










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkThe African Journal of Information and Communication
versão On-line ISSN 2077-7213
versão impressa ISSN 2077-7205
AJIC vol.29 Johannesburg 2022
http://dx.doi.org/10.23962/ajic.i29.13756
Digital Vaccination Records: Exploring Stakeholder Perceptions in Gauteng, South Africa
Wesley MoonsamyI; Shawren SinghII
ILecturer, Department of Information Systems, College of Science, Engineering and Technology (CSET), University of South Africa (UNISA) Science Campus, Johannesburg https://orcid.org/0000-0003-4285-236X
IIAssociate Professor and Chair ofInformation Systems Department, School of Computing, University of South Africa (UNISA) Science Campus, Johannesburg https://orcid.org/0000-0001-5038-0724
ABSTRACT
Electronic health (eHealth) is one of the focus areas of the South African Department of Health (DoH), with the ultimate goal being the development of an electronic health record (EHR) for every citizen. A commonly used subset of eHealth data, vaccination records, is still not yet fully digitised in South Africa. This study aimed to determine the perceptions of key stakeholders (doctors, nurses, parents, and school administrators) about a digital system for vaccination records for minors in South Africa's Gauteng Province. Using a prototype online, cloud-based vaccine records management system created during the research, called e-Vaccination, quantitative and qualitative interaction-related data from 118 participants were collected using a five-point Likert-scale questionnaire. The questionnaire was based on Lund's (2001) USE user perception framework, which considers usefulness, satisfaction, ease of use, and ease of learning. This study found that the participants supported the use of the digital vaccine records management system, with an emphasis on five identified factors: user friendliness, graphical design, practicality, user experience, and usability. Accordingly, this article recommends that policymakers and system designers carefully consider these factors in the design and development of South Africa's digital vaccination records management system.
Keywords: vaccination records, eHealth, digitisation, health information systems, user perception, USE framework, Gauteng, South Africa
1. Introduction
The recent fire at one of South Africa's largest academic hospitals, Charlotte Maxeke Johannesburg Academic Hospital (Motara, Moeng, Mohamed, & Punwasi, 2021), as well as the riots in the KwaZulu-Natal and Gauteng Provinces-in which organisations, including pharmacies and healthcare facilities, were looted and vandalised (South African Government, 2021b)-highlight the need to secure vital medical information such as patient records. Information that is exclusively stored on local servers, on hard drives, and in paper-based files is at risk of total loss during such events and other disasters.
An increasingly critical subset of patient information, vaccination records, has shown a hastened conversion to a digital form as a result of the COVID-19 pandemic (GAVI, 2020). There are several "patient-facing" health information systems in South Africa, including MomConnect and B-wise (DoH, 2020b; Health Enabled, 2021). A new addition to these disparate systems is the Electronic Vaccination Data System (EVDS), which was created as a self-registration portal that allows South Africans to register to receive their vaccination against COVID-19 (South African Government, 2021a).
The hybrid EVDS, with a digital back-end but a physical vaccination card handed to a patient once the vaccination has been administered, allows the government to track and monitor the COVID-19 vaccination rollout. This hybrid approach, however, does not give the patient easy access to a digital version of their vaccination record as it requires the proof of vaccination code, which can easily be misplaced. Decades since the first physical vaccination cards were handed to patients, South Africans must continue to store their physical vaccination cards safely, even with expensive technology having been created to register the patient. Such systems lack patient-centeredness, which is the key to eHealth (Nyatuka & De la Harpe, 2022).
Immunisations are one of the greatest success stories of modern medicine (WHO, 2019). The study considered the grassroots level of vaccines and focused on the digitisation of vaccination records for some of the most vulnerable in our society: minors (from new-born to 12 years of age). The research therefore focused on South Africa's expanded programme on immunisation (EPI) schedule (DoH, 2018). (The research did not focus on the COVID-19 vaccinations because adult vaccination records storage is at the infancy stage in South Africa.)
This study commenced by determining the main challenges associated with the paper-based vaccination card in Gauteng. This was followed by an assessment of how vaccination records are stored by government and non-government entities globally. The eHealth aims of the DoH were then investigated. Based on information collected, a prototype online digital vaccine records management system, named e-Vaccina-tion, was developed and tested with key stakeholders to determine their perceptions of the system. This was achieved by a questionnaire comprising of three sections. Section A was used to collect demographic information, section B collected perceptions of vaccinations in Gauteng, South Africa, and Section C collected user perception (usefulness, satisfaction, ease of use, and ease of learning) information based on the USE tool (Lund, 2001. In addition to these four categories, one more user perception category (design and visual aids) was added due to the graphical nature of e-Vaccination's user interface. The questionnaire was guided by the study's core research question: What are the perceptions of the key stakeholders about replacing the paper-based vaccination card with a digital vaccination record system?
2. Challenges with paper-based vaccination cards
Paper-based records are prone to damage or total destruction by disasters such as fires and flooding. In addition to this, South Africa experienced civil unrest during 2021, in which some healthcare facilities were looted and vandalised. In certain cases, patient records were stolen or damaged. These events fall under the vulnerability challenge. Another challenge, accessibility, has also been noted. In some instances, the vaccination card, which has been the primary storage mechanism for over three decades, has to be presented to a healthcare worker for medical purposes or to school administrators for admission to a school. If the card is not available, the vaccination records cannot be accessed easily. Another challenge related to the use of paper-based vaccination records is the reliability of the data. Handwritten paper-based records are prone to human error and have the added disadvantage of being illegible. This can also cause downstream digital records captured from this medium to be incorrect. Processes that load vaccination records as daily, weekly, or monthly batches cannot provide real-time information. These scenarios result in information that is not always reliable. These three main challenges are further explained in Table 1.
3. Management of vaccination records
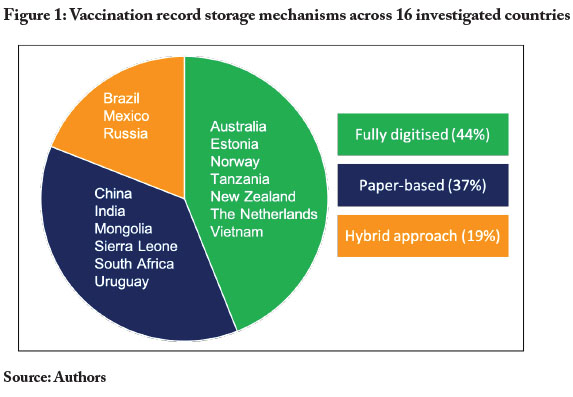
An investigation of 16 countries (developed, developing, and countries in transition) was carried out to determine how they managed their vaccination records. The findings were categorised as follows:
• Fully digitised - A child's entire vaccination record can be accessed with or without the presence of the vaccination card. The card merely serves as proof for the parent or guardian.
• Paper-based - The primary storage mechanism is a paper-based vaccination card or other paper-based documents.
• Hybrid approach - A digital system that stores the vaccination records does exist, but it is not updated in real-time and, healthcare practitioners, as well as parents, cannot access these records. The primary storage mechanism remains the vaccination card.
The investigation revealed that 44% of the investigated countries had a fully digitised storage mechanism whilst 37% were paper-based and 19% used a hybrid approach. This is illustrated in Figure 1.
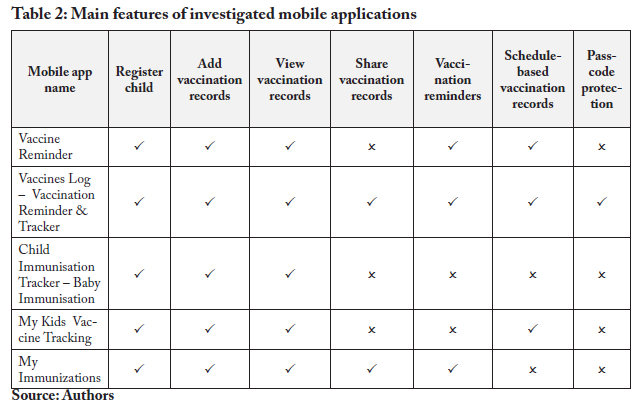
In addition to determining how other countries managed their vaccination records, non-government-related initiatives, such as mobile applications (apps) that can be downloaded from the Apple iStore or Google Play store, were also investigated. The capabilities of the mobile applications that were assessed are listed in Table 2.
The five investigated mobile applications listed in Table 2 had features that were common. These features were the registration of a child, adding a vaccination record, and viewing a vaccination record. These features do represent the core functionality of a vaccination records management system. Similar datasets were noted amongst these mobile applications. It should be noted that none of them shared data with any government entity. The applications were meant to be used as stand-alone systems to assist parents and guardians with keeping track of their children's vaccines.
This led to the understanding that there were no freely available mechanisms for parents to store and retrieve official (verified) vaccination records that share data with government entities in South Africa. An investigation of South Africa's DoH's aims for eHealth was then conducted.
4. Department of Health's aims for eHealth
The 2019-2023 National Digital Health Strategy prioritises EHRs, digital processes, linkage of patient data across various systems, mHealth (mobile health), and knowledge in a digital form (DoH, 2020a). Some of these priorities relate to the previous National eHealth Strategy 2012-2016, which indicates that the measure of success of a country's eHealth maturity is made up of five stages (DoH, 2012). These stages are summarised in Table 3.
The DoH's eHealth maturity model is a framework that guides the development of electronic health records using the flows and sources of health information (DoH, 2020a). Overall, South Africa is at Stage 3 of eHealth maturity. Some provinces, however, are at Stage 4 in certain areas and other provinces are at Stages 1, 2, or 3. The DoH has outlined the following steps for South Africa to reach Stages 4 and 5 of eHealth maturity:
• patient-based health information systems need to be implemented at the point where health care is delivered;
• these systems need to be linked to a national health record system;
• all information should be captured into the electronic system at the point of patient care;
• every South African should have a unique identifier on the Health Information System;
• births and deaths need to be effectively registered; and
• all facilities must be able to access information from other facilities (DoH, 2012).
These steps essentially describe a system that stores the digital records centrally, and which can be accessed and updated from any healthcare facility. This would remove the need to recapture information from the individual healthcare facilities to the district, provincial, and national levels. Equipped with the aims of the DoH, together with generally used datasets and key functions of vaccination record systems, a prototype centrally based digital vaccination records management system called e-Vaccination was developed.
5. e-Vaccination prototype
e-Vaccination was created with four different profiles, one for each of the four key stakeholder types (doctors, nurses, parents, and school administrators). This allowed each stakeholder to engage with e-Vaccination from their particular perspective. With reference to the eHealth aims of the DoH, e-Vaccination was designed as a centralised system that allowed the stakeholders to access it via their internet-enabled devices. This centralised architecture is illustrated in Figure 2.
As illustrated in Figure 2, the key stakeholders could use their internet-enabled device (smartphone, tablet, laptop) to access e-Vaccination via their web browser. e-Vaccination was hosted on a remote server (the cloud) and was accessible via a URL (www.e-vaccination.co.za).
The features that were built into e-Vaccination took into consideration those features that were included in the investigated mobile applications. Since prototypes are normally built with limited purposes (Houde & Hill, 1997), only selected features were included in the design of e-Vaccination. The included features were viewing, requesting, and adding vaccination records. Vaccination statistics, in the form of reports at national, provincial, and district levels, were also included. The features linked to the different stakeholder views are described in Table 4.
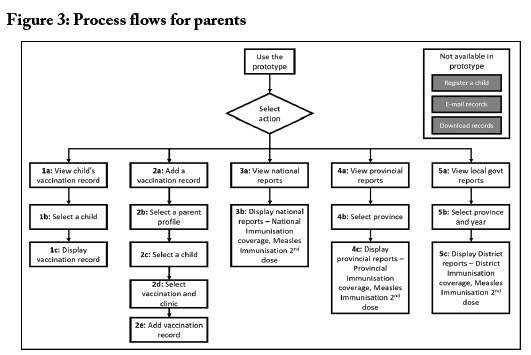
Figure 3 is an illustration of the process flows that were built into e-Vaccination for the parent stakeholder type. Once a parent logged into e-Vaccination, they could select from a list of five processes. To avoid complexity due to e-Vaccination being a prototype and not a live system, some of the processes that were identified early on in the design were not built. These are the "register a child", "e-mail records" and "download records" processes.
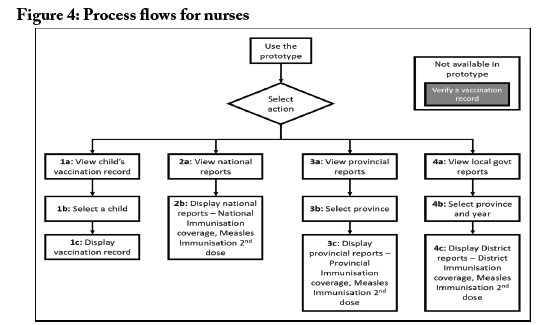
The overall process flows for the nurse stakeholder type are illustrated in Figure 4. Nurses could select from four main processes. These processes are to view a child's vaccination record and to view national, provincial, and local government (district level) vaccination reports. The "verify a vaccination record" process was not built into the prototype.
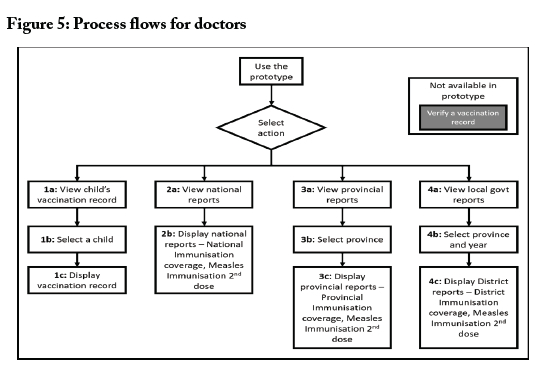
The process flows illustrated in Figure 5 are for the doctor stakeholder type. The process flows for doctors are the same as the process flows for nurses. The "verify a vaccination record" process was not built into the prototype.
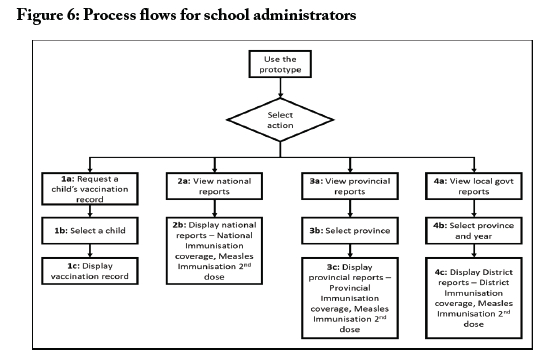
The process flows for the school administrator stakeholder type are illustrated in Figure 6. School administrators could select from four possible processes. Apart from viewing the national, provincial, and local government vaccination reports as the other stakeholder types could, school administrators could also request a child's vaccination record.
e-Vaccination was designed to be more graphical, allowing the user to type as little as possible with most of the options provided by large icons and dropdown lists. Figure 7 shows the actual user interface of e-Vaccination.
6. Assessment of e-Vaccination prototype
To assess the effectiveness of e-Vaccination, a questionnaire was designed to collect feedback from the relevant stakeholders. e-Vaccination was initially piloted by 10 users, who provided their feedback regarding the system. e-Vaccination was thereafter refined and prepared for distribution to the potential participants.
A quantitative research analysis was conducted on the data collected from the questionnaire, which was based on the stakeholder's engagement with e-Vaccination. A questionnaire with three sections was designed to collect demographic information (Section A), perceptions about vaccinations in Gauteng (Section B), and user perception (usefulness, satisfaction, ease of use and ease of learning, design and visual aids) information (Section C). (See Appendix 1 for the questionnaire.)
The participants who completed the questionnaire were anonymous. They were selected by word-of-mouth as well as via contact information that was available in the public domain. A link to e-Vaccination and the questionnaire was distributed to the prospective participants via e-mail, phone call, SMS, or visit. The prospective participants were asked to use e-Vaccination and to select the user profile based on their stakeholder type. Once they had used e-Vaccination, the participants answered the questionnaire and submitted their responses.
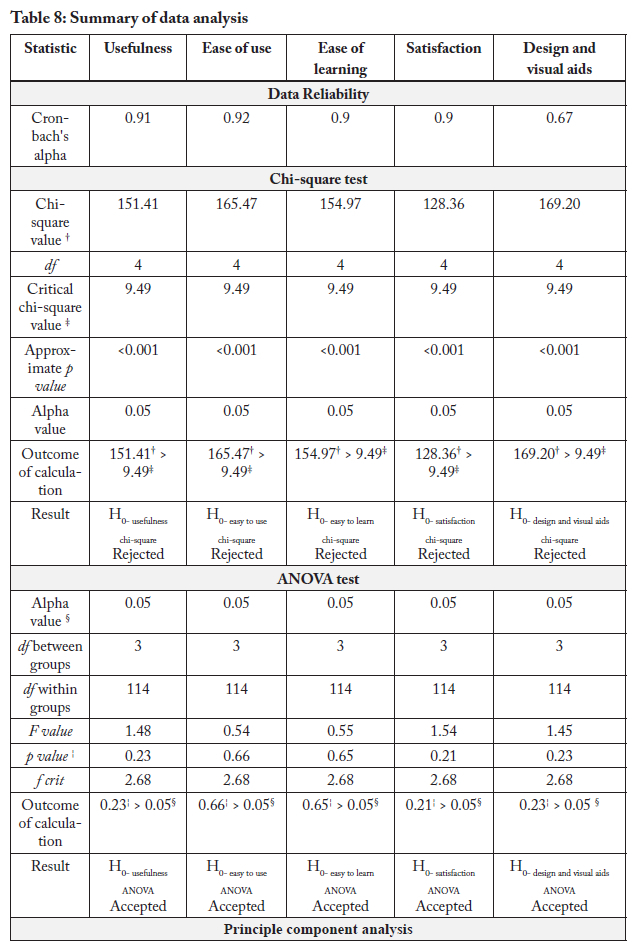
Following the data collection process, the data were statistically tested for reliability using a Cronbach's alpha test. The Cronbach's alpha scores were verified against the rating table by Gliem and Gliem (2003). To confirm that the data collected were not a randomised occurrence, a chi-square goodness of fit test followed as a subsequent step. The ANOVA test was used to determine if there were significant differences between different experimental conditions (Rutherford, 2000). This statistical method was used to analyse Likert-type scales in a similar study by Holtz and Krein (2011). Once it was proven that the data were reliable, not random and that stakeholder groups did not have a significant difference between them in their responses, a principle component analysis (PCA) test was conducted. A PCA is a data reduction method (UCLA IDRE, 2020) that can be used to investigate a relationship between dependent variables (Syms, 2019). The PCA was used to determine whether the responses to the questionnaire were related to the overall research question as well as to uncover any underlying factors that influenced the responses. The data analysis steps are summarised in Figure 8.
7. Results
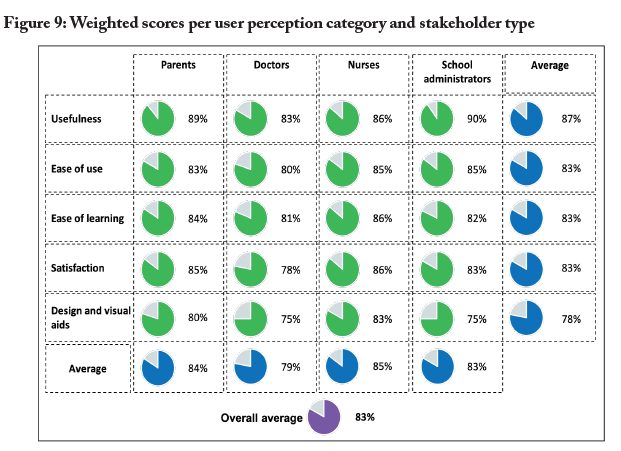
There were 118 respondents to the questionnaire (doctors: 16; nurses: 16; parents: 74; school administrators: 12). Of the 118 respondents, 95% had access to a smartphone and at least 96% had access to the internet and email. The paper-based vaccination card was the primary storage mechanism according to 91% of the respondents, while 5% felt that a digital system was the primary mechanism. Approximately 4% were uncertain. Most of the respondents, 94%, had at least one experience with a lost vaccination card. The results of the Cronbach's alpha test showed that the data collected were reliable. The chi-square test showed that the data collected were not a random occurrence and were due to an underlying factor. There was no significant difference in the data collected between the four stakeholder groups according to the results of the ANOVA test. The weighted scores for the questionnaire per user perception category and stakeholder type are depicted in Figure 9.
The weighted scores as illustrated in Figure 9 show that the overall perceptions about the digitisation of vaccination records scored an 83%. The usefulness of e-Vaccina-tion had the highest weighted score, 87%.
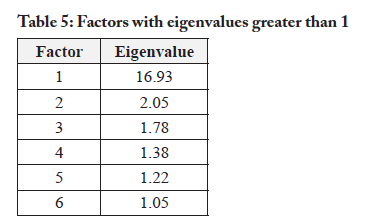
The PCA test was conducted on all 33 questions of section C of the questionnaire for all 118 participants (the full dataset). This test was used to determine the underlying factors relating to the five categories of the questionnaire as well as the perceptions of the stakeholders about the digital vaccination record. Eigenvalues were calculated and thereafter used to determine the main factors for each of the 33 questions. The factors with eigenvalues greater than 1 should be retained (UCLA IDRE, 2020). These factors are the significant factors that make up the principal components of the dataset. The factors with eigenvalues greater than 1 are displayed in Table 5.
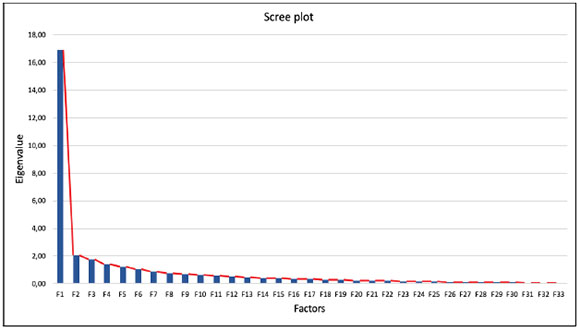
Factor 1, with an eigenvalue of 16.93, generated the steepest gradient on a scree plot (see Appendix 2). This main factor was identified as the one concerning the overall research question on the digitisation of the vaccination record. The remaining factors were renamed Factors 1 to 5. The contributions of the factors towards each of the user perception categories are detailed in Table 6 below.

For each user perception category, the factor that the category contributed most towards was determined. The factors were then labelled based on the underlying reason for why they contributed towards that category. The relationship between the factors and the categories, based on the highest contributions, is illustrated in Figure 10.
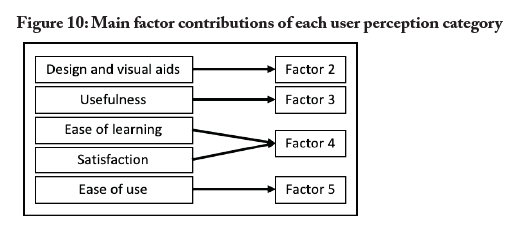
None of the user perception categories made its highest contribution to factor 1. The "ease of use" category which revealed the "user friendliness" factor during the PCA, however, made the highest contribution towards this factor. The contributions, labels, and descriptions are listed in Table 7.
The result of the statistical analysis demonstrated that e-Vaccination is user-friendly, practical, usable, provides a good user experience, and has a graphical design that aids in the use of the system. The results of each statistical test are summarised in Table 8.
The data analysis alone cannot tell us the full story as it is important to consider the current context. Whilst conducting this research, the COVID-19 pandemic reached South Africa, necessitating the implementation of the EVDS. Though the EVDS was not examined in detail, it can be noted that some of the features, such as creating and viewing vaccination records, are common in both systems.
8. Response to new challenges
The current COVID-19 pandemic has introduced a new paradigm, namely vaccination records for adults. Whilst the EVDS has been created primarily as a vaccination registration tool for COVID-19 vaccinations, it also serves a secondary purpose, which is to store the vaccination records of the patients (adults). It is not unreasonable to assume that we will possibly move to adult immunisation schedules on a seasonal basis. The vaccination card, SMS notifications and QR codes provided to the patients after their vaccination still represent one-way information flow from the healthcare facility to the patient. Whilst the EVDS seems to satisfy some of the eHealth aims mentioned earlier, such as the centralisation of data (which facilitates the sharing of data between healthcare facilities), the patient is not yet fully able to access his or her vaccination records through an available portal independently. It must be noted that the sharing of medical information, even with the patient, must take into account the Protection of Personal Information Act (POPIA) (RSA, 2013).
The COVID-19 pandemic has also raised another consideration. This is vaccination coverage, which can contribute towards herd immunity reporting. If the information is appropriately utilised, herd immunity reporting can be done at a national level. Further research needs to be conducted regarding the reporting of herd immunity for other vaccine-preventable diseases based on the EPI schedule and at a more granular level, such as district level or lower.
Though the EVDS does indeed represent a leap towards an EHR for South Africa, it has now contributed to a patchwork of systems created to address an immediate need. It contributes towards an EHR for every citizen, but we should be wary of it becoming the foundation for EHRs. Information Systems principles tell us that a solid foundation must first be laid. This includes getting the interconnectedness between the various systems done (whilst considering aspects such as POPIA) and then getting the related (medical) records appropriately positioned. In the past, other developing countries such as Tanzania have made massive investments in Health Information Systems, but issues relating to the adoption of integration resulted in resources being wasted (Smith et al., 2008). Considering that South Africa has a history of failed e-Government projects (Singh & Travica, 2018), the coupling of the current eHealth foundations and the EVDS needs to be analysed for current and future-readiness. In its haste, the DoH may have failed to adequately assess a key factor, which is the usability of the EVDS. The downstream applications of the EVDS as well as an assessment of whether it fully meets the DoH's eHealth aims are other areas that need further research.
9. Conclusions
The results of the study show that the key stakeholders supported the development of a digital system for the safe and secure storage of vaccination records for minors in Gauteng. The successful design of such a system is influenced by several factors. These factors (user friendliness, graphical design, practicality, user experience, and usability) were identified during this research and should drive the design and development of a digital vaccination records management system.
The DoH's response to the COVID-19 pandemic has accelerated the strides that South Africa is taking towards an EHR for all citizens. Vaccination records for minors (based on the EPI schedule), however, have still not made the same advances.
The reason could be that the move towards stages 4 and 5 of the eHealth model might require a more gradual approach as historic information needs to be considered.
Facets of prototypes such as e-Vaccination, working eHealth systems like the EVDS, and existing healthcare infrastructure should converge when considering the factors uncovered during this study as well as future research. If the usability of the system satisfies the key stakeholders, the chances of the system being used and the overall vision of the DoH being met will increase. To avoid wasteful expenditure, eHealth designers and policymakers should carefully consider the usability of applications that are being proposed for all key stakeholders.
References
Department of Health (DoH). (2012). eHealth Strategy South Africa. https://www.health-e.org.za/wp-content/uploads/2014/08/South-Africa-eHealth-Strategy-2012-2017.pdf
DoH. (2018). Road to Health Book. https://sidebyside.co.za/resources/road-to-health-book
DoH. (2020a). National Digital Health Strategy for South Africa 2019-2024. http://www.health.gov.za/wp-content/uploads/2020/11/national-digital-strategy-for-south-africa-2019-2024-b.pdf
DoH. (2020b). What is MomConnect? http://www.health.gov.za/index.php/mom-connect#momconnect
Gliem, J. A., & Gliem, R. R. (2003). Calculating, interpreting, and reporting Cronbach's alpha reliability coefficient for Likert-type scales. In 2003 Midwest Research to Practice Conference in Adult, Continuing, and Community Education (pp. 82-88). Columbus, OH. https://scholarworks.iupui.edu/bitstream/handle/1805/344/Gliem+&+Gliem.pdf?sequence=1
Global Alliance for Vaccines and Immunisations (GAVI). (2020). Could COVID-19 accelerate the digitisation of vaccine records? https://www.gavi.org/vaccineswork/could-covid-19-accelerate-digitisation-vaccine-records
Health Enabled. (2021). South Africa digital health dashboard. http://healthenabled.org/wordpress/south-africa-digital-health-dashboard
Holtz, B., & Krein, S. (2011). Understanding nurse perceptions of a newly implemented electronic medical record system. Journal of Technology in Human Services, 29(4), 247-262. https://doi.org/10.1080/15228835.2011.639931 [ Links ]
Houde, S., & Hill, C. (1997). What do prototypes prototype? In Martin G. Helander, Thomas K. Landauer & P.V. Prabhu (Eds.), Handbook of human-computer interaction (pp. 367-381). Elsevier. https://doi.org/10.1016/B978-044481862-1.50082-0
Lund, A. M. (2001). Measuring usability with the USE questionnaire. Usability Interface, 8(2), 3-6. [ Links ]
Moonsamy, W. (2021). An investigation into digital vaccination records for minors in Gauteng, South Africa. MSc dissertation, University of South Africa (UNISA). [ Links ]
Motara, F., Moeng, S., Mohamed, A., & Punwasi, J. (2021). Medical disaster related to CMJAH fire. Wits Journal of Clinical Medicine, 3(2), 139-140. https://doi.org/10.18772/26180197.2021.v3n2a8 [ Links ]
Nyatuka, D. R., & De la Harpe, R. (2021). Design considerations for patient- centered eHealth interventions in an underserved context: A case of health and wellbeing services within Nairobi's informal settlements in Kenya. The Electronic Journal of Information Systems in Developing Countries, 88(3). https://doi.org/10.1002/isd2.12164 [ Links ]
Republic of South Africa (RSA). (2013). Protection of Personal Information Act (POPIA) 4 of 2013. https://www.gov.za/sites/default/files/gcisdocument/201409/3706726-11act4of2013protectionofpersonalinforcorrect.pdf
Rutherford, A. (2000). Introducing ANOVA and ANCOVA: A GLM approach (Introducing statistical methods). SAGE. https://0-ebookcentral-proquest-com.oasis.unisa.ac.za/lib/unisa1-ebooks/reader.action?docID=254651
Singh, S., & Travica, B. (2018). E-Government systems in South Africa: An infoculture perspective. The Electronic Journal of Information Systems inDeveloping Countries, 84(4), e12030. https://doi.org/10.1002/isd2.120300 [ Links ]
Smith, M. L., Madon, S., Anifalaje, A., Lazarro-Malecela, M., & Michael, E. (2008). Integrated health information systems in Tanzania: Experience and challenges. The Electronic Journal of Information Systems in Developing Countries, 33(1),1-21. https://doi.org/10.1002/j.1681-4835.2008.tb00227.x [ Links ]
South African Government. (2021a). Electronic Vaccination Data System (EVDS) self registration portal. https://www.gov.za/covid-19/vaccine/evds
South African Government. (2021b, July 13). Health on the impact of violent protests on health services. https://www.gov.za/speeches/health-impact-violent-protests-health-services-13-jul-2021-0000
Syms, C. (2019). Principal components analysis. In B. Fath (Ed.), Encyclopedia of ecology (pp. 566-573). Elsevier.https://doi.org/10.1016/B978-0-12-409548-9.11152-2
UCLA Institute for Digital Research and Education (UCLA IDRE). (2020). Principal components analysis: SPSS annotated output. https://stats.idre.ucla.edu/spss/output/principal components/
World Health Organisation (WHO). (2019). Immunization. https://www.who.int/news-room/facts-in-pictures/detail/immunization
Acknowledgement
This article draws on elements of the first-listed author's MSc dissertation (Moonsamy, 2021).

Appendix 2: Scree plot of eigenvalues


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}