










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkHealth SA Gesondheid (Online)
versão On-line ISSN 2071-9736
versão impressa ISSN 1025-9848
Health SA Gesondheid (Online) vol.22 Cape Town 2017
http://dx.doi.org/10.1016/j.hsag.2016.07.001
REVIEW ARTICLE
Khathutshelo Percy Mashige
University of KwaZulu-Natal, Discipline of Optometry, Private Bag X54001, Durban, 4000, South Africa
ABSTRACT
AIM: To systematically review relevant literature investigating the classification and nomenclature, epidemiology and pathophysiological mechanisms, as well as diagnosis and treatment of ocular allergy.
METHOD: The Medline, PubMed, Elsevier Science Direct, and Google Scholar databases were used to search for evidence-based literature on ocular allergy.
Main outcome measures: Classification and nomenclature, epidemiology and pathophysio-logical mechanisms, diagnosis and management of ocular allergy.
RESULTS: The search retrieved 5200 number of studies of which 6 met the criteria.
CONCLUSIONS: While numerous studies regarding pharmacological and immunological research have identified new treatment options, there is a dearth of clinical studies to discover the biomarkers and immune therapeutic management to control sensitisation and effector phases of this condition. Given the complexity of this condition due to the multifactorial nature of the possible aetiologies, rigorous well-designed scientific studies are needed to determine the exact classification, prevalence and underlying immune pathological processes of ocular allergy.
Keywords: Ocular allergy Perennial conjunctivitis Allergic conjunctivitis Atopic keratoconjunctivitis Vernal keratoconjunctivitis Giant papillary conjunctivitis
1. Introduction
Ocular allergies encompass a group of hypersensitivity disorders to normally harmless substances, known as allergens and can be observed as the only dominant presentation of an allergic sensitisation, or are associated with rhinitis, asthma, atopic dermatitis or food allergy (Leonardi et al., 2012). The most common clinical presentations of ocular allergy are conjunctival hyperaemia (redness) and chemosis (swelling), itching and tearing, and vision loss in severe cases (Chowdhury, 2013; Leonardi, De Dominicis, & Motterle, 2007). Management of this condition is based on minimising contact of the causal allergen with the conjunctiva using a series of protective measures, with medication assisting in controlling the symptoms produced by the allergic inflammatory process (Chowdhury, 2013; La Rosa et al., 2013).
There is currently no universal standard nomenclature and classification, making an estimation of ocular allergy prevalence challenging. In addition, as most ocular allergic diseases are comorbidities of rhinitis, available prevalence data encompasses both ocular and nasal symptoms, making it impossible to separate ocular allergy and allergic rhinitis (La Rosa et al., 2013). Moreover, controversy continues to surround the exact pathophysiological mechanisms involved in ocular allergic diseases. The purpose of this paper is therefore to systematically review scientific and published research studies on the classification and nomenclature, epidemiology and pathophysiological mechanisms, diagnosis and management of ocular allergy.
2. Method and scope of review
The initial search term was 'ocular allergy' by the Information Specialist (IS). An article was considered for review if it met the inclusion criteria of reporting on the classification, nomenclature, epidemiology, pathophysiology, clinical presentation, or an approach to diagnosis and management of ocular allergy. Articles published between 1994 and 2015 years in English, and indexed in the following electronic databases were searched: Medline, PubMed, Elsevier Science Direct, and Google Scholar. The standard process for a systematic literature review was adopted:
1. Titles were reviewed and those which were not relevant were rejected.
2. Abstracts of publications that were not rejected were obtained.
3. Two individuals reviewed the abstracts independently and rejected further papers that were not eligible. A third individual adjudicated if there were any differences.
4. Full text of the abstracts selected was obtained.
5. Further papers were rejected if, on closer inspection, were not relevant or did not provide sufficient detail.
6. Tables for data extraction were prepared.
7. Two people extracted data and compared entries.
The full copies of articles identified by the search, and considered to meet the inclusion criteria based on their title, abstract and subject descriptors, were obtained for the data synthesis. Articles identified through reference lists and bibliographic searches were also considered for data collection based on their title. Two reviewers independently selected articles against the inclusion criteria. Discrepancies in reviewer selections were resolved at a meeting of the reviewers prior the selected articles being retrieved.
2.1. Critical appraisal
Identified studies were assessed independently for quality and validity by two reviewers using the corresponding checklist from the Critical Appraisal Skills Programme (CASP) tools (Critical Appraisal Skills Programme, 2014) before being included in the review. Any disagreements that arose between the reviewers were resolved through discussion and with the assistance of a third person where required.
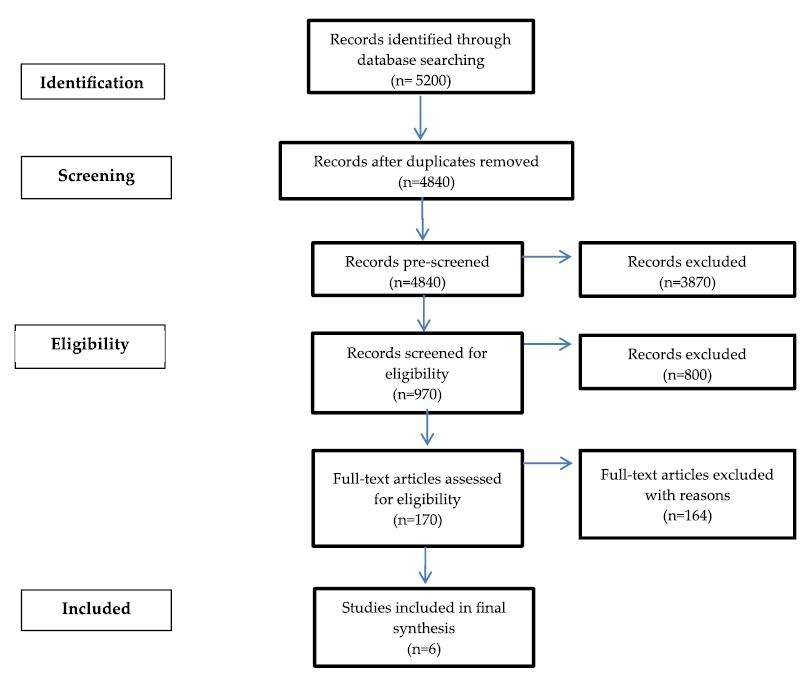
The initial search yielded a total of 5200 records, of which the Information Specialist (IS) removed 360 duplicates and pre-screened 4840 records. Thereafter 3870 records which were not relevant to the scope of the review were removed. The reviewers screened the remaining 970 records and discarded a further 800 records as not meeting the inclusion criteria. A total of 170 full text reports were obtained for further assessment, of which 6 articles met the inclusion criteria and 164 articles were excluded, with reasons, as they were not relevant to the objectives of the review. The flow chart and check list of the CASP tool used are shown in Appendices 1A and 2 respectively. The 6 studies included in the synthesis covered all aspects with respect to the classification and nomenclature, epidemiology, pathophysiological mechanisms, diagnosis and treatment of ocular allergy. A summary of the selected studies is shown in Appendix 1B.
3. Classification and nomenclature
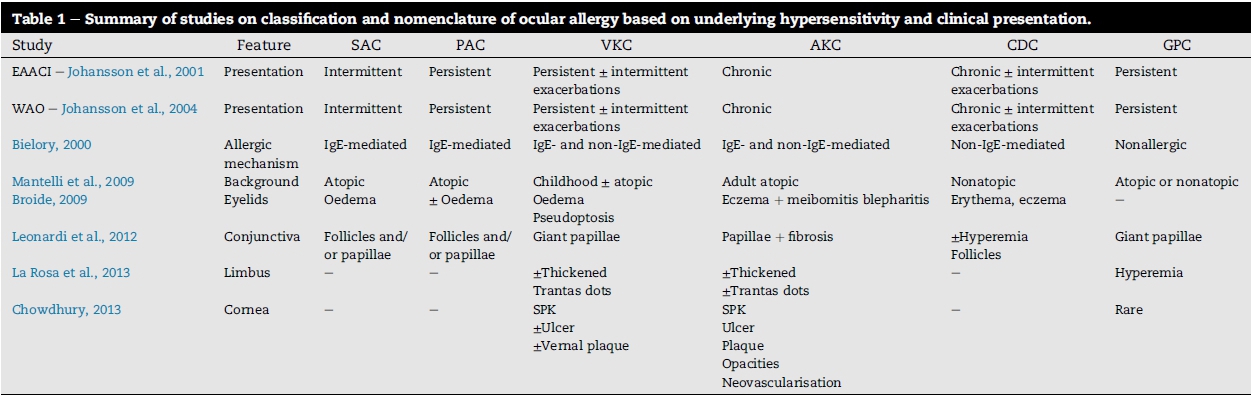
According to the traditional classification of ocular allergy, the six forms are: seasonal (SAC) and perennial allergic conjunctivitis (PAC), vernal keratoconjunctivitis (VKC), atopic keratoconjunctivitis (AKC), contact dermatoconjunctivitis (CDC), and giant papillary conjunctivitis (GPC) (Leonardi et al., 2007). This traditional classification is based on clinical presentation (Table 1) or on pathophysiology, according to the different hypersensitivity mechanisms introduced by Gell and Coombs. Their classification divides allergies into four pathophysio-logical types, namely anaphylaxis (type I), antibody-mediated cytotoxic reactions (type II), immune complex-mediated reactions (type III), and delayed type hypersensitivity (type IV) (Sánchez et al., 2011). However, many hypersensitivity reactions cannot be explained in this context and its use is therefore no longer recommended (Sánchez et al., 2011). Despite these limitations, the Gell and Coombs's classification is still valid in a few well-defined circumstances.
Efforts have recently been made to further clarify the classification and nomenclature of ocular allergy. If different aspects of the condition are considered, such as its clinical presentation and duration or the immunopathogenesis, the criteria for ocular allergy may change (Leonardi et al., 2007). For example, ocular allergies can be classified as 'intermittent' or 'persistent', and 'mild', 'moderate' or 'severe' depending on their evolution and severity. Similarly, symptoms can be considered as 'acute' or 'chronic' and 'recurrent' according to onset and duration, or as 'follicular' and 'papillary conjunctivitis', 'cicatrising' and 'noncicatrising', emphasising the predominant clinical presentations (Leonardi et al., 2007).
In 2001, the European Academy of Allergy and Clinical Immunology (EAACI) and the Nomenclature Review Committee of the World Allergy Committee (WAO) jointly introduced a revised nomenclature that distinguishes between allergic and nonallergic hypersensitivity reactions, with allergic diseases being further divided into IgE- and non-IgE hypersensitivities (Johansson et al., 2001, 2004). The advantage of this new classification was that it gave a more schematic immunopathological approach, with IgE-mediated ocular allergy being divided into intermittent and persistent forms, the latter being classified as VKC and AKC. However, a serious limitation of this classification is contact dermato-conjunctivitis (CDC), which is a 'non-IgE-mediated form of localized contact dermatitis, but immunologically different from VKC or AKC' (Leonardi et al., 2007). In addition, 'contact lens-related GPC should be considered as non-IgE mediated, mechanically related to the lens micro-trauma, which, however, shares some immunopathological aspects with VKC' (Leonardi et al., 2007), which can lead to more confusion. The above-mentioned limitations prompted the international Ocular Inflammation Society (IOIS) to propose a more comprehensive classification that included both the 'IgE-mediated' SAC and PAC and the 'non-IgE-mediated' VKC and AKC (Table 1). However, this latest classification system is unclear, and a new classification system is therefore desirable, preferably derived from the varied pathophysiological mechanisms operating in the different forms of ocular allergy.
4. Epidemiology
Allergic eye diseases are reported to have dramatically increased since the year 2000 and are the most common conditions affecting the external adnexa (Sanchez et al., 2011). The epidemiology of ocular allergy has not been sufficiently investigated to date, and most of the available prevalence data encompasses both ocular and nasal symptoms. For example, a study in Italy involving 898 new patients visiting an allergy clinic found that 40% reported symptoms of ocular allergy, and 66% were also diagnosed with seasonal allergic rhinitis (Bonini, 2006). A study conducted in Japan found that 90% of all patients with pollen allergy presented with allergic conjunctivitis (Takano, Narita, & Kobayashi, 2004). Studies in Sweden (Hesselmar, Aberg, Eriksson, & Arberg, 2001), Spain (Ibanez & Garde, 2009) and Brazil (Riedi & Rosario, 2010) also found the prevalence of ocular allergy among children to be associated to rhinitis in the majority of the cases. The International Study of Asthma and Allergies in Childhood (ISAAC) reported a prevalence of rhinitis with itchy eyes (allergic rhi-noconjunctivitis) of up to 40% of the population in developed countries (La Rosa et al. 2013). The above prevalence figures reflect ocular allergy associated with other coexisting allergic diseases, and not being isolated ocular symptoms. This has important clinical implications, as patients usually seek medical advice for the coexisting allergic diseases, and the ocular symptoms are often not fully appreciated or adequately examined, contributing to the suboptimal management of patients with ocular allergy.
Although the ISAAC study reported that the prevalence of this condition in developing countries was low, it was not assessed for isolated ocular allergic conditions. Recent studies have reported prevalence rates of 7.9%, 9.1% and 32% in Gambia, Ghana, and Nigeria respectively (Abokyi, Koffuor, Ntodie, Kyei, & Gyanfosu, 2012; Malu, 2014; Wade, Iwuora, & Lopez, 2012). In countries with high rates of HIV infection, such as South Africa, ocular allergies have been reported to be more prevalent in patients with HIV/AIDS (Visser, 2013).
The impact of ocular allergy can lead to lost economic gain, missed employment and educational opportunities, and result in a generally reduced quality of life. Pitt et al. (2004) estimated the annual treatment cost per patient to vary from 64£ to 124£ in Oxfordshire, UK, with a reduction in productivity of 2.3 h/week during the pollinic season. A study in Spain showed an estimated cost of 348.50 V/year for each patient with SAC (Smith et al., 2005), indicating that ocular allergy is a major public health concern in these countries. While it has been reported that the prevalence of ocular allergy in many other countries has increased over the last 40 years, the costs related to treating it are not available. A number of questionnaires, validated in the Spanish population, have been developed to explore different aspects of this condition (Sánchez et al., 2011). It is therefore suggested that similar questionnaires be developed and validated for other population groups, including South Africans, to explore the impact of ocular allergy. In addition, well-conducted epidemiological studies are needed to determine the exact prevalence, severity and impact of this condition.
5. Pathophysiology and clinical entities
Allergic eye diseases generally fall into two main categories namely: IgE-mediated and cell-mediated conditions. Substances such as histamines, bradykinins, serotonins, leuko-trienes, prostaglandins, major histocompatibility complex (MHC1), interferons, chemotactic factors and the complement systems have been reported to be involved in the patho-physiology of ocular allergic diseases (Campbell & Mehr, 2015). Pathophysiology involves two stages namely: sensitisation and effector phase reaction. The sensitisation phase results in generating a predominantly Th2 immune response with the subsequent production of IgE antibodies (Abelson, Smith, & Chapin, 2003). The second phase, initiated with a second encounter with an antigen, culminates with the activation of effector mechanisms, such as the release of histamines and granulocytes degranulation (Abelson et al. 2003). More than five decades after being identified as a unique condition, there is still no common understanding of the allergic process or the terms used to describe the underlying immune pathophysio-logical mechanisms of ocular allergy. Research efforts need to be directed towards understanding the possible underlying immune patho-mechanisms in the different types of ocular allergies.
5.1. Seasonal allergic conjunctivitis
Seasonal allergic conjunctivitis (SAC) is the most common form of all ocular allergy disease, and is usually triggered by exposure to airborne pollens produced by plants that cause hay fever, the signs and symptoms typically occurring in spring and summer (La Rosa et al., 2013). The patho-mechanism involves an IgE-mediated type-I hypersensitivity, with the early response clinically lasting for 20-30 min (La Rosa et al., 2013). The late phase reaction is due to the presence of inflammatory cells in the conjunctival mucosa, and is brought about by activation of vascular endothelial cells, which express adhesion molecules, such as intercellular adhesion molecule (ICAM) and vascular cell adhesion molecule (VCAM) (La Rosa et al., 2013). They also express chemo-kines, such as regulated upon activation normal T cell, expressed and secreted (RANTES) chemokines, monocyte chemo attractant protein (MCP), interleukin (IL)-8, eotaxin and macrophage inflammatory protein (MIP)-1 alpha (La Rosa et al., 2013). The released histamine and other mediators cause hyperaemia, itching, burning, swelling and tearing of the eyes, which often irritate the nasal mucosa (Bielory & Friedlaender, 2008). Topical non-steroidal anti-inflammatory drugs (NSAIDS) or steroids, in addition to antihistamine/mast cell stabilisers, are used to treat severe symptoms of SAC. Alrex is the only topical steroid approved for the temporary relief of seasonal and perennial allergies, while preservative-free Lotemax ointment can be used as an alternative (Sánchez et al., 2011).
5.2. Perennial allergic conjunctivitis
Perennial allergic conjunctivitis (PAC) is milder than SAC, and is a chronic condition that occurs throughout the year, being induced by exposure to dust, mites, fungi, animal epithelial and/or occupational allergens (Friedlaender, 2011). PAC affects young adults between 20 and 40 years of age, but has no gender preference (Friedlaender, 2011). The pathophysiology of PAC is the same as that of SAC, with patients presenting with bilateral itching, tearing and burning sensation (Friedlaender, 2011). There is also conjunctival injection but no corneal involvement (Fig. 1). Blurred vision and photophobia may be due to an alteration in the composition and instability of the tear film (Bielory & Friedlaender, 2008).

Identifying potential causes and triggers, and avoiding or limiting exposure to the allergen, are the mainstay treatments (Bielory & Friedlaender, 2008). Environmental modifications, such as the use of indoor air filters, air conditioning, isolating pets, and cleaning dust, dander and moulds, are helpful (Friedlaender, 2011). Driving with the windows closed can help to reduce exposure to other types of allergens (Friedlaender, 2011). Artificial tears and cold compresses can help reduce initial ocular symptoms, but manypatients require short-term therapy with a steroid or an NSAID (Friedlaender, 2011).
5.3. Vernal keratoconjunctivitis
Vernal keratoconjunctivitis (VKC) is a self-limiting, chronic allergic inflammation of the ocular surface that typically affects young people and is usually more common in warm tropical climates (Lambiase et al., 2009). It is more frequent in males, with an increased incidence of those between 11 and 13 years of age (Lambiase et al., 2009). The symptoms may be seasonal or perennial, with exacerbations generally in summer or in autumn (Friedlaender, 2011; Lambiase et al., 2009). It is associated with a history of allergy to pollen or other allergic conditions, such as atopic dermatitis, allergic rhinitis, or asthma (Friedlaender, 2011; Lambiase et al., 2009).
The pathophysiology is not precisely known, although two hypersensitivity mechanisms (type I and type IV) appear to be involved (La Rosa et al., 2013). In the presence of an antigen, lymphocyte activation (predominantly of the Th2 subpopu-lation) takes place and there is abundant mucosal secretion in the affected individuals (Friedlaender, 2011; La Rosa et al., 2013). VKC has three clinical forms: palpebral, limbal, and mixed, the clinical presentation including severe ocular itching, redness, swelling, mucous discharge and photophobia (La Rosa et al., 2013). The most characteristic sign is cobblestonelike swelling called giant papillae on the upper tarsal conjunctiva, which can be seen by flipping the upper eyelid (Figs. 2 and 3). IL-4 and IL-13 are involved in forming giant papillae by inducing extra-cellular matrix production and the proliferation of conjunctival fibroblasts, with these giant papillae being filled with neutrophils, plasma cells, mononuclear cells, eo-sinophils and mast cells (La Rosa et al., 2013).


Corneal involvement is in the form of superficial punctate keratitis, ulcer formation, neovascularisation, pannus formation and Horner Trantas dots (that consist of clumps of necrotic eosinophils, neutrophils and epithelial cells). These eyes are prone to herpetic and fungal keratitis and the patients also develop atopic cataracts that are anterior shieldlike cataracts (La Rosa et al., 2013). High levels of IgE and mast cell mediators are found in the tears of VKC patients (Friedlaender, 2011). Oral and topical antihistamines, as well as mast cell stabilisers, are useful to treat VKC, particularly after the initial inflammation is minimised (Bielory & Friedlaender, 2008). Depending on the severity, Lotemax or Pred Forte may be used for several weeks, and Alrex for longer, due to its improved safety profile (Sánchez et al., 2011).
5.4. Atopic keratoconjunctivitis
Atopic keratoconjunctivitis (AKC) is a bilateral chronic inflammatory disease of the ocular surface and eyelids (La Rosa et al., 2013). Its pathological process involves chronic degranulation of the mast cells mediated by IgE, and immune mechanisms mediated by Th1 and Th2-lymphocytes derived cytokines, eo-sinophils and other inflammatory cells (Leonardi et al., 2007). AKC is often associated with atopic co-morbidities such as asthma and eczema, and therefore requires multi-disciplinary management (Leonardi et al., 2007). Typical ocular findings include mild or severe conjunctival injection and chemosis, giant papillae, conjunctival scarring, and Trantas dots (Bielory & Friedlaender, 2008). AKC patients may also develop atopic cataracts, this being the most debilitating type of allergic conjunctivitis with high rates of vision impairment (Sánchez et al., 2011). Topical corticosteroids are the mainstay treatment for this condition, with antihistamine/mast cell stabilisers reserved for prophylactic use (Sánchez et al., 2011). Topical cyclosporine A has been reported to be effective in improving the symptoms of AKC (Sánchez et al., 2011).
5.5. Contact dermatoconjunctivitis
Contact dermatoconjunctivitis (CDC), contact allergy or allergic contact dermatitis is a type-IV hypersensitivity reaction, and occurs through interaction of an antigen with Th1 and Th2 cell subsets followed by a release of cytokines (Niederkom, Chen, Mellon, Stevens, & Mayhew, 2010). The pathomechanism involves two phases, the first being sensi-tization, where antigen presenting cells process antigen-MHC class II complex interacts with T-lymphocytes, resulting in the differentiation of CD4+ T-lymphocytes into memory T-lym-phocytes (Niederkom et al., 2010). In the second elucidation phase, the interaction between the antigen-MHC-II complex and memory T-cells stimulates the proliferation of T-cells and the release of cytokines (Niederkom et al., 2010).
Allergens are generally simple chemicals that combine with skin protein to form complete allergens, with examples including poison ivy, neomycin, latex, atropine and its derivatives (Niederkom et al., 2010). Contact allergy involves the ocular surface, eyelids and periocular skin, with the initial sensitization with a contact allergen taking several days (Niederkom et al., 2010). The reaction may peak 2-5 days after re-exposure, the delayed reaction being due to the slow migration of lymphocytes to the antigen depot (La Rosa et al., 2013). The term 'delayed hypersensitivity' is sometimes given to these reactions, in contrast to 'immediate hypersensitivity', where the rapid development of reactions is mediated by IgE antibodies (La Rosa et al., 2013). Upon re-exposure to the allergen, an indurated erythematous reaction slowly develops (Figure 4). Withdrawing and avoiding contact with the allergen is effective in treating CDC, however, severe cases may require topical or systemic corticosteroids (La Rosa et al., 2013).

5.6. Giant papillary conjunctivitis
Giant papillary conjunctivitis (GPC) is not a true ocular allergy, but rather an irritant phenomenon that induces giant, medium or small papillae in the superior palpebral conjunctiva (Forister et al., 2009). GPC may occur in the presence of soft, silicone hydrogel and gas-permeable contact lens wear, exposed sutures, scleral and prosthetic contact lenses, and with floppy eyelid syndrome (Forister et al., 2009). The close association between contact lens and GPC is believed to be due to the protein build-up on the surface of the lenses, as well as to their irregular edges that cause irritations (Friedlaender, 2011). This condition used to be classified as an allergic phenomenon due to the similarity of conjunctival changes with vernal conjunctivitis (Figure 2). There is no increase in IgE or histamine in the tears of GPC patients, and the conjunctival tissues may contain mast cells, basophils, or eosinophils, but not to the extent of an allergic reaction (Friedlaender, 2011). Itching and redness, mucous discharge, contact lens discomfort and intolerance, as well as contact lens coating and excessive movement are common (Forister et al., 2009). Antihistamine/mast cell stabilisers and short-term steroid use (such as Lotemax and Fluorometholone) are the preferred treatment options (Forister et al., 2009).
6. Diagnostic tests
The diagnosis of ocular allergy is confirmed by a clinical history of typical eye symptoms, as well as in-uiuo or in-vitro tests directed towards detecting free or cellbound IgE (Friedlaender, 2011). Allergy skin prick tests are used to demonstrate an IgE-mediated reaction and laboratory investigations such as the radio-allergosorbent test, measures allergen specific IgE antibody (Friedlaender, 2011). Eosinophils in conjunctival scrapings are diagnostic of allergy and are elevated in VKC, AKC and GPC, however, their absence do not rule out ocular allergy (Friedlaender, 2011).
7. Differential diagnosis
Mild conjunctival hyperaemia, itching and prominent che-mosis are the typical clinical presentation of ocular allergic conditions (Mantelli, Lambiase, & Bonini, 2009). Ocular allergies are usually associated with a watery discharge, which may contain mucus, making it mucoid in appearance, often leading to erroneous diagnoses of bacterial conjunctivitis (Sanchez et al., 2011). Whereas the symptom of itching is most closely associated with ocular allergy, some patients with blepharitis, dry eye, and irritative, nonallergic conjunctivitis also complain of itching (Bielory & Friedlaender, 2008). Itching that is localised in the conjunctiva and is consistent points to a diagnosis of allergic conjunctivitis. Patients who experience itching that is localised to the eyelids or the peri-orbital skin may have blepharitis, contact dermatitis, atopic eczema, or psoriasis (Bielory & Friedlaender, 2008).
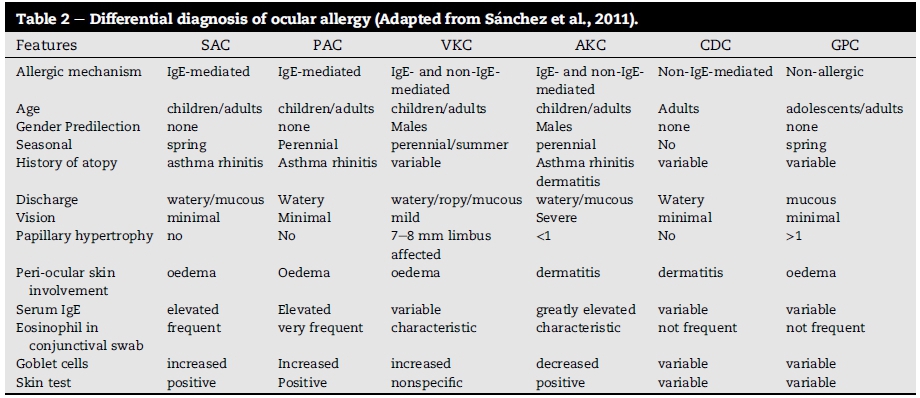
Clinicians need to remember the following: if it itches, it is allergy; if it burns, it is probably dry eye; if the eyelids are stuck together in the morning, it is bacterial infection. For example, ocular disorders such as VKC, AKC, CDC and GPC are due to allergy, while viral, bacterial, fungal and parasitic conjunctivitis are of infectious aetiology, and dry eye, episcleritis, scleritis, uveitis, pseudotumour and pemphigoid are due to autoimmune disorders (Mantelli et al., 2009). Similarly, the differential diagnosis of different types ocular allergy must be established (Table 2).
8. Treatment options
Ocular allergy is often misdiagnosed and overlooked because its clinical presentation is not specific, and some patients with dry eye, blepharitis, and irritative nonallergic conjunctivitis may also complain of similar signs and symptoms. In addition, there is usually a lack of concordance between bothersome ocular symptoms and clinical findings of ocular allergy on examination. Therefore, the clinical diagnosis of ocular allergy may be challenging and the approach to its management may require knowledge about the molecular mechanisms. An interdisciplinary medical group, including allergist/immunol-ogist, ear-nose-throat (ENT) specialists, ophthalmologists, optometrists, nurses and dermatologist need to work together to improve the ocular and systemic health of the allergic patient.
Mild forms of ocular allergy may require no treatment, particularly if asymptomatic. Treatment options for symptomatic ocular allergy include avoidance of the allergen, cold compressors, artificial tears, oral anti-allergies, vasocon-strictor/histamine eye drops, mast cell stabilisers eye drops, NSAIDS, corticosteroids and immunosupressives based on the severity of signs and symptoms (Chowdhury, 2013; La Rosa et al., 2013). Initial attempts at supportive treatment may need to be followed with medical options or surgery, if the patient finds no relief.
8.1. Supportive
Cold compresses, irrigation with saline solution or artificial tears may suffice to relieve mild symptoms of ocular allergy (Chowdhury, 2013; La Rosa et al., 2013). Artificial tear substitutes provide a barrier function and help to improve the first-line defence at the level of conjunctival mucosa by diluting and flushing various allergens and inflammatory mediators that maybe present on the ocular surface (Chowdhury, 2013; La Rosa et al., 2013). Goggles can be worn to decrease the amount of allergen reaching the ocular surface (Chowdhury, 2013).
8.2. Medical
The mainstay of treatment of ocular allergy is anti-allergic drugs, most of which are readily available. These include vasoconstrictors, antihistamines, mast cell stabilisers, dual mode action drugs, corticosteroids and immunosupressives (Leonardi, 2013), each of which will be reviewed.
8.2.1. Vasoconstrictors/antihistamines
Over-the-counter preparations that contain a vasoconstrictor (usually naphazoline hydrochloride) and an H1 antihistamine (usually antazoline or pheniramine) are useful for reducing conjunctival infection, usually providing symptomatic relief without significant side effects (Bielory & Friedlaender, 2008). While first-generation oral antihistamines may partially relieve ocular and nasal symptoms, they may also cause or exacerbate ocular surface dryness, which may impair the protective barrier provided by the ocular tear film (Bielory & Friedlaender, 2008). Combining topical antihistamines and vasoconstrictor may also be useful in the short-term treatment of mild allergic conjunctivitis (Bielory & Friedlaender, 2008). However, adverse effects include burning and stinging on instillation, mydriasis, and rebound hyperaemia or conjunctivitis medicamentosa with chronic use (Sanchez et al., 2011). Systemic antihistamines reduce tear production from the lacrimal glands and mucin secretion from the goblet cells (Sanchez et al., 2011) and should therefore never be used in the absence of systemic allergic disease, e.g. rhino-conjunctivitis (Sanchez et al., 2011).
8.2.2. Mast cell stabilisers
Mast cell stabilisers are available over-the-counter and by prescription (Leonardi et al., 2012), and are effective for treating mild to moderate allergic conjunctivitis. They have a slow onset of action, and prevent the release of histamines and other chemotactic factors from their storage sites around the eye (Sorkin & Waard, 1986). For example, sodium cromoglycate is more suitable for prophylactic and long-term treatment of chronic ocular allergies than for immediate symptom relief in acute seasonal conditions (Sorkin & Waard, 1986). N-acetyl-aspartyl glutamic acid, or spaglumic acid (NAAGA), is a mast cell membrane stabiliser, and acts by inhibiting leukotriene synthesis (Sánchez et al., 2011). Lodoxamide acts by inhibiting eosinophil activation and degranulation, has been shown to be more potent than sodium cromoglycate and NAAGA, and has fewer side effects (Sánchez et al., 2011).
8.2.3. Multiple action drugs
Several multi-modal anti-allergic agents have been introduced in recent years, and are becoming the drugs of choice for providing immediate symptomatic relief for patients with ocular allergy. For example, azelastine, bepostatine, epinas-tine, ketotifen and olopatadine exert multiple pharmacological effects such as histamine receptor antagonist, inhibiting eosinophil activation, mast-cell stabilising and anti-inflammatory effects (Leonardi, 2013). The agents are well tolerated and none are associated with significant ocular drying effects (Leonardi, 2013).
8.2.4. Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs (NSAIDS) can be a useful, short-term treatment option, relieving the pain associated with the allergic inflammatory process (Kari & Saari, 2010). Topical NSAIDS reduce the conjunctival hyperaemia and pruritus associated with allergy by interfering with the synthesis of prostaglandin and leukotrienes by inhibiting the cyclooxygenase enzymes (Kari & Saari, 2010). Ketorolac, diclofenac, indomethacin and pranoprofen have been shown to be effective against itching and conjunctival hyperaemia, and are valid alternatives to steroids (Kari & Saari, 2010). Ketorolac should not be used in asthmatic patients with NSAID intolerance as it has been reported to cause asthmatic crises in these patients (Kari & Saari, 2010).
8.2.5. Corticosteroids
For severe allergic conjunctivitis, low-dose corticosteroids eye drops such as luorometholone and loleprednol, which are more potent than mast cell stabilisers, are preferred (Sánchez et al., 2011). 'Corticosteroids possess immunosuppressive and anti-proliferative properties as they hinder the transcription factor that regulates the transcription of Th2-derived cytokine genes and differentiates activated T-lymphocytes into Th2-lympho-cytes' (La Rosa et al., 2013). Patients receiving corticosteroids eye drops for longer durations should be closely monitored for glaucoma and cataracts (Leonardi, 2013; Sánchez et al., 2011). Other adverse effects of corticosteroids include delayed wound healing and secondary infections (Leonardi, 2013; Sánchez et al., 2011). Intranasal corticosteroids have been reported to be effective for treating nasal symptoms of allergic rhinitis, but their effectiveness for addressing ocular symptoms is inconsistent (Sanchez et al., 2011). As with topical corticosteroids, the use of intranasal corticosteroids has been associated with elevated intraocular pressure and glaucoma damage (Bergmann, Witmer, & Slonim, 2009). Severe cases of ocular allergy that do not respond to any of these topical therapies may require short-term treatment with systemic corticoste-roids (e.g. prednisone 1 mg/kg per day) (Leonardi, 2013).
8.2.6. lmmunosupressives
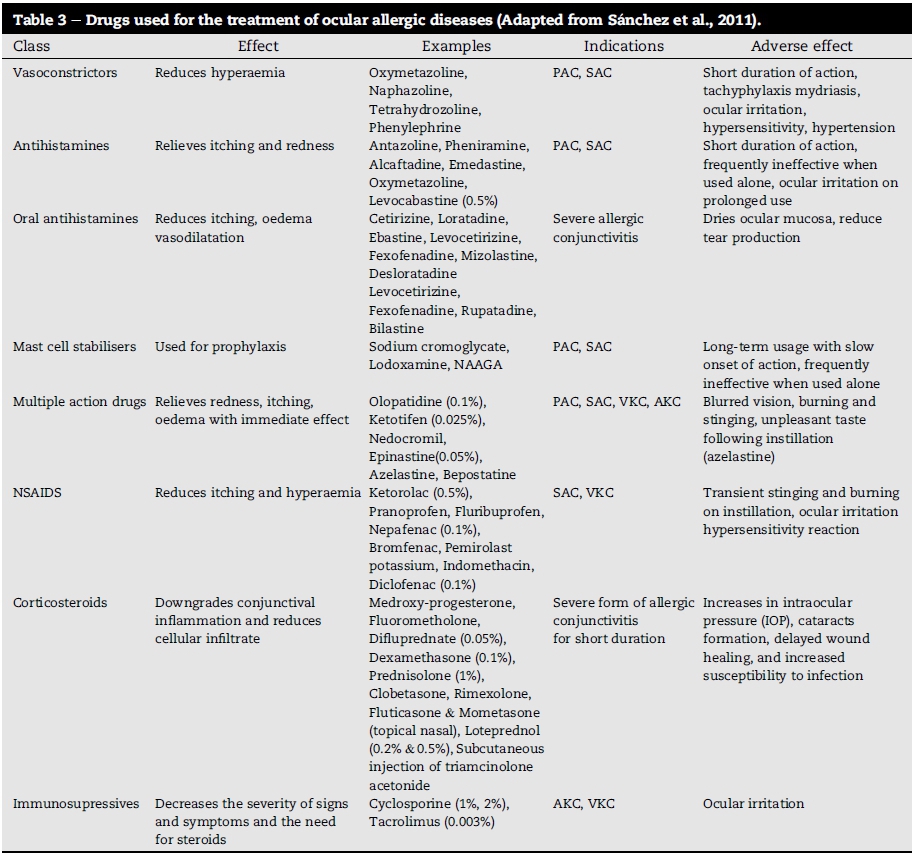
Allergen-specific immunotherapy is an effective treatment in patients with allergic rhinoconjunctivitis who have IgE antibodies to allergens, with cyclosporine and tacrolimus being used in severe cases of VKC and AKC (Leonardi et al., 2012). Cyclosporine inhibits eosinophil infiltration by affecting type IV hypersensitivity, and tacrolimus inhibits the action of T-lymphocytes (Broide, 2009). Cyclosporine and tacrolimus are useful in steroid resistant cases, with no significant side effects, except for a burning sensation during administration having been reported (Utine, Stern, & Akpek, 2010). While immunotherapy is delivered via subcutaneous injection and sublingual (oral) route, ocular symptoms respond less well than nasal symptoms to sublingual route (La Rosa et al., 2011). Oral cyclosporines are however ineffective in treating ocular allergies (Utine et al., 2010). The drugs, their effects, indications and adverse effects used in various types of ocular allergy treatment are summarised in Table 3.
8.3. Surgical
When medical treatment remains ineffective and visual function deteriorates, such as in severe cases of AKC and VKC, surgical treatment should be considered. Procedures such as excision, cryocoagulation, excision with Mitomycin-C 0.02% or CO2 laser are used to manage papillary hypertrophy (Tanaka et al., 2004). Non-healing shield ulcers associated with VKC are best managed by debriding the ulcer base, or using excimer laser keratectomy or amniotic membrane graft/free autolo-gous conjunctival graft, while in cases of mechanical ptosis, tarsal plate resection is recommended (Tanaka et al., 2004).
9. Conclusion
Although the systematic review retrieved 5200 studies, only 6 met the inclusion criteria (Appendices 1A and 1B). The classification, nomenclature and epidemiology of ocular allergy have not yet been adequately defined and require further investigations. The clinical diagnosis of this condition is challenging due to a wide range of overlapping and comorbid entities that might respond differently to conventional therapy. Supporting patients with severe ocular allergy requires adequate knowledge of the molecular mechanisms involved, the use of novel treatments and the involvement of an interdisciplinary treatment group. This will eventually help in completely understanding, treating and controlling symptoms of severe forms of ocular allergy.
Author's contribution
Khathutshelo Percy Mashige is solely responsible for writing this review article.
REFERENCES
Abelson, M. B., Smith, L., & Chapin, M. (2003). Ocular allergic disease: Mechanisms, disease sub-types, treatment. The Ocular Surface, 1, 127-149. [ Links ]
Abokyi, S., Koffuor, G. A., Ntodie, M., Kyei, S., & Gyanfosu, L. (2012). Epidemiological profile and pharmacological management of allergic conjunctivitis: A study in Ghana. International Journal of Pharmaceutical and Biomedical Research, 3, 195-201. [ Links ]
Bergmann, J., Witmer, M. T., & Slonim, C. B. (2009). The relationship of intranasal steroids to intraocular pressure. Current Allergy and Asthma Reports, 9, 311-315. [ Links ]
Bielory, L. (2000). Allergic and immunologic disorders of the eye. Part II: Ocular allergy. Current Reviews ofAllergy and Clinical Immunology, 106, 1019-1032. [ Links ]
Bielory, L., & Friedlaender, M. H. (2008). Allergic conjunctivitis. Immunology and Allergy Clinics ofNorth America, 28,43-58. [ Links ]
Bonini, S. (2006). Allergic conjunctivitis: The forgotten disease. Chemical Immunology and Allergy, 91, 110-120. [ Links ]
Broide, D. H. (2009). Immunomodulation of allergic disease. Annual Review of Medicine, 60(1), 279-291. [ Links ]
Campbell, D. E., & Mehr, S. (2015). Fifty years of allergy: 1965-2015. Journal of Paediatrics and Child Health, 51,91-93. [ Links ]
Chowdhury, B. (2013). Allergic conjunctivitis - A review. Dehli Ophthalmogical Society Times, 19,41-47. [ Links ]
Critical Appraisal Skills Programme (CASP). (2014). Making sense of evidence. Available from: http://www.casp-uk.net Accessed: 20.05.14. [ Links ]
Forister, J. F., Forister, E. F., Yeung, K. K., Ye, P., Chung, M. Y., Tsui, A., et al. (2009). Prevalence of contact lens-related complications: UCLA contact lens study. Eye Contact Lens, 35, 176-180. [ Links ]
Friedlaender, M. H. (2011). Ocular allergy. Current Opinion in Allergy and Clinical Immunology, 11, 477-482. [ Links ]
Hesselmar, B., Aberg, B., Eriksson, B., & Arberg, N. (2001). Allergic rhinoconjunctivitis, eczema, and sensitization in two areas with differing climates. Pediatric Allergy and Immunology, 12, 208-215. [ Links ]
Ibanez, M. D., & Garde, J. M. (2009). Allergy in patients under fourteen years of age in Alergologica 2005. Journal of Investigational Allergology and Clinical Immunology, 19,61-68. [ Links ]
Johansson, S. G., Bieber, T., Dahl, R., Friedmann, P. S., Lanier, B. Q.., Lockey, R. F., et al. (2004). Revised nomenclature for allergy for global use: Report of the nomenclature review committee of the World Allergy Organization, October 2003. Journal ofAllergy and Clinical Immunology, 113, 832-836. [ Links ]
Johansson, S. G., Hourihane, J. O., Bousquet, J., Bruijnzeel- Koomen, C., Dreborg, S., Haahtela, T., et al. (2001). A revised nomenclature for allergy. An EAACI position statement from EAACI nomenclature task force. Allergy, 56, 813-824. [ Links ]
Kari, O., & Saari, K. M. (2010). Updates in the treatment of ocular allergies. Journal of Asthma and Allergy, 24, 149-158. [ Links ]
La Rosa, M., Lionetti, E., Leonardi, S., Salpietro, A., Bianchi, L., Salpietro, C., et al. (2011). Specific immunotherapy in children: The evidence. International Journal ofImmunopathology and Pharmacology, 24,68-78. [ Links ]
La Rosa, M., Lionetti, E., Reibaldi, M., Russo, A., Longo, A., Leonardi, S., et al. (2013). Allergic conjunctivitis: A comprehensive review of the literature. Italian Journal of Pediatrics, 39, 18. http://dx.doi.org/10.1186/1824-7288-39-18. [ Links ]
Lambiase, A., Minchioti, S., Leonardi, A., Secchi, A. G., Rolando, M., Calabria, G., et al. (2009). Prospective, multicenter demographic and epidemiological study on vernal keratoconjunctivitis: A glimpse of ocular surface in Italian population. Ophthalmic Epidemiology, 16,38-41. [ Links ]
Leonardi, A. (2013). Management of vernal keratoconjunctivitis. Ophthalmology and Therapy, 2,73-88. [ Links ]
Leonardi, A., Bogacka, E., Fauquert, J. L., Kowalski, M. L., Groblewska, A., Jedrzejczak-Czechowicz, M., et al. (2012). Ocular allergy: Recognizing and diagnosing hypersensitivity disorders of the ocular surface. Allergy, 67, 1327-1337. [ Links ]
Leonardi, A., De Dominicis, C., & Motterle, L. (2007). Immunopathogenesis of ocular allergy: A systemic approach to different clinical entities. Current Opinion in Allergy and Clinical Immunology, 7, 429-435. [ Links ]
Malu, K. N. (2014). Allergic conjunctivitis in Jos-Nigeria. Nigerian Medical Journal, 55, 166-170. [ Links ]
Mantelli, F., Lambiase, A., & Bonini, S. (2009). A simple and rapid diagnostic algorithm for the detection of ocular allergic diseases. Current Opinion in Allergy and Clinical Immunology, 9, 471-476. [ Links ]
Niederkom, J. Y., Chen, P. W., Mellon, J., Stevens, C., & Mayhew, E. (2010). Allergic conjunctivitis exacerbates corneal allograft rejection by activating Th1 and Th2 alloimmune responses. Journal of Immunology, 184, 6076-6083. [ Links ]
Pitt, A. D., Smith, A. F., Lindsell, L., Voon, L. W., Rose, P. W., & Bron, A. J. (2004). Economic and quality-of-life impact of seasonal allergic conjunctivitis in Oxfordshire. Ophthalmic Epidemiology, 11,17-33. [ Links ]
Riedi, C. A., & Rosario, N. A. (2010). Prevalence of allergic conjunctivitis: A missed opportunity? Allergy, 65, 131-132. [ Links ]
Sánchez, M. C., Fernández Parra, B., Matheu, V., Navarro, A., Ibanez, M. D., Dávila, I., et al. (2011). Allergic conjunctivitis. Journal of Investigational Allergology and Clinical Immunology, 21,1-19. [ Links ]
Schmid, K. I., & Schmid, L. M. (2000). Ocular Allergy: Causes and therapeutic options. Clinical and Experimental Optometry, 83, 257-270. [ Links ]
Smith, A. F., Pitt, A. D., Rodriguez, A. E., Alio, J. L., Marti, N., Teus, M., et al. (2005). The economic and quality of life impact of seasonal allergic conjunctivitis in a Spanish setting. Ophthalmic Epidemiology, 12, 233-242. [ Links ]
Sorkin, E. M., & Waard, A. (1986). Ocular sodium cromoglycate. An overview of its therapeutic efficacy in allergic eye disease. Drugs, 31, 131-148. [ Links ]
Takano, Y., Narita, S., & Kobayashi, K. (2004). Seasonal allergic rhinitis in Hakodote. Nippon Ganka Gakkai Zasshi, 108, 606-611. [ Links ]
Tanaka, M., Takano, Y., Dogru, M., Fukagawa, K., Asano-Kato, N., Tsubota, K., et al. (2004). A comparative evaluation of the efficacy of intraoperative mitomycin C use after the excision of cobblestone like papillae in severe atopic and vernal keratoconjunctivitis. Cornea, 23, 326-329. [ Links ]
Utine, C. T., Stern, M., & Akpek, E. K. (2010). Clinical review: Topical ophthalmic use of cyclosporin A. Ocular Immunology and Inflammation, 18, 352-361. [ Links ]
Visser, L. (2013). HIV and the eye. Continuing Medical Education, 31, 143-146. [ Links ]
Wade, P. D., Iwuora, A. N., & Lopez, L. (2012). Allergic conjunctivitis at Sheikh Zayed regional eye care center, Gambia. Journal of Ophthalmic and Vision Research, 7,24-28. [ Links ]
Received 30 January 2015
Accepted 13 July 2016
E-mail address: mashigek@ukzn.ac.za
Peer review under responsibility of Johannesburg University.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.hsag.2016.07.001.
Appendix 1A. Flow diagram showing the selection process for inclusion of studies
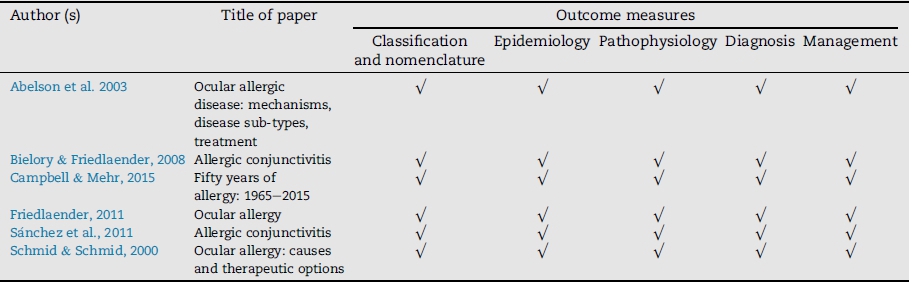
Appendix 1B. A summary of included papers and outcome measures


{kind=link}
{kind=link}
{kind=link}