










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkHealth SA Gesondheid (Online)
versão On-line ISSN 2071-9736
versão impressa ISSN 1025-9848
Health SA Gesondheid (Online) vol.22 Cape Town 2017
http://dx.doi.org/10.1016/j.hsag.2017.03.001
FULL LENGTH ARTICLE
Lived experience of patients on tuberculosis treatment in Tshwane, Gauteng province
Oluwafunmilayo Olabisi Akeju I, *; Susanna C.D. WrightII; Todd M. MajaII
IAdelaide Tambo School of Nursing, Tshwane University of Technology, P O Box 26965, Gezina, 0031, Pretoria, South Africa
IIAdelaide Tambo School of Nursing, Tshwane University of Technology, South Africa
ABSTRACT
Tuberculosis is one of the communicable diseases that still contributes substantially to the worldwide disease burden and is still a major health threat worldwide. In order to gain a better understanding of being a patient taking tuberculosis treatment and to improve adherence to treatment, this phenomenological study was conducted to explore the lived experience of patients on tuberculosis treatment.
The population comprised patients in an identified tuberculosis clinic in Tshwane who had been on treatment for at least four months and who were able to communicate in English. The data gathering instrument was self-report by in-depth interview.
Some of the main themes that emerged include influence of personal social situation, influence of good social support and disclosure, experience of taking medication daily and knowledge about tuberculosis treatment.
Findings revealed that the personal social situations of the participants which include accommodation, unemployment and nutritional requirements influenced the adherence of the participants to treatment. It was discovered that good social support had an influence on adherence which could only be enjoyed when the treatment and diagnosis of tuberculosis is disclosed to the family members and friends. Some of the participants, who had been non-adherent in the past, attributed the reasons for their non-adherence to the side effects that they experienced. Lastly, participants also reported knowledge about tuberculosis, that is, knowledge about its causes, treatment and prevention, as crucial for adherence to treatment.
Keywords: Adherence Lived experience Non-adherence Treatment
1. Introduction and background
Despite the fact that tuberculosis is a curable disease, it is still a major cause of illness and death in South Africa and globally.
Tuberculosis is a complex disease that has biological, social, economic and cultural effects on the patient. These factors affects treatment adherence, which in turn affect treatment outcome. As with other long-term treatment, non-adherence to treatment is a problem in tuberculosis management treatment. Tuberculosis treatment presents particular challenges for adherence because treatment is long and involves taking a number of medications, side-effects are common, and patients usually feel better before treatment has been completed.
In the 2015 Global Tuberculosis Report, the World Health Organisation revealed South Africa as the second African country with a high tuberculosis incidence, behind neighbouring Lesotho with a smaller population (WHO, 2015,p. 159). South Africa was also reported as a country with a high incidence and prevalence rates with an estimated incidence of 450,000 cases of active tuberculosis in 2013 (WHO, 2015,p. 141).
Some of the factors that support the continued spread of tuberculosis include overcrowding, poor ventilation, unemployment, poverty and cultural beliefs (Selala, 2011, pp. 26-32).
The consequences of non-adherence to tuberculosis treatment includes prolong illness and disability for patient, infectiousness of patient causing tuberculosis transmission in the community, development of drug resistant tuberculosis and the possibility of death (Department of Health, 2014,p. 51).
According to The National Tuberculosis Management Guideline (Department of Health, 2014, p. 51) the aim of treatment is to successfully treat all patients who are started on treatment. However, little is known about the lived experience of being a tuberculosis patient taking treatment for long periods of time and few studies have been conducted in South Africa using the phenomenological route (Naidoo, Dick, & Cooper, 2009; Selala, 2011; Sissolak, Marais, & Mehtar, 2010).
1.1. Problem statement and objectives
The study was motivated by the problem of non-adherence to tuberculosis treatment, which has contributed to an increase in the number of drug resistant strains. Studies have shown that people diagnosed with tuberculosis and who are on treatment tend to discontinue their medication once they start feeling better, especially if they are not on directly observed treatment (Amuha, Kutyabami, Kittu, Odoi-Adome, & Kalyango, 2009, p. 10; Volmink, Matchaba, & Garner, 2000, p. 335).
The purpose of the study was to explore and describe the lived experiences of patients on tuberculosis treatment.
The objective of the study was to generate evidence which can be used to improve patients' adherence to tuberculosis treatment, in order to help to enhance tuberculosis cure and control.
The research question therefore was: What is the lived experience of patients who have been on tuberculosis treatment for at least four months?
1.2. Definition of keywords
Adherence to treatment means following the recommended course of treatment by taking all the medication, as prescribed, for the entire length of time necessary (Department of Health, 2014, p. 51).
Lived experience refers to the way individuals or groups make sense of a phenomenon, their world or situation (Speziale & Carpenter, 2002, p. 53).
Non-adherence refers to the failure of a patient to comply with or follow the treatment programme and medication regimen as prescribed (Smeltzer, Bare, Hinkle, & Cheever, 2013, p. 50).
Treatment is defined as the medical or surgical management of a patient (Stedman, 2013, p. 1590). In this study, treatment is the anti-tuberculosis drugs administered to the patient to destroy the tuberculosis bacilli.
2. Research design and methods
The design used for the study was exploratory, phenomeno-logical and qualitative. Qualitative study is a form of social inquiry that focuses on the way people make sense of their experiences and the world they live in (Holloway & Wheeler, 2010, p. 3). A number of different approaches exist within the wider framework of this type of research and many of these shares the same aim: to understand, describe and interpret social phenomenon as perceive by an individual, group, or culture (Holloway & Wheeler, 2010, p. 3). Qualitative research methods of gathering data are ways of gaining insights through discovering meanings (Burns & Grove, 2009,p. 52) and also helps to obtain in-depth information on sensitive issues which otherwise might not be revealed in quantitative studies.
Phenomenological research identifies the essence of human experiences concerning a phenomenon as described by the participants in the study (Lobiondo Wood & Haber, 2006, p. 569). Lived experience of the world of everyday life is the central focus of phenomenological study, gives meaning to each individual perception of a particular phenomenon and is influence by everything internal and external to the individual (Speziale & Carpenter, 2003, p. 53). Phenomenological method also identifies the way of thinking or perceiving a situation, event or phenomenon.
2.1. Target population and sampling
A purposive sampling method was used for selection of participants from the target population. The target population were the tuberculosis patients using a selected clinic in Tshwane and patients that met the criteria were invited to participate in the study. The inclusion criteria includes patients who have been on tuberculosis treatment for at least four months, who use the selected tuberculosis clinic, 18 years above, able to communicate in English and willing to participate.
2.2. Data collection
In-depth interviews were conducted by the principal investigator with the question "please, can you tell me from your own perspective, what has been your lived experience since you started tuberculosis treatment four months ago?" The patients that met all the criteria were approached after their clinic appointment and were then invited to participate in the study. Sample size was determined by saturation of data and the interviews were conducted in one of the consulting rooms in the tuberculosis clinic after participants' clinic appointment. The interviews were recorded and field notes taken. Each interview lasted between 30 and 45 min. A total of 22 participants participated in the study; 14 participants were new cases on treatment for the first time, while eight participants were on retreatment as they had previously defaulted or interrupted their treatment.
2.3. Measures to ensure trustworthiness
Lincoln and Guba's (1985, pp. 281-331) model of trustworthiness was applied. The model has four criteria which are credibility (truth value), applicability (transferability), consistency (dependability) and neutrality (confirmability). Prolonged interaction of the researcher with the patients on tuberculosis treatment and member checking were used to ensure credibility. Triangulation of data was enhanced by transcribing interviews verbatim, taking field notes and conducting a literature control of findings. A dense description of the research method was provided, ensuring transferability. The transcribed data and the field notes were kept by the principal investigator.
2.4. Ethical considerations
The study was approved by the Research Ethics Committee of the Faculty of Science of the Tshwane University of Technology and Gauteng Department of Health. Written consent was sought from the participants after the study and its purpose had been explained to them. Confidentiality and anonymity were ensured by protecting the participants' identity, privacy, worth and dignity. No connection could be made between the participants and research data. Participants were informed about their right to withdraw from the research at any time.
2.5. Data analysis
The interviews were transcribed verbatim by the principal researcher with the co-authors as the coders. Each interview was coded with a defined coding frame to ensure confidentiality and limit bias. Data analysis was done using the three steps identified by Speziale and Carpenter (2007, p. 88). The first step was the naive reading of each text to gain an impression and formulate ideas for further analysis. The second step was structural analysis to identify meaningful statements through revealing the structure and internal dependent relations that constitute the static state of the text. The third step was the understanding of the interpreted whole from reflection on the naive reading and structural analysis. From each transcript, the significant statements pertaining directly to the lived experience of tuberculosis were identified. Meanings were then formulated from the significant statements. The formulated meanings were then clustered together into themes, allowing for the emergence of themes common to all the participants transcripts. The result was then integrated into an in-depth exhaustive description of the phenomenon.
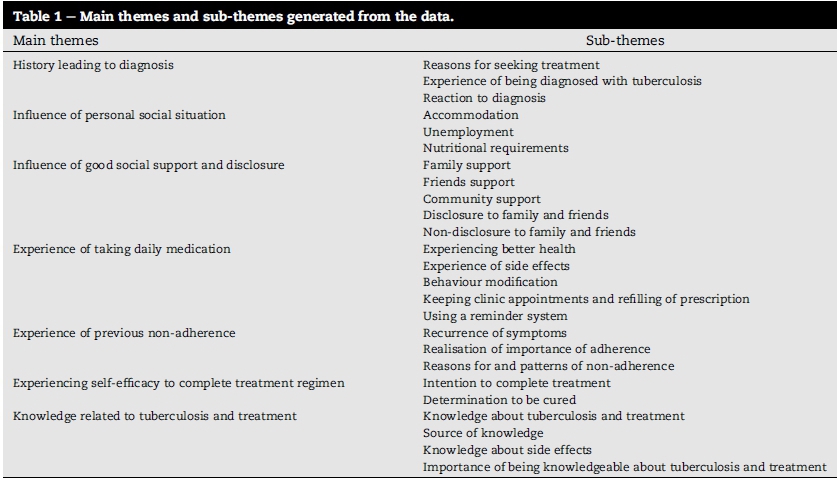
3. Findings
A number of themes and subthemes emerged from the data as reflected in Table 1.
3.1. Demographic information
About half the participants were in the 31-40 years age group while some were agedbetween 41 and 50 years. The participants spoke six languages apart from English, with Sepedi and Sesotho being the most commonly spoken languages, followed by Set-swana. Most of the participants were single, a few were cohabiting and some were married. In addition, most participants achieved an educational level of Grade 8-12, while one-third achieved an educational level of Grade 1-7. Half of the participants were unskilled workers and some were unemployed.
3.2. History leading to diagnosis
History of diagnosis emerged as the first theme and consisted of the sub-themes reasons for seeking treatment, the experience of being diagnosed with tuberculosis and reaction to diagnosis.
3.3. Reason(s) for seeking treatment
Most of the participants sought treatment when the symptoms of tuberculosis became unbearable and they decided to seek a cure. A participant narrated:
'I was weak and I couldn't eat. I went to the doctor and after the test, I was told that I haue tuberculosis.'
A few of the participants did not recognise the tuberculosis symptoms and kept taking over-the-counter medication for months as reported by one participant:
'I mean when I started having the signs of tuberculosis, I didn't know what it was. I was having night sweat and no appetite. Then I was told that I haue tuberculosis after I did the test.'
3.4. Experience of being diagnosed with tuberculosis
Less than one-third of the participants were weak and did not have energy to do anything, some participants had haemoptysis and loss of appetite, and most were coughing with shortness of breath and night sweats. A participant narrated:
'Atfirst, I thought it was just an ordinary cough that will soon go away. So I took some cough medication and I waitedfor it to stop. When it got to one month and I was still coughing, I knew it was something serious.'
Two-fifths of the participants had been diagnosed with tuberculosis before and were being retreated. One participant narrated:
'It was not the first time that I haue had tuberculosis. I had it before and took the treatment. I just didn't complete the treatment.'
3.5. Reaction to diagnosis
Some of the participants felt sad to be diagnosed with tuberculosis and even denied it, a little more than half of the participants were surprised but calmly accepted the diagnosis, while a few were not happy or angry with the diagnosis. One of the participants reported:
'Well I was not coughing, but I was losing weight and did not haue an appetite. After the test, I was diagnosed with tuberculosis. I was surprised to hear that.'
3.6. Influence of personal social situation
Personal social situation encompassed the sub-themes accommodation, unemployment and nutritional requirements.
3.7. Accommodation
Lack of accommodation was prevalent among the participants, as about half of them lacked proper accommodation. One response was:
'I stopped taking my treatment because I was hauing accommodation problems and could no longer stay where I was staying then and I moued to another place.'
3.8. Unemployment
Slightly less than half of the participants were unemployed as narrated by a participant:
'I don't euen haue a job, I only get piece job once in a while.'
3.9. Nutritional requirements
Some of the participants found it difficult to get food and adhere to the nutritional requirement. The unemployed participants were sometimes unable to get food especially the right kind of nutritious food to eat. A participant responded:
'I don't usually eat the fruit and uegetables that they told me to eat in the clinic because I don't haue money to buy food. I just eat any food that I can get from people.'
3.10. Influence of good social support and disclosure
Influence of social support was explored through family support, friends' support and community support, as well as the kind of support and disclosure or non-disclosure to family members and friends.
3.11. Family support
The majority of the participants were able to enjoy good family support. One participant narrated:
'My father checks my clinic appointment date and makes sure I come for it, my mother reminds me to take my medication and my sisters come to the clinic with me wheneuer I haue an appointment.'
The kind of support experienced by the participants was mostly encouragement to continue and complete treatment, provision of food and money where necessary and reminders to take medication daily. One participant responded:
'Yes, my girlfriend supports me. She reminds me to take my medication after eating breakfast. She also comes to the clinic in my place to get the medication whenever I am unable to come...'
3.12. Friends' and community support
The majority of the participants' friends had a positive influence on the participants, although one-fifth of the participants' friends tried to exert negative influences by encouraging participants to take medication irregularly and even to consume alcohol. A participant stated:
'Yes, I told them and though they didn't abandon me, they advised me not to take the medicine sometimes so that I can have drinks with them. But, I do not drink anymore since I started the treatment.'
A few of the participants had some sort of support from their neighbours who helped them with food whenever they did not have food to eat. A participant narrated:
'Sometime when I don't have food I go to my neighbour who gives me some food to eat, then I can take my medicine'.
3.13. Disclosure to family and friends
Three-quarters of the participants disclosed the tuberculosis diagnosis to their family and friends and were able to enjoy some support from them. One of the responses was:
"Yes, I told my husband and children and they are supporting me. They always remind me to take my pills and also encourage me to continue with it until I finish."
3.14. Non-disclosure to family and friends
Some of the participants did not disclose their illness to their family and friends. The reasons included that the participants did not want their families to be worried, were afraid of how their families would receive the news and thought their families would blame them for getting sick. The responses included:
'I don't want my mother to worry about me too, ifI tell her that I am on tuberculosis treatment. Also, I don't know how she will react'.
3.15. Experience of taking daily medication
The experience of taking daily medication was identified as a theme and included the following sub-themes: experiencing better health, experience of side effects, behaviour modification, keeping clinic appointment and refilling of prescriptions, and use of reminders.
3.16. Experiencing better health
All the participants started to experience better health with the commencement of treatment as narrated by a participant:
'I am much better now as I am gaining weight and eating well now. I have been getting better since I started taking the treatment'.
3.17. Experience of side effects
Less than half of the participants experienced side effects. A participant stated:
'The joint pain was unbearable for me, I was much better then and I could not continue to cope with the joint pain. So I just decided to stop taking the treatment and did not come again for my clinic appointment.'
3.18. Behaviour modification
Behaviour modification was interpreted through taking medication daily, practising healthy habits and engaging in moderate exercise.
All participants said that they took their medication every day without missing any, as narrated:
'Immediately after breakfast, I take them. I never miss taking them on any day.'
Some of the participants started to practise healthy habits which they did not do before the diagnosis and treatment. One participant responded:
'I open the window for fresh air to come and I make sure that I take my medicine at the same time every day. I also don't share my plate and cutleries with anyone including my children.'
Two-fifths of the participants among those who were unemployed started doing some form of exercise since they had started treatment to help themselves. A participant narrated:
'Yes, l do more exercise now than before. I walk more and am more active'.
3.19. Keeping of clinic appointments and refilling of prescription
The majority of the participants attended the clinic regularly to keep their appointments and refill their prescription, while a few usually sent someone in their place due to difficulty in getting time off from their employer. A participant stated:
'There were times that I was not release from work to come and my wife had to come to collect the medicine. But today, I told them that the doctor needed to check me and that is why I was released from work to come to the clinic.'
3.20. Use of reminders
All of the participants had set up systems to remind them to take their medication. The systems included putting the medication where the food is kept so that they would see it and be reminded when they got the food and putting reminders/or alarms on their phones. One participant narrated:
'I put a reminder on my phone, so when it goes off, I know it is time to take my medication.'
3.21. Experience of previous non-adherence
The theme experience of previous non-adherence was explored to determine if the participants had ever been non-adherent and included the following sub-themes, reason for and pattern of non-adherence, recurrence of symptoms and realisation of importance of adherence.
3.22. Reasons for and pattern ofnon-adherence
A little more than one-third of the participants had either defaulted on treatment or interrupted treatment previously. The reasons for non-adherence, according to the participants included unavailability of food, sleeping at their own place and experiencing side effects. A participant narrated:
'I find it difficult to get food to eat at times and I was not happy. I could not remember to take my medicine or come for appointment in the clinic'
Among the participants who had defaulted on treatment, the pattern of non-adherence was taking medication irregularly and eventually not taking the medication. A participant responded:
'I still took them once in a while and when it gotfinished, I didn't bother to come to the clinic to get more.'
3.23. Recurrence ofsymptoms
All the participants who had defaulted on treatment reported the return of symptoms as the reason for initiating treatment again. One of the narratives was as follows:
'I fell sick again and I was admitted to the hospital. I was so weak that they put diapers on me and I got tired from just walking to the bathroom. The doctor asked about the reasons why I didn't complete my treatment and I told him about my problems.'
3.24. Realisation of the importance of adherence
As a result of return of the symptoms, the non-adherent participants learnt a lesson on adherence with health education given to them. One of the participant's narratives was:
'I didn't know that I will have to take the treatment for longer once I stopped it and I know now. I must complete my treatment this time so that I can be cured completely.'
3.25. Experiencing self-efficacy to complete treatment regimen
Experiencing self-efficacy to complete treatment regimen was also identified as a theme with the following sub-themes: intention to complete treatment and the determination to be cured.
3.26. Intention to complete treatment
All participants had the intention of completing treatment which they started. A participant narrated:
'I intend to complete my treatment, even ifI move to another area I will ask for transfer to another clinic'"
3.27. Determination to be cured
All participants were ready do all that was required for them to be cured from tuberculosis, so that they could get back to good health. A participant responded:
'Because I want to get well to be able to take care ofmy children, then I have to do what I am told to get well. Taking the treatment is the way to get well, so that is why I must do it.'
3.28. Knowledge related to tuberculosis and treatment
Knowledge related to tuberculosis and treatment emerged as a theme and including the following sub-themes knowledge about tuberculosis and treatment, source of knowledge, knowledge about side effects of medication and importance of being knowledgeable about tuberculosis and treatment.
3.29. Knowledge about tuberculosis and treatment
The participants who had never defaulted on treatment had adequate knowledge about tuberculosis. All of these participants were given health education about tuberculosis at the health facilities, were compliant with health advice and also had knowledge about the consequences of interruption of treatment. A participant narrated:
'The doctor told me and then he explained to me all that I had to do to be cured. I started taking the treatment and I have never missed a day.'
On the other hand, the participants who had previously been non-adherent did not have adequate knowledge about tuberculosis and treatment. A participant narrated:
'I was told when I started the treatment that I must take it for six month in order to be cured. But I didn't know that ifI get sick again, I will have to take the treatment for longer than six months. I thought I will just continue from where I stopped.'
3.30. Knowledge about the side effects of the medication
Half of participants had some knowledge about the side effects of the medication while the other half did not have any knowledge about the side effects. One participant responded:
'Yes I did. I was always dizzy, but because the sister had told me when I was getting the medicine thefirst time that it can happen. I knew that it was the side effect, so I complained to the doctor, who prescribed something for it and then it got better.. .'
3.31. Source of knowledge regarding side effects of the medication
All the participants who had some knowledge about the side effects of the medication were able to access the knowledge through the health education given to them at the health facilities. One response was:
'I just felt like vomiting and since the nurse had told me before that it can happen, I was not surprised and then it passed with time. Since I was okay whenever I took them, I just continued taking them.'
3.32. Importance of being knowledgeable about tuberculosis and treatment
All the participants had understanding about the importance of being knowledgeable about tuberculosis and treatment. A participant responded:
'Eating the right food and taking my medicine like I am supposed to. I decided to do whatever I have to do to get well and be free from tuberculosis.'
4. Discussion of findings
Lived experience and the meaning a person ascribes to it are important if the perception of the patient on treatment is to be understood. The findings from the study revealed that though tuberculosis is such a prevalent disease, the participants did not expect a diagnosis of tuberculosis. The manifestation of tuberculosis made the participants sought diagnosis and treatment. Most of the participants started seeking treatment as soon as they started having serious symptoms such as fatigue, apathy, loss of appetite, persistent coughing with shortness of breath, and haemoptysis. However, some participants who experienced symptoms such as night sweat and weight loss, delayed presenting at the health facilities for diagnosis and treatment until a family member intervened. The findings of this study are similar to those conducted in Brazil by Hino, Takahashi, Bertolozzi, and Yoshikawa (2011,p. 1659) who explored the health needs and vulnerabilities of tuberculosis patients according to the accessibility, attachment and adherence dimensions. Evidence was found that the signs and symptoms of tuberculosis forced the participants to seek diagnosis and treatment.
The personal social situation of the participants influenced their adherence. Unemployed participants had difficulty adhering to treatment because they could not afford the recommended nutritious food. Previous researchers have linked the personal social situation of tuberculosis patients on treatment with non-adherence (Gebremariam, Bjune, & Frich, 2010,p. 3, Jaiswal et al. 2003, p. 630). Patients with social problems or economic constraints are more likely to default on treatment. In as much as the participants were prepared to adhere to their therapeutic regimen, their social economic situation did not help, hence they were not adherent.
Social support was found to be crucial to patients' treatment. All the family support appeared to be a strong influence on patient adherence. The negative attitude of the community and friends coupled with health professionals' attitude may also have an effect on a patient's adherence to treatment. Most of the participants in this study reported that the support that they had from family members, friends and the friendly attitude of the health professionals helped them to adhere to the treatment and they perceived the support to be necessary in their treatment-taking experience. Previous researchers have found evidence to suggest that negative attitudes of health professionals and lack of social support contributes to patients defaulting on treatment (Gebremariam et al., 2010,p. 5; Njozing, Edin, Sebastian, & Hurtig, 2011,p.7, Naidoo et al., 2009, p. 62; Tadesse, Demissie, Berhane, Kebede, & Abebe, 2013, p. 4).
There is need for disclosure, therefore disclosure should be encouraged. Disclosure usually precipitates support which is essential for adherence, as revealed by the participants in the study. The participants who did not disclose their tuberculosis diagnosis and treatment to their families and friends could not get any form of support from them. The participants in this study attested to the fact that social support is essential if the therapeutic regimen is to be adhered to and nondisclosure means no support from these quarters. A study conducted in India by Jaiswal et al. (2003, p. 630), revealed that issues such as poor communication and lack of attention and support from the family as well as health provider to the patient sometimes precipitated default. Health professionals should therefore support patients on treatment by encouraging them to disclose their tuberculosis diagnosis and treatment to their family members and friends, so that they can get some help and support during their treatment period.
In taking the medication daily, the participants were able to enjoy better health as long as they were able to maintain adherence. Experiencing serious side effects is a challenge to tuberculosis treatment and the situation is further aggravated if health professionals do not inform patients about the potential side-effects. A qualitative study in China (Xu et al. 2009, p. 6) reported that side effects of the medication impacted on the adherence of participants in that study, as some of the participants stopped taking the medication just to avoid the side effects. Findings from the current study suggest that adherence counselling is necessary for all patients prior to the commencement of treatment, which might facilitate adherence. Patients need to be informed beforehand about the potential side effects so that they can be prepared and not be taken unawares by the side effects when they do manifest.
The participants in this study also revealed that they believed in the efficacy of the medical treatment and was one of the reasons they were adherent. Previous studies about the beliefs of patients on the efficacy of treatment indicated this may have an impact on adherence to treatment (Edginton, Sekatane, & Goldstein, 2002, p. 1080; Khan, Walley, Witter, Shah, & Javeed, 2005, p. 260). Patient choice in taking treatment is framed by the physiological and psychological impacts of the disease and as well as by the social and cultural structures in which the person is immersed (Sagbakken, Frich, & Bjune, 2008, p. 9). Belief in treatment efficacy appeared to be related to the patients' confidence in the medical health system. When the medical health system functions well, it is useful to the patients. On the other hand, if the medical health system is not functioning well, patients may place their trust and care in the traditional health system (Edginton et al., 2002, p. 1080; Khan et al., 2005, p. 260). However, if the treatment regimen prescribed by a health practitioner is consistent with a patients' understanding of what caused his or her illness, the patient is more likely to adhere to treatment (Edginton et al. 2002, p. 1080).
The knowledge related to tuberculosis and treatment had a significant impact on the adherence of the participants. The participants who had adequate health literacy level in this study indicated they acquired their knowledge from health education and talks from health professionals in the clinic. Molapo (2013, p. 247) found evidence that health education related to a specific condition, such as tuberculosis, improves a patient's knowledge regarding that condition. Patients who have low knowledge about tuberculosis and treatment are usually non-adherent (Kaona, Tuba, Siziya, & Sikaona, 2004,p. 7) Moreover, if there is adequate knowledge about the disease condition, it tends to have a relevant impact on the health behaviour and adherence of the patients. There is need for improve communication and health education in health facilities, clinics and in the communities.
5. Conclusions
The study revealed that tuberculosis patients on treatment had different experiences in adhering to their treatment. The personal social situations of the participants influenced the adherence of the participants to treatment. Furthermore, knowledge about tuberculosis and support from family and friends influenced adherence positively. Side effects of the medicine were identified as a major cause of non-adherence by the participants who had been non-adherent in the past.
5.1. Recommendations
Professional nurses can facilitate adherence through improved communication and counselling by exploring the socio-economic background of each patient. Therefore, the care offered by health professionals must be marked by quality listening, appreciation of patient complaints and identification of their needs. Tuberculosis treatment, its side effects and duration should be discussed before the commencement of treatment. In addition, patients should always be encouraged to inform and include familymembers, friends and, where appropriate, their significant others in their diagnosis and treatment.
Patient support groups should be set up in health facilities, where tuberculosis services are offered and where patients should be referred at the commencement of treatment. The patients support groups will serve as support for patients, providing a common ground where patients meet and are accountable to each other. The support groups can also help empower patients who are economically constrained by providing funds for them so that they become self-sustained and can be the motivation/motivator for the patients.
6. Limitations of the study
The study was limited to a purposive sample of tuberculosis patients who have been on treatment for at least four months and living in Tshwane. As Tshwane is a metropolis, the experience of patients on treatment may be different from those of patients in rural areas. The study was also limited to voluntary participation; therefore, because the nature of the topic material was sensitive and personal; the participants' level of honesty may have been compromised.
Acknowledgements
The authors would like to thank Tshwane University of Technology Full Time Postgraduate Scholarship (2012) for providing the funds for the study, as well as, the management of the clinic for their help during the data collection and most of all, the participants who spared the time to grant the interviews. The funding institution had no involvement in the design, collection, analysis and interpretation of the data.
REFERENCES
Amuha, M. G., Kutyabami, P., Kittu, F. E., Odoi-Adome, R., & Kalyango, J. N. (2009). Non-adherence to anti-TB drugs among TB/HIV co-infected patients in Mbarara Hospital, Uganda: Prevalence and associated factors. African Health Sciences, 9(S1), 8-15. [ Links ]
Burns, N., & Grove, S. K. (2009). Understanding nursing research (6th ed.). Philadelphia: Saunders. [ Links ]
Department of Health. (2014). National tuberculosis management guideline. Viewed 2 May 2016, from http://www.nic.ac.za/assets/files/Acrobat%20Document2.pdf. [ Links ]
Edginton, M. E., Sekatane, C. S., & Goldstein, S. J. (2002). Patients beliefs: Do they affect TB control? A study in a rural district in South Africa'. International Journal of Tuberculosis and Lung Disease, 6(12), 1075-1082. [ Links ]
Gebremariam, M. K., Bjune, G. A., & Frich, J. C. (2010). Barriers and facilitators of adherence to TB treatment in patients on concomitant TB and HIV treatment: A qualitative study. BMC Public Health, 10, 651. viewed 2 May 2016, from http:// bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-10-651. [ Links ]
Hino, P., Takahashi, R. F., Bertolozzi, M. R., & Yoshikawa, E. (2011). The health needs and vulnerabilities of tuberculosis patients according to the accessibility, attachment and adherence dimensions. Revista da Escola de Enfermagem da USP, 45(2), 1656-1660. [ Links ]
Holloway, I., & Wheeler, S. (2010). Qualitative research in nursing and health care (3rd ed.). West Sussex: Wiley and Black well. [ Links ]
Jaiswal, A., Singh, V., Ogden, J. A., Poter, J. D. H., Sharma, P. P., Sarin, R., et al. (2003). Adherence to tuberculosis treatment: Lessons from the urban setting of Delhi, India. Tropical Medicine and International Health, 8(7), 625-633. [ Links ]
Kaona, F. A. D., Tuba, M., Siziya, S., & Sikaona, L. (2004). Assessment of the factors contributing to treatment adherence and knowledge of TB transmission among patient on TB treatment. BMC Public Health, 4, 68. viewed 2 May 2016, from http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-4-68. [ Links ]
Khan, M. A., Walley, J. D., Witter, S. N., Shah, S. K., & Javeed, S. (2005). Tuberculosis patient adherence to direct observation: Results of a social study in Pakistan. Health Policy Plan, 20(6), 354-365. [ Links ]
Lincoln, Y., & Guba, E. (1985). Naturalistic inquiry. Beverley Hills, CA: Sage. [ Links ]
Lobiondo Wood, G., & Haber, J. (2006). Nursing research methods and critical appraisal for euidence-based practice (5th ed.). St Louis: Mosby. [ Links ]
Molapo, J. T. (2013). Tuberculosis specific behaviour change communication material for a low-literacy population in Mamelodi. PhD thesis. Pretoria: Tshwane University of Technology. [ Links ]
Naidoo, P., Dick, J., & Cooper, D. (2009). Exploring tuberculosis patients' adherence to treatment regimens and prevention programmes at a public health site. Qualitative Health Research, 19(1), 55-70. [ Links ]
Njozing, B. N., Edin, K. E., Sebastian, M. S., & Hurtig, A. (2011). Voices from the frontline: Counsellors' perspectives on TB/ HIV collaborative activities in the Northwest Region, Cameroon. BMC Health Services Research, 11, 328. viewed 2 May 2016, from http://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-11-328. [ Links ]
Sagbakken, M., Frich, J. C., & Bjune, G. (2008). Barriers and enablers in the management of tuberculosis treatment in Addis Ababa, Ethiopia: A qualitative study. BMC Public Health, 8, 11. viewed 2 May 2016, from http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-8-11. [ Links ]
Selala, M. T. (2011). Factors contributing to increase in the number of TB patient in the Ehlandeni District. Mpumalanga Province: M.Cur thesis, University of Limpopo. viewed on 20 Sep 2016 from http://ul/netd.ac.za/bitstream/10386/470/3/selala. [ Links ]
Sissolak, D., Marais, F., & Mehtar, S. (2011). TB infection prevention and control experiences of South African nurses: A phenomenological study. BMC Public Health, 11, 262. viewed 20 Sep 2016 from http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-8-11-262. [ Links ]
Smeltzer, S. C., Bare, B. G., Hinkle, J. L., & Cheever, K. H. (2013). Brunner and Suddarth's textbook of medical-surgical nursing (11th ed.). Philadelphia, PA: Lippincott William & Wilkins. [ Links ]
Speziale, H. J. S., & Carpenter, D. R. (2002). Qualitative research in nursing: Advancing the humanistic perspective (3rd ed.). Philadelphia, PA: Lippincott Williams & Wilkins. [ Links ]
Speziale, H. J. S., & Carpenter, D. R. (2003). Qualitative research in nursing: Advancing the humanistic perspective. Philadelphia: Lippincott. [ Links ]
Speziale, H. J. S., & Carpenter, D. R. (2007). Qualitative research in nursing: Advancing the humanistic perspective (4th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. [ Links ]
Stedman, T. L. (2013). Stedman's medical dictionary for the health professions and nursing (6th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. [ Links ]
Tadese, T., Demissie, M., Berhane, Y., Kebede, Y., & Abebe, M. (2013). Long distance travelling and financial burdens discourage tuberculosis DOTS treatment initiation and compliance in Ethiopia: A qualitative study. BMC Public Health, 13, 424. viewed 4 May 2016, from http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-13-424. [ Links ]
Volmink, J., Matchaba, P., & Garner, P. (2000). Directly observed therapy and treatment adherence. Lancet, 355(9212), 1345-1350. [ Links ]
World Health Organisation. (2015). Global tuberculosis report. Viewed 20 Sep 2016 from http://www.who.int/iris/bitstream/10665/191102/1/9789241565059_en.pdf. [ Links ]
Xu, W., Lu, W., Zhou, Y., Zhu, L., Shen, H., & Wang, J. (2009). Adherence to anti-tuberculosis treatment among pulmonary tuberculosis patients: A qualitative and quantitative study. BMC Health Services Research, 9, 169. viewed 2 May 2016, from http://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-9-169. [ Links ]
Received 14 June 2016
Accepted 7 March 2017
* Corresponding author.
E-mail address: phummyobe@gmail.com (O.O. Akeju). Peer review under responsibility of Johannesburg University.


{kind=link}