










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkHealth SA Gesondheid (Online)
versão On-line ISSN 2071-9736
versão impressa ISSN 1025-9848
Health SA Gesondheid (Online) vol.22 Cape Town 2017
http://dx.doi.org/10.1016/j.hsag.2017.05.001
FULL LENGTH ARTICLE
Evidence-based recommendations to facilitate professional collaboration between allopathic and traditional health practitioners
Rachel Magdalena (Dalena) van RooyenI; Blanche PretoriusII; Nomazwi Maudline TembaniI; Wilma ten Ham-BaloyiI, *
IFaculty of Health Sciences, Nelson Mandela Metropolitan University, Port Elizabeth, South Africa
IIResearch Capacity Development, Nelson Mandela Metropolitan University, Port Elizabeth, South Africa
ABSTRACT
BACKGROUND: Globally, and in South Africa, there is an increased demand for consulting both traditional and allopathic health practitioners. As both health practitioners are working within the same communities, their respective practices could complement or undermine the health of consumers using both health services. Professional collaboration between traditional and allopathic health practitioners is therefore desirable and requires collaboration between the systems, which is currently legislated by the Traditional Health Practitioners Act 22 of 2007. However, in the Eastern Cape, no evidence-based recommendations were found that facilitated the collaborative relationship between the two health practitioner groups.
Purpose of the research: To develop evidence-based recommendations aimed at facilitating professional collaboration between allopathic and traditional health practitioners for the benefit of patients.
METHODOLOGY: Descriptive evidence-based recommendations to enhance professional collaboration between both groups of health practitioners were developed based on focus group interviews with allopathic practitioners (n = 10) and individual interviews with traditional health practitioners (n = 18) (traditional health practitioners (n = 14) and traditional healers who are also allopathic health practitioners (n = 4)) practising in the Amathole District in the Eastern Cape, South Africa. Dickoff et al.'s (1968) Survey List was used as a conceptual framework.
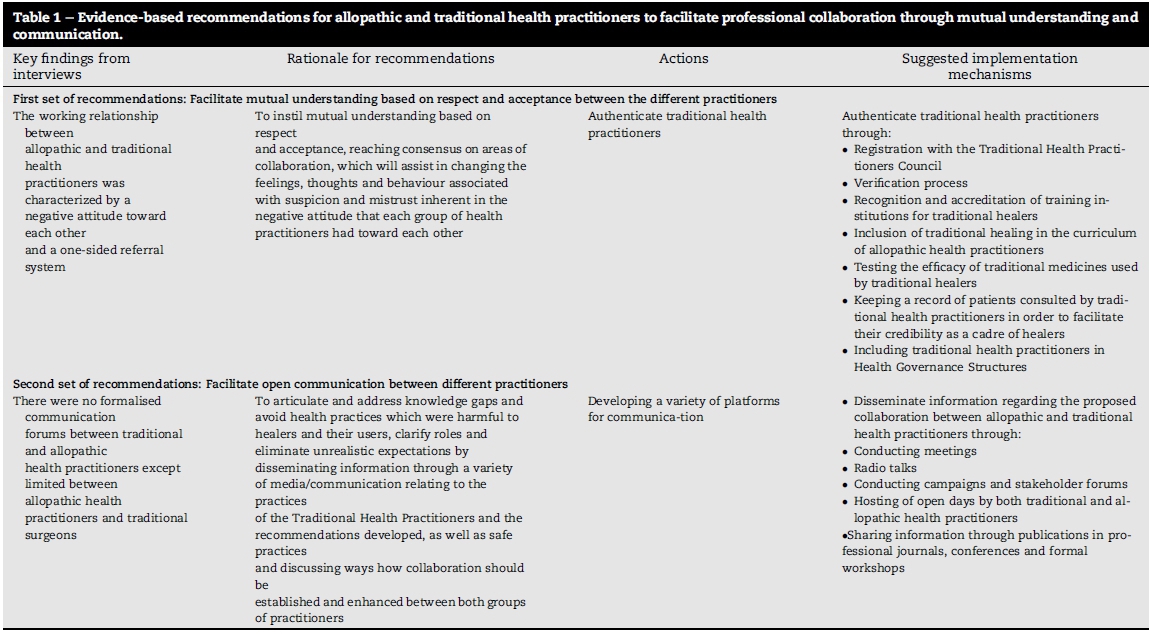
RESULTS: Collaboration was hampered by allopathic practitioners demonstrating negative attitudes by not referring patients to traditional practitioners based on lack of knowledge and mutual understanding of each other's practices. Suggestions for collaboration made by both groups resulted in the development of two distinct sets of evidence-based recommendations. The first set of recommendations aims to enhance professional collaboration between both groups of health practitioners. This is done through facilitating mutual understanding based on respect and acceptance between the different practitioners. The second set of recommendations aims to enhance professional collaboration through facilitating open communication between different practitioners.
CONCLUSION: These evidence-based recommendations can be used to facilitate professional collaboration between allopathic and traditional health practitioners resulting in mutual understanding and open communication, enhancing team work in a multi-professional environment, and ultimately leading to improved patient care.
Keywords: Allopathic health practitioners; Traditional health practitioners; Collaboration; Evidence-based recommendations; South Africa
1. Introduction
Every society has various categories of health practitioners in place to maintain and restore well-being (Figueras & McKee, 2012). These categories are influenced by differences in cultures and the health practitioners' understanding of health and disease. Globally, allopathic health practitioners are often approached by health care users. Allopathic healthcare includes healthcare delivered by physicians of all specialities, as well as recognised allied medical disciplines, for example, physiotherapists, and radiographers, and is generally characterised by the application of health science knowledge and technology to health and the healing process (World Health Organization (WHO), 2001).
However, alternative health practices or traditional healing, which can include homoeopathy, western herbal medicine, reflexology or any mind-body medicine, are often used in parallel to allopathic health practitioners (Frenkel, Ayre, Carlson, & Sierpina, 2008; Torri, 2012). In South Africa, traditional healing is practised by traditional practitioners. These practitioners include traditional doctors, surgeons (Ixhwele)or herbalists who are predominantly men specialised in the use of herbal medicines (Sorsdahl, Stein, & Flisher, 2013); diviners (Igqira) who are usually women who qualify after undergoing a process of acquiring the knowledge and skills of traditional healing (Steinglass, 2002); faith healers who use the power of suggestion, prayer and faith in God to promote healing (Cockerham, 2011); and the traditional birth attendant/traditional midwife, who are females, having gone through birth themselves, with no formal training and who attends to women during pregnancy, labour and the post-natal period by using herbs to facilitate delivery as well as providing psychological support (Austin, 2012; Owens-Ibie, 2011). Another name often used by Southern African tribes for a traditional healer is Sangoma.A Sangoma has multiple roles as physician, counsellor, psychiatrist, and priest and fulfils those roles by connecting with the ancestors (amadlozi), preparing herbal medicines (muti), interpreting dreams, diagnosing illness through forecast with bones, and knowing how to heal both physical and spiritual illness (McKay, 2015). This study focusses on the traditional practitioners cross the various categories as mentioned above.
Globally and in Africa, for the last couple of decennia both health systems have been used increasingly as persons move from one sector of a healthcare system to another or by using both systems simultaneously(Torri, 2012). However, currently there is little to no collaboration between the two types of practitioners. For example, referrals are few, and are mostly from the traditional healers to the modern health sector and seldom in the other direction (van Niekerk, Dladla, Gumbi, Monareng, & Thwala, 2014). Furthermore, the idea that traditional health practitioners must pass a litmus test in which they are scientifically scrutinised before they can be integrated into the national health services still exists. In spite of the prominent role that traditional medicine plays in healthcare it remains the least understood of all medical systems (van Niekerk, 2012).
Professional collaboration between health systems, where both systems can complement each other, is therefore desirable, and involves a process of working together in a climate where these two parties provide mutual assistance and help to attain a common goal (WHO, 2001). Professional collaboration is beneficial as it has shown to improve communication and increase mutual understanding between the two types of practitioners (Gqaleni et al., 2011). In addition, patient and disease information can be shared and better referrals can be achieved which leads to the improvement of health in the communities wherein both type of practitioners are practising (Gqaleni et al., 2011). Therefore, the WHO urged its member states, including South Africa, to prepare specific legislation to govern the practice of traditional medicine as part of the national health legislation (WHO, 2001). The promulgation of the Traditional Health Practitioners Act, Act 35 of 2004 (amended as Act 22 of 2007) (South Africa, 2008) by the South African government is the culmination thereof.
1.1. Problem statement
Although professional collaboration between both health groups of practitioners is meant to be legislated through the Traditional Health Practitioners Act 22 of 2007, in South Africa, including the Eastern Cape Province, there is no clear information as to how allopathic health practitioners have been collaborating with traditional health practitioners. In South Africa, collaboration between these two types of practitioners is specifically beneficial because of the potential for traditional health practitioners to serve as a critical component of a comprehensive health care strategy (Mbatha, Street, Ngcobo, & Nqaleni, 2012). For example, traditional health practitioners could play a significant role in the management and treatment of the most devastating and life-threatening diseases such as HIV and AIDS, tuberculosis, malaria, diabetes mellitus and cancer as they promote the use of natural plant-based remedies which have shown significant health benefits (Street & Prinsloo, 2013). Although promotion of the collaboration between the two groups of practitioners is done in the Traditional Health Practitioners Act (Act 22 of 2007), no formal evidence-based recommendations could be found to facilitate collaboration between allopathic and traditional health practitioners which could assist in optimising and complementing healthcare delivery in South Africa.
The following research question was therefore posed:
"How could professional collaboration between allopathic and traditional health practitioners be facilitated to optimise healthcare delivery in the Eastern Cape?"
1.2. Aim and objectives
The aim of this paper is to provide a detailed description of the evidence-based recommendations (hereafter referred to as 'recommendations') aimed at facilitating professional collaboration between allopathic and traditional health practitioners in a health district in the Eastern Cape, South Africa.
1.3. Definition of key concepts
1.3.1. Allopathic health practitioner
A practitioner is someone involved in a usually skilled job or activity. Allopathic health practitioners are those trained in scientific medicine whose positions are upheld by law and include doctors, nurses and recognised allied medical professionals like radiographers and physiotherapists (van Niekerk et al., 2014). In this study allopathic health practitioners are referred to practitioners such as registered nurses, medical practitioners and pharmacists that are working in South African healthcare settings.
1.3.2. Collaboration
The WHO (2001) defines collaboration as a process of working together in a climate where two parties provide mutual assistance and help to attain a common goal. In this study collaboration refers to the collaboration between allopathic health practittioners and traditional health practitioners.
1.3.3. Recommendations
Recommendations can be referred to as rules or instructions about the best course of action, specifically when put forward to an authority (Longman, 2009). In this study recommendations were developed to facilitate professional collaboration through mutual understanding and communication.
1.3.4. Traditional health practitioner
Traditional health practitioner refers to a person registered or required to be registered in terms of the Traditional Health Practitioners Act, Act No. 22 of 2007 as a traditional birth attendant, traditional surgeon, diviner and herbalist (South Africa, 2008). Faith healers are not mentioned in the Act as they use the power of suggestion, prayer and faith in God to promote healing (Cockerham, 2011). In this study the term "traditional healer" and "traditional health practitioner" will be used interchangeably each time referring to the practitioners in the traditional African medicine context.
2. Design and methods
The recommendations were based on the results of focus group discussions with allopathic health practitioners (n = 10) and individual interviews with traditional health practitioners (n = 14) and traditional healers who are also allopathic health practitioners (n = 4) practising in the Amathole District in the Eastern Cape, South Africa. The interviews revealed that both allopathic and traditional health practitioners experienced negative attitudes towards each other. Participants suggested that mutual understanding through changing attitudes towards each other and communication is crucial for effective collaboration between the two types of practitioners. For detailed findings please be referred to van Rooyen, Pretorius, Tembani, and ten Ham (2015).
The conceptual framework used for the development of the recommendations is Dickoff, James and Wiedenbach (1968)'s Survey List. This method will be explained in the following sections.
2.1. Procedures
The process of the development of the recommendations will be described.
A survey list by Dickoff et al. (1968) was used as the conceptual framework to develop the recommendations. The survey list has six ways of looking at an activity (in this study facilitating collaboration between the two types of practitioners by means of the recommendations) in the hope of revealing different features as point of view shifts (Dickoff et al., 1968). These six aspects are:
(i) Agency or agent: Who or what performs the activity?
(ii) Patiency or recipiency: Who or what is the recipient of the activity?
(iii) Framework: In what context is the activity performed?
(iv) Terminus: What is the end point of the activity?
(v) Procedure: What is the guiding procedure, technique, or protocol of the activity?
(vi) Dynamics: What is the energy source for the activity?
The aspects are explained in the context of the study.
2.1.1. Agency or agent
The agent is the individual who executes or facilitates the goal-directed activity. In this case the general manager who is in charge of district health services in the Eastern Cape Department of Health as agent of change will facilitate the process of operationalising the recommendations to promote collaboration between allopathic and traditional health practitioners. This manager will present the strategies to his/her colleagues in the provincial office of the Eastern Cape Department of Health and to senior managers responsible for health programmes that utilise traditional health practitioners. The agent will also create awareness about the recommendations among traditional health practitioners themselves.
2.1.2. Patiency or recipiency
Under a theoretical notion of a recipient of an activity are included all those persons who receive action from agents or who are receptive to activity that has a specified terminus (Dickoff et al., 1968). The recipients of the recommendations in this study are two groups of health practitioners namely, the traditional health practitioners and allopathic health practitioners. Recipients should have analytical minds as they will in turn be agents of change to their patients, colleagues, communities and community-based organisations. It is expected that some recipients will reject the recommendations. The agent must therefore be vigilant and sensitive when implementing the proposed collaboration recommendations.
2.1.3. Framework
The framework provides a context or setting in which the activity is performed. The setting where the study was conducted was the Amathole District that is made up of five Local Service Areas or health sub-districts, namely, Amahlathi, Nkonkobe, Buffalo City, Mbashe and Mnquma. The major towns in these Local Service Areas are Keiskammahoek, Alice, East London, Idutywa and Butterworth respectively. The District comprises of 39% of the population living in urban areas and 61% of the population living in rural areas. The study was conducted within the context of a healthcare delivery system that emphasises the primary healthcare approach, serving a population of approximately 1.7 million. Health services in the Amathole District Municipality are provided by allopathic health practitioners in one hospital complex (East London Hospital Complex), eleven district hospitals, seven community health centres and two-hundred- and-eight fixed clinics.
The numbers for traditional health practitioners practicing in this municipality are unknown as the registration process is not completed yet, but these type of practitioners are also serving the local population.
2.1.4. Terminus
In the present study, the terminus or endpoint of the activity is the effective collaboration between allopathic and traditional health practitioners. This is the aim of the recommendations.
2.1.5. Procedure
The function of a procedure as outlined by Dickoff et al. (1968) is to provide sufficient detail to enable an activity to be carried out, to serve as a safeguard to agent or recipient and organisation. Where there is danger to the recipient, agent or institution, very determinant procedures may be desirable and where peripheral knowledge of a likely agent is somewhat limited, again explicit, rote-like procedures are advisable in order to safeguard performance of the procedure. Although there is no potential danger in implementing the proposed strategies, the procedure for implementation of the proposed recommendations to facilitate collaboration between traditional and allopathic health practitioners will have to be explicit and according to legislative and ethical principles as knowledge about traditional healing in general is limited.
2.1.6. Dynamics
In explaining the concept of dynamics, Dickoff et al. (1968) assert that the aspect of dynamics of an activity emphasises the power sources for that activity. Power sources can be physical, chemical, biological or psychological. In this study the implementing agent, which is the General Manager who is in charge of district health services in the Eastern Cape Department of Health, has both physical and psychological power sources. This agent need to be energetic, enthusiastic and motivated to have traditional health services established and optimally functional. The agent has the advantage of enjoying a sound working relationship with the National General Secretary of the Traditional Healers Association.
2.1.7. Developing the recommendations
After the framework was developed, the recommendations were developed based on combining the themes from the interviews with both allopathic health practitioners and traditional health practitioners. The purpose of combining the themes of both types of interviews were for data completeness (Adami, 2005). For example, for the recommendations with the aim of facilitating collaboration and enhancing their implementation, the recommendations needed to be based on both type of practitioner's perspective in order to create an in-depth understanding of the phenomena of collaboration and issues facilitating or hindering this collaboration. A discussion of the themes and the developed recommendations is outlined below (see section 3 Results and discussion).
2.2. Ethical considerations
The ethical acceptability of the study was ensured throughout the research process. Ethical clearance was obtained from the relevant university (ethics number H2004-HEA-NUR-001), as well as the Eastern Cape Department of Health. Furthermore, for the qualitative data, the following ethical principles were considered: anonymity by identification of participants by numbers; confidentiality by not stating the participant's name in any of the records used in this study; and freedom from exploitation and deception by not withholding information or offering incorrect information to the participants about the study.
2.3. Trustworthiness
Guba's model (as described by Krefting, 1991), which mentions four criteria of trustworthiness, namely, credibility, applicability, consistency and confirmability, was used. Some of these criteria were used by the researcher in this study to increase trustworthiness. Credibility and applicability of the recommendations was ensured through triangulation by conducting interviews with different categories of traditional health practitioners and different categories of allopathic health practitioners and combining the themes from these interviews for the recommendations. Credibility was further ensured by selecting an appropriate conceptual framework to base the recommendations on (Creswell, 2009).
3. Results and discussion
The themes from the interviews with allopathic health practitioners and traditional health practitioners that were used for the recommendations will be outlined in Table 1 (for full details of the findings of the interviews please refer to van Rooyen et al., 2015).
The two different sets of recommendations that were informed by the findings are discussed as follows:
3.1. First set of recommendations:facilitate mutual understanding based on respect and acceptance between the different practitioners
From the findings, allopathic health practitioners had a negative attitude towards traditional health practitioners, which could explain the one-sided referral system that the traditional health practitioners expressed concerns about. This one-sided referral system was also confirmed by van Niekerk et al. (2014), who found that the majority of traditional health practitioners would refer to allopathic health practitioners, but only a few of the allopathic health practitioners would refer to traditional health practitioners. Contributing factors could be the lack of understanding and knowledge about each other's practices (van Niekerk et al., 2014).
Based on the findings, this first set of recommendations aims to facilitate an attitude of mutual understanding based on respect and acceptance. To facilitate this attitude, the recommendations can be implemented by validating traditional health practitioners' practices. This set of recommendations, guided by the suggestions participants offered to include traditional health practitioners in governing health structures, are in line with previous recommendations suggested internationally by the WHO. The WHO recommends to review each country's national regulation of traditional medicine; reinforcing; or establishing structures to regulate traditional medicine practice; supporting scientific research of traditional medicines; and accelerating the integration of traditional medicine into national health system (WHO, 2005b). For South Africa, the integration of traditional medicine into the national health system and authentication of traditional practitioners was, for example, also outlined in previous studies. These studies support the role traditional health practitioners can play to enhance primary health care as for instance HIV/AIDS counsellors due to their prominence and trustworthiness in the community(Mbatha, 2012; Richter, 2003).
Registration and verification were mentioned by the participants as one of the means to validate traditional health practitioners' practices. Registration with the Traditional Health Practitioners Council was also mentioned by Solomon, Graves and Catherwood (2015) as a means to provide safeguards and credibility for both groups of health professionals, as well as patients. This registration should have clear and unambiguous criteria and continuous development should be encouraged. Furthermore, this would require support from national, provincial and local structures in terms of creating platforms for educational development, as well as provision for administration and possible costs that registration may cause. Currently, as proposed in the Traditional Health Practitioners Act all traditional healers need to register with the Traditional Health Practitioners Council and pay a R200 fee for a certificate before being able to practise (South Africa, 2008). The criteria that need to be met for traditional health practitioners to register include: being a South African citizen; providing character references from people unrelated to the applicant; and proof of qualifications (South Africa, 2008). Besides that credibility could be enhanced, the implementation of this process may impose some challenges. For example, the criteria should have sufficient detail to be implemented and applied equality to each applicant. Providing qualifications could also pose a challenge as it is not clear which qualifications are required per category of health practitioner and whether traditional health practitioners will have to submit their original qualifications. The stipulated criteria should also be communicated in detail to the traditional health practitioners by the Council in order to smoothen the process of registration and avoid confusion. On the other hand, the criteria must be realistic. Furthermore, logistically, there should be several ways in which paying of (annual) registration fees can be paid to avoid travelling in order to pay.
Recognition and accreditation of training institutions for traditional health practitioners were also suggested. Accreditation ensures that quality education is provided (WHO, 2005a). However, in order for education institutions to be accredited, certain standards and criteria for accreditation of such institutions need to be developed and implemented nationally. Furthermore, for an educational institution to be accredited, the training and teaching of traditional practices provided at those institutions should conform to minimum standards proposed by the WHO and other organisations (Walwyn & Maitshotlo, 2010; WHO, 2005b).
Training of traditional health practitioners should be given according to the category of traditional health practitioner and based on the specific requirement per category. Clarity is required regarding the practicalities of the how, when and where of the training should be given. However, currently, the Traditional Practitioners Act (South Africa, 2008) does not specify this.
Moreover, in order for traditional healing to be included in the curriculum of allopathic health practitioners, as recommended by some of the participants, the training should be evidence-based. Testing the efficacy of traditional medicines used by traditional healers could enhance the evidence base relating to traditional medicine. Testing of traditional medicines was also mentioned as one of the means to enhance credibility of the traditional health practitioner. According to Kirksey (2007), studies have been undertaken to test the effectiveness of herbal medication. However, sample sizes were small and little research has been done regarding the effectiveness of herbal medication. Therefore, a need for more research to investigate the effectiveness of herbal medicines, preferably rigorous randomized controlled trials using large samples, is needed. Other forms of traditional healing such as prayer, connecting with the spirit world, and rituals also require more research by means of rigorous qualitative studies to understand these phenomena and how they could contribute to the allopathic health system. Keeping a record of patients consulted by traditional health practitioners in order to facilitate their credibility as a cadre of healers was also mentioned by the practitioners. Walwyn and Maitshotlo (2010) in their study regarding the role of South African traditional health practitioners' practices and use of herbal medicine in the treatment of HIV/AIDS also recommended record keeping as a means of quality control. They also recommended that traditional healers label the herbs they used. Record keeping of people using traditional health services should also be included in the training of traditional health practitioners.
The WHO developed guidelines for training traditional health practitioners in Primary Health Care. The guidelines give broad instructions and can be used by individuals and organisations in South Africa to develop training programmes that will enable traditional health practitioners to play a more significant role in primary health care programmes (WHO, 1995). The guidelines include steps for planning the training, determining the content, methods and materials for the training, training the trainers and evaluating the training (WHO, 1995). However, no publication could be found on a training programme or training of traditional health practitioners in the Eastern Cape, which may indicate that little to no training of traditional health practitioners is currently done in this province.
Furthermore, inclusion of traditional health practitioners as critical stakeholders in governance structures of the Eastern Cape Department of Health, such as the District Health Planning Advisory Council, Hospital Boards and Clinic Committees will expose them to the processes of planning and monitoring health services. This exposure will make them more informed and build their capacity and understanding of health issues including legal control of health service provision. Although there will be only a few traditional health practitioners participating in these structures, theywill be able to share the knowledge and experiences with other traditional health practitioners in their local structures or associations as there is a Provincial Association of Traditional Healers and similar structures at district and sub-district levels. On the other hand such involvement of traditional health practitioners in governance structures may assist in changing the attitude of allopathic health practitioners as they will be compelled to recognise traditional health practitioners as colleagues and critical stakeholders who have to participate in the planning and monitoring of health services. An attempt was made in 2010 in KwaZulu-Natal, where a Traditional Health Practitioner Policy Forum was held on the theme "Integrating Traditional Healers and formal HIV/AIDS prevention, treatment and care". This forum brought together healers, researchers, government, civil society organisations, allopathic health practitioners and others to share ideas and debate policy issues that are crucial to ensure that patients of both groups of practitioners receive the best possible care in the context of the HIV/AIDS epidemic (Traditional Health Practitioner's Policy Forum, 2010). One of the recommendations from this forum was to ensure the inclusion of traditional health practitioners in stakeholder forums at local and district level. Similar initiatives could assist in including traditional health practitioners as critical stakeholders in governance structures.
Currently in South Africa traditional medicine is regulated through the Traditional Practitioners Act (South Africa, 2008). However, implementation of this Act is problematic as establishing a Traditional Health Practitioners' Council as indicated by the Act has yet to be done, causing delays in the authenticating process of traditional health practice as registration and training at recognised institutions is thus not possible. Further, more clarity is needed regarding how authentication in terms of registration, accreditation and training should be done.
Both groups of participants indicated a need for collaboration and a need for information and communication. This resulted in second set of recommendations regarding communication.
3.2. Second set of recommendations: facilitate open communication between different practitioners
Effective communication is established by eliminating communication barriers, thereby ensuring the free flow of information (Fielding, 2006). Furthermore, information should be disseminated that will facilitate a process of instilling mutual understanding and collaboration between allopathic and traditional health practitioners. Communication will enlighten both groups of practitioners about each other's practices and responsibilities and rights according to the Traditional Health Practitioners Act, with particular reference to its purpose and provisions, and will furthermore facilitate a working relationship between both practitioners. Effective communication therefore demands that people work together to ensure that the meaning of a particular concept such as infection, is created and shared (Fielding, 2006). However, communication between traditional practitioners and allopathic practitioners seems to be poor (Gqaleni et al., 2011; WHO, 2005b). Furthermore, there seem to be no strategies in place addressing communication between traditional and allopathic health practitioners. The participants in this study therefore recommended strongly that platforms to enhance communication opportunities between both groups of practitioners should be developed. Such platforms aim to disseminate information about the practices of traditional health practitioners. Meetings and stakeholder forums could be used to disseminate this information, as well as to discuss how collaboration between allopathic and traditional health could be established and enhanced. Other means of communication mentioned included: radio talks, conducting campaigns and a stakeholder forum, hosting of Open Days by both traditional and allopathic health practitioners and sharing information through publications in professional journals, conferences and workshops. Gqaleni et al.'s study regarding medical and traditional healing collaboration on HIV and AIDS in KwaZulu-Natal, South Africa successfully used workshops to discuss traditional methods of HIV prevention. The discussions from the workshops resulted in the development of culturally relevant messages to enhance the prevention of HIV and AIDS which were used to create public awareness and rebuild the image of traditional healing (Gqaleni et al., 2011). Further, in the same province, a forum was established that brought stakeholders (including both groups of health practitioners) together to share ideas and debate policy issues that are crucial to ensure that patients of both groups of practitioners receive the best possible care in terms of HIV/AIDS (Traditional Health Practitioner's Policy Forum, 2010). Recommendations for policy change were made in terms of strengthening the essential role of traditional health practitioners in holistic HIV/AIDS prevention, treatment, care and support. This was enhanced by, amongst other things, setting up a regular dialogue mechanism between allopathic and traditional health practitioners at all levels (Traditional Health Practitioner's Policy Forum, 2010). However, up to date no similar initiatives could be found for the Eastern Cape Province. Efforts to facilitate open communication between both groups of practitioners could therefore be used not only to enhance collaboration between groups, but also to enhance safe practices to treat disease and improve awareness regarding the prevention of disease in communities at large. This is crucial since a significant proportion of these communities consult traditional healers, in combination with seeking regular medical treatment (WHO, 2005a, 2005b).
Although the WHO urged member states, of which South Africa is one, to prepare specific legislation to govern the practice of traditional medicine as part of the national health legislation (WHO, 2001), of which the Traditional Health Practitioners Act is a culmination of, no formal model or strategy could be found that facilitates the collaboration between allopathic and traditional health practitioners. The proposed collaboration recommendations in this study can be implemented by applying various existing change theories and logic models. The agency or agent could play an important role in applying the correct models in order to implement the recommendations and facilitate collaboration.
3.3. Implications of the study
Implementation of both sets of recommendations did not form part of this study. However, before the implementation, the proposed sets of recommendations should undergo an expert panel review. The recommendations can be used to facilitate professional collaboration between allopathic and traditional health practitioners by facilitating mutual understanding, based on respect and acceptance. In addition, the recommendations can be used to facilitate open communication between allopathic and traditional health practitioners that will enhance team work in a multi-professional environment which will ultimately lead to improved patient care.
3.4. Limitations
Both sets of recommendations were informed by only a few allopathic health practitioners as two focus group discussions with a total of 10 allopathic health practitioners could be conducted due to the reality of staff shortages in the clinical situation. The sets of recommendations were based on interviews conducted with allopathic health practitioners and traditional health practitioners from the Amathole District Municipality only. More interviews with both groups of practitioners could have been held throughout South Africa. This could have informed the recommendations more comprehensively.
3.5. Recommendations for future research
The two sets of proposed recommendations focused on mutual understanding and communication. These sets of recommendations require further refinement through an expert panel review, as well as pilot testing their efficacy as an approach to facilitate collaboration between allopathic and traditional health practitioners.
4. Conclusions
This article showed that the support for the development of traditional medicine and the facilitation of collaboration between traditional health practitioners and allopathic health practitioners are promoted globally. A growingdemand exists to use both groups of health practitioners to strengthen health care delivery.
Further, the development of the two sets of recommendations to facilitate collaboration between traditional health practitioners and allopathic health practitioners was outlined as these two groups of health practitioners were not working collaboratively in an optimal manner. The two sets of recommendations can be further developed by reviewing them by an expert panel. When implemented, the two sets of recommendations may assist in facilitating collaboration between the two groups of practitioners. However, for successful implementation, the collaborative process outlined in the recommendations through mutual understanding and open communication, will require buy-in from both groups of health practitioners and may take a considerable amount of time as the Traditional Health Practitioners Act (2008) has not been implemented up to today.
Authors' contributions
NMT conducted the study, collected data, carried out the analyses. WTHB wrote the paper. RMVR and BP supervised the study, contributed to the manuscript and approved the final version.
Acknowledgements
The authors are grateful to all the traditional and allopathic health practitioners who participated in this study.
REFERENCES
Adami, M. F. (2005). The use of triangulation for completeness purposes. Nurse Researcher, 12(4), 19-29. [ Links ]
Austin, J. (2012). Choosing a birth care provider, traditional birth attendants. http://www.birthtakesavillage.com/registered-midwives-traditional-birth-attendants/. [ Links ]
Cockerham, W. C. (2011). Medical sociology. New Jersey: Prentice Hall. [ Links ]
Creswell, J. W. (2009). Research design. Qualitative, quantitative and mixed methods. London: Sage Publications. [ Links ]
Dickoff, J., James, P., & Wiedenbach, E. (1968). Theory in a practice discipline. Part 1 practice oriented theory. Nursing Research, 17(5), 415-435. [ Links ]
Fielding, M. (2006). Effective communication in organizations (3rd ed.). Cape Town: Juta. [ Links ]
Figueras, J., & McKee, M. (2012). Health systems, health, wealth and societal well-being. Berkshire: Open University Press. [ Links ]
Frenkel, M., Ayre, E. B., Carlson, C., & Sierpina, V. (2008). Integrating complementary and alternative medicine into conventional primary care: the patient perspective. Explore, 4, 178-186. [ Links ]
Gqaleni, N., Hlongwane, T., Khondo, C., Mbatha, M., Mhlongo, S., Ngcobo, M., et al. (2011). Biomedical and traditional healing collaboration on HIV and AIDS in KwaZulu-Natal, South Africa. Universitas Forum, 2,2. [ Links ]
Kirksey, K. (2007). M.D. or herbal Remedy.?? The effectiveness of traditional medicine in Africa. http://healthpsych.psy.vanderbilt.edu/Web2007/traditionalMedicine.htm. [ Links ]
Krefting, L. (1991). Rigor in qualitative research. The assessment of trustworthiness. The American Journal of Occupational Nurses, 45(3), 214-219. [ Links ]
Longman Dictionary of Contemporary English. (2009). Recommendation. London: Pearson/Longman. [ Links ]
Mbatha, B. (2012). The contribution of traditional healers to halting the spread of HIV and AIDS in South Africa: The case of soshanguve township in the city of Tshwane. Indilinga African Journal of Indigenous Knowledge Systems, 11(1), 61-72. [ Links ]
Mbatha, N., Street, R. A., Ngcobo, M., & Nqaleni, N. (2012). Sick certificates issued by the South African traditional health practitioners: Current legislation, challenges and the way forward. South African Medical Journal, 102, 129-131. [ Links ]
McKay, G. (2015). Sangoma. http://www.ancestralwisdom.com/sangoma.html. [ Links ]
van Niekerk, M. (2012). Traditional healers formalised? South African Medical Journal, 102,3. [ Links ]
van Niekerk, M., Dladla, A., Gumbi, N., Monareng, L., & Thwala, W. (2014). Perceptions of the traditional health practitioner's role in the management of mental health care users and occupation: A pilot study. South African Journal of Occupational Therapy, 44(1), 20-24. [ Links ]
Owens-Ibie, N. (2011). Traditional birth attendants and the pursuit of maternal and child health in Nigeria. http://www.sas.upenn.edu/ppe/Events/uniconf_2011/documents/Owens.Ibie.Noma.FinalPaper.pdf. [ Links ]
Richter, M. (2003). Traditional medicines and traditional healers in South Africa. Johannesburg: Wits University. [ Links ]
van Rooyen, R. M., Pretorius, B., Tembani, N. M., & ten Ham, W. (2015). Allopathic and traditional health practitioners' collaboration. Curationis, 38,2. [ Links ]
Solomon, D., Graves, N., & Catherwood, J. (2015). Allied health growth: What we do not measure we cannot manage. Human Resources for Health, 13(32), 1-6. [ Links ]
Sorsdahl, K., Stein, D. J., & Flisher, A. J. (2013). Predicting referral practices of traditional healers of their patients with a mental illness: An application of the theory of planned behaviour. African Journal of Psychiatry, 16,35-40. [ Links ]
South Africa. (2008). Traditional Health Practitioners Act 22 of2007 as amended. Government gazette (511), no 30660. Cape Town: Government Printers. [ Links ]
Steinglass, M. (2002). 'It takes a village healer - anthropologists believe traditional medicines can remedy Africa's AIDS crisis. Are they right?". Lingua Franca, 32. [ Links ]
Street, R. A., & Prinsloo, G. A. (2013). Commercially important medicinal plants of South Africa: A review. Journal of Chemistry, 2013,1-16. [ Links ]
Torri, M. C. (2012). Intercultural health practices: Towards an equal recognition between indigenous medicine and biomedicine? A case study from Chile. Health Care Annals, 20, 31-49. [ Links ]
Traditional Health Practitioner's Policy Forum. (2010). Culture and health policy forum paper no. 1. https://www.aids.org.za/wp-content/uploads/2015/05/Traditional-Health-Practitioners-Policy-Forum-Report-Final.pdf. [ Links ]
Walwyn, D., & Maitshotlo, B. (2010). The role of South African traditional health practitioners in the treatment of HIV/AIDS: A study of their practices and use of herbal medicines. The Southern African Journal of HIV Medicine,11-17. [ Links ]
World Health Organization. (1995). Traditional practitioners as primary health care workers. http://apps.who.int/medicinedocs/pdf/h2940e/h2940e.pdf. [ Links ]
World Health Organization. (2001). African forum on the role of traditional medicine in health systems. Final Report. Harare: World Health Organization. [ Links ]
World Health Organization. (2005a). Accreditation ofmedical education institutions. Geneva: World Health Organization [ Links ]
World Health Organization. (2005b). National policy on traditional medicine and regulation of herbal medicines - Report of a WHO global survey. Geneva: World Health Organization. [ Links ]
Received 1 September 2015
Accepted 2 May 2017
Peer review under responsibility of Johannesburg University.
* Corresponding author. Fax: +27 (0) 41 504 1626.
E-mail addresses: dalena.vanrooyen@nmmu.ac.za (R.M. (Dalena) van Rooyen), blanche.pretorius@nmmu.ac.za (B. Pretorius), wilma.tenham-baloyi@nmmu.ac.za (W. ten Ham-Baloyi).


{kind=link}