










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Health Professions Education
On-line version ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.13 n.4 Pretoria Dec. 2021
http://dx.doi.org/10.7196/ajhpe.2021.v13i4.1251
RESEARCH
Teaching about disability and food security in the School of Health Sciences, University of KwaZulu-Natal, South Africa
H E ListerI; K MostertII; M PillayIII
IB Occ Ther, M Dev Studies; Discipline of Public Health, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; and Department of Occupational Therapy, School of Health Care Sciences, University of Pretoria, South Africa
IIBSc PT, MBA, PhD; Department of Physiotherapy, School of Health Care Sciences, University of Pretoria, South Africa
IIIBSHT, MSpPath, DEd; Discipline of Speech Language Pathology, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; and Speech and Language Therapy, Massey University, Auckland, New Zealand
ABSTRACT
BACKGROUND: Food security is a significant challenge in South Africa, especially for persons with disabilities. This topic is therefore important for educators in the health sciences. Nevertheless, little is known about educators' awareness of the relationship between food security and people with disabilities, or to what extent the topic is included in their curricula or what their attitudes are regarding this topic
OBJECTIVES: We explored the knowledge and attitudes of educators pertaining to food security and people with disabilities. We assessed the current teaching practice associated with the food security of people with disabilities in the School of Health Sciences, University of KwaZulu-Natal
METHODS: Thirty-five participants completed a cross-sectional online survey. The participants represented diverse disciplines including audiology, occupational therapy, optometry, physiotherapy, speech-language pathology and sports science. Quantitative data were analysed using descriptive statistics and qualitative data were analysed thematically
RESULTS: The participants had limited self-reported knowledge about the definition of food security. Fewer than 60% of the participants reported a relationship between three of the dimensions of food security and disability, and 80% for one of the dimensions (food utilisation). Of the participants, 88% did not teach food security and disability theoretically, and 80% did not teach it practically. According to the participants, students were not equipped to assess if their clients with disability had food security problems, and were unsure of appropriate interventions
CONCLUSION: Despite a lack of knowledge, participants had positive attitudes towards including food security into their teaching, although limited teaching existed at the time of the study
Food security remains a significant challenge in South Africa (SA), as in other economically developing countries, with persons with disabilities specifically being at risk of inadequate nutrition.[1] In SA, according to the General Household Survey of 2016, 22.3% of households had inadequate or severely inadequate access to food, 11.8% households experienced hunger and 13.4% individuals experienced hunger.[2] Based on the same survey, 4.7% of South Africans aged 5 years and older were classified as disabled.[2] Persons with disabilities are vulnerable to food insecurity, because they are often economically marginalised and therefore chronically poor.[3] The relationships between poverty, food security and disability are bi-directional as one can cause the other.[4-6] For example, poverty results in limited purchasing power for food and limited intake, rendering the individual unable to work, further reducing available income. Malnutrition arising from food insecurity may drive disability in individuals with chronic illnesses, such as HIV/AIDS, further limiting their ability to access, prepare and consume food. Disability may therefore cause poverty and vice versa, especially if there is limited access to healthcare services[7] and inadequate community support.
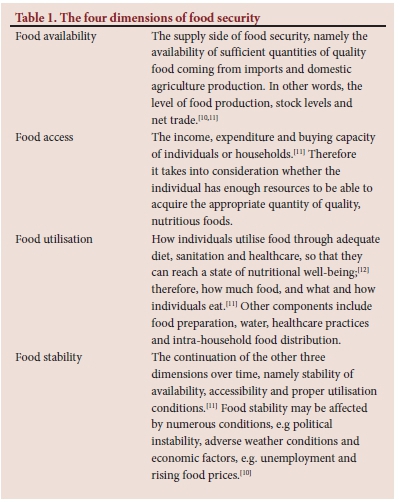
Baro and Deubel[8] argue that community involvement, new technologies and support from both international and national governments and non-governmental organisations (NGOs) are vital to food security responses in Africa. Drimie and McLachlan[9] agree that solving the complex food security challenge requires an explicit transdisciplinary approach, including input from health sciences professionals. Health sciences professionals work with individuals on a one-on-one basis and multidisciplinary teams are often in contact with persons with disabilities. Community healthcare workers should also be aware of and able to assess the nutritional status of persons with disabilities, and be able to identify appropriate interventions to promote food security (Table 1) in these individuals.
Many healthcare professionals work with persons with disabilities, and healthcare students should be trained to assess and work with affected persons. The extent to which the relationship between food security and persons with disabilities is covered in health sciences curricula is unknown, both internationally and in SA. We found no literature on the attitudes of educators towards teaching this subject, even though the subject is societally important. We aimed to discover the knowledge, attitudes and practices associated with including food security and disability into curricula in the School of Health Sciences at the University of KwaZulu-Natal (UKZN).
Methods
We conducted an explorative cross-sectional online survey using closed- and open-ended questions. We structured the questionnaire into three sections, based on a literature review, and input from a statistician, a research expert and an expert in food security. We established content validity by sending the questionnaire to five experts for review.[13] This panel determined whether the questions were understandable, easy to answer and appropriate for what the researcher was wanting to determine. The questionnaire was then piloted with three health sciences professionals not currently employed at UKZN, improving the clarity and content of the instrument.
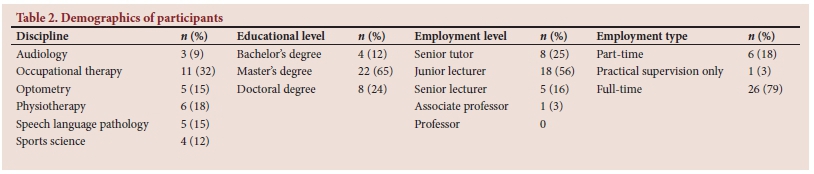
The population comprised all educators whose email addresses were received from the heads of departments within the professions of audiology, occupational therapy, optometry, physiotherapy, speech language pathology and sports science (n=70 in January 2017). A link to the survey, together with the information document and informed consent form, was emailed to all educators. Thirty-five staff responded (response rate of 50%). Table 2 depicts the demographics of the participants.
Quantitative data were analysed using descriptive statistics and qualitative data were analysed thematically using Nvivo 11 software. Themes were established through three-level coding. Data were coded in Nvivo, using the exact words in the text, and descriptively, where the text was described and interpreted by the researcher. The study was approved by the Humanities and Social Sciences Research Ethics Committee at UKZN (ref. no. HSS/1740/016). Gatekeeper permission was also obtained from the registrar of UKZN.
Results
Knowledge of food security and disability
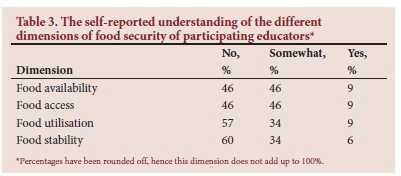
We asked the participants if they understood the different dimensions of food security (Table 1). Participants either answered 'no', 'somewhat' or 'yes', and if they answered 'yes' or 'somewhat', we asked them to elaborate. Table 3 indicates the participants' self-reported understanding of the different dimensions of food security.
Upon further elaboration, the participants understood food availability as having sufficient quantities of food; food that is available (locally and internationally); that there is food being produced; the 'percentage of fats, carbohydrates etc. (that are) contained in food'; or having access to good food for all in a group of people.
Participants understood food access as the ability to 'get' food, through finding the means, being in close proximity, affordability, ease of obtaining, or physical and economic access to nutritious food; all people having access to food; 'the percentage of fats, carbohydrates etc. (that are) contained in the food'; or having 'reliable and trusted access to food'.
Participants understood food utilisation as using food, either how they use it, or 'how the body uses food', how much food is eaten, for what purpose and 'how much of a specific food group' is used; using the 'available channels to access food'; one's ability to eat food that is available; the 'correct consumption patterns of food'; the 'ability of an individual to prepare regular meals using food'; or the ability of a person to choose what food is 'good'.
In addition, participants understood food stability as having sustained and sufficient food in terms of supply, over a period of time, at a given time, consistently and regularly; the shelf-life of food; 'all the variables of food production and supply'; or 'having food and being able to get food and eat food that is available.
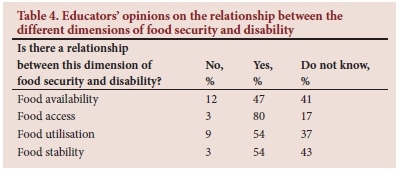
The final questions within this section gauged participants' opinions regarding the relationship between the different dimensions of food security and disability. The dimensions were further explained within the question so that the participants had a clear understanding of the dimensions. Refer to Table 4 for findings.
Five themes, as seen in Table 5, emerged from the data. The categories are represented under the four dimensions of food security.
Attitude about including food security and disability in the curriculum
We provided the participants with 15 items that could possibly be included in the curriculum. We asked participants to rank the items on a scale of 1 to 5, with 1 being 'definitely exclude from teaching' and 5 being 'essential to include in teaching'. Of the 15 items, 10 items were ranked by 80% of participants as either 'important to include in teaching' or 'essential to include in teaching'. These were:
• the definition of food security
• the influence of the social context on food security
• the influence of the environmental context on food security
• the influence of the economic context on food security
• the risk factors of food insecurity
• the consequences of food insecurity
• the macro factors influencing the food security of persons with disabilities
• the micro factors influencing the food security of persons with disabilities
• how to incorporate food security into the assessment of persons with disabilities
• how to incorporate food security into the treatment of persons with disabilities.
Current practice of teaching about the relationship between food security and disability
In the final section of the survey questionnaire, participants were asked, 'Do you currently teach anything about the relationship between disability and food security in clinical settings' practically and theoretically, and 'Do you think students are currently equipped to treat and advise persons with disabilities who have food insecurity problems?'
Theoretical teaching about the relationship between disability and food security
Of the participants, only 11.8% reported that they included something in their teaching about the relationship between disability and food security theoretically and 88.2% said that they did not. Where it was taught, it was done in the study themes 'accessibility issues on disability issues'; incorporating the social and economic context into assessment; within intervention required for visual problems (e.g. glasses) so that the individual with visual problems can see the food; and in referrals to a dietician.
Practical teaching about the relationship between disability and food security
Twenty percent of participants included teaching something about the relationship between disability and food security practically, while 80% did not include anything. The practical teaching occurred within assessment, intervention, and on a case-by-case basis. Regarding assessment, if 'the patient was found to have poor nutrition/low socio-economic status and disability then emphasis is placed on the vulnerability of the patient to this kind of crisis'; it is addressed if there is poor volition of the client to attend therapy and why this may be so; and in incorporating the social and economic context into assessment. Regarding intervention, it was included for those who have visual problems, and referral to the dietician.
Educators' opinion on whether students are equipped to treat and advise persons with disabilities who have food insecurity problems
Regarding the perception of participants on whether students are equipped to treat and advise persons with disabilities who have food insecurity problems, 37.1% stated that they felt students were somewhat prepared and 62.9% felt that students were unprepared. Participants further explained that this situation was a curriculum problem (on why it was not included), that it may be covered in some places, should be included, or even that it should not be included as there was already an overload of teaching. Participants felt that students learn incidentally and should be encouraged to think and treat holistically, and that they should make use of allied team members. In this way, food security is addressed within individualised healthcare, as opposed to only on a larger scale.
These factors are integral to the realisation that it is essential to address disability and food security holistically within health sciences professions.
Discussion
We assessed the knowledge, attitude about inclusion in teaching and the current teaching practice of educators regarding food security and disability in the School of Health Sciences at UKZN. Educators had little theoretical understanding of the different dimensions of food security but once the dimensions were explained, they acknowledged the importance of the relationship between disability and food availability and that it should be included more extensively in the curriculum.
Knowledge: What the educators understood about the relationship between disability and food security
Despite not understanding the different dimensions of food security, health sciences educators showed a general appreciation for the relationship between food security and disability. More than 40% of participants (this study) stated that they did not understand the food security dimension. However, less than 12% of participants did not acknowledge the relationship between the different food security dimensions and disability. We were unable to find literature that specifically links the dimensions of food security to disability. We were, however, able to find examples of how food insecurity drives disability and vice versa. Studies have shown, that food insecurity is associated with reduced physical and mental health status.[4-6] Persons with disabilities experience high levels of poverty and unemployment.[14] This increases food insecurity of the individual and of the household.[5] Food insecurity is also a barrier to accessing health care.[15] The SA Department of Agriculture[16] notes in its 'Integrated Food Security Strategy for South Africa' that access to food may be affected because of disability. Additionally,
malnutrition, considered under 'food utilisation', is a cause of disability.[17-19] Malnutrition can be caused by the inability to feed. Feeding can be impaired through different types of disabilities, e.g. cerebral palsy, which is characterised by low muscle tone that can cause difficulties in swallowing.[20,21]
Attitude: Educator's attitudes to providing instruction about disability and food security
We were unable to find any direct guidelines on what the curriculum content for the various professions within health sciences should be, as well as what is needed in order to intervene appropriately with affected persons. When presented with relevant items to be included in the curriculum, participants placed much importance on these various themes. In SA, especially KwaZulu-Natal Province, almost half of the people live in rural areas. Rural areas are usually low-resource areas, where most of the population relies on subsistence farming, comprise single-income households and have inadequate access to resources. In this milieu, the relationship between food security and disability is vitally important and community health workers need to know how to approach the problem.
Practice: What educators already included in the curriculum about the relationship between disability and food security
We were unable to find any information about what health sciences educators at other institutions teach about the relationship between disability and food security. In this study, we ascertained that, when included, this topic is not taught in a structured, explicit way, but rather as the need arises and as a part of the so-called hidden curriculum. The ad hoc way in which the topic is included also leads to the limited presentation of themes related to food security. For example, one participant teaches about intervention for persons with visual impairments, so that they can see the food (e.g. with glasses); however, visual impairments encompass a much broader range of consequences for food security. These individuals may experience difficulties in shopping, and accessing environments, as well as being able to prepare food and have a variety of food to eat (because of inaccessibility to materials).'221 Food security should be addressed in individualised healthcare, to ensure that the intervention is person-specific, as opposed to being a generic solution. Generic solutions do not cater for individuals who have specific needs. For example, having a food kitchen will not necessarily ensure that a person who requires a wheelchair will be able to access meals.
Study limitations
This study was only conducted at one university. The study did not specify the results of the questionnaire in accordance with the various professions. The implications of including food security and disability into the curriculum may be different according to each profession's scope of practice. We propose that the theory of food security should be included as a generic subject at first- or second-year level, with the theme adapting as students in different disciplines progress.
Recommendations
One of the possible reasons for the lack of content in the curriculum is that the food security of people with disabilities living in rural areas is not currently being studied in SA. The prioritisation of research in this field would promote inclusion into the curriculum.
Further studies should be conducted among the health sciences professions at other universities in SA and cover how to include food security and disability into the curriculum. The health science professions should review how they can intervene with persons with disabilities who are food insecure. These issues should also be discussed with the Health Professions Councils, including a review of the scope of practice, as well as the curriculum of the various disciplines with specific exit-level competencies being identified.
Conclusion
According to the present study, educators had a limited subjective knowledge of food security at a specific School of Health Sciences.
Educators had a somewhat good understanding of the link between the different dimensions of food security and disability and they felt that more should be taught about disability and food security in the School of Health Sciences professions. Including this content should enable students and graduates who deal with persons with disabilities who are at risk of food insecurity. If students learn about this link, they should have the necessary awareness to address food security to be able to intervene with their clients and patients holistically. For example, if someone with a swallowing disability does not have access to appropriate food, teaching them how to eat will not ensure that they receive appropriate nourishment. Therefore, as food security is a baseline challenge which impacts all areas of functioning, rehabilitation can either remain incomplete or be unsuccessful if this basic need is not addressed.
The study raised awareness among participants about the importance of food security and disability. The findings will be used to inform participants of gaps within their curricula, and ensure that this pertinent aspect of disability is addressed in student education. These aspects should be foregrounded by important discussions with the Health Professions Council of South Africa (HPCSA) to address the different disciplines' scope of practice.
Declaration. None.
Acknowledgements. The work reported here was made possible through funding by the South African Medical Research Council (SAMRC) through its Division of Research Capacity Development under the Bongani Mayosi National Health Scholars Programme from funding received from the Public Health Enhancement Fund/South African National Department of Health. The content is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC. Thank you to the SAMRC, the sub-Saharan Africa-FAIMER Regional Institute (SAFRI) for their support of this project by a fellowship granted to the first author, and to the participants of the study.
Author contributions. All authors conceptualised the study. HL completed the data collection, KM and HL analysed the data, and MP reviewed the data analysis. HL wrote the first article draft, and KM and MP contributed to the integration and refinement of information for the article. MP provided the conceptual base for connecting food security and disability.
Funding. None.
Conflicts of interest. None.
References
1. Quarmby CA, Pillay M. The intersection of disability and food security: Perspectives of health and humanitarian aid workers. Afr J Disabil 2018;7(0):a332. https://doi.org/10.4102/ajod.v7i0.322 [ Links ]
2. Statistics South Africa. Statistical Release P0318 General Household Survey 2016. Pretoria: StatsSA, 2016. [ Links ]
3. South African Department of Agriculture. Food insecurity in Sekhukhune. Food Security Information; Brief 1. 2006. http://www.fanrpan.org/documents/d00498/FIVIMS_Info_Brief1_Food_insecurity_Sekhukhune.pdf (accessed 25 May 2017). [ Links ]
4. Siefert K, Heflin CM, Corcoran ME, Williams DR. Food insufficiency and physical and mental health in a longitudinal survey of welfare recipients. J Health Soc Behav 2004;45(2):171-186. https://doi.org/10.1177/002214650404500204 [ Links ]
5. Nord M. Disability is an important risk factor for food insecurity. 2008. https://www.ers.usda.gov/amber-waves/2008/february/disability-is-an-important-risk-factor-for-food-insecurity/ (accessed 20 June 2017). [ Links ]
6. Huang J, Guo B, Kim Y. Food insecurity and disability: Do economic resources matter? Soc Sci Res 2009;39(1):111-124. https://doi.org/10.1016/j.ssresearch.2009.07.002 [ Links ]
7. Elwan A. Poverty and disability. Washington, DC: World Bank, 1999. https://documents1.worldbank.org/curated/en/488521468764667300/pdf/multi-page.pdf (accessed 20 June 2017). [ Links ]
8. Baro M, Deubel TF. Persistent hunger: Perspectives on vulnerability, famine, and food security in sub-Saharan Africa. Annu Rev Anthropol 2006;35:521-538. https://doi.org/10.1146/annurev.anthro.35.081705.123224. [ Links ]
9. Drimie S, McLachlan M. Food security in South Africa - first steps toward a transdisciplinary approach. Food Secur 2013;5(2):217-226. [ Links ]
10. FAO. An Introduction to the Basic Concepts of Food Security Food Security Information for Action. Food Security Information for Action: Practical Guides 2008; 1-3. https://www.fao.org/documents/card/en/c/2357d07c-b359-55d8-930a-13060cedd3e3/ (accessed 20 June 2017). [ Links ]
11. Bajagai YS. Basic concepts of food security: Definition, dimensions and integrated phase classification. Food & Environment http://www.foodandenvironment.com/2013/01/basic-concept-of-food-security.html (accessed 20 June 2017). [ Links ]
12. FAO. Food Security Policy Brief. http://www.fao.org/forestry/13128-0e6f36f27e0091055bec28ebe830f46b3.pdf (accessed 20 June 2017). [ Links ]
13. Lawshe CH. A quantitative approach to content validity. Personnel Psychology 1975;28(4):563-575. [ Links ]
14. World Health Organization. World report on disability. Malta. http://www.who.int/disabilities/world_report/2011/report.pdf (accessed 20 June 2017). [ Links ]
15. Anema A, Vogenthaler N, Frongillo EA, et al. Food insecurity and HIV/AIDS: Current knowledge, gaps, and research priorities. Curr HIV/AIDS Rep 2009;6(4):224-231. [ Links ]
16. South African Department of Agriculture. The integrated food security strategy for South Africa. Pretoria: Government Printer, 2002. [ Links ]
17. Konje JC, Ladipo OA. Nutrition and obstructed labor. Am J Clin Nutr 2000;72(1 Suppl):291S-297S. https://doi.org/10.1093/ajcn/72.1.291S. [ Links ]
18. Kerac M, Postels DG, Mallewa M, et al The interaction of malnutrition and neurologic disability in Africa. Semin Pediatr Neurol 2014;21(1):42-49. https://doLorg/10.1016/j.spen.2014.01.003. [ Links ]
19. Wu L, Katz J, Mullany LC, et al. Association between nutritional status and positive childhood disability screening using the ten questions plus tool in Sarlahi, Nepal. J Heal Popul Nutr 2010;28:585-594. [ Links ]
20. Arvedson JC. Assessment of pediatric dysphagia and feeding disorders: Clinical and instrumental approaches. Dev Disabil Res Rev 2008;14:118-127. https://doi.org/10.1002/ddrr.17 [ Links ]
21. Cox MS, Holm SE, Lynch AK, et al. Specialised knowledge and skills in feeding, eating, and swallowing for occupational therapy practice. Am J Occup Ther 2007;61:686-700. https://doi.org/10.5014/ajot.6L6.686 [ Links ]
22. Muurinen SM, Soini HH, Suominen MH, Saarela RK, Savikko NM, Pitkälä KH. Vision impairment and nutritional status among older assisted living residents. Arch Gerontol Geriatr 2014;58:384-387. https://doi.org/10.1016/j.archger.2013.12.002 [ Links ]
 Correspondence:
Correspondence:
H E Lister
helga.lister@up.ac.za
Accepted 29 October 2020


{kind=link}
{kind=link}