










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkHealth SA Gesondheid (Online)
On-line version ISSN 2071-9736
Print version ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 n.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2015.12.002
SPECIAL ISSUE: TOPIC 1
Perception and attitude of healthcare workers towards the use of a female condom in Gaborone, Botswana
B. Mashanda-Tafaune; L.V. Monareng*
Department of Health Studies, University of South Africa, South Africa
ABSTRACT
BACKGROUND: Although the female condom (FC) is viewed as an effective female controlled barrier contraceptive device that can be used by women to prevent them from contracting the Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS), other sexually transmitted infections (STIs) and unwanted or unintended pregnancy, the perception and attitude of healthcare workers (HCW) plays a key role in its effective use and distribution amongst women.
OBJECTIVES: To identify and examine factors that influences the perception and attitude of HCWs towards the use and distribution FCs.
METHOD: A quantitative, explorative and descriptive design was used to conduct the study based on the Health Belief Model (HBM) as a conceptual framework. A pre-tested questionnaire was utilised in June 2013 to collect data from a convenience sample of 164 HCWs with a 100% return rate. Data was analysed using the Statistical Package for Social Sciences (SPSS) version 13.0 and Statistical Analysis Systems (SAS) version 9.2.
RESULTS: The results showed that 64.0% (n = 105) of the respondents perceived unavailability of FCs as contributing to lack of adequate use. Only 31.7% (n = 52) [95% CI: 24.7-39.4] of them reported to be using the FC. There was an association with increasing use of a FC with age (Fischer's exact = 0.05), marital status [Fischer's exact = 0.037] and training [χ2 = 53.3; p < 0.05]. The results revealed that lack of knowledge and training on the use of a FC might prevent its effective use and distribution.
CONCLUSION: The results showed evidence that the FC was a safe method of contraception and protection against STIs and that it empowers women to make decisions related to sexuality. However, awareness campaigns, increased availability of FCs and training of HCWs are essential to enhance positive perception and attitudinal change to reduce sexual risks related infections and poor quality of life for women.
Keywords: Attitude; Female condom; Healthcare workers; Perception
1. Introduction and background
Young women aged between 15 and 24 years are eight times more likely to be infected with HIV than men (Female Condom, 2006:1; UNAIDS, 2010:12).). In Sub-Saharan Africa, around 60% of those living with HIV are female, and the proportion of women living with HIV has been increasing in the last 10 years (Jones et al. 2009:70).The increased vulnerability to transmission of HIV among women is influenced by a number of social, economic, biological or anatomical political factors. The practice of family planning (FP) assists in reducing the rates of unintended pregnancies, maternal and child mortality and of induced abortions. Using contraceptives has been shown to promote a sense of autonomy among women and to increase their ability to make decisions in other areas of their lives especially with regards to sexuality (Mahadeen, Khalil, Hamdan-Mansour, Sato, & Imoto, 2012:568).
Condoms have played a decisive role in HIV prevention efforts in many countries. Both male and FCs form a main component of an overall comprehensive strategy to reduce risks of sexual exposure to HIV. The FC has the potential to decrease STI statistics, as the only female-initiated dual protection device that is believed to be effective in preventing STIs, HIV and unintended pregnancy. Latex and polyurethane type of FCs are materials commonly used to create an effective barrier method against the most common STIs, which in Sub-Saharan Africa includes HIV. Currently, it has been noted that the most widely used biomedical barrier intervention is the male condom. It provides a barrier to HIV and if properly used is effective to prevent transmission of infection. Both male and FCs are available, but FCs are more expensive and seemingly more difficult to use (Barnett & Whiteside, 2006:46). FCs offers a similar degree of protection from STIs as the male latex condom, although the level of protection has not been quantified or researched for each specific STI. For maximum effect, the WHO (2011:8) emphasizes that any barrier method for contraception or infection prevention must be used correctly and consistently.
However, the male condom can only be used by a willing male user and with the predominantly patriarchal culture in Southern Africa and socioeconomic imbalances having most of the men being breadwinners, leaves women in a vulnerable state to insist on the use of a male condom. Therefore, the FC seem to be an essential alternative to empower women to make decisions in this regard (Female Condoms, 2011:1; Mantell, Scheepers, & Karim, 2000:589).
1.1. Problem statement
Perception, as defined by King (1981:24) cited in Ross and Cobb (1990:24), is "a process of organizing, interpreting, and transforming information from sense data and memory. It is a process of human transactions with the environment." Perception in the context of this study about use and distribution of FCs as environmental stimuli is a key operational concept for HCWs. Although the FC seems to be a necessary device for females to use in order to prevent HIV, STIs and unwanted pregnancy, the main or primary distributers of the condoms, who are the HCWs, seem to have a negative perception towards use of the device. This perception seem to be influenced by their past experience and history on its use resulting in low usage and reluctance to promote it among women. Although the use of the FC is reported by findings from a study conducted by Aimee et al. (2011:329) as effective in reducing woman's risk of re-infection, with different strains of HIV, and transmitting HIV or other STIs to their partners, it however remains underutilized. Therefore, the perception of the HCWs on the environmental stimuli which is about the use and distribution of FC makes them have their own disposition on the phenomena that influences their attitude towards its use and distribution.
One of the main ways to gauge an individual's view of the world is through attitude. The Chambers Paperback Thesaurus (2012:51) records that attitude concerns how an individual thinks, believes, views an object, makes conclusions or expresses feelings of like or dislike of an object which will ultimately influence resultant actions. Neilands and Choi (2002:158) identified some negative attitude towards use of FC to be due to lack of partner cooperation; mechanical problems with device insertion and removal; lack of sexual communication; lack of access to the FC immediately prior to intercourse and the high cost of FCs.
Therefore, an empirical investigation on perception and attitude of HCWs towards the use of FCs was imperative in order to identify contributory factors that need to be dealt with to improve the quality of life for women.
1.2. Aim of the study
The aim of this study was to examine factors related to the perception and attitude of HCWs towards the use of FCs as the core distributors of the FCs.
1.3. Objectives of this study were to
To explore and describe factors that influences HCWs to develop positive or negative perception and attitude towards the use of a FC.
2. Research design and method
2.1. Study context
The study was conducted at Bokamoso Hospital with 73.2% (n = 120) respondents, Extension 2 Clinic with 18.3% (n = 30) respondents and the Village Clinic with 8.5% (n = 14) respondents in Gaborone, Botswana. Bokamoso Hospital is a 200 bedded multidisciplinary hospital in the Kweneng District. It is designed to cater for inpatients, outpatients and specialised clinics. It has approximately 300 HCWs which include: doctors; nurses, physiotherapists, occupational therapists and other support staff. Extension 2 Clinic is a 24 h clinic which has 3 consulting rooms and a 3 bedded emergency room with a turnover of 300 patients. The Village Clinic is an 8 h clinic with 2 consulting rooms and has a turnover of 50-60 patients. The setting for the study was appropriate as most of the staff members are involved in the distribution of contraceptives including FCs.
2.2. Research design and method
A quantitative, explorative and descriptive survey design was used to conduct the study. The study population included all male and female HCWs who had two years or more working experience as a HCW, above 18 years of age and at different levels of education. The convenience sampling method was used to recruit an accessible sample of 164 respondents with a return rate of 100%.
2.3. Development of the data collecting instrument
The desired information to construct the data collecting instrument was made possible through conducting a comprehensive literature review on the study construct. Previously validated and reliable questionnaires used for studies similar were reviewed and some items carefully selected. The degree of formality in which questions were formatted was done carefully with a permissive tone, suggesting that any of the possible responses would be acceptable and that each item in the questionnaire had a response set, which provided parameters within which the respondent could answer. The response set was narrow and directed, with a list of alternatives from which to select as closed-ended questions were used.
The first section was about the biographical information of the respondents. Secondly, the Likert scale, as a composite measure of perception and attitude involving a summation of scores on a set of items was used. This type of scale was used in this research as HCWs had to express perception, attitude or other responses in terms of the ordinal-level categories such agree or disagree that were ranked in a continuum (De Vos, Strydom, Fouche, & Delport, 2011:212). The data collection instrument was pre-tested and modifications done accordingly, especially in terms of the sequencing of the items.
2.4. Validity and reliability
Face, content and construct validity of the instrument were ensured by seeking the input of the three experienced doctors as distributors of FCs, statistician and that of the academics who were experts on the study phenomena. Their input was sought for to determine the readability and clarity of content. Construct validity was ensured by conducting an extensive literature review and consulting a variety of dictionaries and discipline sources to provide conceptual and operational definitions of all the key concepts of the construct. The Cronbach's alpha (co-efficient alpha) reliability of the instrument was done. Coefficient alpha is an index of internal consistency to estimate the extent to which different items of an instrument are reliably measuring the construct (Polit & Beck, 2012:333). The Cronbach's alpha reliability results of this study were 0.7 which indicated internal consistency.
2.5. Ethical considerations
Ethical clearance was obtained from the Research and Ethics Committee of the Department of Health Studies at the University of South Africa. Permission to conduct the study was obtained from the management of the hospital and the clinics. A written, informed consent was obtained from the respondents. Confidentiality, anonymity and privacy were ensured by omitting respondents' names and contact details on the questionnaire.
2.6. Data collection process
After permission was obtained, data were collected on site using a structured questionnaire and the questionnaires were administered to the HCWs by the researcher and two trained volunteers over a period of one week in June 2013. Respondents were informed briefly about the purpose of the study and received guidance on how to complete the forms anonymously, correctly and return them immediately. Each self-reporting completed questionnaire was confidentially placed in a secure separate folder from other questionnaires. The same process was followed at each study context until the desired size was obtained.
2.7. Data analysis
The collected data were entered for analysis using the SSPS program version 13.0 and SAS version 9.2 statistical software packages (SAS software systems for windows, 2009). Statistical tests such as Fischer's exact, chi squareχ2, descriptive and inferential reasoning were utilised to calculate frequencies, summarise the results and to draw conclusions.
3. Research results
The major areas under which the results are presented in a form of percentages are in relation to the socio demographic data, FC use, perception and attitude of HCWs.
3.1. Socio-demographic data
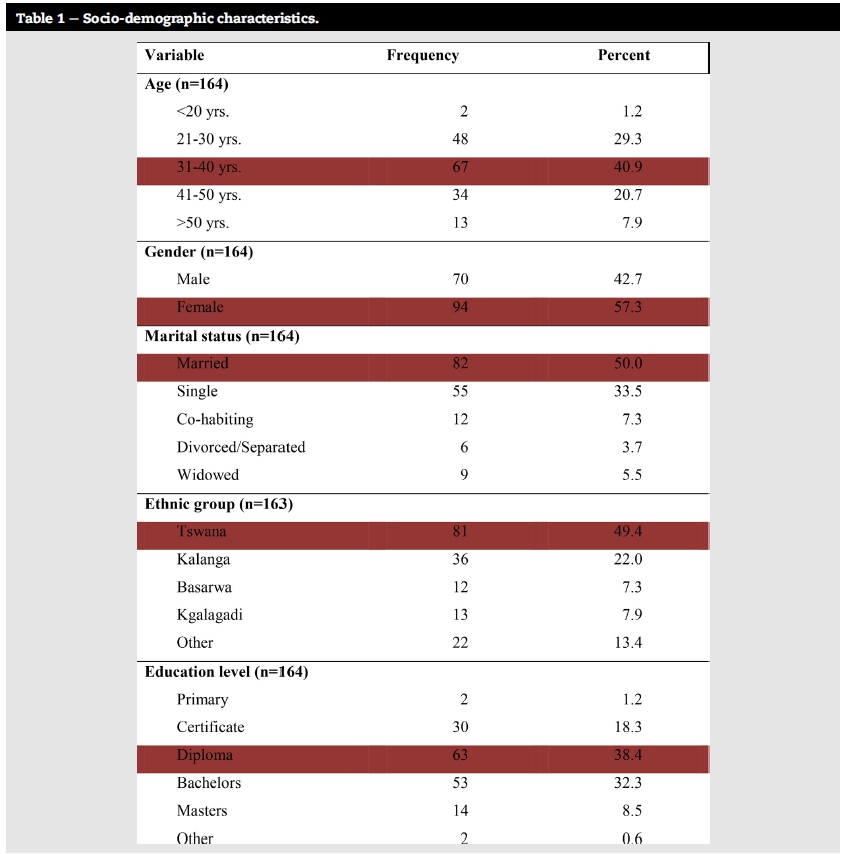
Table 1 summarises the results related to the socio demo-graphic data for the convenient sample (n = 164) of the HCWs in the order of their significance.
Only demographic variables of age, gender and marital status evidenced a statistically significant association with regard to the use of a FC.
Of the respondents, 1.2% (n = 2) respondents were less than 20 years, 29.3% (n = 48) were aged between 21 and 30 years, most of them 40.9% (n = 67) were aged between 31 and 40 years which was also the median age group, 20.7% (n = 34) were between the age of 41 and 50 and 7.9% (n = 13) were 50 years and older. There was a trend and a significant association towards increasing use of a FC with age (Fischer's exact = 0.051).
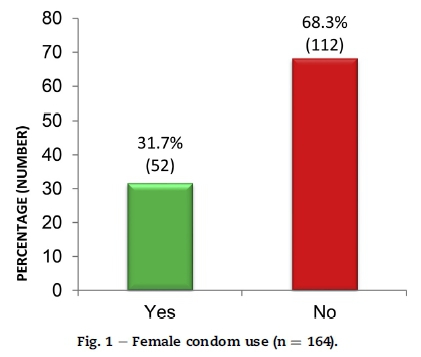
Of the respondents 31.7% (n = 52) [95% CI 24.7-39.4] of the respondents reported to be using the FC whilst 68.3% (n = 112) of the respondents reported that they had never used a FC as illustrated in Fig. 1. This confirmed that most HCWs in the study context had not used a FC. A study conducted by Mantell, West, et al. (2011:66) concurs with this finding as out of 78 healthcare providers only 9 providers, 11.5% comprising of eight women and one man reported having used the FC. In this study, there were more female respondents 57.3% (n = 94) than male 42.7% (n = 70) who completed the questionnaire as illustrated in Table 1.
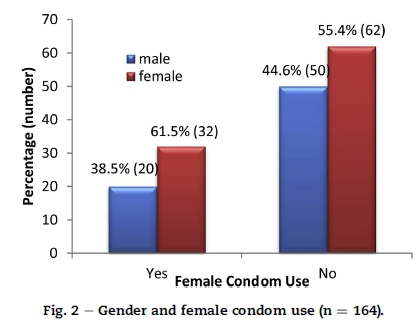
Out of the respondents, 31.7% (n = 52) reported using the FC, 38.5% of whom (n = 20) were male while 61.5% (n = 32) were female. Out of the 68.3% (n = 112) respondents that have never used a FC, 44.6% (n = 50) were male and 55.4% (n = 62) were female. There was a significant association between gender and use of the FC as evidenced by a chi square result of χ2 = 0.555 with a p value of 0.454. Therefore, in this study more females used the device than men. According to a study conducted by Mantell, West, et al. (2011:69), gender seemed to influence providers' attitude about the use of a FC. Fig. 2.
Half of the respondents were married 50.0% (n = 82), almost a third were single 33.5% (n = 55), 7.3% (n = 12) were cohabiting, 3.7% (n = 6) were separated or divorced and 5.5% (n = 9) were widowed. There was significant association observed between marital status and use of FC as identified by Fischer's exact = 0.037. However, in a study conducted by Mbarushimana and Ntaganira (2013:16), more single respondents had knowledge on the use of the FC than married respondents which does not concur with the findings of this study where more married people had higher rates of FC knowledge and use.
Findings in this study also support the need for training of HCWs to enhance translation of knowledge to actual positive perception, attitude change and positive behavioural outcomes as the need is displayed in Fig. 3.
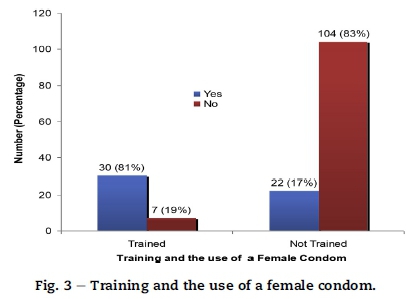
Of the trained 37 HCWs, 81% (n = 30) had used the FC and 19% (n = 7) had not used the FC and of the 126 respondents who had not been trained on the use of a FC, 17% (n = 22) had used it while 83% (n = 104) had not used it. There was evidence of a strong association between the training and the use of a FC (χ2 = 53.3; p < 0.05). This result is supported by Brady, Austrian, Geibel, Mwangi, and Sudha (2009:5) who alluded that service providers need to be adequately trained so that they can confidently demonstrate use of a FC to clients, provide accurate information, counselling and support for its use.
Most of the HCWs 93.9% (n = 154) had not used a FC in the past 3 months, 92.1% (n = 151) had not used the FC in the past 6 months and a total of 90.9% (n = 149) had used the FC in the past 12 months. There is general evidence of underutilisation of FCs based on this result.
Table 2 provides an exhibit of the perception of health care workers with regard to the use of a FC.
The majority of the respondents 64% (n = 104) disagreed that the FC was readily available on the market as supported by Peters, Jansen, and Van Driel (2012:124) who reported in their findings that FCs are not readily available on the market. Of the respondents 36.6% (n = 60) disagreed that the FC was not expensive.
Comparing the male condom and FC, 43.9% (n = 72) of the respondents were undecided while most of them 46.3% (n = 76) disagreed and majority of respondents were undecided 57.5% (n = 95) as to whether sex was more comfortable with a FC while 33.5% (n = 55) disagreed that sex was more comfortable with a FC. In a study conducted by Choi and Gregorich (2009:1-2) on social network influences on male and female condom use among women, state that although FC use can reduce the risk if HIV infections, but most women are comfortable with male condom use if used correctly and consistently for comfort, pleasure and prevention of sexual transmission of HIV.
Most of the respondents 60.4% (n = 99) agreed that using the FC does not interrupt the sexual act while 34.8% (n = 57) were undecided. On the item of comparing the material of the FC if it was more durable than the male condom, 69.5% (n = 114) were undecided while 20.7% (n = 34) disagreed and only 9.7% (n = 16) agreed that it was durable.
The majority of the respondents 46.3% (n = 76) agree, 31.7% (n = 52) were undecided and 25.9% (n = 36) disagreed that the level of education influences perceptions on the use of a FC. Most of the respondents 84.8% (n = 139) agreed that counselling sessions with women would help influence their choice with regards to the use of a FC, 12.8% (n = 21) were undecided and 2.4% (n = 4) were disagreeing. According to Holt et al. (2013:2), several health care providers reported support for FCs owing to the belief that counselling women on the use of FCs gives them choice and control over their sexuality.
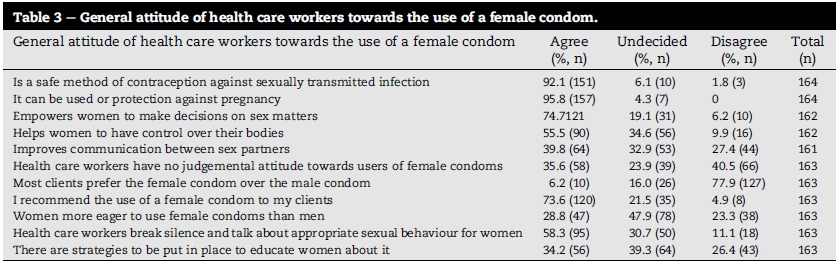
It is worthy to note that the attitude of HCWs can mediate as an intervention to promote use of a FC or discourage potential users of the device to protect themselves as evidenced on Table 3.
Most of the respondents 92.1% (n = 151) agreed, and 6.1% (n = 10) were undecided that the FC was a safe method of contraception against HIV/STI. However, the respondents showed a positive attitude towards use of a FC for protection against pregnancy as 95.8% (n = 157) agreed. The majority of respondents 74.7% (n = 121) agreed, 19.1% (n = 31) were undecided and 6.2% (n = 10) disagreed that the FC empowered women to make decisions. Most respondents 77.9% (n = 127) disagreed that clients prefer the FC over the male condom as supported by information in the National condom strategy that says that FC use is very low, with an estimated Condom Prevalence Rate of 0.1% against over 10% for male condoms (Botswana Ministry of Health, 2012:16). The majority of the respondents agreed 73.6% (n = 120) and 4.9% (n = 8) disagreed that they would recommend the use of the FC to their clients while 21.5% (n = 35) were undecided. The study revealed that approximately half the respondents 58.3% (n = 95) would break the silence and talk about appropriate sexual behaviour for women.
However, the findings highlighted a number of general issues that have a bearing on how HCWs are influenced to promote use and distribution of FCs.
Of the respondents 89.6% (n = 146) agreed that HCWs have the potential to influence positive use of the FC, 95.1% (n = 155) agreed that HCWs needed to be empowered with knowledge about the FC use. Of the respondents, 54.6% (n = 89) agreed and 5.5% (n = 9) disagreed that more funding should be made available to increase the number of FCs in the market while 39.9% (n = 65) were undecided. Most of the respondents 82.2% (n = 134) agreed that the media should be used to teach the public about FCs.
Out of 164 respondents 95.7% (n = 157) agreed that the level of knowledge about the FC influences HCWs with regards to its use which concurs with the result of the number of HCWs that are trained as displayed in Fig. 3 and the evident low use of the device.
3.2. Discussion
The use of the FC according to Aimee et al. (2011:338) correlates positively with the use of a male condom. However in this study, FC was noted as the only FP method that is controlled by females themselves as a barrier method for dual protection against HIV/STI infections and unwanted pregnancy. Gender inequities in sexual relationships due to dominating male power, often limit women from taking control on decisions related to sexuality and accounts for much of the spread of HIV and STIs (Shai, Jewkes, Nduna, & Dunkle 2012).
Although use of a FC is regarded as a safe method, Peters et al. (2012:120) argue that FCs are far less accepted and accessible, and have remained expensive and highly underfunded and consequently, most women and girls in sub-Saharan Africa lack access to it. The evidenced low usage of a FC seem to influence the knowledge about its quality and value to reduce high sexually risk related infections. Shai et al. (2012:2) contend that women therefore, need to be familiarised with the use of male condoms which are readily available and less costly for HIV prevention.
Women are those whose quality of health is most affected by HIV/AIDS and STIs which has implications on the health outcomes for their children, especially the under-five. An information brochure was developed from the results of this study on FC use to provide guidance on how to empower the HCWs to demystify the negative myths about its use, so that they may advocate for the vigorous distribution and its use.
The information brochure is an educational tool, which will aid HCWs during campaigns to train and empower patients on the advantages, technique of insertion and use of a FC. Such material should be readily available in areas that are easily accessible to sexually active clients, especially hospital and clinic consultation rooms, waiting areas and shops that sell contraceptive devices.
However, understanding the factors that influence HCWs perception and attitude related to FC use is valuable for explaining why there is such low usage of the FC device (Shai et al. 2012:1).
Healthcare providers according to Warren and Philpott (2003:137), and perhaps more importantly peer educators and outreach workers, ought to develop an expertise in answering queries about sexuality, female anatomy as well as specific issues about the use of a FC. Challenges related to initial use of a FC need to be addressed because HCWs can be uncomfortable about recommending products with which they are not familiar with. Some key elements of the HBM provide a way to understand and predict how HCWs will behave in relation to their health along with that of their clients. The model is firstly based on the understanding that individuals engage in health related behaviour such as use of a FC if they are convinced that a negative health condition such as HIV/AIDS can be avoided. Secondly, if they perceive that they can successfully take a recommended health action such as use of a FC comfortably and with confidence (Hayden, 2009:31-32). Hence, training of HCWs is paramount in promoting use of FCs. FCs can provide dual protection depending on the way in which information and counselling services are effectively provided. With the high rates of HIV/AIDS globally and particularly in Sub-Saharan Africa and at the study context, HCWs play a key role in educating women, who are the higher consumers of FP services. Training on condom skills and benefits of various methods of FP, particularly the use of FC, as well as in distributing them so that they may prevent HIV/AIDS and other STIs from spreading are of paramount importance (Aimee et al. 2011:330).
With regards to perception of HCWs towards the use of a FC, it is interesting to note that most of the respondents were undecided in their responses which may be because most of them had not used a FC before or had used it few times as evidenced on Table 2. However, there are still some issues that need to be attended to by the relevant authorities, Health Ministries and health organisations to enhance the use and distribution of FCs for improving the quality of life for women.
3.3. Limitations
Limitations are those theoretical and methodological restrictions or weaknesses in a study that may decrease the generalizability of the results (Burns & Grove, 2013:598, 699). The study was limited to one geographical area, three non-randomly selected study settings which poses a limitation on the scope of this study and generalization of results because of the small sample size. The use of a convenience sample to recruit participants threatened the internal validity. Due to a lack of randomisation processes, the representation of the population was limited. The sample was largely women which could have led to desirability bias to support the research hypothesis.
4. Implications
The following implications based on the findings are notable pertaining to the use and distribution of FCs in terms of education, public health and further research.
4.1. Education related implications
Media awareness campaigns are recommended to target specific groups of people such as women, teenage girls as well as men. In-service workshops ought to be held for HCWs and the public to demonstrate the insertion techniques and opportunities to practice inserting a FC. Counsel should be provided to government policy-makers, programmers or strategic planners and healthcare clinical practitioners about the need for their strategic involvement and input. Education on the use of a FC needs to be further expanded to all health professionals who attend to patients such as doctors, nurses, pharmacists and staff at rehabilitation centres. They will assist in effectively conducting health education talks and distribution of the FC and other forms of contraception to patients and the general public. The training curriculum of HCWs should evidence teaching and assessment on content related to the use of FCs.
4.2. Public health implications
Availability of the FC in all healthcare centres as well as public places where the general public can access them such as public toilets is recommended. The Department of Health and local authorities should distribute pamphlets or brochures that have information about the use of a FC in English as well as other local languages. Use of simple, well written brochures on the phenomena will provide readily available information to those visiting the health centers.
4.3. Further research implications
Similar but larger qualitative and quantitative studies may be conducted or replicated in other parts of Botswana or beyond as on the effective use of a FC as well as contraception as a whole to combat spread of HIV/STIs and prevention of unwanted pregnancy.
4.4. Concluding remark
Most respondents in this study concurred with the notion that a FC can be used for prevention of pregnancy, spread of HIV/AIDS and STIs. Therefore, educating and training the HCWs plays a major role in the use and distribution of FCs. This was illustrated by more HCWs, 81% (n = 30) who had been trained on the FC actually using the FC, hence becoming better advocates for its use. The results of this study do support the research hypothesis that a positive attitude and perception of HCWs about the use and distribution of FCs would significantly determine effective use and distribution of FCs.
5. Conclusion
Given the current challenges that the medical field and researchers has to discover an effective vaccine against HIV/STs, a female controlled method for dual protection against the stated infections and unwanted pregnancy seems to be promising. Although perception and attitude change is important for effective use and distribution of FCs, other factors such as availability, training and cost implications have an notable impact. The timing of this study is good to encourage all the stakeholders such as managers of the services, researchers, service providers, pharmaceutical companies and male partners to promote interest on the sustainable use of a FC.
Author contributions
The student (Dr B Mashanda-Tafaune) was the primary researcher under the guidance of the supervisor (Professor LV Monareng) from proposal writing until the final submission of the dissertation. Both authors participated in drafting the article, correcting it and approving its submission for publication.
Acknowledgements
Sincere appreciation is expressed to the research respondents for their corporation. Sincere thanks to the management of Bokamoso Hospital, Extension 2 Clinic, and the Village Clinic in Gaborone, Botswana for granting permission to conduct the study. Gratitude is also expressed to the Department of Health Studies Research and Ethics Committee (HSREC) of UNISA for approving the study.
References
Aimee, N. C. C., Tross, S., Mei-Chen, H., Pavlicova, M., Kenney, J., & Nunes, E. V. (2011). Female condom skill and attitude: results from a nida clinical trials network gender-specific HIV risk reduction study. AIDS Education and Prevention, 32(4), 329e340. [ Links ]
Barnett, T., & Whiteside, A. W. (2006). AIDS in the Twenty-first century: disease and globalization (2nd ed.). United Kingdom: Palgrave Macmillan. [ Links ]
Botswana Ministry of Health. (2012). National health policy. Gaborone: Government Printer. [ Links ]
Brady, M., Austrian, K., Geibel, S., Mwangi, D., & Sudha, S. (2009). Female initiated prevention: Integrating female condoms into HIV reduction risk activities in Kenya. Nairobi: Population Council. [ Links ]
Burns, N., & Grove, S. K. (2013). The practice of nursing research: Appraisal, synthesis, and generation of evidence (7th ed.). St Louis: Elsievier Saunders. [ Links ]
Choi, K. H., & Gregorich, E. (2009). Social network influences on male and female condom use among women attending family planning clinics in the US. Sexually Transmitted Diseases, 36(12), 757e762. http://dx.doi.org/10.1097/QLQ.0b013e3181afefc1. [ Links ]
De Vos, A. S., Strydom, H., Fouche, C. B., & Delport, C. L. S. (2011). Research at grass roots: For the social sciences and human service professions (4th ed.). Van Schaik. [ Links ]
Female Condom. (2006). A powerful tool for protection. Seattle: UNFPA, PATH. viewed 03 June 2011, from http://www.unfpa.org/webdav/site/global/shared/documents/publications/2006/ female_condom.pdf. [ Links ]
Female Condoms. (2011). Prevention for women. viewed 29 August 2011, from http://www.genderhealth.org/the_issues/women_girls_and_hiv/female.condoms/. [ Links ]
Hayden, J. (2009). Introduction to health behavior theory. Sudbury: Jones and Bartlett. [ Links ]
Holt, K., Blanchard, K., Chipato, T., Nhemachena, T., Blum, M., Stratton, L., et al. (2013). A nationally representative survey of healthcare provider counselling and provision of the female condom in South Africa and Zimbabwe. British Medical Journal, 3(3), 1e8. [ Links ]
Jones, D. L., Chitalu, N., Ndubani, P., Mumbi, M., Weiss, S. M., Villar- Loubet, O., et al. (2009). Sexual risk reduction among Zambian couples. Journal of Social Aspects of HIV/AIDS, 6(2), 69e75. [ Links ]
Mahadeen, A. I., Khalil, A. O., Hamdan-Mansour, A. M., Sato, T., & Imoto, A. (2012). Knowledge, attitudes and practices towards family planning among women in the rural southern region of Jordan. Eastern Mediterranean Health Journal, 18(6), 567e572. [ Links ]
Mantell, J. E., Scheepers, E., & Karim, Q. A. (2000). Introducing the female condom through the public health sector: experiences from South Africa. Aids Care, 12(5), 589e601. [ Links ]
Mantell, J. E., West, B. S., Sue, K., Hoffman, S., Exner, T. M., Kelvin, E., et al. (2011). Health care providers: a missing link in understanding acceptability of the female condom. AIDS Education and Prevention, 23(1), 65e77. [ Links ]
Mbarushimana, V., & Ntaganira, J. (2013). Knowledge and attitude to female condom use among undergraduates of Kigali Health Institute. Rwanda Journal of Health Sciences, 2(1), 16e25. [ Links ]
Neilands, T. B., & Choi, K. H. (2002). A validation and reduced form of the female condom attitude scale. AIDS Education and Prevention, 14(2), 158e171. [ Links ]
New edition. The Chambers paperback thesaurus (2012). Edinburgh: Chambers Harrap Publishers. [ Links ]
Peters, A., Jansen, W., & Van Driel, F. (2012). The female condom: the international denial of a strong potential. Reproductive Health Matters, 18(35), 119e128. [ Links ]
Polit, D. F., & Beck, C. T. (2012). Nursing research, generating and assessing evidence for nursing practice (9th ed.). Philadelphia: Lippincott, Williams & Wilkins. [ Links ]
Ross, B., & Cobb, K. (1990). Family nursing: A nursing process approach. Redwood City, CA: Addison-Wesley Nursing. [ Links ]
Shai, N. J., Jewkes, R., Nduna, M., & Dunkle, K. (2012). Masculinities and condom use patterns among young rural South Africa men: a cross sectional baseline survey. BMC Public Health, 12, 1e9. [ Links ]
UNAIDS, United. (2010). Nations joint programme on HIV/AIDS. Geneva: Report on the Global AIDS Epidemic. [ Links ]
Warren, M., & Philpott, A. (2003). Expanding safer sex options: introducing the female condom into national programmes. Reproductive Health Matters, 11(21), 130e139. [ Links ]
World Health Organization. (2011). HIV/AIDS-Microbicides. Geneva:WHO. [ Links ]
SAS software systems for windows computer program. (2009). Cary, NC: SAS Institute. Version 9.2. [ Links ]
Further reading
Compact Oxford Dictionary and Thesaurus. (2009). Sv "attitude" (3rd ed.). Oxford: Oxford University Press. [ Links ]
King, I. M. (2011). King's conceptual system and theory of goal attainment and transactional process. From http://nursingtheories.weebly.com/imogene-m-king.html Accessed on 12.06.13. [ Links ]
Mantell, J. E., Smit, J. A., Beksinska, M., Scorgie, F., Milford, C., Balch, E., et al. (2011). Everywhere you go, everyone is saying condom, condom. But are they being used consistently? Reflections of South African male students about male and female condom use. Health Education Research, 26, 859e871. [ Links ]
Received 17 February 2015
Accepted 3 December 2015
Available online 25 March 2016
E-mail address: monarlv@unisa.ac.za (L.V. Monareng).
Peer review under responsibility of Johannesburg University.
* Corresponding author. Department of Health Studies, PO Box 392, University of South Africa, 0003, South Africa.


{kind=link}
{kind=link}
{kind=link}