










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.22 Cape Town 2017
http://dx.doi.org/10.1016/j.hsag.2017.01.005
FULL LENGTH ARTICLE
A review of the transportability of cognitive therapy for the treatment of PTSD among South African rape survivors
Anita Padmanabhanunni*
Private Bag X17, Department of Psychology, University of the Western Cape, Cape Town, South Africa
ABSTRACT
This study aimed to evaluate the transportability of cognitive therapy (CT) for rape survivors with PTSD to South African conditions. Ten local treatment outcome studies investigating the transportability of CT were identified and appraised. The common elements of CT for PTSD including psychoeducation, exposure therapy and cognitive restructuring of trauma-related appraisals were found to be transportable to local contexts. Contextual factors that can complicate treatment delivery were also identified namely exposure to multiple traumatic events, HIV, absence of safety and support in the external environment and language barriers. The augmentations made to an existing evidence-based treatment protocol to address these contextual factors are described.
Keywords: Cognitive treatment; PTSD; Rape survivors; South Africa; Transportability
1. Introduction
Rape represents a serious societal crisis and major public health concern in South Africa. Compared to other traumatic events, rape is associated with the highest frequency of post-traumatic stress disorder (PTSD) among survivors (Atwoli et al., 2013; Breslau, 2009; Ullman, Townsend, Filipas, & Starzynski, 2007). PTSD represents a debilitating psychiatric condition characterised by intrusive re-experiencing of the traumatic event, cognitive and behavioural attempts to avoid reminders, negative alterations in cognition and mood and symptoms of alterations in arousal and reactivity (American Psychiatric Association, 2013). Depression, suicidal ideation, self-harming behaviours and alcohol abuse often co-occur with PTSD (Ullman et al., 2007).
Several South African studies have confirmed the prevalence of PTSD following exposure to rape. For instance, Atwoli et al. (2013), in a nationally representative survey of South African adults, found that rape was the traumatic event with one of the highest risks for PTSD. A comparative study of different types of traumatic events (Seedat Nyamai, Njenga, Vythilingum & Stein 2004) concluded that sexual assault, when compared to all other traumas, was associated with the greatest risk of PTSD. Studies conducted in community settings (Dinan, McCall, & Gibson, 2004) and university contexts (Padmanabhanunni & Edwards, 2015) have further corroborated these findings.
In treating PTSD following rape, the majority of interventions with evidence of efficacy are cognitive-behavioural treatments (Edwards, 2013; Foa, Keane, Friedman, & Cohen, 2008; Vickerman & Margolin, 2009; Wilson, Friedman, & Lindy, 2012). Some of the existing protocols (e.g. Stress Inoculation Training) have been adapted for the treatment of rape survivors while others such as prolonged exposure therapy (PET) and cognitive processing therapy (CPT) were specifically developed for this population group. Other cognitive therapy (CT) treatments that have been used with rape survivors and found to be effective include Ehlers and Clark (2000) Cognitive Therapy (ECCT) and eye movement desensitisation and reprocessing (EMDR) (Foa et al., 2008; Ford & Courtois, 2009; Vickerman & Margolin, 2009). These treatments typically have a number of common components (Schnyder et al., 2015) namely psychoeducation about PTSD and the impact of traumatic events, exposure therapy aimed at facilitating processing of the trauma memory and cognitive restructuring of problematic cognitive appraisals associated with the trauma and its sequelae.
Each of these protocols have been assessed in randomised controlled trials (RCT's), that is, efficacy studies designed to demonstrate whether a treatment produces the desired clinical outcome (e.g. reduction and resolution of PTSD symptoms) under ideal clinical settings (e.g. those characterised by the presence of trained clinicians and with client populations that do not present with co-morbid diagnoses). A detailed discussion of each of these clinical trials is beyond the scope of this paper (see Foa et al., 2008; Vickerman & Margolin, 2009 for a more complete description of these studies).
Despite the availability of efficacious CT protocols for PTSD, there is evidence that these interventions are underutilised in clinical practice both internationally and locally and this has been attributed to concerns regarding transportability (Borntrager, Chorpita, Higa-McMillan, & Weisz, 2015; Edwards, 2013; Higson-Smith, Thacker, & Sikhakane, 2005). According to Schoenwald and Hoagwood (2001), transportability refers to the extent to which treatments developed in Western clinical trials are applicable in other settings. Current findings (e.g. Borntrager et al., 2015) suggest that many clinicians are sceptical about the foundations of evidence-based interventions predominantly because treatment conditions in clinical trials do not reflect the complexities encountered in real-world settings. For this reason, various researchers (Chorpita & Regan, 2009; Schoenwald & Hoagwood, 2001) have emphasized that evidence of transportability is a precursor to adoption. This means that for efficacious treatments to ultimately be adopted by clinicians there needs to be evidence that these interventions are applicable in standard clinical contexts.
South African society is characterised by high levels of poverty, unemployment, crime and under-resourced public sector services. In addition, clients seen in local settings tend to differ in terms of race, culture, socio-economic status and historical background and often have to contend with complex life circumstances (Young, 2009). Clinicians in South Africa also differ in terms of their cultural background, level of expertise and their general approach to therapy. Furthermore, owing to historical factors, the majority of clinicians in the country are White and this can have implications when working with clients from different racial and socio-economic backgrounds (Eagle, 2005). It is probable that these contextual factors may impact on the transportability of interventions.
This study aims to evaluate the transportability of CT in the treatment of rape-related PTSD to local contexts by appraising the evidence from local treatment outcome studies.
2. Methodology
The present study used systematic review methodology. Systematic reviews are a form of secondary research that involves a comprehensive survey of a topic in which all of the primary studies are systematically identified, appraised and then summarised according to an explicit and reproducible methodology. Systematic reviews have become a well-established means of informing policies and decisions regarding the delivery of health care services (Petticrew & Roberts, 2008).
2.1. Article selection
The treatment outcome studies that were reviewed form part of a larger project spearheaded by Professor David Edwards and aimed at investigating the transportability of ECCT in local contexts. This project generated a series of systematic case studies on the treatment of PTSD among survivors of various types of traumatic events. The clinicians in each of these case studies were Master's and Doctoral students in Psychology. The present study exclusively reviewed those cases focusing on the treatment of rape survivors. Although the intervention used in each case was ECCT, these studies provide an opportunity to examine the transportability of the core components of CT in the treatment of rape survivors to local contexts.
The inclusion criteria were case studies focusing solely on the treatment of rape survivors with PTSD. Participants in the primary studies had to be adolescent or adult female rape survivors who were formally diagnosed with PTSD and treated using CT. Case studies were excluded if they focused on traumatic events other than rape. There were two independent reviewers for the study namely, a primary reviewer (the principal researcher) and a second reviewer. The second reviewer independently screened the studies identified by the primary reviewer.
3. Results
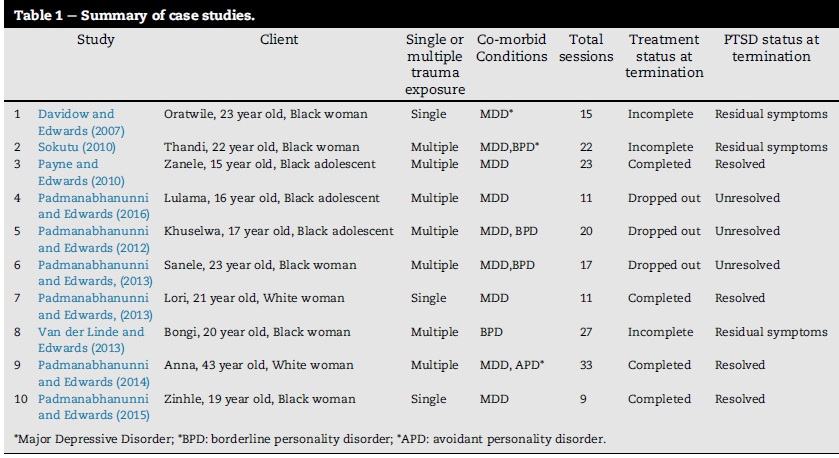
Ten systematic case studies were identified. Eight were published in peer-reviewed journals while two were unpublished dissertations. These studies are summarised in Table 1. Pseudonyms were used in these studies to protect the identities of participants.
An analysis of these studies revealed that in three cases (Padmanabhanunni & Edwards, 2012, 2013, 2016) the client dropped out of treatment by failing to attend a scheduled session and subsequently not returning for therapy. Dropout occurred during the treatment phase. In three of the studies (Davidow & Edwards, 2007; Sokutu, 2010; Van der Linde & Edwards, 2013) treatment was incomplete at the time of termination due to either the clinician's internship coming to an end or the client relocating. This was an anticipated outcome and factored into the treatment plan. As such, at the time treatment concluded the client experienced only residual symptoms of PTSD or there was a significant reduction in the overall symptom picture (Sokutu, 2010; Van der Linde & Edwards, 2013). In four studies Padmanabhanunni & Edwards, 2013, 2014, 2015; Payne & Edwards, 2010 ) treatment was complete at the time of termination and the client no longer met criteria for PTSD. Thus of the ten studies, treatment was unsuccessful in three cases and effective in seven cases. However, even in cases where treatment was successful, it was not straightforward and contextual factors were encountered that led to treatment augmentations. In the subsequent section, the extent to which the active components of CT are transportable to the South African context is evaluated. Thereafter, contextual factors that impact on treatment delivery are discussed and augmentations made to the treatment model to address these aspects are described.
3.1. Are the core components of CT transportable to South African contexts?
This section evaluates the extent to which the core components of CT can be applied in local settings. These components include psychoeducation, exposure therapy and cognitive restructuring of dysfunctional trauma-related appraisals.
3.1.1. Psychoeducation
The provision of psychoeducation is a common feature of CT treatments for trauma. It is typically provided at the outset of treatment and involves imparting information aboutcommon reactions to traumatic events, the nature and prevalence of PTSD and orienting the client to the CT treatment approach. Foa et al. (2008) state that psychoeducation is beneficial in providing survivors with a roadmap to understand the nature of their difficulties and that this can serve to reduce distress. Psychoeducation has also been found to be beneficial in cross-cultural studies but as a stand-alone intervention it is insufficient in addressing PTSD (Neuner, Schauer, Klaschik, Karunakara, & Elbert, 2004).
In each of the case studies, psychoeducation was shown to have favourable effects (see Davidow & Edwards, 2007; Payne & Edwards, 2010). Even in cases where the client eventually dropped out of treatment, psychoeducation was effective in normalizing symptoms, addressing certain types of problematic appraisals and in promoting re-engagement with avoided activities and situations. It was also beneficial in eliciting a detailed account of the traumatic event from clients who were ambivalent about disclosing. This can be seen in the treatment of Lulama (Padmanabhanunni & Edwards, 2016), an adolescent survivor of two incidents of sexual assault, one of which was a gang rape. In this case, psychoeducation on the cognitive mechanisms underlying PTSD addressed her appraisals that her flashbacks were a sign that she "was going crazy" and that her life would never be the same again. This intervention led to some improvement in her mood and prompted her to provide a detailed verbal account of the trauma. Similarly, in the treatment of Khuselwa (Padmanabhanunni & Edwards, 2012), an adolescent survivor of multiple episodes of childhood sexual abuse (CSA), psy-choeducation on CSA addressed self-blame and led to her providing a written account of her experiences of abuse. In sum, the evidence from the case series suggests that in the treatment of rape survivors in local contexts, psycho-education can produce important shifts in negative appraisals of the trauma and thereby improve mood and increase motivation to engage with active treatment components.
3.1.2. Exposure based interventions
Exposure based interventions are a universal component of CT for PTSD and involve repeated confrontation with memories of the traumatic event in imagination and with avoided situations, objects or activities in vivo (Foa et al., 2008). A core feature of ECCT is imaginal reliving of distressing parts of the traumatic event. The patient is guided to vividly imagine and recount the traumatic event along with associated emotions and appraisals (Ehlers & Clark, 2000). Exposure has been hypothesized to facilitate the integration of the traumatic event into memory and modify dysfunctional cognitive appraisals that underlie PTSD. Despite the demonstrated efficacy, the use of exposure based interventions has been regarded as one of the primary factors underlying the high dropout rate in clinical trials (Wilson et al., 2012). In addition, there are questions regarding the cross-cultural applicability of exposure therapy. It has been suggested that these techniques are more likely to produce negative results for clients from other cultural groups including worsening of symptoms and increased dropout (Hinton, Hofmann, Rivera, Otto, & Pollack, 2011). For example, Lester, Resick, Young-Xu and Artz (2010) in an exposure-based treatment study reported higher dropout rates among African-American compared to White patients.
In each of the case studies that formed part of this review, exposure based interventions were used. This involved guiding the client to provide a narrative (e.g. Davidow & Edwards, 2007; Sokutu, 2010; Padmanabhanunni & Edwards, 2016) of the traumatic event while remaining emotionally connected to the memory. In addition, imaginal exposure to the worst parts of the traumatic event was used to address problematic peri-traumatic appraisals (e.g. Davidow & Edwards, 2007; Padmanabhanunni & Edwards,, 2013, 2014). Significantly, none of the clients in these case studies dropped out of treatment following the use of an exposure based intervention, suggesting cross-cultural applicability. Increased tolerance of exposure-based interventions in these cases may be attributed to the ECCT model's emphasis on shortened reliving sessions that focus specifically on the distressing components of the trauma associated with negative appraisals. In contrast to other treatment protocols such as PET and CPT, the exposure to anxiety provoking material is limited and therefore possibly more tolerable for the client.
3.1.3. Cognitive restructuring of negative trauma-related cognitive appraisals
In terms of the prevailing cognitive models of PTSD, negative cognitive appraisals of the traumatic event and its sequelae are seen as playing a central role in the persistence of PTSD and are therefore a significant focus of treatment. These appraisals involve negative beliefs about the self (e.g. "I have been tainted"), the world (e.g. "nowhere is safe"), other people (e.g. "I can't trust others") and PTSD symptoms (e.g. "I'm going crazy"). Ehlers and Clark (2000) argue that these types of problematic appraisals contribute to the sense of current threat experienced by survivors and serve to maintain symptoms.
Various researchers (Eagle, 2005; Engelbrecht & Jobson, 2014) have argued that cultural belief systems can act as perceptual filters and influence the nature of the appraisals associated with traumatic events. As such, it is important to consider the extent to which existing interventions are effective in targeting culturally influenced appraisals (Engelbrecht & Jobson, 2014). In South Africa, Eagle (2005) has documented the influence of traditional African belief systems on trauma-related appraisals and how, in certain instances, these beliefs can complicate treatment. In the case studies reviewed, the majority of clients (8) were Black women and there were differences in their socio-economic and cultural backgrounds. Their trauma-related appraisals corresponded to those described by universal models of the cognitive impact of trauma and standard cognitive restructuring techniques were used to target these beliefs. For example, a common appraisal among these clients involved self-blame and the cognitive restructuring technique of using a pie chart to guide the client to re-apportion responsibility was effective in reducing blame (see Davidow & Edwards, 2007; Van der Linde & Edwards, 2013). Other common appraisals included the assumption that "nowhere is safe" and other people cannot be trusted. These generalizations were also successfully targeted using cognitive restructuring techniques (see Sokutu, 2010; Padmanabhanunni & Edwards, 2016)
3.2. Implementation considerations
The evidence from this review suggests that the common elements of CT for rape-related PTSD are transportable to local contexts. Nevertheless, in most of the case studies, modifications to treatment were made owing to contextual factors. This included the presence of multiple traumatic events, issues regarding HIV, absence of safety and support in the external environment and issues related to race and language. These contextual factors are considered below and the augmentations made to treatment are discussed.
3.2.1. Multiple traumatic events
Five of the studies reviewed involved cases where the client had been exposed to multiple traumatic events including severe childhood neglect and repeated instances of sexual abuse, beginning in childhood (Sokutu, 2010; Van der Linde & Edwards, 2013; Padmanabhanunni & Edwards, 2012, 2013, 2014). In South Africa exposure to multiple traumatic events is common (Atwoli et al., 2013; Seedat, Van Niekerk, Jewkes, Suffla, & Ratele, 2009) and it is likely that clinicians working in this context will encounter these types of cases. Repeated exposure to trauma is associated with a more complex symptom picture. In four of the case studies, the client displayed symptoms characteristic of complex PTSD and was diagnosed with co-morbid borderline personality disorder (BPD) Padmanabhanunni & Edwards, 2012, 2013; Sokutu, 2010; Van der Linde & Edwards, 2013). In one case, the client was diagnosed with avoidant personality disorder (APD) (Padmanabhanunni & Edwards, 2014).
Existing CT treatment protocols like ECCT are designed to treat single isolated incidents of trauma. Survivors of prolonged and repeated trauma respond less well to standard treatments for PTSD. These clients typically experience a range of problems including difficulties with affect regulation, impulsivity and suicidal behaviour and difficulties with interpersonal relatedness. In addition, they may also experience issues related to personal safety and have a limited capacity for self-care. In such cases, exposing these clients too directly to their trauma history can lead to re-traumatisation. In the case studies, a phased approach was used in treating clients with more complex symptom presentations. The initial phase of treatment focused on stabilisation, which involved enhancing the client's capacity to regulate strong emotions, self-nurture and establish healthy relationship boundaries (see Sokutu, 2010). There was also a focus on developing particular skills including rational problem solving, safety planning and strategies to manage trauma symptoms (see Padmanabhanunni & Edwards, 2013). In certain cases (e.g. Sokutu, 2010; Padmanabhanunni & Edwards, 2014), Schema Therapy (ST) (Young, Klosko, & Weishaar, 2003) was used to guide treatment planning and to achieve goals related to stabilisation. Only once the client had acquired the capacity to tolerate strong emotions, developed a sense of trust in the therapist and was not in crises would treatment progress to the next phase involving exposure-based interventions. This type of phased approach was beneficial in promoting recovery in three cases (Padmanabhanunni & Edwards, 2014; Sokutu, 2010; Van der Linde & Edwards, 2013 ). Issues related to personal safety hampered stabilisation efforts in two cases and led to dropout (Padmanabhanunni & Edwards, 2012, 2013).
3.2.2. Safety and support in the external environment
One of the prerequisites for treating psychological trauma is the presence of safety and support in the clients' external environment. In South Africa, owing to low conviction rates in rape cases (Vetten, 2011), survivors have to content with the possibility of encountering the perpetrator in their community, which places them at increased risk of further harm and aggravates distress. This was illustrated in Padmanabhanunni & Edwards (2016), Padmanabhanunni & Edwards (2012, 2013), Payne and Edwards (2010). In these instances, it is recommended that clinicians work with relevant stakeholders in promoting the safety of the client (Edwards, 2013). In the Payne and Edwards (2010) case study, for example, the clinician was in frequent contact with the investigating officer and this was of some benefit in the case being attended to. In Padmanabhanunni and Edwards (2016), the clinician liaised with the Department of Social Development to promote the safety of the client. In certain instances, individual outpatient treatment may not be ideal owing to the real risk of revictimisation. This was highlighted in two studies (Padmanabhanunni & Edwards, 2012, 2013) where dropout from treatment was linked to limited safety in the external environment. In such cases, it is recommended that the client be placed in a women's shelter or inpatient facility while undergoing treatment.
Enhancing social support is a feature of most CT treatment protocols for trauma. In South Africa social support for survivors, particularly those who live in disadvantaged communities are often minimal and this can complicate treatment. Often the client's family does not have an understanding of the impact of trauma and this may hinder their ability to help the survivor to cope. This was evident in the case of Zinhle (Padmanabhanunni & Edwards, 2015), an adult survivor of CSA. Her family, believing that speaking about the trauma would only exacerbate her distress, enforced silence on the topic. This led to her feeling alienated and enhanced her self-blame. In this case, psycho-education was useful in facilitating Zinhle's re-connection with her family.
In other situations, social support may be compromised due to neglectful circumstances including parental substance abuse (e.g. Padmanabhanunni & Edwards, 2016; 2012). In the case of Lulama, liaising with relevant stakeholders led to a social worker being assigned to address the absence of safety in her home environment owing to her mother's substance abuse. Although she eventually dropped out of treatment, these interventions led to her feeling safer and more supported. Her depression had resolved at the time she stopped treatment and there were significant reductions in her PTSD symptoms. It was hypothesized that these improvements underlay her decision not to return to therapy.
3.2.3. HIV
South Africa is characterised by a high incidence of HIV/AIDS and this can increase the probability of a survivor being infected with the virus. HIV status can have implications for PTSD treatment. This was illustrated in Payne and Edwards (2010) study where the client discovered during the course of treatment that the rape had led to her being infected with HIV. Therapy work on the trauma was then halted and the focus shifted to exploring the implications of the diagnosis on the client's life and processing her sense of grief and loss regarding her future. In Davidow and Edwards (2007) study, the client's uncertainty about her HIV status was an important focus of treatment. This uncertainty exacerbated existing feelings of helplessness and shame and her sense of having been permanently affected by the rape. An important focus area for treatment in this case involved encouraging the client to undergo HIV testing and exploring with the client the implications of being HIV positive.
3.2.4. Race and language
A discussion of contextual factors is not complete without consideration of the role of race and language in treatment delivery. In South Africa, race was used as an ideological device to justify an apartheid system of governance aimed at securing White privilege (Leach, Akhurst, & Basson, 2003). For this reason when conducting psychotherapy, an important part of cross-cultural sensitivity is an awareness of the history of the country and its possible effects on the therapeutic relationship. The clients in the case series under review were diverse and in almost all cases (9) there were racial as well as language differences between client and clinician. In addition, in many instances it was the client's first experience of psychotherapy. For example, in Payne and Edwards (2010) study, the client was a Black adolescent who was not fluent in English and had never previously interacted with a White person. Nevertheless, in these studies, these differences did not have a salient impact on treatment delivery or on the client's ability to engage with the therapy process. Language differences did pose a barrier in the use of imaginal reliving in one of the cases (Padmanabhanunni & Edwards, 2013) as the client was minimally fluent in English. One of the aims of reliving is to identify problematic appraisals and language differences can complicate this. In such cases, Padmanabhanunni & Edwards (2013) has suggested that the use of an interpreter needs to be carefully considered in treatment planning. In sum, the evidence from the case series suggests that CT is cross-culturally applicable and that it is possible for clients and clinicians from diverse cultural and socio-economic backgrounds to work together in achieving treatment goals.
4. Discussion and conclusion
This study aimed to investigate the transportability of CT for rape-related PTSD to the South African context. The review provides evidence to suggest that the basic components of CT are transportable to local settings. Contextual factors that can complicate treatment engagement were identified and the augmentations made to an existing evidence-based treatment were described. The study also highlighted that in certain instances individual outpatient treatment may not be appropriate particularly where the client's capacity for self-protection is low and there is a risk of revictimisation.
Author contribution
Anita Padmanabhanunni conceptualised the project, carried out the research and wrote the manuscript.
Funding
The author acknowledges the financial support of the University of the Western Cape and the National Research Foundation (NRF) of South Africa.
Potential reviewers
Prof. Kelvin Mwaba. Email: kmwaba@uwc.ac.za, Department of Psychology, University of the Western Cape, Private Bag X17, Bellville, Cape Town.
Dr. Shazly Savahl. Email: ssavahl@uwc.ac.za, Department of Psychology, University of the Western Cape, Private Bag X17, Bellville, Cape Town.
Dr. Mario Smith. Email:mrsmith@uwc.ac.za, Department of Psychology, University of the Western Cape, Private Bag X17, Bellville, Cape Town.
Acknowledgements
The author acknowledges the support of the National Research Foundation (NRF) of South Africa in supporting her research.
REFERENCES
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington: American Psychiatric Association. [ Links ]
Atwoli, L., Stein, D. J., Williams, D. R., Mclaughlin, K. A., Petukhova, M., Kessler, R. C., et al. (2013). Trauma and posttraumatic stress disorder in South Africa: Analysis from the South African stress and health study. BMC Psychiatry, 13(1), 182. [ Links ]
Borntrager, C. F., Chorpita, B. F., Higa-McMillan, C., & Weisz, J. R. (2015). Provider attitudes toward evidence-based practices: Are the concerns with the evidence or with the manuals? Psychiatric Services, 60(5), 1-5. [ Links ]
Breslau, N. (2009). The epidemiology of trauma, PTSD, and other post-trauma disorders. Trauma, Violence, and Abuse, 10(3), 198-210. [ Links ]
Chorpita, B. F., & Regan, J. (2009). Dissemination of effective mental health treatment procedures: Maximizing the return on a significant investment. Behaviour Research and Therapy, 47(11), 990-993. [ Links ]
Davidow, A., & Edwards, D. J. A. (2007). Treatment of PTSD and depression in a black South African rape survivor. In Paper presented at the world congress ofbehavioural and cognitive therapies: Barcelona, Spain (July). [ Links ]
Dinan, B. A., McCall, G. J., & Gibson, D. (2004). Community violence and PTSD in selected South African townships. Journal of Interpersonal Violence, 19(6), 727-742. [ Links ]
Eagle, G. T. (2005). Therapy at the cultural interface: Implications of African cosmology for traumatic stress intervention. Journal of Contemporary Psychotherapy, 35(2), 199-209. [ Links ]
Edwards, D. (2013). Responsive integrative treatment ofclients with PTSD and trauma-related disorders: An expanded evidence- based model. Journal of Psychology in Africa, 23(1), 7-20. [ Links ]
Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319-345. [ Links ]
Engelbrecht, A., & Jobson, L. (2014). An investigation of trauma- associated appraisals and posttraumatic stress disorder in British and Asian trauma survivors: The development of the public and communal self appraisals measure (PCSAM). SpringerPlus, 3(1), 1. [ Links ]
Foa, E. B., Keane, T. M., Friedman, M. J., & Cohen, J. A. (2008). Effective treatments for PTSD: Practice guidelines from the international society for traumatic stress studies. New York, NY: Guilford Press. [ Links ]
Ford, J. D., & Courtois, C. A. (2009). Defining and understanding complex trauma and complex traumatic stress disorders. In C. A. Courtois, & J. D. Ford (Eds.), Treating complex traumatic stress disorders: An evidence-based guide (pp. 13-31). New York, NY: Guilford Press. [ Links ]
Higson-Smith, C., Thacker, M., & Sikhakane, N. (2005). Needs assessment for integrated traumatic stress services: Mpumalanga Province, South Africa, 10 March 2014, from viewed: http://www.craighigsonsmith.com/file.php/1/Publications/Mpumalanga_final.pdf. [ Links ]
Hinton, D. E., Hofmann, S. G., Rivera, E., Otto, M. W., & Pollack, M. H. (2011). Culturally adapted CBT (CA-CBT) for Latino women with treatment-resistant PTSD: A pilot study comparing CA-CBT to applied muscle relaxation. Behaviour Research and Therapy, 49(4), 275-280. [ Links ]
Leach, M. M., Akhurst, J., & Basson, C. (2003). Counseling psychology in South Africa: Current political and professional challenges and future promise. The Counseling Psychologist, 31(5), 619-640. [ Links ]
Lester, K., Artz, C., Resick, P. A., & Young-Xu, Y. (2010). Impact of race on early treatment termination and outcomes in posttraumatic stress disorder treatment. Journal of Consulting and Clinical Psychology, 78(4), 480. [ Links ]
Neuner, F., Schauer, M., Klaschik, C., Karunakara, U., & Elbert, T. (2004). A comparison of narrative exposure therapy, supportive counseling, and psychoeducation for treating posttraumatic stress disorder in an African refugee settlement. Journal of Consulting and Clinical Psychology, 72(4), 579. [ Links ]
Payne, C., & Edwards, D. (2010). What services and supports are needed to enable trauma survivors to rebuild their lives? Implications of a systematic case study of cognitive therapy with a township adolescent girl with PTSD following rape'. Child Abuse Research in South Africa, 10(1), 27-40. [ Links ]
Petticrew, M., & Roberts, H. (2008). Systematic reviews in the social sciences: A practical guide. Victoria, Australia: Blackwell Publishing. [ Links ]
Schnyder, U., Ehlers, A., Elbert, T., Foa, E. B., Gersons, B. P., Resick, P. A., et al. (2015). Psychotherapies for PTSD: What do they have in common? European Journal of Psychotraumatology, 6(10), 281-286. [ Links ]
Schoenwald, S. K., & Hoagwood, K. (2001). Effectiveness, transportability, and dissemination of interventions: What matters when? Psychiatric Services, 52(9), 1190-1197. [ Links ]
Seedat, S., Nyamai, C., Njenga, F., Vythilingum, B., & Stein, D. J. (2004). Trauma exposure and post-traumatic stress symptoms in urban African schools survey in CapeTown and Nairobi. The British Journal of Psychiatry, 184(2), 169-175. [ Links ]
Seedat, M., Van Niekerk, A., Jewkes, R., Suffla, S., & Ratele, K. (2009). Violence and injuries in South Africa: Prioritising an agenda for prevention. The Lancet, 374(9694), 1011-1022. [ Links ]
Sokutu, N. (2010). Longstanding trauma, disrupted interpersonal relations: An evaluation of the Ehlers and Clark model for PTSD in a complex case. MA thesis. Psychology Dept, Rhodes University. [ Links ]
Ullman, S. E., Townsend, S. M., Filipas, H. H., & Starzynski, L. L. (2007). Structural models of the relations of assault severity, social support, avoidance coping, self-blame, and PTSD among sexual assault survivors. Psychology of Women Quarterly, 31(1), 23-37. [ Links ]
Van der Linde, F., & Edwards, D. (2013). "It's like Uprooting Trees": Responsive treatment for a case of complex post-traumatic stress disorder following multiple rapes. Journal of Psychology in Africa, 23(1), 21-29. [ Links ]
Vetten, L. (2011). Paradox and policy: Addressing rape in post- apartheid South Africa. International Approaches to Rape, 169-192. [ Links ]
Vickerman, K. A., & Margolin, G. (2009). Rape treatment outcome research: Empirical findings and state of the literature. Clinical Psychology Review, 29(5), 431-448. [ Links ]
Wilson, J. P., Friedman, M. J., & Lindy, J. D. (2012). Treating psychological trauma and PTSD. New York, NY: Guilford Press. [ Links ]
Padmanabhanunni, A., & Edwards, D. (2016). Derailed by a sugar daddy: An investigation of the failed treatment of an adolescent township rape survivor with PTSD. Child Abuse Research in South Africa, 17(2), 83-94. [ Links ]
Padmanabhanunni, A., & Edwards, D. (2012). Treating complex post-traumatic stress disorder following childhood neglect, sexual abuse and revictimisation: Interpretative reflections on the case of Khuselwa. Journal of Child Abuse Research in South Africa, 13(1), 40-54. [ Links ]
Padmanabhanunni, A., & Edwards, D. (2013). Victimisation in the lives of lesbian-identified women in South Africa: Implications for clinical assessment and treatment. Journal of Psychology in Africa, 23(3), 385-392. [ Links ]
Padmanabhanunni, A., & Edwards, D. (2014). A phenomenological case study of the therapeutic impact of imagery: Rescripting of memories of a rape and episodes of childhood abuse and neglect. The Indo-pacific Journal of Phenomenology, 14(1), 1-16. [ Links ]
Padmanabhanunni, A., & Edwards, D. (2015). A Case study of social cognitive treatment of PTSD in a South African rape survivor: The central role of case formulation. Journal of Child Sexual Abuse, 24(2), 174-194. [ Links ]
Young, C. (2009). The transportability and utility of cognitive therapy in South African contexts: A review. Journal of Psychology in Africa, 19(3), 407-422. [ Links ]
Young, J. E., Klosko, J. S., & Weishaar, M. E. (2003). Schema therapy: A practitioner's guide. Guilford Press. [ Links ]
Received 1 September 2015
Accepted 16 January 2017
Peer review under responsibility of Johannesburg University.
* E-mail address: apadmana@uwc.ac.za.


{kind=link}