










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Health Professions Education
versão On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.13 no.2 Pretoria Jun. 2021
http://dx.doi.org/10.7196/ajhpe.2021.v13i2.1246
RESEARCH
Improving South African medical curricula related to traditional health systems
C LawrenceI, II; J BollingerIII; K A StewartIV; M MoshabelaV, VI
IMD; Centre for Rural Health, School of Nursing and Public Health, University of KwaZulu-Natal, Durban, South Africa
IIMD; Mount Sinai Hospital, New York City, USA
IIIMSc (Global Health) student; Duke University, Durham, USA
IVPhD; Duke University, Durham, USA
VMB ChB, MFamMed; Centre for Rural Health, School of Nursing and Public Health, University of KwaZulu-Natal, Durban, South Africa
VIMB ChB, MFamMed; Africa Health Research Institute, University of Kwa-Zulu Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Increased co-ordination and co-operation between traditional and biomedical health systems in South Africa (SA) is a national priority. To improve care, practitioners in both systems must learn to recognise the value of their parallel counterparts, and such lessons should begin in medical school. However, there is little research regarding the way in which SA's medical students are taught to interact with the traditional medicine (TM) system
OBJECTIVES: To explore how SA medical students perceive their curriculum as it relates to the traditional health system and to describe their suggestions for improvement
METHODS: We conducted individual in-depth interviews and focus group discussions with 43 final-year medical students across 3 SA medical schools. We applied thematic analysis to improve our understanding of student-reported experiences with TM in their medical school curricula
RESULTS: All 3 medical schools rely heavily on hidden curricula to educate students on the SA traditional health system. These hidden curricula are largely negative and learnt primarily from witnessing faculty-client interactions involving TM use. Students across the institutions agree that this problematic deficit in formal teaching contributes to their incompetence in treating patients who use TM. Their suggestions for improvement focused largely around 3 themes: (i) understanding the fundamentals of the traditional health system; (ii) empathising with patient use of TM; and (iii) promoting broader structural integration of the two health systems
CONCLUSION: Medical students in SA recognise the value of increased exposure to and education surrounding the traditional health system. Future curricular interventions should focus on increasing formal teaching of TM, directly addressing the hidden curriculum related to the topic, and instituting policies and initiatives that improve integration of the SA biomedical and traditional healing paradigms on a structural level
An unexamined education
South African (SA) medical curricula on traditional health systems remain a largely unexamined topic, despite millions of South Africans using traditional healthcare daily. Chitindingu et al's[1] 2014 study outlined the major formal elements of the traditional healing curricula, as described by administrators at each of SA's eight medical schools. Our study aims to answer their call for better understanding of this topic from the perspective of medical students' experience of the curricula - not that of the administrators. Specifically, our study objectives were to determine the hidden curriculum surrounding traditional medicine (TM) in SA medical schools, and how students describe the impact of this hidden curriculum on their perceptions of TM. We define the hidden curriculum as an interpersonal/social concept and a contextual/cultural concept, based on student descriptions of interactions and cultural norms experienced during medical training.[2] Finally, we provide recommendations to mitigate the hidden curriculum's harmful effects, while promoting its more positive aspects.
Broad efforts at integration
Globally, the use of TM is widespread.[3] In SA, TM use is increasingly recognised as an essential element of and opportunity to improve the health of the nation.[4-6] Traditional health practitioners (THPs) have various roles in the healthcare system outside of healing, including spiritual protectors, counsellors and cultural repositories.[5,7] Furthermore, THPs represent an area of under-utilised potential in the fight against HIV/AIDS, particularly due to their overwhelming willingness to engage in HIV/AIDS training and refer patients to biomedical facilities when necessary.[6,8] Discouragingly, however, the tension between biomedicine and TM, largely due to historical injustices, gaps in scientific evidence and mistrust, has resulted in a fragmented and inefficient health system.[6,9,10] Medical schools provide a prime location to combat these challenges, ideally fostering understanding and integration of the two health systems.[1,11] A recent study in Uganda argued that training medical students in the principles of TM was feasible and may improve health outcomes; therefore, integration should not be delayed.[12]
Curricular reforms
Health professions education systems in SA, due to their roots in imperialism, colonialism and apartheid, often produce providers who are incompletely equipped to properly care for many patients, specifically the black African population.[13] Recognition of this deficit has led to a movement to decolonise the nation's graduate education system, including medical schools.[13] Our research aims to look at how we can progress towards decolonisation via integration of traditional health education in medical schools. Although TM is increasingly regarded as a critical element of medical education, much of the recent curricular overhauls has focused on addressing the shortage of medical professionals.[14-16] Solutions to the shortage include the introduction of decentralised medical training and integration of an array of healthcare professionals into the medical system.[15,16] Using a decentralised approach to medical training increases the number of medical professionals receiving training by promoting education outside of tertiary hospitals.[16-18] This approach serves to strengthen primary healthcare and community-based education by producing more medical professionals directly trained in community settings.[16-18] These community sites offer key opportunities for student exposure to TM.[19]
SA health legislation, such as the Traditional Health Practitioners Act 22 of 2007, encouraged the integration of TM into the medical curriculum.[1,20,21] However, these policies have yet to translate into practical integration or large actionable commitments.[5,6] SA is certainly not the first country to struggle with the integration of its various healing systems. In countries around the globe, from Thailand and Taiwan, to the USA and the UK, efforts to adequately train medical professionals are wide spread.[22-25] Ghana, for example, identifies TM experts in the medical curriculum as repositories of indigenous medical knowledge with much to teach health professionals, but SA has no such policy.[26] Chitindingu et al.[1] provided important groundwork by evaluating the inadequacies of the formal medical curriculum relating to TM. Research also demonstrates that the hidden curriculum is often the major force in shaping physicians' professional identity.[27] We aim to describe medical student perspectives on TM and the hidden curriculum, coupled with their own suggestions for its integration into medical curricula. Medical students offer unique first-hand perspectives of the lived experience of the curriculum and its effects on their views of the traditional health system. These data are invaluable in uncovering areas for improvement of the student experience to produce better-prepared future health professionals. This article seeks to use these data to provide concrete recommendations for educators and policymakers to further improve medical syncretism, the harmonious integration of various health systems to improve population wellbeing, both within SA and beyond.
Methods
The study methodology follows the Consolidated criteria for Reporting Qualitative research checklist (COREQ).[28]
Research team and reflexivity
Researchers (CL, BH, NM) interviewed final-year medical students across 3 medical schools in SA: University of KwaZulu-Natal (UKZN), University of the Witwatersrand (Wits) and Walter Sisulu University (WSU). We selected these 3 of 8 medical schools in SA to ensure geographical and demographic diversity. Interviews occurred from October 2015 through June 2016. As part of the broader Transformation in Medical Education (TiME) study facilitated by the Centre for Rural Health (CRH) at UKZN, interviewers were trained in administering the specific questionnaire and other qualitative research techniques during formal training sessions.
Study design
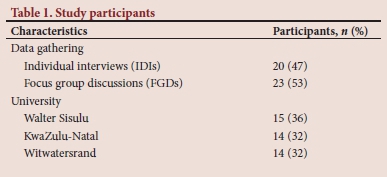
Researchers interviewed 43 participants for the study, 23 during in-depth key informant interviews and 20 across a total of 5 focus group discussions at each institution (Table 1). Interviewees were distributed evenly across the 3 sites: 15 participants from WSU (total estimated class population of 120 students), and 14 participants from UKZN and Wits each (both with total estimated class populations of 250 students).[29] Participants were recruited by convenience sample through email and by word-of-mouth from faculty and current students at the various institutions, with the inclusion criteria being students in their final year at their respective medical schools. Students had to speak English, which is largely a requirement for medical school admission - it was not a problem. Interviews were conducted at each of the 3 medical schools. The questionnaire, developed in conjunction with the CRH, explored students' perspectives on TM and how current medical school curricula shaped or determined these views. Individual interviews (IDIs) and focus group discussions (FGDs) of ~60 minutes were conducted in English, recorded with digital voice recorders and transcribed. The interviewers went through a standardised review of the questionnaire with the principal investigator to ensure that the purpose of each question was clear. After each interview, researchers also wrote field notes to describe their initial impressions, key moments and take-away impressions from the interview. The data were entered into the qualitative research software program NVivo version12 (QSR International, Australia).
Data analysis
The framework analysis technique, derived from applied thematic analysis, was applied to the data using the qualitative data software NVivo.[30] Deductive analysis focused on the interview guide questions according to provided initial codes. The reviewers (JB and CL) used these codes to induce novel codes, synthesised into themes via the NVivo data tree function. After applying these themes to an initial sample of the data, overlay in themes was compared between reviewers to ensure mutual agreement.
Ethical approval
The researchers obtained signed informed consent from all participants. Ethical approval was obtained from Duke University (ref. no. D0195) in the USA and from the 3 SA medical schools involved: UKZN (ref. no. BE466/15), Wits (ref. no. M151191) and WSU (ref. no. 068/15).
Results
Current state of the formal curriculum
'What have you learned in medical school relating to traditional medicine and traditional medicine use?' (Interviewer CL) 'Honestly, I haven't learned anything.' (UKZN FGD B)
The students across all universities in the study cited a lack of a formal curriculum, defined as the medical curriculum knowingly and explicitly planned by the medical school. Although it varied slightly in specifics, the formal curricula across the 3 sites were largely described similarly.
Therefore, unless noted, data reported here are aggregated by location.
Exposures to TM at each school involved a combination of a meeting with or lecture from a traditional healer. This was often remembered as a single lecture, with content that included the importance of TM integration in the biomedical health system and a description of the uses of specific TMs. Students largely described these encounters as low impact, and many participants failed to recall any formal lecture during their medical school tenure. Students at WSU notably described an additional encounter with TM, most likely because they were required to develop and report on a collaborative project with a traditional healer. WSU students enthusiastically endorsed this pedagogical innovation; no students at the other institutions reported on a similar experience.
The hidden curriculum of traditional medicine
'The attitude of doctors - when in that kind of [situation] - is always scorn and distain for the patient that [has] dared see a traditional healer.' (Wits IDI 4)
'The doctors, the nursing staff, everyone. They don't condone it [traditional medicine].' (WSU FGD D)
'Had we come to medical school and been taught that every time we treat a patient, [we must] try as much as we can to incorporate traditional medicine in our management ... that's what we'd be doing. But, we came in, and most of what was told to us about traditional medicine was negative.' (UKZN FGD E)
The majority of students reported that the hidden curriculum was largely a negative influence on their views of both TM and the patients who use the alternative health system. This was the case across institutions. Contributions to this negative impression occurred during students' clinical years. The main factors cited by students were: (i) open criticism of the practices by their clinic preceptors; (ii) witnessing negative effects of certain TMs, specifically in the paediatric population; and (iii) experiencing exasperation at patients hiding TM use during history-taking. There was one notable positive outlier in the hidden curricula, which was that students felt they developed a more complete and less biased understanding of TM when senior students took time to explain its uses and effects during clinical scenarios.
Student proposals for curricular improvement
Participants across the 3 institutions expressed nearly universal motivation for curricular change surrounding traditional healing. Students recognise TM as an integral part of patients' lives and agree that their training creates a largely negative and unhealthy opinion of this alternative healing system. They identified clear deficits and proposed numerous interventions to improve current learning.
Participant suggestions for improvement focused on 3 themes:
(i) understanding the fundamentals of the traditional health system;
(ii) empathising with patient use of TM; and (iii) promoting broader structural integration of the two health systems:
• Fundamentals of traditional health system
'I would love if from the first day that people come [to medical school] that they actually understand that it [traditional medicine] is not purely about the science. It's about the spirituality, which no one addresses,
[either] of the patient or you yourself.' (UKZN IDI 2) '[I'm] not saying whole curriculum now must be all about traditional medicine but . just for us to have a background understanding and when we get to [see] these patients maybe we will understand better where they're coming from, because it's easy for us to just judge them.' (UKZN FGD B)
Students cited a dearth of factual understanding of the fundamentals of TMs, their indications, typical dosing and potential side-effects. Although students understand that they are not intended to be practitioners of traditional health systems, they believe increased teaching regarding the foundations of the system will make them better physicians. These foundations include, but are not limited to, specific examples of TMs, common indications, methods of use and known side-effects. Students recognise that their unfamiliarity with the basics of traditional healing, coupled with their exposure to the hidden curriculum of medical school, creates a largely stigmatising atmosphere for patients using TM and affects patient care. They recognise the harms of these deficits and actively desire curricular remedies.
• Empathising with patient use of TM
'I mean there are patients who tell you, "You know what? I have diabetes. I'm not going to take insulin because I have so much faith in my god." As a doctor, I would come and say, "Listen, if you don't take insulin, you will collapse, and you will die." But they still refuse, so I think the [best] approach would be for students to be taught to reach an agreement [regarding traditional medicines] as opposed to imposing.' (Wits IDI 9) 'It [TM-use] wasn't a good thing ... the doctor would get the history from the nurses and the nurses would shout at a patient like why didn't you come to the clinic? Why did you have to take this? ... What I've seen is never a good response to it [TM-use].' (UKZN FGD B)
The second theme, empathy with patient use, stems from student requests for increased teaching around the reasons why patients use TM, the cultural and religious connection of the practices, and the larger history of the healing paradigm. As reported by the students, their lack of understanding often makes its difficult to interact with TM-using patients in a collaborative fashion and exacerbates stigma and barriers to care. Students find it difficult to empathise with these patients and request training to bridge the divide. As opposed to the first theme, which requires more concrete scientific and historical teaching to increase education on TM, this learning centres on how to create a sphere of mutual respect in the patient-doctor relationship. Similar to their lack of fundamental TM knowledge, the students are aware of their own stigma and request increased training on this topic to mitigate harmful effects.
To address their concerns regarding empathy, participants requested structured learning on how to approach a clinical interaction that involves TM. Much of their learning comes from watching preceptors, which students cited as a largely negative experience. Participants desired step-wise guidance on the clinical encounter, including, but not limited to, how to take a TM patient's history and how to best form a therapeutic alliance with patients who practise traditional healing.
• Structural integration of the healing systems
'Going forward I think ... the government needs to incorporate traditional medicines ... But I think [now] it's just recognizing them, it's not incorporating them. There's a difference between the two ... It will have to be that traditional medicine is taught in all medical schools in South Africa because the government has incorporated it into the health system.' (UKZN FGD E)
Finally, students see themselves as operating within a system unfavourable to integration of the two healing paradigms. They highlight that, although the government and medical institutions often express a desire for integration of the traditional and biomedical, this does not occur in practice. According to students, a more top-down integration would promote a culture of patient respect over patient denigration.
Participants often viewed formal teaching as the main mechanism to improve their understanding of and interaction with the traditional health system. Although students described some formal teaching on the topic, they nearly universally described it as inadequate. They request increased emphasis on longitudinal learning opportunities, such as traditional healing lectures series, discussion groups and increased integration with traditional healers and patients using TM.
Discussion
Proposed curricular interventions
Students are keenly aware of their learning environment surrounding the traditional health system. They recognise its strengths and deficits and its impact on their medical practice. They are willing and motivated to improve their understanding, but look to the medical curriculum to guide this goal. The deficit therefore lies not in the desire of the students, but in the current educational milieu of the medical schools. The focus for improvement must lie largely in addressing curricular deficits, particularly those involving hidden curricula.[31] This does not assume ill-will on the part of medical educators, but instead creates a sense of urgency for further practical research into why such gaps exist despite student motivation. We must move beyond statements of the importance of integration of the traditional and biomedical in health professions and into rigorous evaluation of curricular interventions that succeed at this goal. The proposals of the students, organised into the previously outlined 3 themes, provide a foundation from which to start.
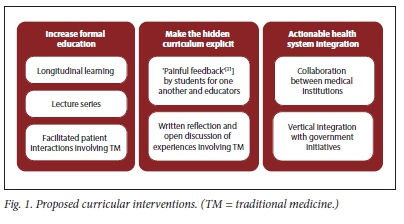
We propose a threefold strategy to address the students' concerns, focusing interventions on 3 levels of medical school organisation: institutional, departmental and individual.[32] These interventions focus on: (i) increasing formal teaching of the traditional health system; (ii) making the hidden curriculum explicit; and (iii) structural integration of the two medical systems (Fig. 1).
Increasing formal teaching of the traditional health system
Students view their lack of formal education as fundamental to their problematic understanding of the traditional health system. We therefore propose that SA medical schools make clear their formal support for a dynamic SA health system that supports integration of the biomedical and traditional healing paradigms, not separation of the two.[6] We support course guidelines that review common TMs, their typical indications and their historical and cultural importance. Teaching sessions should provide students with an opportunity to simulate clinical interactions with patients who use TMs and hone student skills in this regard. Formal examinations should, at some level, include information on traditional health systems. Schools should consider implementing a longitudinal traditional healing component, lecture series, increased interaction with traditional healers and formalised learning from patients who practise TM.
Making the hidden curriculum explicit
Interventions must focus heavily on addressing the hidden curriculum, which students state is largely responsible for their negative, inaccurate and incomplete views of TM. The literature is clear that one of the most effective ways to address the hidden curriculum is to make it explicit.[33-38] We propose that institutions incorporate the idea of 'painful feedback', where students are presented direct evidence of the hidden curriculum's known negative effects to facilitate reflection and promote insulation from these effects.[31] Our study highlights many of these more harmful elements and thus may be used to promote discussion of the current climate and propose suggestions for change. Furthermore, traditional formats of open discussion and written self-reflection protect against negative elements of the hidden curriculum.[39-45] These interventions should occur on multiple levels of organisation, including student-student, student-faculty, faculty-faculty and among learners and patients using TM and practitioners.
Structural integration of SA health systems
There is well-established value in integrating traditional and Western health systems to achieve a mutually respectful co-existence.[9,46-48] Multiple interviewees made note of this point. Medical students will practise what they witness. Therefore, medical schools and healthcare institutions should increase their involvement with broader initiatives, government-sponsored or otherwise. This shift must occur across levels of organisation, both within and across medical schools. These institutions should specifically seek to support initiatives that make clear the value of the traditional health system and collaborate between medical institutions on curricular reforms. Most of the students' curricular complaints and suggestions were similar across the 3 sites, thus idea-sharing between institutions will benefit SA students. Students have demonstrated their desire for this change, and it is now the responsibility of the medical schools to create an institutional culture that propagates respect through all levels of learning.
The shift does not have to occur from the top down, as a response to broad national initiatives or government mandates. Medical schools, faculty and students must advocate for the changes they want to see. The agency of the physicians and future physicians in these institutions is not minimal. Actively promoting integration and leading, e.g. by publicly demonstrating and calling for mutual respect and recognising value in traditional healing, would push the narrative towards one that bridges the two health systems and deconstruct the larger forces that continue to propogate division.
Conclusion
Medical students in SA recognise the value of increased exposure and education to TM. They cite a lack of teaching rather than a lack of student desire as the cause for perceived deficits in knowledge and skills to treat patients using TM. They specifically request teaching regarding the fundamentals of traditional healing, how to empathise with patient use of TM and how to approach such patients during a clinical encounter. We recognise that the solution is not only about changing curricula and student understanding, but about shifting the mindset of faculty. Going forward, it will require investment of faculty, medical institutions and government agencies to accomplish these goals. The national government has stated their interest in bettering the relationship between traditional and biomedical health systems, and SA medical schools need to make the same commitment.[1,21] Improving TM education in medical school will benefit patients and providers and should be a priority for SA education reform.
Declaration. None.
Acknowledgements. We wish to acknowledge members of the Transformation in Medical Education study team, Bonnie Hughes and Neeri Moodley, for their help with interviewing participants. We also acknowledge the College of Health Sciences and US NIH Medical Education Partnership Initiative (MEPI) at the University of KwaZulu-Natal (http://mepi.ukzn.ac.za/Homepage.aspx), the Duke Global Health Institute (https://globalhealth.duke.edu/) and the US Fulbright Fellowship Program. This publication contributes to the hidden curriculum theme of Transformation in Medical Education (TiME).
Authors contributions. CL, KAS and MM made substantial contributions to the conception, design, analysis and drafting of the work. JB made significant contributions to the analysis, interpretation, and drafting of the manuscript. All authors read and approved the final manuscript.
Funding. The sudy was supported by the US Department of State Institute of International Education Fulbright Fellowship Program and the Medical Education Partnership Initiative (MEPI) at the University of KwaZulu-Natal. The study was also supported by the South Africa National Research Foundation (NRF) (grant number 90394) and the US National Institute of Health (grant number 5R24TW008863).
Conflicts of interest. None.
References
1. Chitindingu E, George G, Gow J. A review of the integration of traditional, complementary and alternative medicine into the curriculum of South African medical schools. BMC Med Educ 2014;14(40):1-6. https://doi.org/10.1186/1472-6920-14-40 [ Links ]
2. Lawrence C, Mhlaba T, Stewart KA, Moletsane R, Gaede B, Moshabela M. The hidden curricula of medical education: A scoping review. Acad Med 2018;93(4):648-656. https://doi.org/10.1097/ACM.0000000000002004 [ Links ]
3. Nxumalo N, Alaba O, Harris B, Chersich M, Goudge J. Utilization of traditional healers in South Africa and costs to patients: Findings from a national household survey. J Public Health Pol 2011;32(1):S124-S136. https://doi.org/10.1057/jphp.2011.26 [ Links ]
4. Kasilo O. Traditional African medicine. In: World Health Organization. Traditional Medicine, Better Science, Policy and Services for Health Development: Proceedings of a WHO international symposium, Awaji Island, Hyogo Prefecture, Japan, 2000:86-94. [ Links ]
5. Louw G, Duvenhage A. The present and future roles of traditional health practitioners within the formal healthcare sector of South Africa, as guided by the Traditional Health Practitioners Act No. 22 (2007). Austral Med J 2016;9(12):489-497. https://doi.org/10.21767/AMJ.2016.2725 [ Links ]
6. Moshabela M, Moshabela M, Zuma T, Gaede B. Bridging the gap between biomedical and traditional health practitioners in South Africa. S Afr Health Rev 2016;2016(1):83-92. [ Links ]
7. Zuma T, Wight D, Rochat T, Moshabela M. The role of traditional health practitioners in rural KwaZulu-Natal, South Africa: Generic or mode specific? BMC Complement Altern Med 2016;16(1):304:1-13. https://doi.org/10.1186/s12906-016-1293-8 [ Links ]
8. Zuma T, Wight D, Rochat T, Moshabela M. Traditional health practitioners' management of HIV/AIDS in rural South Africa in the era of widespread antiretroviral therapy. Glob Health Action 2017;10(1):1-12. https://doi.org/10.1080/16549716.2017.1352210 [ Links ]
9. Mokgobi MG. Towards integration of traditional healing and western healing: Is this a remote possibility? Afr J Phys Health Educ Recreat Dance 2013;2013(Suppl 1):47-57. [ Links ]
10. Wreford J. Missing each other: Problems and potential for collaborative efforts between biomedicine and traditional healers in South Africa in the time of AIDS. Soc Dynamics 200;31(2):55-89. https://doi.org/10.1080/02533950508628708 [ Links ]
11. Milan FB, Landau C, Murphy DR, et al. Teaching residents about complementary and alternative medicine in the United States. J Gen Intern Med 1998;13(8):562-567. https://doi.org/10.1046/j.1525-1497.1998.00168.x [ Links ]
12. Mwaka AD, Tusabe G, Orach Garimoi C, Vohra S. Turning a blind eye and a deaf ear to traditional and complementary medicine practice does not make it go away: A qualitative study exploring perceptions and attitudes of stakeholders towards the integration of traditional and complementary medicine into medical school curriculum in Uganda. BMC Med Educ 2018;18(1):1-16. https://doi.org/10.1186/s12909-018-1419-4 [ Links ]
13. Kathard H, Pillay M. Decolonizing health professionals' education: Audiology and speech therapy in South Africa. 2015. https://www.ingentaconnect.com/content/sabinet/aarrhetoric/2015/00000007/00000001/art00010 (accessed 5 February 2019). [ Links ]
14. Bateman C. Doctor shortages: Unpacking the 'Cuban solution'. S Afr Med J 2013;103(9):603-605. https://doi.org/10.7196/SAMJ.7323 [ Links ]
15. Couper ID, Hugo JFM. Addressing the shortage of health professionals in South Africa through the development of a new cadre of health worker: The creation of clinical associates. Rural Remote Health 2014;14(3):1-8. [ Links ]
16. Mlambo M, Dreyer A, Dube R, Mapukata N, Couper I, Cooke R. Transformation of medical education through decentralised training platforms a scoping review. Rural Remote Health 2018;18(1):1-16. https://doi.org/10.22605/RRH4337 [ Links ]
17. De Villiers MR, Blitz J, Couper I, et al. Decentralised training for medical students: Towards a South African consensus. Afr J Prim Health Care Fam Med 2017;9(1):1-6. https://doi.org/10.4102/phcfm.v9i1.1449 [ Links ]
18. De Villiers M, van Schalkwyk S, Blitz J, et al. Decentralised training for medical students: A scoping review. BMC Med Educ 2017;17(196):1-13. https://doi.org/10.1186/s12909-017-1050-9 [ Links ]
19. Mokgobi MG. Western-trained health care practitioners' knowledge of and experiences with traditional healing. Afr J Phys Health Educ Recreat Dance 2014;2014(Suppl 2):1-13. [ Links ]
20. Street RA. Unpacking the new proposed regulations for South African traditional health practitioners. S Afr Med J 2016;106(4):22-23. https://doi.org/10.7196/SAMJ.2016.v106i4.10623 [ Links ]
21. South Africa. The Traditional Health Practitioners Act No. 22 of 2007. [ Links ]
22. Peltzer K, Pengpid S. A survey of the training of traditional, complementary, and alternative medicine in universities in Thailand. J Multidiscip Healthc 2019;12 (1):119-124. https://doi.org/10.2147/JMDH.S189644 [ Links ]
23. Chi C. Integrating traditional medicine into modern health care systems: Examining the role of Chinese medicine in Taiwan. Soc Sci Med 1994;39(3):307-321. https://doi.org/10.1016/0277-9536(94)90127-9 [ Links ]
24. Cowen VS, Cyr V. Complementary and alternative medicine in US medical schools. Adv Med Educ Pract 2015;6(1):113-117. https://doi.org/10.2147/AMEP.S69761 [ Links ]
25. Quartey NK, Ma PHX, Chung VCH, Griffiths SM. Complementary and alternative medicine education for medical profession: Systematic review. Evidence-based complementary and alternative medicine. 2012. https://www.hindawi.com/journals/ecam/2012/656812/ (accessed 5 February 2019). [ Links ]
26. Innocent E. Trends and challenges toward integration of traditional medicine in formal health-care system: Historical perspectives and appraisal of education curricula in sub-Sahara Africa. J Intercultural Ethnopharmacol 2016;5(3):312-316. https://doi.org/10.5455/jice.20160421125217 [ Links ]
27. Hafferty FW. Beyond curriculum reform: Confronting medicine's hidden curriculum. Acad Med 1998;73(4):403-407. https://doi.org/10.1097/00001888-199804000-00013 [ Links ]
28. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19(6):349-357. https://doi.org/10.1093/intqhc/mzm042 [ Links ]
29. Van der Merwe LJ, van Zyl GJ, St Clair Gibson A, et al. South African medical schools: Current state of selection criteria and medical students' demographic profile. S Afr Med J 2016;106(1):76-81. https://doi.org/10.7196/SAMJ.2016.v106i1.9913 [ Links ]
30. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13(1):117. https://doi.org/10.1186/1471-2288-13-117 [ Links ]
31. Austin JP. Trickle-down professionalism: Hidden curriculum and the pediatric hospitalist. Hosp Pediatr 2015;5(6):352-354. https://doi.org/10.1542/hpeds.2014-0180 [ Links ]
32. Chuang AW, Nuthalapaty FS, Casey PM, et al. To the point: Reviews in medical education - taking control of the hidden curriculum. Am J Obstet Gynecol 2010;203(4):e1-e6. https://doi.org/10.1016/j.ajog.2010.04.035 [ Links ]
33. Bignold S. Towards the reflexive medical school: The hidden curriculum and medical education research. Stud High Educ 1999;24(2):195-209. https://doi.org/10.1080/03075079912331379888 [ Links ]
34. Doja A, Bould MD, Clarkin C, Eady K, Sutherland S, Writer H. The hidden and informal curriculum across the continuum of training: A cross-sectional qualitative study. Med Teach 2016;38(4):410-418. https://doi.org/10.3109/0142159X.2015.1073241 [ Links ]
35. Hundert EM, Hafferty F, Christakis D. Characteristics of the informal curriculum and trainees' ethical choices. Acad Med 1996;71(6):624-642. https://doi.org/10.1097/00001888-199606000-00014 [ Links ]
36. Martimianakis MA, Hafferty FW. Exploring the interstitial space between the ideal and the practised: Humanism and the hidden curriculum of system reform. Med Educ 2016;50(3):278-280. https://doi.org/10.1111/medu.12982 [ Links ]
37. O'Callaghan A. Emotional congruence in learning and health encounters in medicine: Addressing an aspect of the hidden curriculum. Adv Health Sci Educ Theory Pract 2013;18(2):305-317. https://doi.org/10.1007/s10459-012-9353-4 [ Links ]
38. Wilkinson TJ. Stereotypes and the hidden curriculum of students. Med Educ 2016;50(8):802-804. https://doi.org/10.1111/medu.13008 [ Links ]
39. Baker M, Wrubel J, Rabow MW. Professional development and the informal curriculum in end-of-life care. J Cancer Educ 2011;26(3):444-450. https://doi.org/10.1007/s13187-011-0199-x [ Links ]
40. Bandini J, Mitchell C, Epstein-Peterson ZD, et al. Student and faculty reflections of the hidden curriculum. Am J Hosp Palliat Care 2017;34(1):57-63. https://doi.org/10.1177/1049909115616359 [ Links ]
41. Chretien K, Goldman E, Faselis C. The reflective writing class blog Using technology to promote reflection and professional development. J Gen Intern Med 2008;23(12):2066-2070. https://doi.org/10.1007/s11606-008-0796-5 [ Links ]
42. Gaufberg EH, Batalden M, Sands R, Bell SK. The hidden curriculum: What can we learn from third-year medical student narrative reflections? Acad Med 2010;85(11):1709-1716. https://doi.org/10.1097/ACM.0b013e3181f57899 [ Links ]
43. Karnieli-Miller O, Vu TR, Frankel RM, et al. Which experiences in the hidden curriculum teach students about professionalism? Acad Med 2011;86(3):369-377. https://doi.org/10.1097/ACM.0b013e3182087d15 [ Links ]
44. Rabow MW, Remen RN, Parmelee DX, Inui TS. Professional formation: Extending medicine's lineage of service into the next century. Acad Med 2010;85(2):310-317. https://doi.org/10.1097/ACM.0b013e3181c887f7 [ Links ]
45. White CB, Perlman RL, Fantone JC, Kumagai AK. The interpretive project: A creative educational approach to fostering medical students' reflections and advancing humanistic medicine. Reflect Pract 2010;11(4):517-527. https://doi.org/10.1080/14623943.2010.505718 [ Links ]
46. Carrie H, Mackey TK, Laird SN. Integrating traditional indigenous medicine and western biomedicine into health systems: A review of Nicaraguan health policies and miskitu health services. Int J Equity Health 2015;14(129):1-7. https://doi.org/10.1186/s12939-015-0260-1 [ Links ]
47. Kesler DO, Hopkins LO, Torres E, Prasad A. Assimilating traditional healing into preventive medicine residency curriculum. Am J Prev Med 2015;49(5 Suppl 3):S263-S269. https://doi.org/10.1016/j.amepre.2015.07.007 [ Links ]
48. Krah E, de Kruijf J, Ragno L. Integrating traditional healers into the health care system: Challenges and opportunities in rural northern Ghana. J Commun Health 2018;43(1):157-163. https://doi.org/10.1007/s10900-017-0398-4 [ Links ]
 Correspondence:
Correspondence:
C Lawrence
carlton_lawrence@hms.harvard.edu
Accepted 1 July 2020

