










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkHealth SA Gesondheid (Online)
On-line version ISSN 2071-9736
Print version ISSN 1025-9848
Health SA Gesondheid (Online) vol.22 Cape Town 2017
http://dx.doi.org/10.1016/j.hsag.2016.09.0061025-9848
SPECIAL EDITION 2016
The quality of life of HIV-infected and non-infected women post-caesarean section delivery
Preshani ReddyI, *; José Merle FrantzII
ICollege of Health Sciences, University of KwaZulu-Natal, Westuille Campus, Faculty of Health Science, South Africa
IIFaculty of Community and Health Science, University of the Western Cape, South Africa
ABSTRACT
There is a dearth of literature on the postnatal quality of life (QoL) of women. This study aimed to determine to QoL of HIV-infected and non-infected women post-caesarean section delivery.
This prospective, longitudinal and comparative study was conducted at four public hospitals in KwaZulu-Natal. The participants were followed for six-months post-delivery and the QoL was measured using the SF-36 and the pelvic floor impact questionnaire (PFIQ-7).
The results showed that the QoL of women were negatively affected post-operatively with the HIV-infected group scoring lower over the six-months.
Understanding postpartum QoL problems is essential in efforts to provide effective comprehensive care.
Keywords: Quality of life HIV, Caesarean section delivery, Postnatal
1. Introduction
Improving the quality of health care particularly in the field of women's health, has become an urgent global priority (Hassim, Heywood, & Berger, 2007; UN, 2013). Focussing on the health of women is seen as an investment in present and future generations (WHO, 2009). This highlights the need for health programmes that are tailored specifically to cater for women throughout their lifespan (WHO, 2009). While research is required in many areas of women's health the rate of caesarean section delivery (CSD) is steadily increasing in South Africa (Massyn et al. 2014) and is currently the most common procedure perform by obstetricians. The long-term impact of this procedure a women's quality of life (QoL) in the HIV and non-HIV infected population therefore necessitates understanding.
The national CSD rate in South Africa has steadily increased over the past decade from 12.7% in 2001/02 to 20.8% in 2012/13 (Massyn et al. 2013) and at present accounts for 24.4% of all births (Massyn et al. 2014). This figure is the highest in Africa (Betrán et al. 2007). Nationally, the KwaZulu-Natal Province (KZN) recorded the highest CSD rate of 27.7% (Massyn et al. 2014). Although various postoperative complications have been identified, most of the related research is internationally based (Belfort et al. 2010; Jamieson et al. 2007; Koroukian, 2004) with postpartum quality of life (QoL) not being well understood, as studies have focused on serious morbidities and preventing maternal mortality (Bekinska, Kunene, & Mullick, 2006; Moodliar, Moodley, & Esterhuizen, 2007). In addition, there is no national research on the QoL of HIV-infected women post-CSD despite South Africa having the highest HIV prevalence rate globally and KZN being the epicentre of the virus (South African Department of Health, 2011). However, research in this area is a priority because improving the quality of health care in South Africa is presently of significance, and forms part of the country's 2030 national developmental plan (National Planning Commission, 2011).
The history of South Africa has had a profound effect on the health care policy and services of the present day, and despite the progress made, the country is still struggling to promote equitable health care (Coovadia, Jewkes, Barron, Sanders, & McIntyre, 2009; Pillay & Skordis-Worrall, 2013). Low staff morale, a higher burden of disease linked to HIV/ AIDS, and weak health systems management have resulted in the erosion of the health care system (Harrison, 2009). In terms of women's health, enhancing antenatal and postnatal care is part of the goals stipulated in the national developmental plan with improving the quality of health care as a strategy to achieve this (National Planning Commission, 2011). Improving the quality of health care will promote efficient use of resources by preventing many of the morbidities that generate a demand for services, thus reducing the present strain on the health care system. Specific suggestions to improve the quality of health care in South Africa are highlighted in the Quality in Health Care policy, with research and dissemination of research specific to South African needs forming the core (South African Department of Health, 2007).
In terms of postnatal care, there have been no recent South African studies detailing the current situation or the post-partum QoL of HIV-infected and non-infected women, despite literature having previously noted that postnatal care has not been adequately prioritised in the maternal health care service (Bekinska et al., 2006). The postpartum maternal services tend to be task-orientated rather than patient-orientated, resulting in impersonal and incomplete patient care (Bekinska et al., 2006). In terms of HIV-infected women, the interaction between pregnancy, the pathophysiology of the virus, and social determinants, may influence the patients' QoL (Larrabee, Monga, Eriksen, & Helfgott, 1996). Research in this area is therefore essential in order to improve the quality of health care in the country.
1.1. Problem statement
The South African CSD rate is presently considered high and still steadily increasing (Massyn et al. 2014). Despite the high rate there is currently no national research available on the postpartum QoL and factors contributing to QoL in women post-CSD in HIV-infected and non-infected women. Understanding and addressing QoL issues are important in providing patients with comprehensive postpartum health care.
1.2. Aim of the study
To determine to QoL of HIV-infected and non-infected women post-caesarean section delivery.
1.3. Significance of the work
Because of past gender inequalities, the area of women's health has been neglected, resulting in national and international efforts to improve the quality of health care services offered to women (Hassim et al. 2007; UN 2013). South Africa is a developing country, and an increased use of public sector health services (Cooper et al. 2004) coupled with a lack of human and financial resources, especially in the rural areas of South Africa, has resulted in inadequate service delivery (Cooper et al. 2004). This has negatively affected the quality of care offered to patients. Many women live in informal settlements and/or rural areas with limited access to health care facilities, which can be attributed to financial and/or social constraints. In addition, women from disadvantaged backgrounds are also not properly educated about health conditions, and may not perceive a health problem until it is too late or requires intensive therapy. The information generated from this study will provide insight into the QoL of patients post-CSD. This information will assist health care professionals in identifying the affected areas of both HIV-infected and non-infected patients post-partum, which can subsequently be improved to provide the patient with comprehensive health care. In the South African context, this may assist in preventing complications thus reducing the number of additional out-patient post-surgical follow-up patient visits. This will inevitably save the patient time and money, and reduce the strain on the health system. Furthermore, it will add to the dearth of literature in this area.
2. Study design and research methods
The study was prospective, longitudinal, comparative and descriptive in nature. It was conducted at four public hospitals in KwaZulu-Natal. The sample size was calculated using a confidence level of 95% and ±5% precision by a qualified statistician. The calculation was based on an article by Watson (2001) using the caesarean section surgery numbers over a six-month period at the respective hospitals. Stratification of the population into HIV-infected and HIV non-infected groups was done prior to calculation by the researcher, based on anecdotal information from the relevant consultants.
Purposive probability sampling was used to select potential participants following which participants were scrutinized to ensure that they met the inclusion criteria of the study (Table 1). The participants selected were then stratified into HIV-infected (n = 155) and HIV non-infected (n = 155) groups. The participants (N = 310) were followed for six months post-delivery, and the QoL was measured using the SF-36 health survey and the pelvic floor impact questionnaire (PFIQ-7) at baseline, one, three and six months.
![]()
The SF 36 health questionnaire consists of eight multi-item scales (35 likert scale questions) that are collated and summarized into two measures: the Physical (PCS) and Mental (MCS) Component Summary scores (Ware, Snow, Kosinski, & Gandek, 1993). The eight scales are designed to address the following areas (Ware et al. 1993): assessing physical function (10 items), role limitations due to physical health problems (4 items), bodily pain (2 items), general health (5 items), vitality (4 items), social functioning (2 items), role limitations due to emotional problems (3 items) and emotional well-being (5 items). The questionnaire is a reliable and valid tool and has been translated in more than 40 countries, which included South Africa (English and isiZulu) (Ware, 2000). The reliability of the questionnaire was determined using both internal consistency and the test-retest methods with a reliability coefficient range of 0.70-0.90 the questionnaire is considered a reliable tool (Ware, 2000). Additionally, the questionnaire was deemed valid with studies having yielded content, concurrent, criterion, construct and predictive evidence of validity (Ware, 2000). This is a condition specific tool that was developed to evaluate the QoL of women with all forms of pelvic floor disorders (Barber, Walters, & Bump, 2005). The questionnaire is a valid and reliable tool (Barber et al. 2005). The test-retest reliability had a correlation coefficient range of 0.70-0.93 and in terms of validity, the scales "demonstrated significant association with appropriate measures of symptom severity and pelvic floor diagnoses, thereby demonstrating construct validity" (Barber et al. 2005). The questionnaire consists of the following three scales with seven Likert scale items namely: urinary impact questionnaire, colorectal-impact questionnaire and pelvic organ prolapse impact questionnaire. The questionnaire was translated into isiZulu using forward and back translation by two qualified independent translators.
Descriptive (mean) and inferential statistics (Pearson chi-square test) were used to summarise the results and determine the relationship between categorical variables respectively. The generalised estimating equation (GEE) for longitudinal data (Zeger & Liang, 1986) was used to determine the effect of the explanatory variables on the response variables used during data analysis.
2.1. Ethical considerations
Ethical clearance was granted by the Senate Research Committee of the University of the Western Cape. Approval to conduct the study was then granted from the KZN Department of Health, following which, the relevant hospitals were provided with a copy of both approval letters. Each participant was given an information sheet in a language of their preference, and they signed a consent form prior to participation. They were informed that they could withdraw from the study at any time. Data was collected, coded and stored on a password-protected personal computer with the questionnaires in a secure cabinet.
3. Results
A total of 310 participants (HIV-infected n = 155, HIV non-infected n = 155) were evaluated at baseline level. The overall attrition rate was 9 participants (2.9%; Fig. 1).
![]()
The ages of the participants ranged from 18 to 43 years, with a mean age of 26.49 years (SD ± 5.52). There were no significant differences (p = 0.069) between the mean ages of the HIV-infected and non-infected group. The mean number of children the participating mothers (N = 310) had, was 3.01 (SD ± 0.96). The majority (n = 303; 98%) of participants had undergone previous CSDs, with over half (n = 165; 53.2%) being emergency CSDs. However, there was no significant statistical difference (p = 0.56) between the HIV-infected and non-infected participants and the type of CSD.
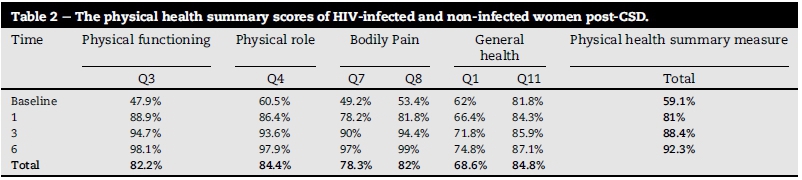
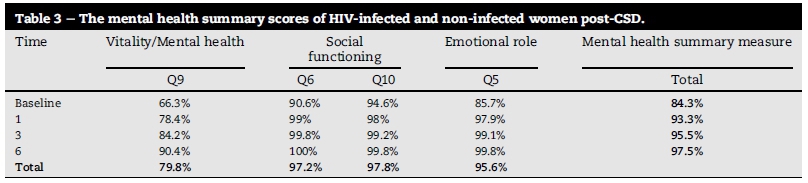
The results showed that the QoL of all the participants improved over the six-month time period (Table 2 and Table 3) irrespective of their HIV status. However, there was a substantial difference between the scores, with lower scores in the physical health summary measure (Table 2) than the mental health summary measure (Table 3) over this time period.
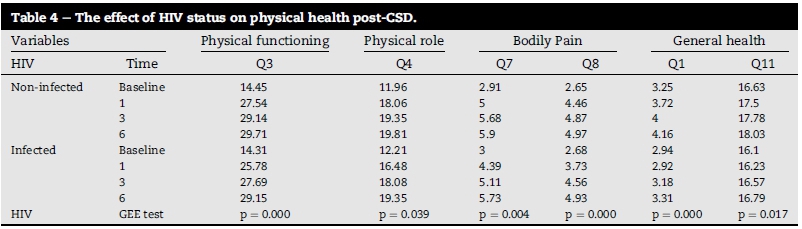
In terms of HIV status, the results in indicate that there was a statistically significant difference in score in all the physical health scales between the two groups, with the HIV-infected participants scoring significantly lower (Table 4).
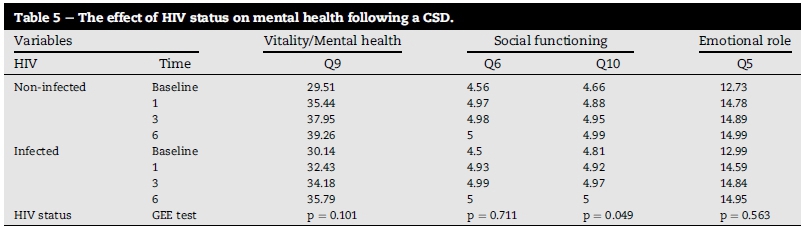
The only statistically significant difference noted in the mental health category was for question 10 (p = 0.49) in the social functioning scale, with the HIV-infected group scoring slightly higher than the non-infected group (Table 5).
The results showed no significant difference between the HIV non-infected and the HIV-infected group (p = 0.881) in terms of the reported health transition.
In the PFIQ-7, participants who experienced urinary incontinence (UI) post-CSD scored significantly lower (p = 0.000) in the six-month time period than those who did not experience UI post-CSD. However, an improvement from months one to six in the bladder/urine section was noted. The overall scores were 84% in month one, 91.8% in month three, and 96.3% in month six. In the bowel/rectum section, the results show that all participants had a score of 100% (maximum value = 28) over the three time points. A significant difference was only noted in the bladder/urine section of the HIV groups, with the mean of the HIV non-infected group being greater than that of the HIV-infected group (p = 0.000).
4. Discussion
The results of this study showed that despite the QoL improving over the various time-points, participants still experienced physical health problems thatnegativelyaffected their QoL. The results also suggest that the physical health of the participants was more affected than the mental health, with HIV-infected women scoring significantly lower in all the subsets of the physical health category. A woman's body undergoes endocrine changes following childbirth (Huang, Tao, Liu, & Wu, 2012), and coupled with a compromised immune system, this could be the reason that HIV-infected women scored lower. The public health care system is also mainly used by South Africa's lower income group, which implies that social determinants may also be influencing factors on the patients' postnatal QoL, specifically the physical aspect. The results were similar to other findings, which demonstrated that women had better improvements in the mental health section of the SF36 health questionnaire post-CSD (Jansen et al. 2007; Torkan, Parsay, Lamyian, Kazemnejad, & Montazeri, 2009), but the participants in these studies were HIV non-infected. An interesting result from the social functioning question in the mental health sub-section, was that HIV-infected women scored higher than the non-infected group. A similar study by Larrabee et al. (1996) in Houston, Texas comparing HIV-infected and non-infected women, showed worse social and cognitive functioning among HIV-infected women. The authors stated that the decreased societal functioning might be due to cultural and social reactions to the virus (Larrabee et al. 1996). Despite the stigma associated with HIV still being rife in South Africa (Gilbert & Walker, 2010), a decrease has been noted (Mall, Middelkoop, Mark, Wood, & Bekker, 2013). The improved social interaction could be due to an increase in knowledge about the virus, resulting from South Africans being more exposed to HIV due to the high prevalence rates (Mall et al. 2013) and therefore socially aware of HIV.
Another interesting finding in this study was the negative effect UI has on a women's QoL post-partum. Urinary incontinence is not viewed as a life-threating disease, which could be the reason for research into the effects of UI on the QoL of women only commencing about 15 years ago (Segedi, Segedi, & llić, 2011). The reality is that UI has a serious psychological affect on women, and leads to social seclusion and economic burden (Herzog, Diokno, Brown, Fultz, & Goldstein, 1994; Segedi et al. 2011). The QoL of participants who complained of UI post-CSD was negatively affected, which is similar to another study in this area (Handa et al. 2007). This, coupled with other postoperative complications as well as a baby, can be extremely stressful for a woman postpartum, especially if she does not understand what is happening to her body. The results also showed that HIV-infected women were more impaired in terms of the QoL. This could be because HIV-infected women who are already socially excluded by social stigma (Gilbert & Walker, 2010) now have to cope with UI, which can be embarrassing. However, UI can be avoided or corrected, because effective treatments are available (Handa et al. 2007; Mantle, Haslam & Barton 2004). Health care professionals caring for postpartum patients should therefore screen them in order to identify UI at follow-up visits (Handa et al. 2007).
5. Conclusion
Understanding the QoL of women postpartum will assist in guiding the development of post-natal care programmes to improve the quality of care, which is a goal that has been highlighted in various South African government documents (National Planning Commission, 2011). The results from this study suggest that to improve postpartum QoL, educational programmes need to be centred on physical health problems, and UI with a referral system in place if the patient requires it. These programmes should target all women with special attention on HIV-infected women.
6. Limitations of the study
The following limitations are noted with respect to the study:
1. The questionnaire(s) relied on the participants' ability to recall information, which they may not always have been able to do. .
2. Participants could have answered the questions based on what they considered to be socially or scientifically acceptable, rather than based on what they were experiencing.
3. Caution should be taken in generalising the results of the study to HIV-infected women and HIV non-infected women following a caesarean section in KwaZulu-Natal.
Authors' contributions
Dr Preshani Reddy (University of KwaZulu-Natal) is the researcher and wrote the manuscript, which was part of her PhD. Professor Jose Frantz (University of the Western Cape) was her supervisor and facilitated the process.
REFERENCES
Barber, M. D., Walters, M. D., & Bump, R. C. (2005). Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7). American Journal ofObstetrics and Gynecology, 193(1), 103-113. [ Links ]
Bekinska, M., Kunene, B., & Mullick, S. (2006). Maternal care: Antenatal, peri and postnatal. In P. Ijumba, & A. Padarath (Eds.), South African health review 2006 (pp. 297-314). Durban: Health Systems Trust. [ Links ]
Belfort, M., Clark, S., Saade, G., Kleja, K., Dildy, G. A., III, van Veen, T. R., et al. (2010). Hospital readmission after delivery: Evidence for an increased incidence of non-urogenital infection in the immediate postpartum period. American Journal of Obstetrics and Gynecology, 202(1), 35.e1-e7. [ Links ]
Betrán, A. P., Merialdi, M., Lauer, J. A., Bing-shun, W., Thomas, J., Look, P. V., et al. (2007). Rates of cesarean section: Analysis of global, regional and national estimates. Paediatric and Perinatal Epidemiology, 21(2), 98-113. [ Links ]
Cooper, D., Morroni, C., Phyllis, O., Moodley, J., Harries, J., Cullingworth, L., et al. (2004). Ten years of democracy in South Africa: Documenting transformation in reproductive health policy and status. Reproductive Health Matters, 12(24), 70-85. [ Links ]
Coovadia, H., Jewkes, R., Barron, P., Sanders, D., & McIntyre, D. (2009). The health and health system of South Africa: Historical roots of current public health challenges. Lancet, 374(9692), 817-834. [ Links ]
Gilbert, L., & Walker, L. (2010). My biggest fear was that people would reject me once they knew my status...": Stigma as experienced by patients in an HIV/AIDS clinic in Johannesburg, South Africa. Health & Social Care in the Community, 18(2), 139-146. [ Links ]
Handa, V. L., Zyczynski, H. M., Burgio, K. L., Fitzgerald, M. P., Borello-France, D., Janz, N. K., et al. (2007). The impact of fecal and urinary incontinence on quality of life 6 months after childbirth. American Journal of Obstetrics and Gynecology, 197(6), 636-636. [ Links ]
Harrison, D. (2009). An overview ofhealth and health care in South Africa 1994 - 2010: Priorities, progress and prospects for New Gains, Muldersdrift, South Africa. [ Links ]
Hassim, A., Heywood, M., & Berger, J. (2007). Health & democracy. Cape Town: Siber Ink. [ Links ]
Herzog, A. R., Diokno, A. C., Brown, M. B., Fultz, N. H., & Goldstein, N. E. (1994). Urinary incontinence as a risk factor for mortality. Journal ofthe American Geriatrics Society, 42(3), 264-268. [ Links ]
Huang, K., Tao, F., Liu, L., & Wu, X. (2012). Does delivery mode affect women's postpartum quality of life in rural China? Journal ofclinical nursing, 21(11-12), 1534-1543. [ Links ]
Jamieson, D. J., Read, J. S., Kourtis, A. P., Durant, T. M., Lampe, M. A., & Dominguez, K. L. (2007). Cesarean delivery for HIV-infected women: Recommendations and controversies. American Journal ofObstetrics and Gynecology, 197(S3), s96-s100. [ Links ]
Jansen, G. A. J., Duvekot, J. J., Hop, J. W. C., Essink-Bot, M.-L., Beckers, E. A. M., Karsdorp, V. H. M., et al. (2007). New insights into fatigue and health-related quality of life after delivery. Acta Obstetricia et Gynecologica, 86(5), 579-584. [ Links ]
Koroukian, S. M. (2004). Relative risk of postpartum complications in the Ohio medic-aid population: Vaginal versus cesarean delivery. Medical Care Research and Review, 61(2), 203-224. [ Links ]
Larrabee, K. D., Monga, M., Eriksen, N., & Helfgott, A. (1996). Quality of life assessment in pregnant women with the human immunodeficiency virus. Obstetrics & Gynecology, 88(6), 1016-1020. [ Links ]
Mall, S., Middelkoop, K., Mark, D., Wood, R., & Bekker, L. G. (2013). Changing patterns in HIV/AIDS stigma and uptake of voluntary counselling and testing services: The results of two consecutive community surveys conducted in the Western Cape, South Africa. AIDS Care, 25(2), 194-201. [ Links ]
Mantle, M., Haslam, J., & Barton, S. (Eds.). (2004). Physiotherapy in obstetrics and gynaecology. Britain: Butterworth-Heinemann. [ Links ]
Massyn, N., Day, C., Dombo, M., Barron, P., English, R., & Padarath, A. (Eds.). (2013). District health barometer 2012/13. Durban: Health Systems Trust. [ Links ]
Massyn, N., Day, C., Peer, N., Padarath, A., Barron, P., & English, R. (Eds.). (2014). District health barometer 2013/14. Durban: Health Systems Trust. [ Links ]
Moodliar, S., Moodley, J., & Esterhuizen, T. M. (2007). Complications associated with caesarean delivery in a setting with high HIV prevalence rates. European Journal of Obstetrics & Gynecology and Reproductive Biology, 131(2), 138-145. http://dx.doi.org/10.1016/j.ejogrb.2006.05.004. [ Links ]
National Planning Commission. (2011). Our future make it work: National development plan 2030. Pretoria: National Department of Health. [ Links ]
Pillay, T. D., & Skordis-Worrall, J. (2013). South African health financing reform 2000-2010: Understanding the agenda setting process. Health Policy (Amsterdam, Netherlands), 109(3), 321-331. [ Links ]
Segedi, L. M., Segedi, D., & Iliác, K. P. (2011). Quality of life in women with urinary incontinence. Medicinski Glasnik, 8(2), 237-242. [ Links ]
South African Department of Health. (2007). A policy on quality in health care for South Africa. Pretoria: National Department of Health. [ Links ]
South African Department of Health. (2011). The national antenatal sentinel HIV and syphilis prevalence survey. Pretoria: South African Department of Health. [ Links ]
Torkan, B., Parsay, S., Lamyian, M., Kazemnejad, A., & Montazeri, A. (2009). Postnatal Quality of Life in women after normal vaginal delivery and caesarean section. BioMed Central Pregnancy and Childbirth, 9(4), 1-7. [ Links ]
United Nations (UN). (2013). The millennium development goals report. New York: United Nations. [ Links ]
Ware, J. E. (2000). SF-36 health survey update. Spine, 25(24), 3130-3139. [ Links ]
Ware, J. E., Snow, K. K., Kosinski, M., & Gandek, B. (1993). SF-36 health survey manual and interpretation guide, New England Medical Center. Boston: The Health Institute. [ Links ]
Watson, J. (2001). How to determine a sample size: Tipsheet #60. University Park, PA: Penn State Cooperative Extension. viewed 24 May 2011, from http://ww.extention.psu.edu/evaluation./pdf/TS60.pdf. [ Links ]
World Health Organization. (2009). Women and health: today's evidence tomorrow's agenda. Geneva: WHO press. [ Links ]
Zeger, S. L., & Liang, K.-Y. (1986). Longitudinal data analysis for discrete and continuous outcomes. Biometrics, 42(1), 121-130. [ Links ]
Received 9 September 2015
Accepted 26 September 2016
* Corresponding author. E-mail address: shani.reddy@gmail.com (P. Reddy).


{kind=link}
{kind=link}
{kind=link}
{kind=link}