200) considered the online platform to teach application and clinical relevance challenging. They reported that, on return to the clinical platform, the preclinical block course was of great value in preparing students for administering LA. Although the standard method of teaching at the chairside continued on the return of students to the clinical platform, clinical teachers had to be cognisant of the challenges students experienced regarding the use of personal protective equipment (PPE) in performing injection techniques.
Core concept 2: Contextual factors affecting teaching and learning
Lecturers reflected on their experiences of programme delivery during the lockdown period. Using the ERTE framework,[10] they specifically reflected on the challenges encountered and affordances gained. The latter appeared to be standard, i.e. collegial support and the learning and use of new technology. The main themes generated during the first iteration of reflection included the emotions experienced by lecturers, lecturers' concern for students, rapid change in the academic environment, transition to technology, academic programme concerns, information technology (IT) issues, assessment concerns and communication challenges. The second iteration included additional themes and a deeper understanding of themes raised in the first iteration (Table 3).
Discussion
Through systematic curricula evaluation, developers can optimise the curricula to ensure that their goals are met.[15] The CIM framework, a comprehensive tool encompassing the perspectives and expertise of all stakeholders, provided the necessary rigour for this evaluation. The ERTE framework, although used by primary school teachers,[10] has been found to be of value by the lecturers at the tertiary academic institution where this study was conducted.
Triangulation of data indicates views being corroborated by different sources. The use of multiple stakeholders and data sources in module evaluations has been shown to provide a useful overview of both modules, highlighting aspects that may need further investigation. Although teaching diverse modules, lecturers appeared to have similar concerns regarding the coping mechanisms of students with respect to personal and academic challenges imposed by the pandemic. Lecturers being approachable and supportive of student learning, and the interactive nature of the module presentation, as highlighted by students, may be an indication that lecturers acted on these concerns. All students who participated for the entire academic year passed the modules, which is an indication of students' resilience to cope in adverse conditions. A concern, however, is the attrition of 4 students in a relatively small class.
The suggestion by the OHP213 content specialist to increase visual material in lectures is supported by the literature.[16] This may make this resource more useful to students, particularly as they found recorded lectures supportive to learning. The LOS200 content specialist's suggestions highlight that professional programmes have different approaches to presenting the oral hygiene clinical scope of practice, e.g. regarding administration of LA, with regard to content and clinical teaching thereof. Although second-year modules are not subject to external review, the results of this study may make an argument for collegial discussions to inform oral hygiene curricula design across programmes in SA, as done in the USA.[17] Presenting outcomes as integrated competencies, as suggested by the teaching and learning specialist, may make learning outcomes more explicit to students.
Evidence of the inherent differences between the two modules was highlighted in the student evaluation. In OHP213, one aspect of competence in health promotion is developed through community-based activities.
During the pandemic, the home environment was used as a proxy for the community, resulting in additional and more independent learning activities and assessments. In contrast, the nature of the LOS200 module was such that online demonstrations and video clips could be used to scaffold learning until return to the clinical platform to achieve clinical competence. The different teaching and learning methodologies, coupled with their styles and demands, may explain the varied experiences of students. The duration of LOS200 compared with OHP213, may also have contributed to the difference in experience of students, as the longer contact period with LOS200 allowed students to acclimatise to the 'new norm' as the academic year progressed. Within a context such as ERTE, curriculum planning should be informed by an understanding of the demands of diverse modules.
The global concern for validity and reliability of online assessment has been addressed by some dental schools using IT applications, e.g. LockDown Browser.[15] Such technology, however, may be a challenge for resource-poor countries.
The external review highlights the possible inconsistency of LA as a competence between at least two oral hygiene programmes in SA. It may therefore be useful for oral hygiene programmes to institute collegial review platforms, where subject specialists can develop a common framework to meet minimum standards for competence, particularly clinical procedures as implemented in dental hygiene curricula in the USA.[17]
Emergency remote teaching required HEIs to offer programmes in a new hybrid format. The evaluation of the modules indicated reasonable success, as seen in completion rates, lecturers' perceptions of teaching and students' learning experiences. Hodges et al.[3] caution against using such outcomes as a basis to introduce online teaching as a new norm at contact universities. These authors argue that the lecturer, together with learning and teaching, is but one aspect within a university ecosystem. Other aspects of contact, online or distance universities include library services, different levels of student support and lecturers providing additional support such as mentoring.[3] Therefore, in considering the affordances presented by ERTE, such as lecturers learning new skills, students becoming more independent, spending less time on travelling and being able to study at their own pace, one should consider and research the infrastructure needed. Factors that may need to be examined regarding an expanded university ecosystem include developing appropriate student support systems, building student agency, ensuring that lecturers are informed of the pedagogy of online teaching and learning, providing lecturers with support to develop and administer online learning and monitoring the entire learning process.
Feedback from students on components that were helpful to their learning included the design of the course, followed by comfort with technologies, motivation and time management.[15] Students' views highlighted the importance of effective instructional design for online courses. Reporting on dental student satisfaction with online learning during the COVID-19 pandemic, Wang et al.[1] found that online learning content provided the highest satisfaction, while interaction between teachers and students showed the lowest satisfaction. Factors such as network instability, objective teaching assessments, inefficient online teaching ability and platform instability were noted. A number of these aspects appear to be common to our study. In resource-poor contexts, as seemingly is the case in this study, the use of technology without the necessary support may further hinder success. If online teaching is to be a feature of university education, universities should develop creative spaces for students to study.
Student evaluation systems are routine to the HEI environment, but do not necessarily result in changes in lecturer practices.[18] In this study, feedback indicated that students are able to provide meaningful input into factors that affect their learning and contribute to solutions, as also demonstrated by Brooman et al.[19] Academics, as reflective practitioners, need to determine how such evaluations should be structured and administered to reflect student voice and agency fully.
Contact universities' academic staff with limited experience in the pedagogy or delivery of online learning should upskill themselves rapidly regarding online learning platforms and its demands.[3,4] This view is supported by the stresses and challenges highlighted by lecturers in this study. Hodges et al.[3] liken the experiences to 'faculty feeling like instructional MacGyvers, having to improvise quick solutions in less than ideal circumstances'.[18] Although lecturers reported finding innovative means to conduct online teaching (blended learning), these were noted to be stressful owing to concern for student resources and participation and their own anxieties. Blended learning is potentially a transformative process, requiring careful, thoughtful and informed design inclusive of, but more than the addition of technology.[20]
Remedial efforts by universities such as providing devices and data contribute little to help students living in remote areas where electricity supply is inconsistent and network coverage poor.[4] These concerns were reported in this study. Contextual factors affecting learning appear to be more extensive than in other studies.[1,15] This is particularly evident in the reported loss of family income and insufficient money for basic necessities during the lockdown period. When appraising extended online teaching and learning, universities should take cognisance of these factors.[20]
Conclusions
The curricula were generally found to be aligned in terms of outcomes, content and assessment. The emergency remote teaching presented affordances from the perspective of students and lecturers, which could be explored further. If online teaching were to be a feature of university education, the affordances highlighted by students and staff may argue for a revised hybrid approach to delivering an oral health programme. However, such a system would require thorough research, with the necessary support being built into the university as an ecosystem.
Declaration. None.
Acknowledgements. We acknowledge the contribution of Dr I Moodley, subject specialist, Oral Surgery and Local Anaesthesia (University of KwaZulu-Natal), Ms N Sofala, subject specialist, Oral Health Promotion (University of Pretoria), Dr S Lundie, learning and teaching specialist (UWC) and Dr R Maart, facilitator (UWC).
Author contributions. All authors contributed equally to the article.
Funding. None.
Conflicts of interest. None.
References
1. Wang K, Zhang L, Ye L. A nationwide survey of online teaching strategies in dental education in China. J Dent Educ 2021;85(2):128-134. https://doi.org/10.1002/jdd.12413 [ Links ]
2. Chang TY, Hong G, Paganelli C, et al. Innovation of dental education during COVID-19 pandemic. J Dent Sci 2021;16(1):15-20. https://doi.org/10.1016/j.jds.2020.07.011 [ Links ]
3. Hodges C, Moore S, Lockee B, Trust T, Bond A. The difference between emergency remote teaching and online learning. Educause Rev 2020;27:1-2. [ Links ]
4. Hedding DW, Greve M, Breetzke GD, Nel W, van Vuuren BJ. COVID-19 and the academe in South Africa: Not business as usual. S Afr J Sci 2020;116(7-8):1-3. https://doi.org/10.17159/sajs.2020/8298 [ Links ]
5. Wong TW, Gao Y, Tam WWS. Anxiety among university students during the SARS epidemic in Hong Kong. Stress Heal 2007;23(1):31-35. https://doi.org/10.1002/smi.1116 [ Links ]
6. Greenwood X. South Africa is the most unequal country in the world and its poverty is the 'enduring legacy of apartheid'. The Independent, 4 April 2018. https://www.independent.co.uk/news/world/ africa/south-africa-unequal-counttry-povertty-legacy-aparttheid-world-bank-a8288986.html (accessed 7 February 2022). [ Links ]
7. Statistics South Africa. Housing From a Human Settlement Perspective: In Depth Analysis of the General Household Survey Data, 2002 - 2014. Pretoria: Stats SA, 2016. [ Links ]
8. Shisana O, Labadarios D, Rehle T, et al. South African National Health and Nutrition Examination Survey (SANHANES-1). Cape Town: Human Sciences Research Council, 2013. [ Links ]
9. Van den Berg L, Raubenheimer J. Food insecurity among students at the University of the Free State, South Africa. S Afr J Clin Nutr 2015;28(4):160-169. https://doi.org/10.1080/16070658.2015.11734556 [ Links ]
10. Whittle C, Tiwari S, Yan S, Williams J. Emergency remote teaching environment: A conceptual framework for responsive online teaching in crises. Inform Learn Sci 2020;121(5/6):311-319. https://doi.org/10.1108/ILS-04-2020-0099 [ Links ]
11. Bowen DM, Pieren JA. Darby and Walsh Dental Hygiene: Theory and Practice. 5th ed. Amsterdam: Elsevier, 2019. [ Links ]
12. Harris L, Driscoll P, Lewis M, Matthews L, Russell C, Cumming S. Implementing curriculum evaluation: Case study of a generic undergraduate degree in health sciences. Assess Eval High Educ 2010;35(4):477-490. https://doi.org/10.1080/02602930902862883 [ Links ]
13. Waggie F. Development of an evaluation matrix for a community-based interdisciplinary health-promotion course. Afr J Health Professions Educ 2015;7(1):58-63. https://doi.org/10.7196/AJHPE.432 [ Links ]
14. Tsang AKL. Oral health students as reflective practitioners: Changing patterns of student clinical reflections over a period of 12 months. J Dent Hyg 2012;86(2):120-129. [ Links ]
15. Song L, Singleton ES, Hill JR, Koh MH. Improving online learning: Student perceptions of useful and challenging characteristics. High Educ 2004;7(1):59-70. https://doi.org/10.1016/j.iheduc.2003.11.003 [ Links ]
16. Asiry MA. Learning styles of dental students. Saudi J Dent Res 2016;7(1):13-17. https://doi.org/10.1016/j.sjdr.2015.02.002 [ Links ]
17. McComas MJ, Hurlbutt M, Fontana M. A survey of cariology education in US dental hygiene programs: The need for a core curriculum framework. J Dent Educ 2020;84(12):1348-1358. https://doi.org/10.1002/jdd.12348 [ Links ]
18. Blair E, Valdez Noel K. Improving higher education practice through student evaluation systems: Is the student voice being heard? Assess Eval High Educ 2014;39(7):879-894. https://doi.org/10.1080/02602938.2013.875984 [ Links ]
19. Brooman S, Darwent S, Pimor A. The student voice in higher education curriculum design: Is there value in listening? Innov Educ Teach Int 2015;52(6):663-674. https://doi.org/10.1080/14703297.2014.910128 [ Links ]
20. Mackey J, Gilmore F, Dabner N, Breeze D, Buckley P. Blended learning for academic resilience in times of disaster or crises. J Online Learn Teach 2012;8(2):35-48. [ Links ]
 Correspondence:
Correspondence:
M Cupido
macupido@uwc.ac.za
Accepted 17 January 2022


{kind=link}
{kind=link}
{kind=link}