










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.22 Cape Town 2017
http://dx.doi.org/10.1016/j.hsag.2016.09.003
FULL LENGTH ARTICLE
Strengths of families to limit relapse in mentally ill family members
Tlhalefi T. TlhoweI; Emmerentia du PlessisI, *; Magdalene P. KoenII
ISchool of Nursing Science, North-West University, Potchefstroom Campus, Priuate Bag X 6001, Potchefstroom, 2520, South Africa
IISchool of Nursing Science, North-West University, Mafikeng Campus, Priuate Bag X 2046, Mmabatho, 2745, South Africa
ABSTRACT
BACKGROUND: Relapse prevention in mental health care is important. Utilising the strengths of families can be a valuable approach in relapse prevention. Studies on family strengths have been conducted but little has been done on the strengths of family members to help limit relapse in mental health care users. The purpose of this research was to explore and describe the strengths of family members in assisting mental health care users to limit relapses.
METHODS: A phenomenological design was followed. Purposive sampling was used and 15 family members of mental health care users who have not relapsed in the previous two years participated. Individual unstructured interviews were conducted. Data were analysed using thematic analysis.
RESULTS: Four main themes were identified, namely accepting the condition of the mental health care users, having faith, involving the mentally ill family members in daily activities and being aware of what aggravates the mentally ill family members.
CONCLUSIONS: Family members go through a process of acceptance and receive educational information and assistance from health professionals. In this process families discover and apply their strengths to limit relapses of mentally ill family members. It is important that family members caring for mentally ill family members are involved in their treatment from the onset, and that they are guided through a process of acceptance.
Keywords: Families mental health care users; Mentally ill family members; Resilience; Relapse; Strengths
1. Introduction
According to Berglund, Vahlne and Edman (2003), caring for mental health care users can be a burden to these families, while a lack of support by families can lead to mental health care users experiencing relapses. Relapse prevention is found to be important because it reduces the negative impact of mental illnesses on individuals, families and communities, and relapse prevention improves the quality of life of people with mental illnesses, enabling them to participate more fully in their work, leisure activities and relationships. Building the strengths of families can be a valuable approach to relapse prevention (Sittner, Hudson, & Defrain, 2007).
In such an approach, nurses help families define their visions and hopes for the future instead of looking at what factors contribute to family problems (Sittner et al., 2007). A study conducted by Sousa, Ribeiro and Rodrigues (2006) indicate that the incorporation of a strengths-centred approach into the practitioner's intervention can improve the lives of families with multiple problems such as caring for mental health care users. Asay and DeFrain (2012) confirm that all families have strengths, and mention that exploring how families use their strengths to their advantage can be a powerful strategy.
This article reports on research on the strengths of families to limite relapse in mentally ill family members.
1.1. Problem statement
Studies on family strengths have been conducted (Mokgothu, Du Plessis, & Koen, 2015) but little has been done on strengths of families to help limit relapse in mental health care users. Relapses in mental health care users have been noted as a major problem both nationally and internationally (Kazadi, Moosa, & Jeenah, 2008). This problem poses a very serious burden on families who provide care for such mental health care users. Families caring for mental health care users need support from health care practitioners to assist them to cope. One approach is to explore family strengths in order to improve the life of families as well as that of the mental health care users. Family strengths should thus be looked into to explore how families can be assisted to care for mental health care users and to limit relapses.
This research formed part of the RISE1 project (Koen & Du Plessis, 2011), which focuses on strengthening the resilience of health caregivers and risk groups, such as mental health care users and their families, by means of a multi-faceted approach. The following research question was relevant in this research: What are the strengths of families in assisting mental health care users to limit relapses?
1.2. Purpose of the research
The purpose of this research was to explore and describe the strengths of families in assisting mental health care users to limit relapses. This information contributed to the formulation of recommendations for psychiatric nurses to empower family members in limiting the relapse of mental health care users.
1.3. Definition of key concepts
1.3.1. Family strengths
According to Mace cited in Defrain and Stinnet (2003), family strengths are those relationship qualities that contribute to the emotional health and well-being of the family. Family strength qualities are; therefore, regarded as aspects such as commitment, appreciation and affection, positive communication, time together, a sense of spiritual well-being and the ability to cope with stress and crisis (Sittner et al., 2007). In this review family strengths refer to qualities of families with a mentally ill family member that helps them to limit relapse.
1.3.2. Relapses
Relapses are defined as the recurrence of symptoms of mental illnesses similar to those that have previously been experienced (The Free Dictionary, 2016). This research focussed on strengths of families that contribute to limiting relapse in mentally ill family members.
1.3.3. Mentally ill family members/mental health care users According to the Mental Health Care Act (17/2002) (South Africa, 2002), mental health care users are persons receiving care, treatment and rehabilitation services or using health services at health establishments aimed at enhancing the mental status of users. In this research the focus was on mental health care users living with and supported by their families.
2. Research design and methods
2.1. Research design
A phenomenological design (Laverty, 2003) was used in this research. This design was applicable, as this research focused on the strengths of families as they experienced these strengths in their unique context, namely being families of mentally ill persons, and the meaning these families attach to their strengths.
2.2. Research method
2.2.1. Population and sampling
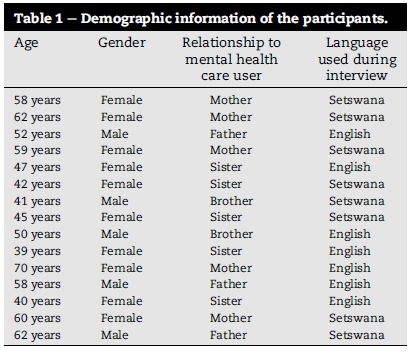
The population for this study was all families of mental health care users who received treatment at a particular mental health institution. Purposive sampling was used, using inclusion criteria, namely family members caring for mental health care users who gave consent to participate in the study. The focus was on mental health care users who have been following up at the outpatient department and who have not relapsed in the past two years. The sample for this research was identified via the register used in the mental health institution. Twenty five family members of such users were contacted telephonically to participate in the study. They were all given a chance to choose whether they want to be interviewed at home or at the mental health institution and they all chose to come to the mental health institution. From the 25 participants contacted telephonically, 15 came for interviews and gave voluntary consent. Table 1 contains the demographic information of the participants.
2.2.2. Data collection
The researcher obtained ethical clearance from the Ethics Committee of the North-West University. Thereafter permission was obtained from the North West Province Department of Health and the management of the mental health institution to conduct the study. Participants were recruited and interviewed after the researcher had received permission.
Data were collected by conducting unstructured interviews with family members using an open-ended question where participants were asked to verbally describe their strengths that contribute to limiting relapses. Such unstructured interviews was beneficial in this research as it allowed the researcher to conduct intensive conversations with the participants and to explore the phenomena in depth (Boyce & Neale, 2006). The open-ended question asked was: What do you think are your strengths in taking care of your mentally ill family member to limit a relapse? A trial run interview was conducted to determine whether the question was relevant and clear. Communication techniques, as described by Okun and Kantrowitz (2008), were used during the interviews. Field notes were documented immediately after each interview and included reflective, descriptive and demographic notes (Creswell, 2009). All the interviews conducted for the study were audio-recorded. The interviews were conducted in a private room at the mental health institution to ensure privacy and confidentiality.
The interviews were conducted in Setswana and English. Eight participants preferred to be interviewed in Setswana and seven in English. The interviews conducted in Setswana were translated into English by the researcher. The duration of interviews was 30-45 min. The researcher made use of field notes immediately after each interview. Data saturation was reached after 13 interviews, and a further two interviews confirmed data saturation.
2.2.3. Data analysis
The audio recorded interviews were transcribed for the data analysis process. Data were analysed according to the steps outlined by Tesch cited in Creswell (2007). A work protocol was given to the co-analyser who independently analysed the data. A consensus discussion followed to reach consensus on the themes that emerged from the data.
3. Trustworthiness
The goal of trustworthiness in qualitative research is to accurately represent the experiences of the participants of the study (Speziale & Carpenter, 2007). Trustworthiness was ensured by applying strategies to maintain credibility, dependability, conformability and transferability (Polit & Beck, 2010). Examples of these strategies applied are: conducting a trial run, conducting data collection until data saturation was reached, reflexivity through taking field notes, conducting a literature control and densely describing the research process and results in order to ensure an audit trail.
4. Ethical considerations
Ethical clearance was obtained from the North-West University (Reference NWU-00036-11-A1). Ethical principles, namely the principle of beneficence, respect for human dignity and justice (Polit & Beck, 2010) were applied. Beneficence was ensured by setting a conducive physical environment for data collection to make participants feel at ease and by explaining how the research might benefit them and the wider community, namely that the results obtained during the research study will be provided as recommendations to psychiatric nurses to assist other families in the same situation. Respect for human dignity was applied by giving participants detailed information on the research and obtaining informed consent. The principle of justice was applied through fair selection, conducting the interviews in a private room, and ensuring confidentiality. Confidentiality was ensured by not sharing any identifying information of the participants in the transcripts or any other reports, and data was protected by storing it on a password protected computer.
5. Findings and discussion
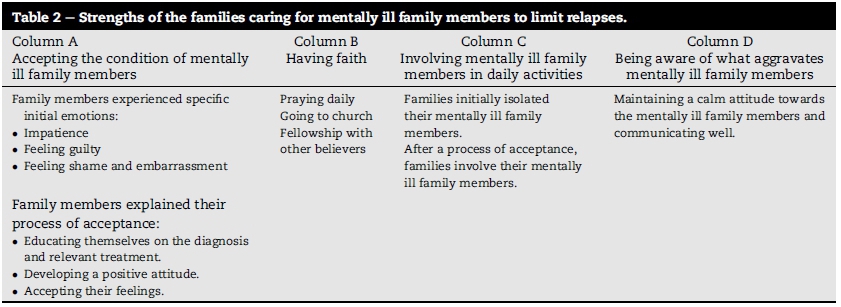
Four main themes were identified, as displayed in Table 2. Table 2 summarises the four main themes in Columns A, B, C and D with regard to what family members expressed as strengths to help them limit relapse in mentally ill family members. These themes as well as sub-themes are discussed in detail with direct relevant quotations from the transcripts to enrich the data. The discussion of the literature follows this directly and serves to confirm the findings.
5.1. Accepting the condition of the mentally ill family members
5.1.1. The family members experienced specific initial emotions
From the findings of this research it seems that family members experience specific emotions and difficulties when their mentally ill family members are diagnosed the first time with a mental illness. Similar results were found by Monyaluoe, Mokoena-Mvandaba, Du Plessis and Koen (2014), namely that families of mentally ill family members experience emotional pain, guilt and concern.
The following sub-themes were identified:
Being impatient: The family members who were interviewed, expressed their impatience towards the behaviour of their mentally ill family members. Most of them indicated that they thought that their mentally ill family members were just acting out when they displayed unusual behaviour. They only realised that their family members were ill when they started to become violent, fighting and destroying property. The following are examples of direct quotations from the transcriptions of interviews:
"I ignored him when he refused to bath and was locking himself in the room."
"I used to shout at him because I thought he is just naughty."
Literature confirms that at the onset of mental illness, family members may deny that the person has a continuing illness and during acute episodes, family members may be alarmed by what is happening to their loved one (Nichols, 2008). Croft (2008) also confirms that most people go through a phase of denial when faced with the diagnosis of a mental illness and this makes it difficult for them to cope.
Feeling guilty: The family members interviewed, indicated that they felt guilty because they thought that they contributed to the mental illness of their loved one. For example:
" I remember the days when my son used to lock himselfin his room but I just ignored him because I thought it is an adolescent stage."
" My sister used to listen a lot to a very loud music because she said there were people talking to her ears. I took her for granted because I did not understand that those were hallucinations."
These findings are confirmed by Tartakovsky (2011) who mentions that feeling guilty is a normal reaction. Some families may worry that they did not support their loved one into treatment sooner; others may think they caused the disorder. Another confirmation is that families wonder how the illness developed and they may feel that they might be responsible for their mentally ill family member's illness (Croft, 2008).
Feelings of shame and embarrassment: The families indicated how they would not tell their friends about their loved one's illness because stigmatisation of mental illnesses is a common occurrence. During the admission of mentally ill family members, they indicated that they would not even tell their colleagues at their work places because they felt embarrassed by the diagnosis. The following quotations confirm these findings:
" My sister was undressing in the street and this was really embarrassing, I could not even walk freely at the mall."
"I could not tell my fiance what was wrong with my younger brother because I was embarrassed."
" I changed my work place because everybody at work knew my sister before she became ill. She used to come to my office during school holidays when she was at university."
The feeling of embarrassment is closely related to stigma, which is defined as a sign of disgrace or discredit which sets a person apart from others (Byrne, 2000). Self-stigmatisation has been described in literature as similar to what was found in this research and there are numerous personal accounts of psychiatric illnesses, where shame overrides even the most extreme of symptoms (Byrne, 2000). The attitude of family members towards mental illnesses contributes to the feeling of shame and embarrassment and that can be difficult to overcome. They may feel that they cannot tell anyone about the condition of their mentally ill family members (Croft, 2008).
5.1.2. The families explained their process of acceptance
The family members expressed how they struggled to accept the condition of their mentally ill family members. They indicated that the more they struggled, the more their family members were also experiencing problems because they did not receive enough support from them and they ended up being admitted several times because they relapsed. Berglund et al. (2003) confirm that a lack of support by families can lead to the relapse of mentally ill family members. The families furthermore reported how they were concerned about their loved ones and how this concern prompted them to do something about what they were going through. This finding is similar to the finding by Monyaluoe et al. (2014) as well as Mokgothu et al. (2015) who also found that families of mentally ill family members undergo a process of acceptance.
The following sub-themes were identified:
Educating themselves on the diagnosis and relevant treatment: The families who were interviewed, mentioned that they decided to seek information on the condition of their loved ones in order to understand how to behave towards them. Most of them indicated that they started asking the doctor who was treating their family members to explain the diagnosis and the treatment in detail. The family members reported that they also obtained information from the internet and by reading about the diagnosis. For example:
"I had to request leave from work just to come and meet the doctor in order to get information on my brother's condition."
Monyaluoe et al. (2014) also found that one of the strengths of families of mentally ill family members is that they seek education on the mental illness of the family members. Literature confirms that if families are provided with educational information and are involved in the treatment process, mentally ill family members experience a reduction in symptoms, hospitalisation days and relapses (Tartakovsky, 2011; Yap, Reavley, & Jorm, 2012).
Developing a positive attitude: It emerged from the findings of this research that the family members accepted the conditions of their mentally ill family members when they stopped being negative. They learned to treat their mentally ill family members with respect. Most of the families explained that they learned a lot from the group sessions they used to attend with a specific psychologist who helped them to change their attitude towards their loved ones and they are now treating their loved ones well. For example:
" I stopped shouting at my sister because I realised that she is really sick, it is not adolescent stage like I thought."
"I realised that my daughter was really sick and I decided to talk to her well and gave her support by ensuring that she takes her medication as prescribed by the doctor."
Nichols (2008) confirms that positive attitudes help families to provide better support for family members with a mental illness.
Accepting their feelings: The family members expressed how they felt about their mentally ill family members when they were first diagnosed with a mental illness. They were in denial, ashamed and embarrassed but they realised that they had to accept their feelings in order to accept their loved ones' conditions. The direct quotations below are from interviews which were written in Setswana and translated into English:
" Wa itse ke ne ke sa dumele gore morwa waka o lwala tlhogo. Ke ne ke nagana fela gore o tlhakatlhakane ka ntlha ya stress mme go tla fela e se kgale. Ke ne ke palelwa ke go bolelela tsala yame gore ngwanake wa lwala mme ga jaana re bua ka yone re lokologile ka gore ke amogetse gore morwaake wa lwala." [You know I did not believe that my son is mentally ill, I thought it was just a confusion caused by stress that will clear up with time. I could not even tell my best friend that my son is sick, but now we can discuss it freely because I have accepted my son's condition.]
" Ke ne ke tlhabiwa ke ditlhong ga batho ba mpotsa ka bolwetse ba nnake. Ka gale ke ne ke ba ikgatholosa, mare gompieno ga ba mpotsa ke tlhalosa bolwetse ba nnake e kete ke bame." [I was always feeling ashamed when people asked me about my sister's condition. I used to ignore them, but currently when they ask me I explain my sister's condition as though it is mine.]
According to Geggie, De Frain, Hitchcock and Silberberg (2000), who conducted a family strengths research project, acceptance is indeed one of eight family strengths these authors identified. As in this case, acceptance was seen as showing respect, appreciation and understanding for the individuality of their family members (Geggie et al., 2000).
5.2. Having faith
Column B of Table 2 portrays a second theme, namely having faith as a strength that contributes to limiting relapses oftheir mentally ill family members. This theme could be divided into three sub-themes.
5.2.1. Praying together
The family members interviewed, indicated that they are strengthened by having faith in God. They expressed that praying together in their families assist them to carry on providing support to their mentally ill family members. They further indicated how prayer kept them going irrespective of the challenges they experienced with their mentally ill family members. The following are some of the direct quotations from the transcripts:
"You know sister, I have a strong relationship with God and that always give me courage to go on with life because God is a source ofmy strength."
"I am always strengthened by prayer especially when I pray with my prayer partners."
" Prayer brings me very close to God because when I am burdened I communicate with my God and I receive power to carry on with life."
Mokgothu et al. (2015) also report that faith and prayer are coping strategies in families caring for mentally ill relatives. Rammohan, Rao and Subbakrishna (2002) confirm that religious beliefs and practices are important resources for family members involved in caring for mentally ill relatives.
5.2.2. Going to church
From the interviews it emerged that going to church assists the families to have a strong spiritual base because they receive encouraging words from their pastors. The following are direct quotations from interviews translated into English:
" Ke rata go ya kerekeng ka gore moruti o phela a rera message o nthotlhoetsang thata. Le fa ausi a ne a le kwa sepetlele, moruti o ne a mo etela." [I always go to church because the pastor preaches messages of encouragement. Even when my sister was admitted at the hospital, the pastor visited her.]
" Ga nke ke rata go fetwa ke sermon go tswa go moruti wa rona ka gore ke kereya matla go tsawa mo melaetseng e a e rerang." [I don't want to miss any sermon from our pastor because I always receive strength from his messages.]
A strong spiritual base gives families a sense of belonging and acceptance by a higher being. It gives meaning and purpose to families that provide strength and hope in times of adversity (Thames & Thomason, 2000).
5.2.3. Fellowship with other believers
The families indicated that they have a good relationship with fellow believers and these believers provide them with support. They expressed that they sometimes feel down and they are always encouraged by fellow believers. For example:
" I always meet with a group ofladies in our church and they always give me a lot ofsupport especially when my son is not well."
" Every Wednesday I meet with my prayer partners and that gives me strength to go on even during tough times."
"During men's fellowship, I always get encouragement because we discuss our problems and we pray together for different problems."
Mokgothu et al. (2015) as well as Monyaluoe et al. (2014) also found that families should obtain social support to enable them to support their mentally ill family members. Thames and Thomason (2000) confirm that spirituality offers a belief system that can show people how to have healthy relationships within their family unit and with others.
5.3. Involving mentally ill family members in daily activities
The families experienced that involving their mentally ill family members in daily activities was a strength contributing to limiting a relapse. It seems that this strength developed over time, as seen in Column C of Table 2 and in the following discussion.
5.3.1. The families initially isolated their mentally ill family members
The family members indicated that they were not comfortable in involving their loved ones in daily activities the first time they were diagnosed with a mental illness. They thought that they will make mistakes because they thought the mental illness would permanently disable their family members.
Most of them reported that they did not allow their family members to do any household chores because they thought they will damage their property. As a result, mentally ill family members were isolating themselves as well because they also felt neglected by their families. For example:
" I did not want to allow him to touch anything in the kitchen because I thought he will break all my glasses because he broke some before he was admitted in hospital."
"I stopped her from doing the washing because I was scared that she will flood the house like it happened in the past."
" My daughter used to spend time in her bedroom, she would eat and do everything in her room, but now she sits with us in the dining room for meals and she is able to watch TV with us."
Nichols (2008) confirms that families can behave negatively towards their mentally ill family members as a result of the negative associations that mental illness carries.
5.3.2. After a process of acceptance, the families involve their mentally ill family members
It was indicated by most of the family members who were interviewed that they changed their approach after receiving more information on the condition of their mentally ill family members. Some reported that after meeting the doctors and nurses treating their family members, their attitude towards their loved ones changed a lot. They started involving them in activities such as household chores and they realised that these activities helped their family members to discover new things about themselves. For example:
" My son enjoy helping in the kitchen with cooking and washing of dishes because I allow him to cook for us. He is the best cook."
" I like to do shopping with my son because he helps me a lot especially when I want to buy new clothes. He has a very good eye when it comes to fashion."
Similarly, Mokgothu et al. (2015) found that families involve mentally ill members in daily activities, to keep them occupied and to provide intellectual stimulation. Hsiao and Van Riper (2010) also argue that it is valuable when families involve their mentally ill family members in an attempt to reintegrate them into the community.
5.4. Being aware of what aggravates mentally ill family members
Another family strength that may limit relapses is being aware of what aggravates the mentally ill family members (see Column D of Table 2). Similar to other strengths, it seems that this strength also developed through a process as explained in the following sub-theme.
5.4.1. Maintaining a calm attitude towards the mentally ill family members and communicating well
The family members expressed during the interviews how they used to have a negative attitude towards their mentally ill family members. They indicated that when their family members became agitated, they would shout at them and some would even fight with them. They realised that when they treated them like that, the mentally ill family members became more agitated and they would sometimes end up destroying something or injuring someone in the house. Most of the families interviewed, indicated that they changed their attitude towards their mentally ill family members through the help of professionals at the hospital. They attended group sessions and they learned from these sessions that when their mentally ill family members become agitated or angry, they should stay calm at all times to avoid aggravating their mentally ill family members. They also learned how to communicate with their mentally ill family members in order to avoid agitating them. The following quotations substantiate the above:
"I used to shout at him when he was agitated, but now when he start I move out ofthe room to give him space and I stay calm."
" I knew that my sister was mentally ill but I thought she is also stubborn and want to control us at home. I would shout at her and evenfight with her and she ultimately injured me on the arm, here is the scar. Now lately when she start becoming angry, I avoid her as much as possible and concentrate in doing something else until she is calm."
Mokgothu et al. (2015) also found that families use calming techniques, creative communication and praise as strengths. These findings are confirmed by Swink (2010) and Dangdomyouth, Stern, Oumtanee and Yunibhand (2008) who report that families use calm attitudes and respect as strengths in their communication with mentally ill family members.
6. Limitations, recommendations and conclusions
6.1. Limitations
The study was restricted to the clinical area of one mental health institution. Twenty five family members caring for mental health care users who attend their follow-ups at the mental health institution were contacted to participate in the study. Only 15 familymembers responded and participated in the study. The findings of the study cannot; therefore, be generalised.
6.2. Recommendations
Recommendations for nursing practices include the following: Psychiatric nurses helping family members who care for mentally ill family members should assist them through a process of acceptance and by providing educational information. The spiritual base of family members may be explored with the family as a strength to limit relapse. Psychiatric nurses should also facilitate the discovery of strengths of the family members and implementing these strengths in limiting relapse of their mentally ill family members. This may involve building trusting relationships, exploring family strengths together with the family, and evaluating if the family strengths explored assisted in limiting the relapse of mentally ill family members. Home visits might be very valuable in this regard. It would also be helpful if psychiatric nurses mobilise family support through utilising and enhancing existing support, for example to reflect with families on their available support from church members. This could also be organised by identifying and recruiting families caring for mentally ill family members in an area who are interested in joining a support group. These recommendations may also be included in nursing curricula, to prepare nurses to guide families to discover and implement their strengths to limit relapses in mentally ill family members.
In future research it may be valuable to implement and evaluate the recommendations made for nursing practices, to explore the acceptance process of families in more depth and to explore and describe the role of faith and faith communities in supporting families caring for mentally ill family members.
7. Conclusions
Reflecting on the data gained from the family members which literature confirmed, it became evident that these family members go through a process of initially not accepting the mentally ill family members due to emotional disturbance and negative attitudes, but through education from health professionals they accepted them. They discovered their strengths and started applying them to limit relapses in the mentally ill family members. From the findings it seems that there is a need that family members caring for mentally ill family members should be involved in their treatment from the onset, and that they should be guided through a process of acceptance.
One of the strengths the family members stressed to limit relapse in mentally ill family members is "acceptance through education". Educational information about the mental illness assisted them in developing a positive attitude and acceptance of their feelings as well as the condition of their mentally ill family members. Acceptance through education helped them to give their mentally ill family members the support they needed.
Another strength employed by the family members is "having faith". By having faith they are able to provide support to their mentally ill family members irrespective of the challenges they experience. Because they are strengthened by prayer, they have a strong spiritual base and they have access to support during difficult times through the availability of fellowship with church members. A strong spiritual base and support gives the family members a sense of belonging and acceptance. It also provides strength and hope in times of adversity.
A third strength used by the families is to involve mentally ill family members in daily activities. Involving mentally ill family members in daily activities helped them to take responsibility for their lives and for their own mental health.
The families also use the strength of maintaining a calm attitude, being aware of what aggravates mentally ill family members and using good communication skills, to limit relapses in mentally ill family members. Interacting with each other in an open, positive, honest and frequent manner thus contribute to the well-being of the families and the mental health of the mentally ill family members.
These strengths were incorporated in the recommendations for nursing practice, education and future research. These recommendations have the potential to contribute to limiting relapse in mentally ill family members.
Acknowledgements
The authors would like to acknowledge Johnson and Johnson as well as the North-West University for financial support in the research.
REFERENCES
Asay, S. M., & DeFrain, J. (2012). The international family strength model. Retrieved from http://congresomundial.eslup-content/uploads/Sylvia-Asay-The-international-family-strength. [ Links ]
Berglund, N., Vahlne, J. O., & Edman, A. (2003). Family interventions in schizophrenia: Impact on family burden and attitude. Social Psychiatry and Psychiatric Epidemiology, 38(3), 116-121. [ Links ]
Boyce, C., & Neale, P. (2006). Conducting in-depth interviews: A guide for designing and conducting in-depth interviews for evaluation input, monitoring and evaluation. Retrieved from https://www.measureevaluation.org/resources/training/materials/data-quality-portuguese/m_e_tool_series_indepth_interviews.pdf/view. [ Links ]
Byrne, P. (2000). Stigma of mental illness and ways of diminishing it. Advances in Psychiatric Treatment, 6(1), 65-72. [ Links ]
Creswell, J. W. (2007). Qualitative inquiry and research design: Choosing among five approaches. Thousand Oaks, CA: Sage. [ Links ]
Creswell, J. W. (2009). Research design: Qualitative, quantitative and mixed methods approach. Los Angeles, CA: Sage. [ Links ]
Croft, H. (2008). Accepting your loved one has mental illness. Retrieved from http://www.healthyplace.com/parenting/stress/accepting-mental-illness/. [ Links ]
Dangdomyouth, P., Stern, P. N., Oumtanee, A., & Yunibhand, J. (2008). Tactful monitoring: How Thai caregivers manage their relative with schizophrenia at home. Issues in Mental Health Nursing, 29(1), 37-50. [ Links ]
Defrain, J., & Stinnet, N. (2003). Family strengths. Retrieved from http://www.amazon.com/family-strengths-macmillan-international-encyclopedia.html. [ Links ]
Geggie, J., De Frain, J., Hitchcock, S., & Silberberg, S. (2000). Family strengths research project. Australia: University of Newcastle. [ Links ]
Hsiao, C. Y., & Van Riper, M. (2010). Research on care-giving in Chinese families living with mental illness: A critical review. Journal of Family Nursing, 16(1), 68-100. [ Links ]
Kazadi, K. J. B., Moosa, M. Y. H., & Jeenah, F. Y. (2008). Factors associated with relapse in schizophrenia. South African Journal of Psychiatry, 14(2), 52-62. [ Links ]
Koen, D., & Du Plessis, E. (2011). Strengthening resilience ofhealth caregivers and risk groups. Unpublished research proposal. NWU, Potchefstroom Campus, School of Nursing Science. [ Links ]
Laverty, S. M. (2003). Hermeneutic phenomenology and phenomenology: A comparison of historical and methodological considerations. International Journal of Qualitative Research, 2(3), 21-35. [ Links ]
Mokgothu, M. C., Du Plessis, E., & Koen, M. P. (2015). The strengths of families in supporting mentally-ill family members. Curationis, 38(1). http://dx.doi.org/10.4102/curationis.v38i1.1258. [ Links ]
Monyaluoe, M., Mvandaba, M., Plessis, E. D., & Koen, M. P. (2014). Experiences of families living with a mentally ill family member. Journal of Psychiatry, 17, 131. http://dx.doi.org/10.4172/Psychiatry.1000131. [ Links ]
Nichols, M. (2008). What can I do? Helping a friend or family member with a mental illness. Retrieved from http://anxietypanichealth.com/2008/10/09/what-can-i-do-helping-a-friend-or-family-member-with-a-mental-illness/. [ Links ]
Okun, B., & Kantrowitz, R. E. (2008). Effective helping: Interviewing and counselling techniques. Belmart, CA: Thomson Brooks/Cole. [ Links ]
Polit, D. F., & Beck, C. T. (2010). Essentials of nursing research: Appraising evidence for nursing practice. Philadelphia: Lippincot Williams & Wilkins. [ Links ]
Rammohan, A., Rao, K., & Subbakrishna, D. K. (2002). Religious coping and psychological wellbeing in carers of relatives with schizophrenia. Acta Psychiatrica Scandinavica, 105(5), 356-362. [ Links ]
Sittner, B. J., Hudson, D. B., & Defrain, J. (2007). Using the concept of family strengths to enhance Nursing care. The American Journal of Maternal Child Nursing, 32(6), 353-357. [ Links ]
Sousa, L., Ribeiro, C., & Rodrigues, S. (2006). Are practitioners incorporating a strengths focused approach when working with multi-problem poor families? Journal of Community & Applied Social Psychology, 17(1), 53-66. [ Links ]
South Africa. (2002). Mental Health Care Act 17 of2002. Pretoria. [ Links ]
Speziale, H. J. S., & Carpenter, D. R. (2007). Qualitative research in nursing. Philadelphia: Lippincott Williams and Wilkins. [ Links ]
Swink, D. F. (2010). Strategies for communicating effectively with people with mental illness. Retrieved from https://www.psychologytoday.com/blog/threat-management/201010/communicating-people-mental-illness-the-publics-guide. [ Links ]
Tartakovsky, M. (2011). 15 ways to support a loved one with serious mental illness. Retrieved from http://psychcentral.com/lib/211/15. [ Links ]
Thames, B. J., & Thomason, D. J. (2000). Family relationships: Building family strengths. Retrieved from http://www.clemson.edu/psapublishing/pages/FYD/FL529.PDF. [ Links ]
The Free Dictionary. (2016). Relapse. Retrieved from http://www.thefreedictionary.com/relapse. [ Links ]
Yap, M. B. H., Reavley, N. J., & Jorm, A. F. (2012). Intentions and helpfulness beliefs about first aid responses for young people with mental disorders: Findings from two Australian national surveys of youth. Journal of Affective Disorders, 136(3), 430-442. [ Links ]
Received 7 March 2016
Accepted 12 September 2016
Peer review under responsibility of Johannesburg University.
E-mail address: emmerentia.duplessis@nwu.ac.za (E. du Plessis).
* Corresponding author. Fax: +27 018 299 1827.
1 RISE: Strengthening the resilience of health caregivers and risk groups.


{kind=link}