










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Health Professions Education
versão On-line ISSN 2078-5127
Afr. J. Health Prof. Educ. (Online) vol.12 no.4 Pretoria Nov. 2020
http://dx.doi.org/10.7196/AJHPE.2020.v12i4.1380
RESEARCH
Mentors' and student nurses' experiences of the clinical competence assessment tool
M SserumagaI; A G MubuukeII; J NakiguddeIII; I G MunabiIV; R B OpokaV; S KiguliV
IBMed Educ, MHPE; Rakai Community School of Nursing, Masaka, Uganda
IIPhD; Department of Radiology, School of Medicine, Makerere University, Kampala, Uganda
IIIPhD; Department of Psychiatry, School of Medicine, Makerere University, Kampala, Uganda
IVPhD; Department of Anatomy, School of Biomedical Sciences, Makerere University, Kampala, Uganda
VMMed (Paediatrics), MHPE; Department of Paediatrics, School of Medicine, Makerere University, Kampala, Uganda
ABSTRACT
BACKGROUND. The assessment tool for registered comprehensive nursing was introduced in nursing education in Uganda in 2005 with the main purpose of facilitating nurse mentors to easily assess the clinical competency of student nurses. The tool contributes to the formative and summative assessment of students. Despite continued use of the assessment tool over the years, no study has been conducted to explore the perceptions of nurse mentors and students regarding its use.
OBJECTIVE. To explore the experiences of nursing students and their mentors regarding the clinical competence assessment tool.
METHODS. A qualitative exploratory study design was used. The study was conducted at Masaka School of Comprehensive Nursing in Uganda. The participants included 48 final-year nursing students and 5 nurse/midwifery mentors. Purposive sampling was used to select the participants. Data were collected using 6 focus group discussions with students and 5 key informant interviews with mentors, and thematic analysis was used to interpret the data.
RESULTS. From the responses, the participants generally had mixed experiences of the tool and suggestions were put forward for improvement. Five major themes emerged from student responses: (i) the orientation process; (ii) using the assessment tool; (iii) strengths of the assessment tool; (iv) challenges with the assessment tool; and (v) suggestions for improvement. The nurse mentors generally corroborated what the students reported, i.e. that the tool had challenges when one assesses student performance and gives feedback.
CONCLUSION. The participants reported satisfaction with the design of the assessment tool. However, some challenges were identified regarding its implementation by students and mentors. Key among these were the failure to have immediate assessment and feedback to students. Findings from the study could offer insights on how the tool could be improved.
Nursing education in Uganda has undergone major transformations, from certificate-level training through registration level up to degree level and higher degree level in line with the national health policy of Uganda of training more skilled nurses to address the health needs of the population.[1-4 Through all these training levels, attainment of clinical competency is key. This study focuses on the clinical training in the registered comprehensive nursing (RCN) programme - a diploma-level programme. Clinical training in the RCN programme is guided by the clinical competence assessment tool that should be completed by nursing students after every clinical procedure. Thereafter, nurse mentors are expected to evaluate student competence based on records in the clinical competence assessment tool.
The clinical competence assessment tool was introduced by the Uganda Nursing and Midwifery Council with support from the Ministry of Education to assist students to keep track of their clinical procedures, to assist nurse mentors in evaluating the progressive performance in clinical competency of student nurses and to provide corrective feedback, if necessary. The tool is in the form of a checklist with procedures that the students are expected to perform during clinical rotations.
The nurse mentor observes if the student is able to complete the tasks of a particular procedure. The mentor ticks off each task that is performed correctly, awards a mark and is expected to give some feedback. This is done with all procedures performed by students. The tool resembles a logbook with an assessment checklist. The procedures outlined in the tool are performed on real patients in the wards. However, other aspects of the tool, such as bed making and damp dusting, are sometimes performed outside the clinical ward. The procedures in the tool are spread over 3 years, which is the duration of training for nursing on RCN level. The programme is hospital based. The tool covers most of the nursing procedures expected of a registered comprehensive nurse, such as bed making, patient admission, drug administration, feeding of patients, catheterisation and collecting specimens. A record of having performed these procedures is a requirement for registration with the nursing council. Assessment of this clinical competence tool is also a requirement to successfully complete the nursing course. Although the tool was meant for formative and summative use, it is currently being used only for summative assessment of a student's clinical competency. The clinical nurse mentors receive some orientation on the tool before students present it in the hospital. Nurses lack some of the key clinical skills, which are drivers behind relooking at this tool. However, despite being in operation for several years, perceptions of students and mentors towards its use have not been previously explored, which necessitated the need for this study.
Nurses' attainment of the desired clinical skills is an important part of nursing education. The assessment tool introduced for RCN in Uganda was aimed at aggregating the skills acquired by student nurses in various nursing procedures at different levels of learning throughout the 3 years of their training. The tool contains almost all nursing procedures expected to be performed after qualification. It was designed to facilitate the students' carrying out of procedures under direct supervision of nurse mentors, who then score the students, discuss the assessment outcomes and provide corrective feedback. It was intended to be a mechanism for students to document a portfolio of their progression throughout their clinical rotations, which they then present to the regulatory body for registration. Most of the intentions of this assessment tool have been alluded to in literature.
Various scholars have described an effective assessment tool for nurses. For example, Skúladóttir and Svavarsdóttir[5] suggested that an assessment tool in nursing education needs to be based on nursing care theories and principles. Helminen et al.[6]added that a good assessment tool must have capacity to address the cognitive, psychomotor and affective domains of the learning process. An effective assessment tool must also be able to assess the student's ability to integrate theory and practical procedures at clinical sites.[7] The tool should provide an effective mechanism of giving constructive feedback to facilitate student learning.[8] The quality, utilisation and perception of the tool have to reflect the quality of the nursing education offered, and of the healthcare services eventually delivered.'[9] Therefore, the assessment tool for RCN used in Uganda has to possess all the qualities of a good assessment tool as outlined in literature.
The competent professional nurse should have had acceptable clinical placements, as required by the training institution, and should have been effectively assessed on knowledge, attitudes and skills[10,11] - key aspects that the assessment tool for RCN in Uganda targeted. Teaching without assessment is incomplete, as they complement each other. Training would be regarded as incomplete without effective assessment to judge the nurses' competence.[12,13] As stated above, the assessment tool has never been reviewed, and some of the drivers calling for its review originate from the poor clinical skills of the students, as well as complaints from students and nurse mentors. To inform a more comprehensive review of the tool, including its validity and reliability, there was a need to generate baseline informative data on how the students and mentors who use this tool perceive it. Views obtained from students and mentors can inform future reviews and improvements of the tool. Therefore, the purpose of this study was to explore the experiences of student nurses and their mentors regarding the clinical assessment tool currently used for the RCN programme in Uganda. It is hoped that baseline information obtained will inform not only continuous improvement of the tool, but also future empirical studies on its validity and reliability.
Methods
Research design
This was an exploratory qualitative study. This design was found to be the most appropriate, as the intention of the study was to explore the perceptions of nurse mentors and students regarding the practical assessment tool.
Study setting
The study was conducted at Masaka School of Comprehensive Nursing (MSCN), Masaka, Uganda. MSCN is a rural-based government-aided nurses' training school established in 1946 to train nursing aides. It later started training certificate nurses and RCN students in 1992. At the time of this study, MSCN has 352 students, of whom 104 were in third-year (final group), with 14 nurse mentors.
Participants
The participants were final-year RCN students and their mentors. Some of the nursing students in the RCN programme join directly, while others upgrade from certificate level to RCN diploma level. The mentors are clinical nurse tutors who supervise students during clinical rotations. They were selected purposively, depending on their gender, sponsorship and criteria for entry into the course. Sampling from different categories of participants aimed at achieving maximum variation, where heterogeneity was achieved by representation from each category of the targeted participants.
Data collection
Data were collected using focus group discussions (FGDs) and key informant interviews (KIIs). FGDs were conducted with final-year nursing students. Six FGDs of 8 students in each group were conducted. The FGDs were guided by semi-structured questions. Five KIIs were conducted with nurse tutors. The final number of KIIs was determined at data saturation point, where responses from the tutors became repetitive. The KIIs were conducted in addition to the student FGDs to triangulate data and obtain an explanation from the tutors regarding the responses of students about the assessment tool. Data for the FGDs and KIIs were collected by a research assistant with a social science background and expertise in qualitative data collection and transcribing. The research assistant did not have any relationship with the students or mentors.
Quality control
Data tools were developed by the researcher. These guides were pretested with second-year students to ensure that they were appropriate for the study and that the questions were clear. Unclear question items in the tool were corrected and addressed. During the process of data collection, the interviewer asked questions and the scribe took notes. Audio-recording was done to prevent missing any of the data. To ensure adequate rigour, KIIs and FGDs were used to triangulate the data. There was prolonged engagement with the participants and the developed themes were sent to them to confirm whether their opinions were represented. The researchers ensured reflexivity by bracketing off their own ideas and interpreting information, as reported by the participants.
Data analysis
Thematic analysis was used in this study. Data were immediately transcribed by the investigator following each interview and FGD. The data, being purely qualitative, were analysed through a process of coding, assisted by software R as a platform (qualitative data analytical software).
Ethical approval
Approval to conduct the study was granted by the School of Medicine Research and Ethics Committee, Makerere University (ref. no. REC REF 2019-077). Administrative clearance to conduct the study was obtained from Masaka School of Comprehensive Nursing. Written informed consent was obtained from the participants before they were enrolled in the study. They were also assured of the confidentiality of their responses. Raw data were kept securely by a password, which was only accessible by the researchers.
Results
Demographics
A total of 53 participants were recruited into this study. Of these, 90.6% (n=48) were nursing students and the remaining 9.4% (n=5) were nurse tutors, 56.7% (n=30) were females and 43.4% (n=23) were males. All the participants were familiar with the tool that was being used to assess clinical competency.
Findings from the nursing students
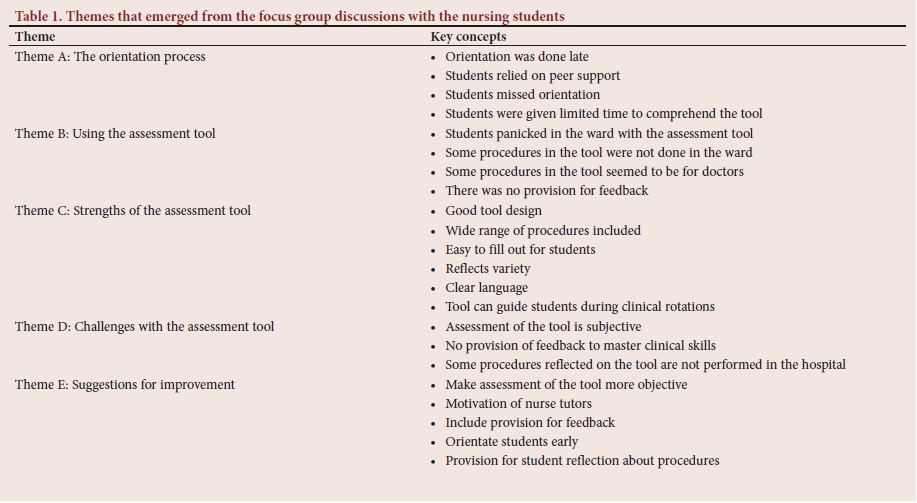
From analysis of the qualitative data, 5 key themes emerged from the FGDs with the students. All the themes related to the perceptions of student nurses towards the assessment tool. Key representative participant quotations have been provided to contextualise each theme. Table 1 summarises these themes.
Theme A: The orientation process
One of the major themes from the FGDs related to the orientation of students regarding the assessment tool. All the students reported that they were orientated with regard to the assessment tool before using it. However, they expressed concern about the orientation process, as it was not explicit:
' The orientation was done and we were introduced to the assessment tool. However, the process was not detailed ... as we were taken through it, some aspects were not touched, such as how the tool is marked and targeted learning goals . and thus did not get to know what was expected of us ... the main focus was put on those areas, which are a bit complicated ... .' (FGD1)
Another key concern regarding the orientation was that it was conducted late and in a rush, without adequate time for the students to comprehend the tool and get to know how to use it:
' The orientation process starts late when we have already commenced our clinical training. Therefore, the tutors rush through the process . and also they give out these books very late when we have already gone through some procedures unrecorded . .' (FGD2)
From the abovementioned responses, it can be seen that student orientation regarding the assessment tool is done late and they are given limited time to fully comprehend the tool before using it in the clinical areas.
From the analysis of the responses, some of the students resorted to consulting their colleagues regarding the use of the tool during clinical procedures, which is a clear indication that the tutors did not orientate the students adequately. The following response resonated through all the FGDs:
'Since we were not properly introduced to the tool, the only option was to consult each other ... those who had got a better understanding of the tool helped other colleagues.' (FGD5)
Participants also felt that the orientation process was conducted when some students were absent. This led to a number of students missing out on this important exercise. This is reflected in the following response:
I remember in the first week when we reported to school, they oriented us about the tool, but many students were missing. No more orientation was done and they just gave us the assessment tool weeks later to use during our clinical practice.' (FGD6).
In summary, the students therefore felt that the process of orientating them with regard to the tool was not adequate to fully comprehend it.
Theme B: Using the assessment tool
The second theme related to the students' experiences of using the tool during clinical training. Students reported that they became too anxious and panicky to complete the tool. Using and filling out the tool became a challenge during clinical procedures, because the nurse tutors (preceptors) were too busy and could not adequately supervise completion of the tool. The following responses reflected these observations:
'It was a tense moment in the clinical ward to complete the tool because we had not been properly introduced to the tool and yet as finalists, we had to complete the tool . so when it usually comes to the finalists, the students usually panic to sign the assessment tools ... .' (FGD6)
'The nurse tutors who were supposed to supervise our clinical work were most times too busy to guide us during procedures and also to guide us on how to accurately fill out the tool. This caused a lot of panic among us and yet we needed these tools filled up.' (FGD3)
It was also observed that the assessment tool might not have reflected what was on the ground as far as some procedures were concerned and it contained procedures that were no longer performed; yet, students had to log them into the tool. In addition, there was no time for feedback regarding the procedures performed. These observations can be seen in the following student responses:
' During ward rotations, using the tool sometimes proved a challenge because it contained nursing procedures that are not done any more or some procedures that are not done by nurses. This was challenging because you could not fill in these procedures and yet the tutors were asking for them.' (FGD4)
' Lack of feedback from our tutors was a big challenge. The assessment tool had no provision for feedback and the tutors were also busy on the ward and they could not give us feedback as we wanted in time.' (FGD2)
From the abovementioned responses it can be observed that using the tool in the real clinical context seemed to be a challenge to the students owing to a number of factors, such as limited feedback, busy clinical setting and anxiety.
Theme C: Strengths of the assessment tool
This theme is about the strengths of the assessment tool from the students' point of view. Despite the weaknesses of the assessment tool, some strengths were reported. Key among these were that the tool design and organisation to record most of the procedures performed and the coverage of skills required within the tool seemed to be wide:
'The assessment tool has a wide variety of nursing clinical procedures that we are supposed to cover and this at least guides us on what we should look out for. This is good and if our mentors were always present for us as the procedures are performed, and after for feedback, this would be a good tool for us.' (FGD6)
Most of us think it is a good tool, especially when it comes to the way it is organised with most skills required incorporated within. Its content coverage for all competencies including attitudes is good. Its design and language used are also easy to use, especially that the wards are always busy and we have to perform procedures as we fill the tool for later assessment.' (FGD1)
From the abovementioned observations, it therefore appears that the design of the tool and nursing skills captured by the tool seem adequate and met the expectations of the students.
Theme D: Challenges regarding the assessment tool
Despite the observed strengths of the assessment tool, the students also reported some challenges. The key challenges seemed to rotate around the assessment of the procedures and feedback. The following responses reflected this theme:
' The marking of the recorded nursing procedures has bias because the tool is marked way after procedures were done and recorded and the tutors lack the time to devote to the supervision of the students and mark the tools according to their familiarity.' (FGD3)
' In many situations, the tutors on wards are busy and we also get busy, so we just fill in procedures for the sake of completion and these tools are looked at by the tutors weeks after procedures are done or even at the end of the semester. When they start marking, it is hard for them to objectively mark you.' (FGD6)
'The issue of feedback needs serious attention. We are not given feedback that can help us in future procedures because tutors look at these tools way after procedures. This immediate feedback that is important is not there since tutors are few. Even the tool itself has limited opportunities for tutors to write feedback comments for the students.' (FGD1)
There were also challenges, as the tool included procedures that were not performed in the wards; yet, students were required to fill in the procedures. Students reported that there was always inadequate medical equipment and supplies, as well as a limited number of supervisors required for proper administration of the assessment tool:
' When it comes to the practice, you cannot apply the standards of the book because health centres lack some instruments.' (FGD2)
From the abovementioned responses, it can be demonstrated that the major challenge with the tool seemed to be the subjectivity of assessment, which at times used to happen several weeks after the students had completed the tool.
Theme E: Suggestions for improvement
All participants recognised that the tool needed to be improved. This theme gives suggestions of students for improving the tool. The key suggestions that resonated through the FGDs related to improving the orientation process so that students are introduced to the tool early, thus improving the assessment of the tool, as well as provision of feedback, motivation of mentors to supervise the completion of the tool during clinical practice, revising the tool to eliminate any outdated procedures and provision of a mechanism in the tool for students to reflect on their clinical procedures:
'One way to improve the utilisation of this tool is that we should receive the books the moment we come to start the course . .' (FGD2) 'The mentors who are supervising the students need to be motivated in order to ensure that students fill out the tool and they get feedback from them . the mentors seem unmotivated. The feedback for the procedures carried out needs to be given early enough when it is still useful to facilitate our learning. In addition, the marking of the tool needs to be looked into. Currently, the marking is subjective as tutors mark our work many weeks after the procedure when a student cannot do much corrective action.' (FDG3) 'We need to think about the procedures we do and also give feedback to the tutors. We should include a provision for students' remarks in the tool so that we can write the situation where we perform the procedure and comment on the score.' (FGD6)
Findings: Nurse tutors
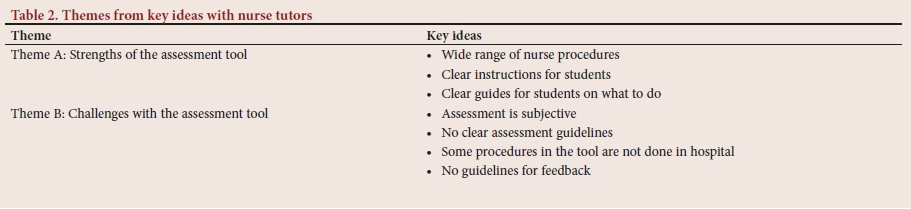
Five KIIs were conducted with nurse tutors in addition to the FGDs with students to gain a better understanding of how the students responded from the perspective of the teachers, who used the assessment tool to evaluate the students' clinical competency. An exploration of the perceptions of the nurse tutors generated two themes (Table 2).
Theme A: Strengths of the assessment tool
One of the themes that emerged from the interviews with the nurse tutors was about the strengths of the assessment tool. As with the students, the tutors reported that the tool provides for a wide variety of nursing procedures expected of students, thus making it more suitable to use. The other strength of the tool is its clarity and ability to guide students during clinical rotations. The following tutors' responses captured these strengths:
' The assessment tool is very important because it was designed with a wide range of clinical procedures, thus giving students an opportunity to capture all procedures participated in.' (P1)
'The current assessment tool was designed to enable students to participate in many examinations and record them. It contains all examinations expected of a nurse at registered level to know.' (P2) 'The tool is written in clear language, which gives students an opportunity to follow. In addition, every procedure has clear instructions on what to do and document, making it suitable for students to use even in the absence of nurse supervisors.' (P5)
The mentors seemed to agree that the tool has a wide variety of nursing procedures that students are expected to perform and it has clear instructions for students to follow.
Theme B: Challenges regarding the assessment tool
Another theme highlighted by the nurse tutors related to challenges regarding the assessment tool. All the nurse tutors felt that the tool lacks guidelines on how to objectively assess the students, which often leads to subjective assessment. This was particularly manifested when tutors assessed the records of students several weeks after they had filled in the tool:
'The assessment of student performance with this tool is still a challenge. Many times we are busy and it is difficult to assess students as they fill in the tool. This forces us to look at the tool weeks after students have recorded procedures. Unfortunately, it is difficult to remember what exactly they were able to perform, especially when it comes to specific details of the procedure.' (P3)
'There is a lot of subjectivity while evaluating student performance using this tool. In addition, the tool has no clear assessment guidelines for us as tutors for both formative use as well as summative use, yet I think the tool is intended for both functions.' (P4)
The tutors also reported that the tool lacks clear guidelines on how to give feedback to students, and some of the procedures in the tool are not done in the hospital; yet, students are required to record them:
'Most of us are not trained in giving feedback and the tool lacks clear guidelines for us to give feedback to students. This combined with the fact that we are few on the ward makes giving feedback to students very difficult.' (P1)
'The tool is comprehensive enough; however, there are many procedures included in the tool that are not performed in the hospital. At the same time, some of the procedures are not performed because there are other better procedures. Therefore, perhaps the tool needs to be revised to bring it up to date.' (P4)
From these abovementioned responses, therefore, the assessment tool has some challenges, despite various advantages. The challenges pointed out by the nurse mentors correspond to what the students pointed out. Key among these are the subjective assessment, as well as limited opportunity to deliver immediate corrective feedback to support learning.
Discussion
The purpose of this study was to explore the experiences of student nurses and their mentors regarding the clinical competence assessment tool. Findings demonstrated that the students received orientation regarding the tool. This orientation process assisted them to become familiar with the tool and its requirements. The importance of such an orientation process before implementation of the assessment tool has also been emphasised in studies by Helminen et al.[6]and Baumgartner et al.[12]These scholars reported that mentors and students need to be orientated with regard to any type of assessment the tool before maximum benefit is achieved. Orientation will possibly achieve the following: students are given an opportunity to become familiar with tool and what is required of them. Any questions that arise can then be addressed before the tool is applied in the clinical setting. However, the findings revealed some drawbacks. The orientation process seemed to have missed addressing some of the student expectations, such as targeted learning goals and outcomes, as well as criteria for scoring student performance. Such discrepancies in the orientation process of students and faculty towards the use of the assessment tool can therefore influence its effectiveness. The implication for nursing education is that any assessment method for clinical skills needs to be explained to the students. Filling in the assessment tool forms part of the requirement for professional registration, which further strengthens the importance of properly introducing the tool to the students. Some of the students missed the orientation session -perhaps because they had not reported to school during the first year. There is a greater need to phase in the orientation sessions to ensure that all students benefit. Doing it once during the first year for a tool that is supposed to be used over 3 years, needs attention. The goal of the tool is to ensure that students use it to track their attainment of the desired nursing procedures. Therefore, periodic debriefing sessions with the students should be considered.
As alluded to in this study, peer-to-peer support in utilisation of the tool is important, especially when senior students guide junior students on how to use it. There are too few nurse mentors compared with students. Therefore, the possibility of senior students mentoring junior students in using the assessment tool may be one way of addressing this challenge. In most situations, senior nursing students have probably gone through a similar assessment process using a similar tool. Therefore, they can be a great resource in mentoring their junior colleagues on the use of the tool so that students can attain the desired outcomes. This suggestion is in agreement with that in a previous study, which emphasised the benefit of peer mentoring, where senior students assist junior students, thereby empowering them to provide constructive feedback during the learning and mentorship process.[14]
It was also noted that there is a need to increase awareness regarding the importance of assessment, particularly when using the tool that has been designed to track and monitor student progress. The assessment of the tool seemed to be rather subjective, as pointed out by students and mentors. This calls for the training of mentors on how to conduct assessment using the tool. Although it would have been good for formative assessment, the mentors seemed to have used it for summative purposes, which was subjective. To reliably evaluate the achievement of competency in nursing procedures, there should be an objective way of assessing the tool. For example, use of standardised checklists that specify important aspects is key. In addition, faculty need to be trained on how to assess the tool through participatory and interactive workshops, e.g. McCarty and Higgins[15] advised that mentors should be prepared for their complex and demanding roles, especially how they view the assessment tool and how such a tool can be effectively used to facilitate the learning process. Part of this preparation can therefore be achieved through training. There was also a challenge with provision of feedback to the students. Corrective feedback is paramount, especially when students are learning clinical skills. The assessment tool had no guidelines for delivering feedback to students. It was also observed from the interviews with mentors that they lacked skills on how to provide feedback. One way of addressing this challenge is to include some structured guidelines in the tool on aspects with regard to feedback. Leaving it open to mentors creates some gaps, which unfortunately impacts on effective learning. Another solution would be to train mentors on how to deliver feedback and what particular aspects to focus on.
As observed from this study, some students occasionally became too anxious and panicky in an effort to complete the assessment tool, probably because the tool is later needed for professional registration. Students were also possibly anxious because they had not received adequate orientation regarding the tool. This finding requires urgent attention, because assessment is meant to facilitate learning and not to create panic among learners. Therefore, nurse mentors and clinical preceptors are potentially needed to guide and mentor the students. It can be argued that it is the responsibility of mentors to facilitate, coach and guide students to perform nursing procedures, create a supportive and motivating learning environment and evaluate the performance of student nurses through the use of the assessment tool. This calls for training of mentors - also on how to guide the students as they implement the tool. Such preparation is necessary if valid and reliable decisions are to be made about the students' competency based on the assessment tool.
There are definitely more challenges in using the assessment tool, which involve the clinical setting and the educational process. The same observation has been reported in the literature, i.e. that challenges continue to exist in the clinical setting despite the assessment tool possibly being effective.[16] Challenges were observed, such as laziness of students to complete the assessment tool and record procedures, failure to allocate procedures per semester, inclusion of rare and obsolete procedures in the assessment tool, limited time of mentors, who sometimes sign off procedures that have not been performed, and increasing numbers of students in the clinical wards. All these challenges may limit the effective implementation of the assessment tool in the clinical setting. One way of mitigating this could be to have a timetable of student rotations on the wards, to train nurse mentors and to occasionally use senior students to mentor junior students. The study findings therefore concur with those of Al-Kadri et al.,[14] who observed that mentors can empower students through provision of effective feedback to their peers.
If such challenges are not addressed, the implementation of the assessment tool becomes ineffective. For example, from this study it was shown that at times the scores within the assessment tool did not reflect students' competencies. Morgan[7] argued that any effective assessment tool must be able to assess the students' ability to integrate theory and practical procedures in clinical settings. Overall, it has been shown that, although we may design very good assessment tools to evaluate the competency of nurse trainees, such tools may be ineffective if they are not properly organised and if nurse mentors and students are not satisfactorily orientated or trained to use the tool. Provision of feedback is crucial. Clinical nursing procedures are important for any professional nurse. Assessment of mastery of those procedures is perhaps even more crucial. Findings from this study open up a debate regarding nursing education and particularly regarding learning and assessment of clinical nursing skills. The question arises whether the tool discussed in this study is best for assessing acquisition of clinical nursing skills and using it as a regulatory framework for registration. With key drawbacks identified, such as unreliable assessment, suboptimal orientation regarding the tool, limited feedback and subjective assessment, the need to rethink how nurse educators assess clinical skills is important. Going forward, using a tool such as a learning portfolio may be more important than including students' reflections of their learning. This could be combined with other assessments of clinical competency, such as an objective structured clinical examination (OSCE), which can contribute to requirements for registration rather than solely relying on records logged into a paper tool. Therefore, this study highlights some key issues that all nursing institutions need to give some thought as they design effective assessment tools to evaluate clinical and practical competency for nurses, especially when such assessment forms part of the requirements for certification to practise independently.
Study limitations
Despite the observed strengths and positive insights that have emerged from this study, there are some limitations. It was carried out in only one nurse training institution, whose context might be quite different from other nursing institutions globally. There could be other context-specific factors that contributed to study observations. This, coupled with the small number of participants, may limit the generalisability of the findings to many other settings. However, the findings generate important insights regarding assessment of nurse clinical competency, especially when educators design assessment tools. Important key issues have been generated in this study.
Further research
There are implications for further research, e.g. this study focused on exploring the perceptions of nurse mentors and students regarding the clinical assessment tool. However, further research is needed to evaluate the reliability and validity of the tool. More empirical studies focusing on this direction in many more settings are therefore encouraged.
Conclusions
The students and mentors generally had positive perceptions towards the assessment tool, and participants appreciated its design. The tool had adequately covered all domains in the curriculum. However, orientation regarding the tool was inadequate and affected its applicability in the clinical environment. It lacked a sufficient structured guide for rating student competency in procedures, thus occasionally making the assessment largely subjective. Mentors were not able to mark and sign the tool immediately after a procedure, as required. Some procedures were rare and others outdated. However, there were procedures that were frequently performed by students during their placement, but which were not included in the tool.
Declaration. None.
Acknowledgements. Special thanks go to the students and mentors who participated in this study.
Author contributions. MS: conceptualised and developed the idea, drafted the protocol, collected data, participated in the analysis and wrote the initial draft; AGM: participated in the analysis, refined the methodology, did critical reading and refined the final manuscript; JN: participated in refining the methodology and data analysis; IGM: refined the initial manuscript draft and assisted in the analysis; RBO: participated in the analysis and refined the manuscript draft; SK: assisted in refining the methods and proofread the final manuscript.
Funding. Research reported in this publication was supported by the Fogarty International Center of the National Institutes of Health (NIH), US Department of State's Office of the US Global AIDS Coordinator and Health Diplomacy (S/GAC), and the President's Emergency Plan for AIDS Relief (PEPFAR) (award no. 1R25TW011213). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflicts of interest. None.
References
1. Uganda Ministry of Health. Scheme of Service for the Nursing and Midwifery Cadre. Kampala: Ministry of Public Service, 2017. [ Links ]
2. African Medical Research Foundation. Registered comprehensive nursing curriculum. 1994. moodle.amref.org (accessed 10 January 2017). [ Links ]
3. Uganda Ministry of Education and Sports. Registered Comprehensive Nursing Programme. Kampala: Uganda Ministry of Education and Sports, 2004. [ Links ]
4. African Medical Research Foundation. Practical competence assessment tool for registered comprehensive nursing course. 2005. moodle.amref.org (accessed 17 January 2017). [ Links ]
5. Skúladóttir H, Svavarsdóttir MH. Development and validation of a clinical assessment tool for nursing education (CAT-NE). Nurse Educ Pract 2016;20:31-38. https://doi.org/10.1016/j.nepr.2016.06.008 [ Links ]
6. Helminen K, Coco K, Johnson M, Turunen H, Tossavainen K. Summative assessment of clinical practice of student nurses. A review of the literature. Int J Nurs Stud 2016;53:308-319. https://doi.org/10.1016/j.ijnurstu.2015.09.014 [ Links ]
7. Morgan R. Using clinical skills laboratories to promote theory-practice integration during first practice placement: An Irish perspective. J Clin Nurs 2006;15(2):155-161. https://doi.org/10.1111/j.1365-2702.2006.01237.x [ Links ]
8. Ramani S, Leinster S. AMEE Guide No. 34: Teaching in the clinical environment. Med Teach 2008;30(4):347-364. https://doi.org/10.1080/01421590802061613 [ Links ]
9. Mansour M. Current assessment of patient safety education. Br J Nurs 2012;21(9):536-543. https://doi.org/10.12968/bjon.2012.21.9.536 [ Links ]
10. Embo M, Driessen E, Valcke M, van der Vleuten CP. Integrating learning assessment and supervision in a competency framework for clinical workplace education. Nurse Educ Today 2015;35(2):341-346. https://doi.org/10.1016/j.nedt.2014.11.022 [ Links ]
11. Museene HS, Mayers PM. A structured and collaborative clinical teaching training program for nursing preceptors in Uganda. 2016. https://sigma.nursingrepository.org/handle/10755/616445 (accessed 20 February 2018). [ Links ]
12. Baumgartner R, Häckter Stâhl C, Manninen K, Rydholm Hedman A. Assessment of nursing students in clinical practice. An intervention study of a modified process. J Nurs Educ Pract 2017;7(11):111. https://doi.org/10.5430/jnep.v7n11p111 [ Links ]
13. Yonge O, Billay D, Myrick F, Luhanga F. Preceptorship and mentorship: Not merely a matter of semantics. Int J Nurs Educ Scholar 2007;4(1). https://doi.org/10.2202/1548-923X.1384 [ Links ]
14. Al-Kadri H, Al-Moamary MS, Al-Takroni H, Roberts C, van der Vleuten CP. Self-assessment and students' study strategies in a community of clinical practice: A qualitative study. Med Educ 2012;17(1):11204. https://doi.org/10.3402/meo.v17i0.11204 [ Links ]
15. McCarty M, Higgins A. Moving to an all graduate profession: Preparing preceptors for their role. Nurse Educ Today 2003;23(2):89-95. https://doi.org/10.1016/s0260-6917(02)00187-9 [ Links ]
16. Wade GH, Hayes E. Education: Challenges and opportunities associated with preceptored community health clinical experiences. Public Health Nursing 2010;27(5):459-467. https://doi.org/10.1111/j.1525-1446.2010.00879.x [ Links ]
 Correspondence:
Correspondence:
A G Mubuuke
gmubuuke@gmail.com
Accepted 13 August 2020


{kind=link}
{kind=link}